臨床特徵 (Clinical features)
- 噴發性黃色瘤(eruptive xanthomata)為小型(1–4 mm)黃色丘疹,伴 red halo,好發於臀部、肩部與四肢伸側。
- 亦可見於 antecubital 與 popliteal fossae、axillae、lips、eyelids、ears。
- 常成群出現(crops),可隨血漿 lipoprotein 濃度起伏(wax and wane)。
- 病灶通常於數週內自行消退(spontaneously over a period of weeks)。
- 常伴搔癢,丘疹有時有壓痛;偶可表現 Koebner phenomenon;癒合偶伴 hyperpigmented scars。
- Langerhans cell histiocytosis 的皮膚病灶與 adenocarcinoma 的皮膚侵犯可模擬 eruptive xanthoma。
組織特徵 (Histologic features)
- 組織學變化主要見於 superficial reticular dermis。
- 早期病灶 histiocytes 眾多,而典型 ‘foam cells’ 有時數目少;浸潤可混雜 lymphocytes 與 neutrophils。
- 成熟丘疹中以具典型透明或泡沫狀胞質的 xanthoma cells 為主;偶見低倍下 palisading 外觀與 urate-like crystals。
病因與關聯 (Etiology & associations)
- 與 hypertriglyceridemia 相關,最常發生於 hyperchylomicronemic states;有時與 VLDL 增高相關。
- 最常見原因為 secondary hyperlipoproteinemia(HPL),尤其伴 diabetes mellitus 與 alcohol ingestion,或藥物誘發(例:exogenous estrogens、corticosteroids、retinoids)。
- 亦可因 lipoprotein lipase 活性下降、ApoCII deficiency 或 VLDL 合成增加(阻斷 chylomicron 取得 lipoprotein lipase)而發生。
- 常伴其他高血脂特徵:lipemia retinalis、hepatosplenomegaly、abdominal pain、pancreatitis。
- 常於數天內快速發展,偶伴自發消退。
- 胞內脂質(與其他多含 cholesterol 的 xanthomata 相反,主要為 triglyceride)處於變動狀態,可伴細胞外沉積,此現象在其他類型 xanthomata 罕見或無。
- 所有 xanthomata 中巨噬細胞內脂質以脂肪染色(oil red O、scarlet 或 Sudan red)呈陽性。
鑑別診斷 (Differential diagnosis)
- 與 granuloma annulare 組織學上可混淆,兩者皆有真皮間質性組織球浸潤伴不等量黏液增加。
- 雖然細胞外脂質可破壞真皮膠原,但 necrobiosis 非 eruptive xanthoma 特徵,palisading 亦非其特徵;其巨細胞少,血管周浸潤為 histiocytic(granuloma annulare 為血管周 lymphocytes)。
- 帶 urate-like crystals 的 eruptive xanthoma 曾被誤診為 gout;免疫組化提示這些 urate-like crystals 由 chylomicrons 構成。

圖 13-3:Eruptive xanthoma:臀部出現眾多小型黃色丘疹。
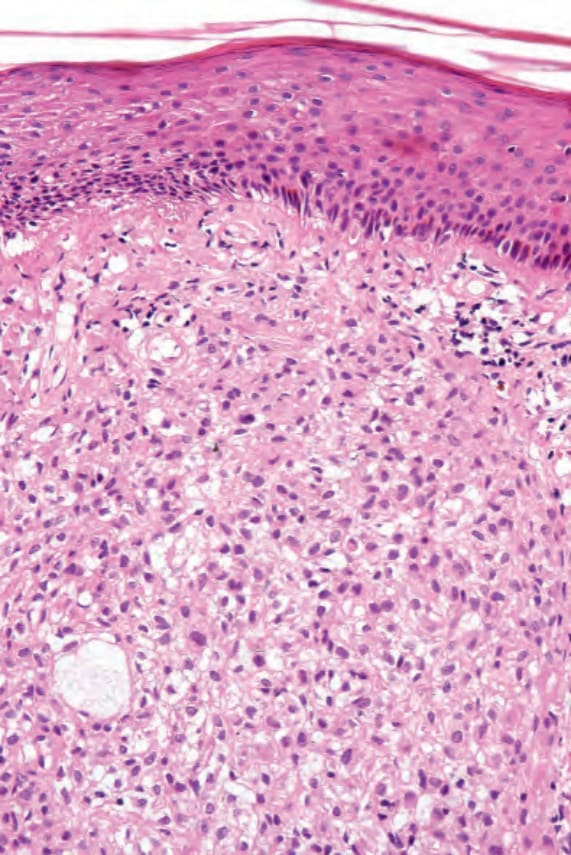
圖 13-4:Eruptive xanthoma:成熟病灶切片,histiocytes 具豐富空泡狀胞質。
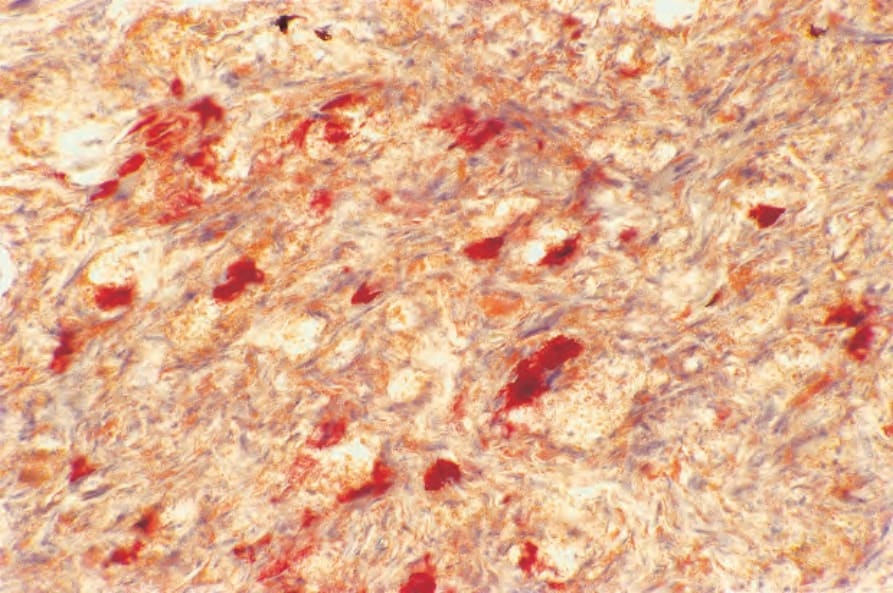
圖 13-7:Eruptive xanthoma:巨噬細胞內脂質以 oil red O 呈陽性。