Eruptive xanthomata
Eruptive xanthomata
Clinical features Eruptive xanthomata are small (1–4 mm) yellowish papules with a red halo that have a predilection for the buttocks, shoulders, and extensor surfaces of the limbs (Fig. 13.3).1 They may also present in the antecubital and popliteal fossae, axillae, lips, eyelids, and ears.2 They often appear in crops and may wax and wane with plasma lipoprotein levels.3 Lesions usually resolve spontaneously over a period of weeks. Pruritus is frequently present and the papules are sometimes tender.2 Eruptive xanthomata may rarely display a Koebner phenomenon.4,5 Healing is occasionally associated with the development of hyperpigmented scars.2 Cutaneous lesions of Langerhans cell histiocytosis and cutaneous involvement by adenocarcinoma may mimic eruptive xanthoma.6,7
Histologic features The histologic features are seen predominantly within the superficial reticular dermis. In early lesions histiocytes are numerous and the fully developed ‘foam cells’, which characterize xanthomata, are sometimes few in number. The infiltrate may also contain an admixture of lymphocytes and neutrophils.19,20 In an established papule, xanthoma cells with characteristic clear or foamy cytoplasm form the predominant cell type (Figs 13.4–13.6). Occasional cases show a palisading appearance at low magnification and urate-like crystals.13,21,22
Eruptive xanthomata are associated with hypertriglyceridemia and most often occur in hyperchylomicronemic states. Sometimes their presence correlates with increased levels of VLDL. The most common cause, however, is secondary hyperlipoproteinemia (HPL), especially in those cases associated with diabetes mellitus and alcohol ingestion, or in those that are drug induced (e.g., due to exogenous estrogens, corticosteroids or retinoids).2,8 They may also develop as a consequence of decreased lipoprotein lipase activity, ApoCII deficiency or increased synthesis of VLDL, which effectively blocks chylomicron access to lipoprotein lipase.2,9 Eruptive xanthomata are therefore often accompanied by other features of hyperlipidemia, including lipemia retinalis, hepatosplenomegaly, abdominal pain, and pancreatitis.
Eruptive xanthomata often develop rapidly over the course of several days and occasionally are associated with spontaneous resolution. The quantity of intracytoplasmic lipid (predominantly triglyceride in contrast to other xanthomata, which contain mostly cholesterol) is in a state of flux and may be associated with extracellular deposition, a phenomenon that is rare or absent in the other types of xanthomata. In all xanthomata the lipid within the macrophage stains positively with fat stains such as oil red O, scarlet or Sudan red (Fig. 13.7).
Differential diagnosis There can be confusion with granuloma annulare histologically as both conditions have certain features in common, namely a dermal interstitial histiocytic infiltrate with variably increased mucin.13,19,20 Although extracellular lipid may disrupt dermal collagen, necrobiosis is not characteristic of
563 The hyperlipidemias
eruptive xanthoma and palisading is not a feature of the latter. Additionally, it contains few giant cells and the perivascular infiltrate is histiocytic, in contrast to the perivascular lymphocytes seen in granuloma annulare.13 Cases of eruptive xanthoma with urate-like crystals have been misdiagnosed as gout.22 Immunohistochemical studies of these urate-like crystals suggest that they are, not surprisingly, composed of chylomicrons.23

Fig. 13.3 Eruptive xanthoma: numerous small yellow papules are present on the buttocks. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
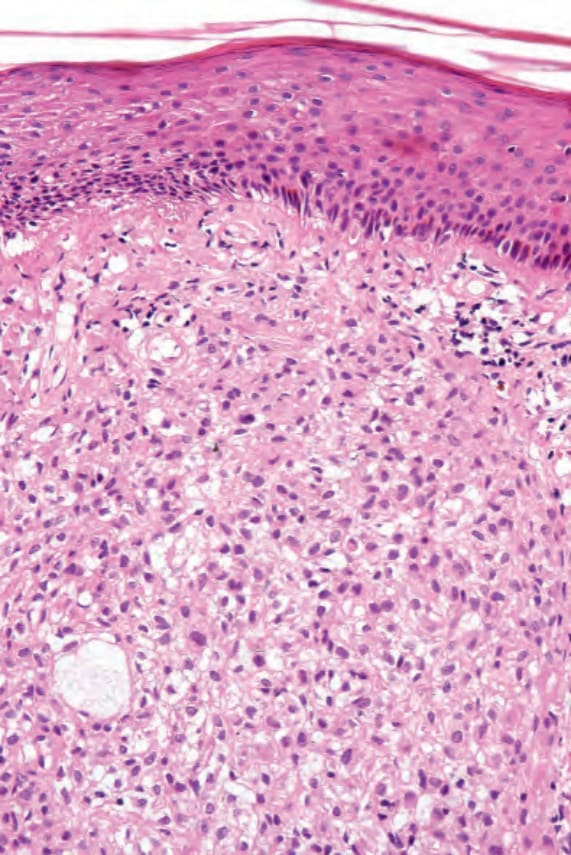
Fig. 13.4 Eruptive xanthoma: biopsy of an established lesion. The histiocytes have abundant vacuolated cytoplasm.
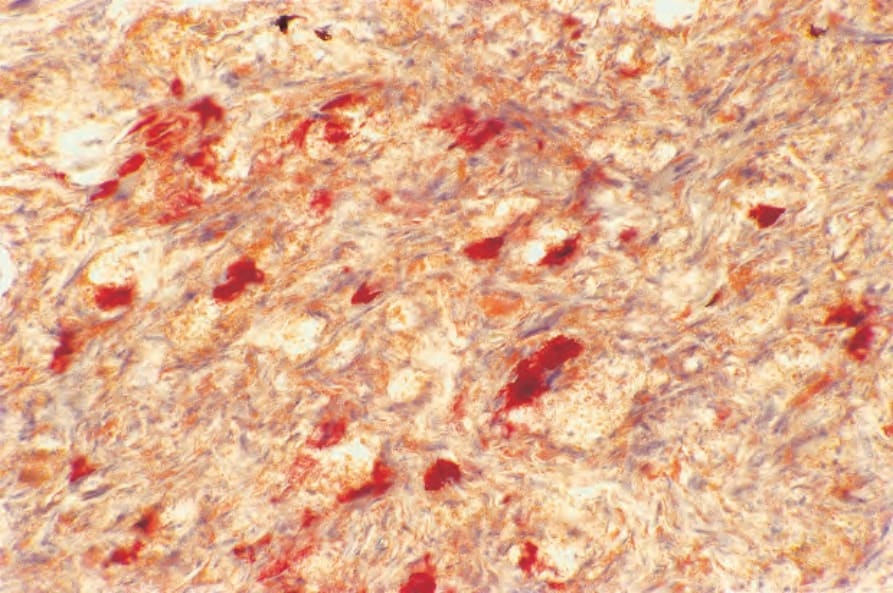
Fig. 13.7 Eruptive xanthoma: the lipid within the macrophages stains positively with oil red O.