Neurofibromatosis
神經纖維瘤病 (neurofibromatosis)
臨床特徵 (Clinical Features)
傳統上 neurofibromatosis 分類為:
- 經典周邊皮膚變異型 (classic peripheral cutaneous variant),或稱第一型神經纖維瘤病 (type I neurofibromatosis;NF1,von Recklinghausen disease;NF1 基因位於 17q11.2),
出生時即出現的 neurofibroma 常為叢狀 (plexiform),特別位於眼周與頸部;部分病灶呈全身性分布。26 至兒童晚期或青春期時,會發展出大量皮膚腫瘤,可呈結節狀 (nodular)、無蒂 (sessile) 或帶蒂 (pedunculated)(Figs 35.345–35.349)。NFI 的 neurofibroma 血管增生增加,此可導致明顯出血,尤其在手術切除大型 plexiform 變異型時。此血管增生增加可能源自腫瘤細胞表現 basic fibroblast growth factor 與 endothelial growth factor 升高。27
部分病例會在頭部、頸部與背部發現的瀰漫性 neurofibroma (diffuse neurofibroma) 亦與 neurofibromatosis 相關;
1795 Benign neural tumors
1796 Connective tissue tumors
Neurofibromatosis 亦可能與多種其他表現相關,包括身材矮小 (short stature)、嗜鉻細胞瘤 (pheochromocytoma)、胃腸道腫瘤(包括 adenocarcinoma、carcinoid、somatostatinoma 與 gastrointestinal stromal tumor)、智能不足 (mental retardation),以及各種中樞神經系統腫瘤(主要為 low-grade gliomas,但亦包括高惡性度腫瘤如 medulloblastoma)。11,12,29–33 兒童病例中亦已知與 juvenile xanthogranuloma 及白血病 (leukemia) 相關。34 已有少數 achondroplasia 與 NF1 併存的病例報告。35 另已記載多項其他關聯,但這些很可能屬於偶然併存,包括 cutaneous T-cell lymphoma、epidermodysplasia verruciformis、urticaria pigmentosa、piebaldism、eccrine angiomatous hamartoma、segmental unilateral lentiginosis 與 multiple glomus tumors。36–43
然而,與 plexiform 型不同,此型除少數罕見病例外,似乎不會伴隨惡性轉化風險增加(Figs 35.350 and 35.351)。
值得注意的是,NF1 患者正常皮膚的切片顯示 S100 protein 陽性細胞數目增加。28
偶爾,大型 plexiform neurofibroma 可伴隨過多冗餘的皮膚皺褶,形成所謂的象皮病樣神經纖維瘤 (elephantiasiform neurofibroma)(Fig. 35.352)。
Lisch nodules 為虹膜的色素性錯構瘤 (pigmented hamartomas of the iris),是 NF1 的特異性病徵 (pathognomonic)(Fig. 35.353)。12 然而,這些結節從未在聽神經型 (acoustic) 或節段型 (segmental) 變異中發現。
Neurofibromatosis 患者可在身體任何部位發展出腫瘤,包括內部神經幹 (internal nerve trunks) 與內臟 (viscera)(Figs 35.354 and 35.355)。由於這是一種進行性疾病,年齡增長會伴隨進一步結節的形成;最終患者可能呈現有時頗為怪異的外觀,並伴隨心理與社會問題。
然而,指(趾)部多發性血管球瘤 (multiple glomus tumors of the digits) 已被確認為 NF1 的一項重要關聯。44,45 與 Noonan syndrome 的關聯亦很常見,且兩種疾病在致病機轉上相關。46,47
近期一項研究發現,與 NF1 死亡率獨立相關的因子包括皮下 neurofibromas 的存在、皮膚 neurofibromas 的缺乏,以及顏面不對稱。48 與內部 neurofibromas 相關的獨立皮膚預測因子包括至少兩個皮下 neurofibromas 的存在、年齡等於或小於 30 歲、皮膚 neurofibromas 的缺乏,以及少於六個咖啡牛奶斑 (café-au-lait
1797 Benign neural tumors
spots)。49,50 基於後者,已有人提出一套評分系統以計算內部 neurofibromas 的風險。
NF1 患者的藍紅色斑 (blue–red macules) 與假萎縮性斑 (pseudoatrophic macules) 已被證實可指示 neurofibromas 的存在。51
NF1 的 plexiform neurofibromas 在懷孕期間可能增大,但腫瘤似乎不表現 progesterone receptors。52,53
如前所述,NF1 患者發展惡性周邊神經鞘瘤 (malignant peripheral nerve sheath tumors) 的風險增加,終生發生率介於 8% 與 13% 之間。54–59 NF1 患者較散發性惡性腫瘤患者傾向於在人生較早期發病。59 他們亦較散發性腫瘤患者傾向於在較短的間隔內出現復發與轉移擴散。60 疼痛與腫大是提示惡性轉化的最常見徵象。大多數病灶發生於四肢;這些是高度侵襲性的腫瘤,患者的平均存活期為 18 個月。已發現腫瘤體積與 TP53 表現是預測不良行為的獨立因子。61,62 透過小鼠模型 (murine models) 的運用,已證實 tumor suppressor PTEN (phosphatase and tensin homolog) 的缺失合併 KRAS oncogene 的過度表現,在惡性轉化的發展中至關重要。63,64
黑色素細胞分化 (melanocytic differentiation) 在極例外的情況下曾被記載。65
聽神經型神經纖維瘤病 (Acoustic neurofibromatosis,NF2) 構成一個症候群,包含聽神經瘤 (acoustic neuroma;schwannoma;見 Fig. 35.277),常為雙側,以及顱內與脊髓內腫瘤,包括 astrocytomas、meningiomas 與 ependymomas。曾有與軟組織 perineurioma 併存的例外病例報告。66 NF2 的基因已被選殖至第 22 號染色體 (chromosome 22)。67,68
節段型神經纖維瘤病 (Segmental neurofibromatosis) 因體細胞鑲嵌 (somatic mosaicism) 而可發生於 NF1 與 NF2。69–74 Segmental neurofibromatosis 可發生於經典 NF1 患者,或更常見地發生於除咖啡牛奶斑 (café-au-lait spots) 外無其他 neurofibromatosis 徵象的患者。大多數 segmental neurofibromatosis 病例無陽性家族史。75,76 侵犯通常為單側,但亦可為雙側。74
1798 Connective tissue tumors
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
第一型神經纖維瘤病 (neurofibromatosis type 1) 源自 NF1 基因的基因突變。NF1 基因位於第 17q11.2 號染色體,編碼蛋白質 neurofibromin。涉及腫瘤生成的分子機轉大多仍未明;NF1 基因的大量突變已被研究。第二型神經纖維瘤病 (neurofibromatosis type 2) 由 NF2 基因 (22q12.2) 的功能喪失所驅動,該基因編碼蛋白質 merlin(亦見 schwannoma)。77–91
Neurofibromatosis 中所見皮膚與皮下腫瘤的組織學表現,已在前述各標題下描述過。曾有一名 NF1 患者報告 pacinian corpuscles 肥大。92 約五分之一的病例可見細胞數增加 (increased cellularity) 與細胞學異型性 (cytologic atypia),此可能代表惡性轉化風險增加的指標。93 雖然曾有報告指出花瓣狀巨細胞 (floret-like giant cells) 與 neurofibromatosis type 1 的腫瘤相關,但這些細胞亦可在散發性 neurofibromas 中辨識出來。94,95 Malignant peripheral nerve sheath tumors 較散發性腫瘤傾向於細胞數較多,但多形性 (pleomorphic) 較少。60
咖啡牛奶斑 (café-au-lait macules) 顯示功能活躍的黑色素細胞 (melanocytes) 數目增加,並帶有巨大黑色素體 (giant melanosomes)。
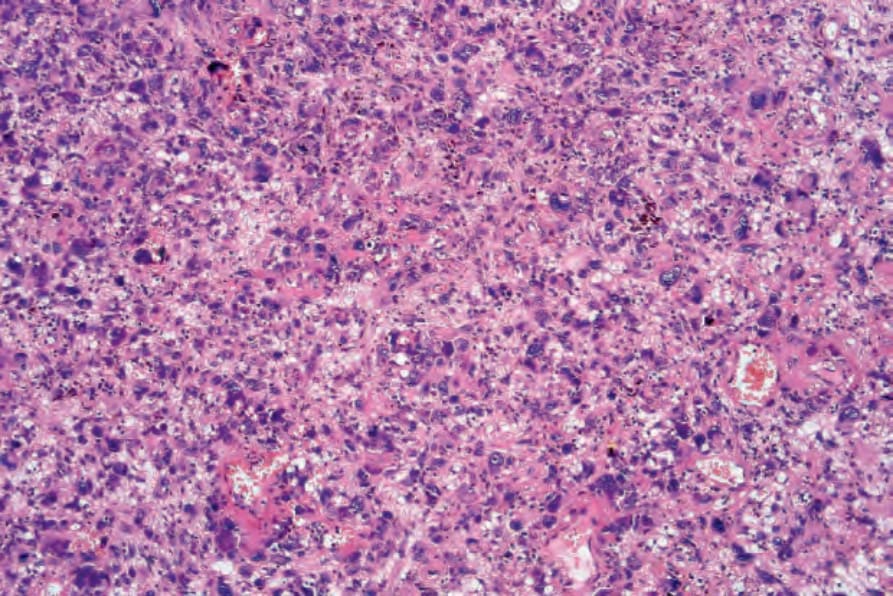
圖 35-277:非典型纖維黃色瘤 (atypical fibroxanthoma):中倍視野顯示高度富細胞且多形性的腫瘤細胞浸潤 (highly cellular and pleomorphic tumor cell infiltrate)。
Fig. 35.277 Atypical fibroxanthoma: medium-power view showing a highly cellular and pleomorphic tumor cell infiltrate.

圖 35-343:第一型神經纖維瘤病 (type I neurofibromatosis):典型咖啡牛奶斑 (café-au-lait macules) 的存在為其特徵。By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Fig. 35.343 Type I neurofibromatosis: the presence of typical café-au-lait macules is characteristic. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 35-344:第一型神經纖維瘤病 (type I neurofibromatosis):此重度色素沉著的隆起病灶覆蓋於一個皮膚 plexiform neurofibroma 之上。By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Fig. 35.344 Type I neurofibromatosis: this heavily pigmented raised lesion overlies a cutaneous plexiform neurofibroma. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
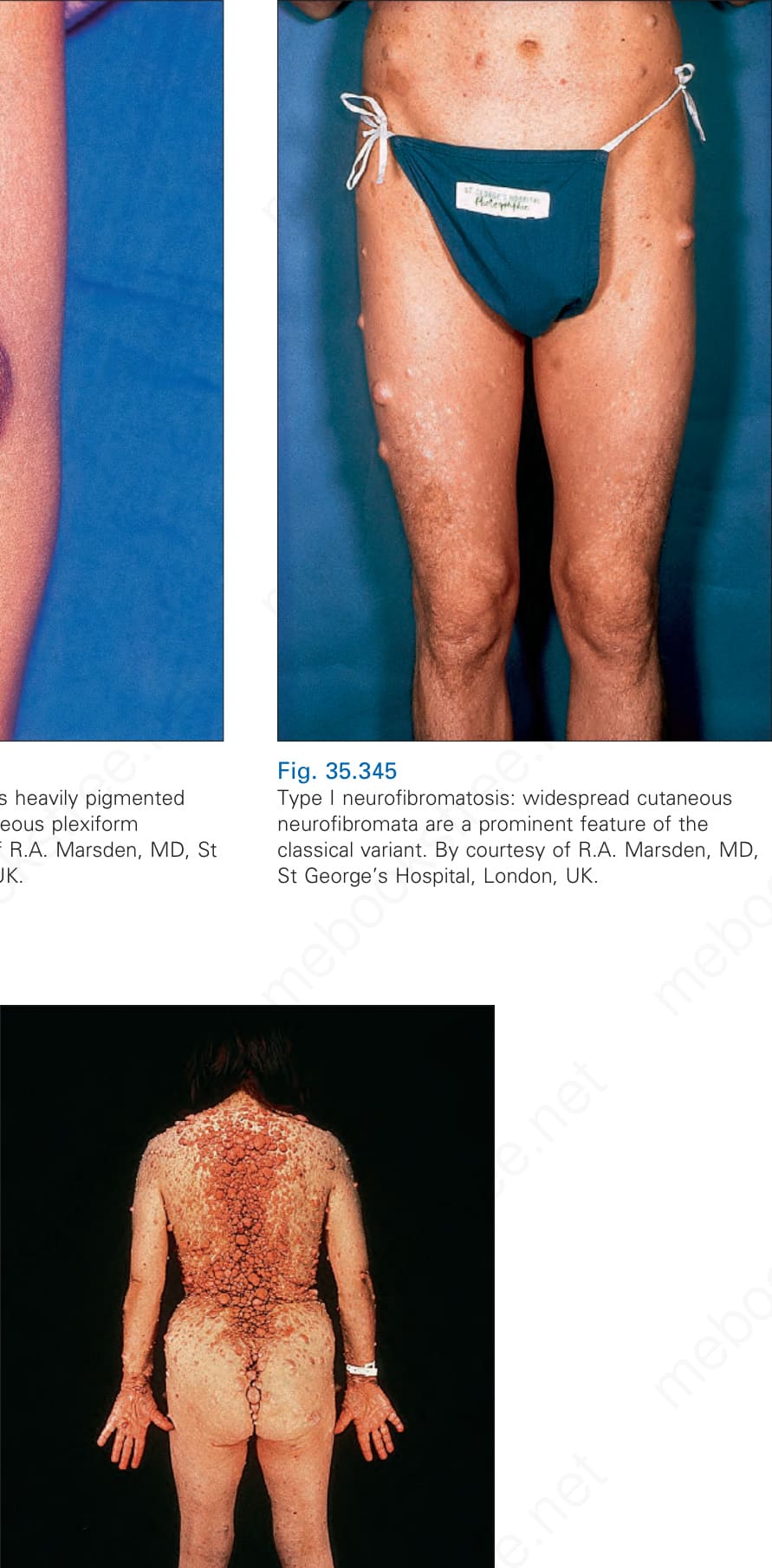
圖 35-345:第一型神經纖維瘤病 (type I neurofibromatosis):廣泛分布的皮膚 neurofibromata 是經典變異型的顯著特徵。By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Fig. 35.345 Type I neurofibromatosis: widespread cutaneous neurofibromata are a prominent feature of the classical variant. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 35-346:第一型神經纖維瘤病 (type 1 neurofibromatosis):病灶常為柔軟,呈息肉狀 (polypoid) 或無蒂 (sessile) 的丘疹與斑塊。By courtesy of the Institute of Dermatology, London, UK.
Fig. 35.346 Type 1 neurofibromatosis: lesions are often soft and appear as polypoid or sessile papules and plaques. By courtesy of the Institute of Dermatology, London, UK.
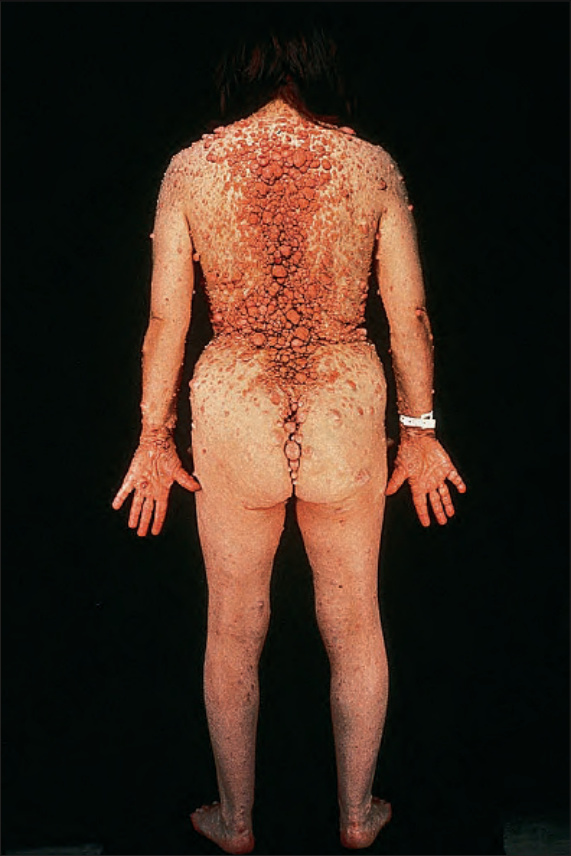
圖 35-347:第一型神經纖維瘤病 (type I neurofibromatosis):此疾病可造成極度毀容。By courtesy of the Institute of Dermatology, London, UK.
Fig. 35.347 Type I neurofibromatosis: this disease can be extremely disfiguring. By courtesy of the Institute of Dermatology, London, UK.

圖 35-348:第一型神經纖維瘤病 (type 1 neurofibromatosis):近距離視野。By courtesy of the Institute of Dermatology, London, UK.
Fig. 35.348 Type 1 neurofibromatosis: close-up view. By courtesy of the Institute of Dermatology, London, UK.

圖 35-349:第一型神經纖維瘤病 (type 1 neurofibromatosis):有顯著的顏面毀容。By courtesy of the Institute of Dermatology, London, UK.
Fig. 35.349 Type 1 neurofibromatosis: there is marked facial disfigurement. By courtesy of the Institute of Dermatology, London, UK.

圖 35-350:第一型神經纖維瘤病 (type I neurofibromatosis):真皮與皮下脂肪被均質的淡黃色腫瘤廣泛取代——一個瀰漫性 neurofibroma (diffuse neurofibroma)。
Fig. 35.350 Type I neurofibromatosis: there is extensive replacement of dermis and subcutaneous fat by a homogeneous pale yellow tumor – a diffuse neurofibroma.

圖 35-351:第一型神經纖維瘤病 (type 1 neurofibromatosis):覆蓋於腫瘤之上的皮膚呈現皺褶、不均勻隆起的外觀。
Fig. 35.351 Type 1 neurofibromatosis: the skin overlying the tumor has a wrinkled, unevenly elevated appearance.

圖 35-352:第一型神經纖維瘤病 (type I neurofibromatosis):象皮病樣變異型 (elephantiasiform variant)。By courtesy of D. Allen, MD, St Thomas’ Hospital, London, UK.
Fig. 35.352 Type I neurofibromatosis: the elephantiasiform variant. By courtesy of D. Allen, MD, St Thomas’ Hospital, London, UK.
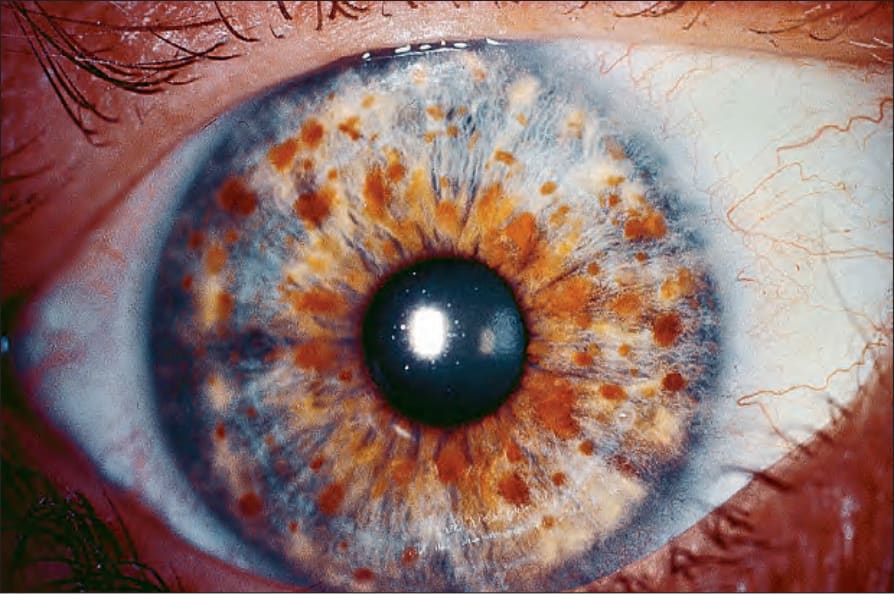
圖 35-353:第一型神經纖維瘤病 (type I neurofibromatosis):多發性 Lisch nodules(虹膜痣 iris nevi)是一項特異性病徵 (pathognomonic feature)。By courtesy of D. Spalton, MD, St Thomas’ Hospital, London, UK.
Fig. 35.353 Type I neurofibromatosis: multiple Lisch nodules (iris nevi) are a pathognomonic feature. By courtesy of D. Spalton, MD, St Thomas’ Hospital, London, UK.
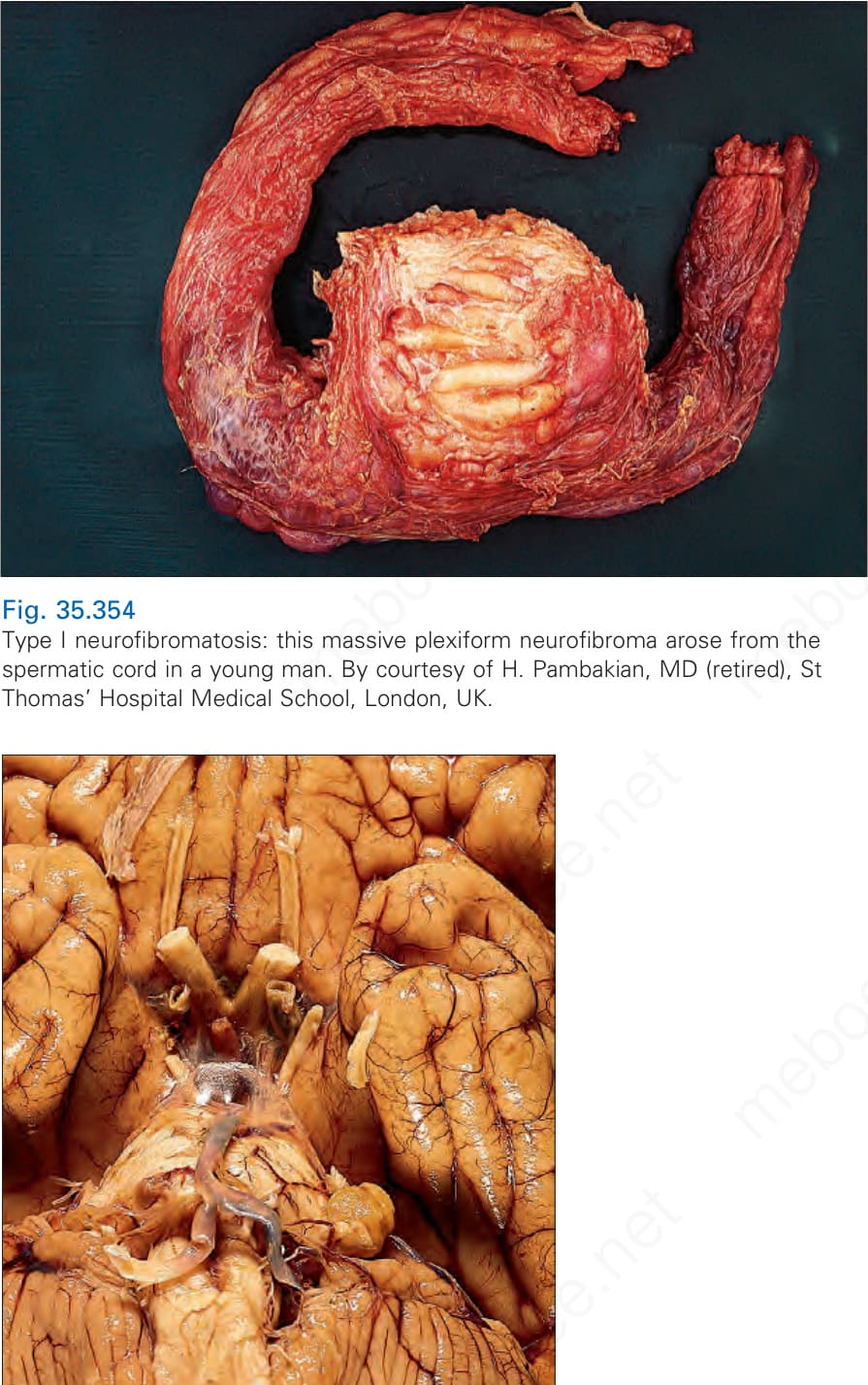
圖 35-354:第一型神經纖維瘤病 (type I neurofibromatosis):此巨大的 plexiform neurofibroma 發生於一名年輕男性的精索 (spermatic cord)。By courtesy of H. Pambakian, MD (retired), St Thomas’ Hospital Medical School, London, UK.
Fig. 35.354 Type I neurofibromatosis: this massive plexiform neurofibroma arose from the spermatic cord in a young man. By courtesy of H. Pambakian, MD (retired), St Thomas’ Hospital Medical School, London, UK.

圖 35-355:第一型神經纖維瘤病 (type I neurofibromatosis):左側第八對顱神經 (eighth cranial nerve) 的典型聽神經瘤 (acoustic neuroma) 可見於小腦橋腦角 (cerebellopontine angle)。
Fig. 35.355 Type I neurofibromatosis: a typical acoustic neuroma of the left eighth cranial nerve is visible in the cerebellopontine angle.