細胞性神經鞘黏液瘤 (Cellular Neurothekeoma)
臨床特徵 (Clinical Features)
- 細胞性神經鞘黏液瘤 (cellular neurothekeoma) 通常出現在兒童與年輕成人的頭部、頸部與上肢,其次為軀幹,並好發於女性。老年患者的腫瘤罕見。
- 不尋常的發生部位包括上頜骨 (maxilla)、球結膜 (bulbar conjunctiva)、口腔、唇、眼瞼、下咽 (hypopharynx)、耳與外陰 (vulva)。
- 病灶為長期存在、膚色的丘疹,通常直徑小於 1 cm,多數情況下小於 2 cm。多發病灶與爆發性 (eruptive) 病例極為例外。曾有一例發生於 Guillain-Barre 患者。
- 局部復發少見,大型系列研究中報告約 7% 的數字可能反映了轉診偏差 (referral bias)。復發性腫瘤在臉部較常見。
- 部分病例呈現非典型特徵 (見下文),引發惡性的可能性。然而這些腫瘤的行為屬良性。
- 近期描述了 perineurioma 與細胞性「neurothekeoma」的混合性腫瘤 (hybrid tumors)(見下文);絕大多數以唇部單發丘疹的形式出現。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
- 細胞性神經鞘黏液瘤已不再被視為神經來源 (neural lineage) 的腫瘤。其起源仍不明,雖然曾有人提出與叢狀纖維組織細胞瘤 (plexiform fibrohistiocytic tumor) 的關聯,但此說法可能性不大。
- 病灶界線不清,位於網狀真皮 (reticular dermis),常局部延伸至皮下組織。非典型變異型 (見下文) 更深入皮下組織,並曾記錄一例純皮下表現的例外案例。臉部腫瘤可局部侵犯骨骼肌。
- 腫瘤呈分葉狀生長型態 (lobular growth pattern),由上皮樣 (epithelioid) 與短梭形細胞 (short spindled cells) 構成的小巢 (nests) 與束 (fascicles) 組成,這些細胞具有淡嗜伊紅性細胞質 (pale eosinophilic cytoplasm)、囊泡狀核 (vesicular nuclei) 以及輕微或無細胞學異型性 (cytologic atypia)(Figs 35.252 and 35.253)。
- 較明顯的細胞學異型性可見於高達 25% 的病例。正常的有絲分裂相 (mitotic figures) 相當常見,部分病例中相當明顯,而在例外的情況下可見非典型有絲分裂相 (atypical mitotic figures)(Fig. 35.254)。
- 可見多核巨細胞 (multinucleated giant cells),包括破骨細胞樣巨細胞 (osteoclast-like giant cells)。腫瘤細胞周圍的膠原 (collagen) 有時顯得略呈硬化 (sclerotic)。在某些病例中,後者的變化相當明顯,這類病灶被視為硬纖維性 (desmoplastic)。
- 以叢狀型態 (plexiform pattern) 為主者極為罕見,偶有病例可見較大的小葉 (lobules)。束狀 (fascicular) 與片狀 (sheet-like) 型態屬例外。黏液樣變化 (myxoid change) 經常被觀察到,傾向局部出現,較少為主要表現。曾記錄兩例含黑色素 (melanin) 的罕見腫瘤。
- 非典型細胞性神經鞘黏液瘤 (atypical cellular neurothekeoma) 的特徵為較大的體積、深部侵犯、浸潤性生長型態 (infiltrative growth pattern)、血管侵犯 (vascular invasion)、神經周圍侵犯 (perineural invasion)、高有絲分裂率以及顯著的細胞學異型性(Figs 35.255 and 35.256)。可見淋巴球套狀浸潤 (lymphocytic cuffing)、黃色瘤樣區域 (xanthomatoid areas)、假痣樣外觀 (pseudonevoid appearance) 與軟骨樣間質 (chondroid stroma)。亦曾報告一例具神經內分泌分化 (neuroendocrine differentiation) 的病例。
- 此腫瘤的組織發生 (histogenesis) 仍是個謎。曾有人提出其分化線屬纖維母細胞性/肌纖維母細胞性 (fibroblastic/myofibroblastic),並可能代表叢狀纖維組織細胞瘤 (plexiform fibrous histiocytoma) 譜系的一部分。
免疫組化 (Immunohistochemistry)
- 免疫組化相當具特徵性,病例一致為 S100 protein 與 SOX10 陰性,而 NSE、NKI/C3(最初描述為黑色素瘤標記,且為非常非特異性的標記)與 CD10 陽性(Fig. 35.257)。
- 雖然曾有報告指出 NKI/C3 在以梭形細胞為主的腫瘤中傾向陰性,但這並非我們個人的經驗。雖然 S100 protein 為陰性,S100A6 在所有已報告的病例中皆為陽性。
- 一部分病例對 SMA 呈局部陽性。PGP 9.5、microphthalmia transcription factor 1 (MITF-1) 與 podoplanin (D2–40) 也被報告為細胞性神經鞘黏液瘤的有用標記。曾有單一病例對 desmin 呈陽性。
- 具有 perineurioma 與細胞性神經鞘黏液瘤特徵的混合性腫瘤為界線清楚、無包膜的叢狀病灶 (unencapsulated plexiform lesions),由位於局部黏液樣間質 (focally myxoid stroma) 中的腫瘤細胞巢/結節 (nests/nodules) 組成。個別腫瘤細胞排列成漩渦狀 (whorls) 或層板狀型態 (lamellar pattern)。免疫組化上,多數細胞對 S100A6、MITF1、NKI/C3、PGP9.5、EMA 與 NSE 有強烈免疫反應。某些病例中,對 CD34、claudin-1 與 Glut-1 有較弱且局部的陽性。亦曾報告一例雙相非叢狀混合性腫瘤 (biphasic non-plexiform hybrid tumor)。
鑑別診斷 (Differential Diagnosis)
- 雖然整體呈巢狀的生長型態略似黑色素細胞病灶 (melanocytic lesion),但並無表皮成分,且病灶對 S100 protein、HMB-45 與 Melan-A 皆為陰性。
- 神經鞘黏液瘤 (nerve sheath myxoma) 主要為肢端 (acral) 腫瘤,缺乏細胞性區域,由星狀細胞 (stellate cells) 的黏液樣小葉 (myxoid lobules) 組成,這些細胞對 S100 protein 陽性、對 NKI/C3 陰性。
- 當鑑別診斷考慮叢狀纖維組織細胞瘤 (plexiform fibrohistiocytic tumor) 時,MITF1 陽性可能有所幫助。PG9.5 並非有用的標記,因其特異性非常低。
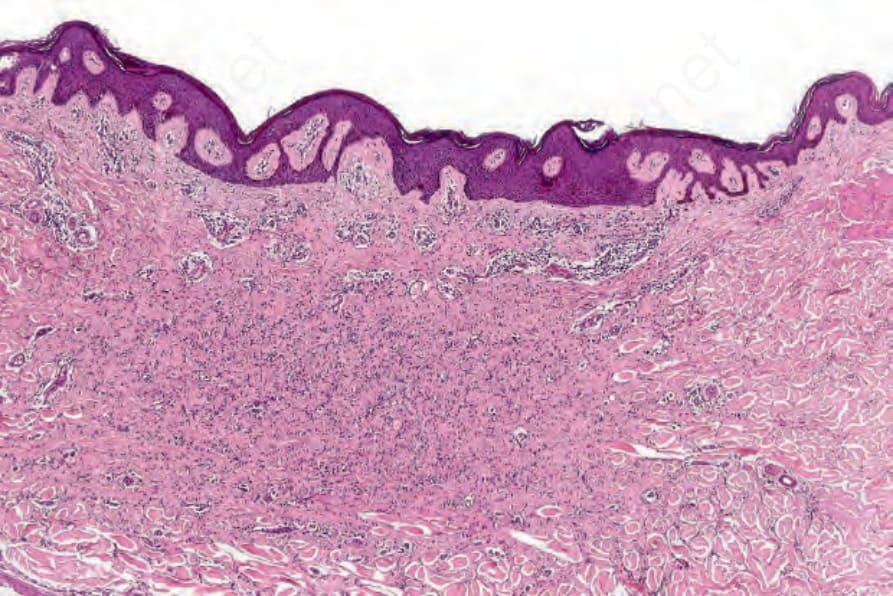
圖 35-250:萎縮性纖維組織細胞瘤 (atrophic fibrous histiocytoma):此變異型呈現低細胞密度 (hypocellular),並與表面上皮平行排列。
Fig. 35.250 Atrophic fibrous histiocytoma: this variant appears hypocellular and orientated parallel to the surface epithelium.
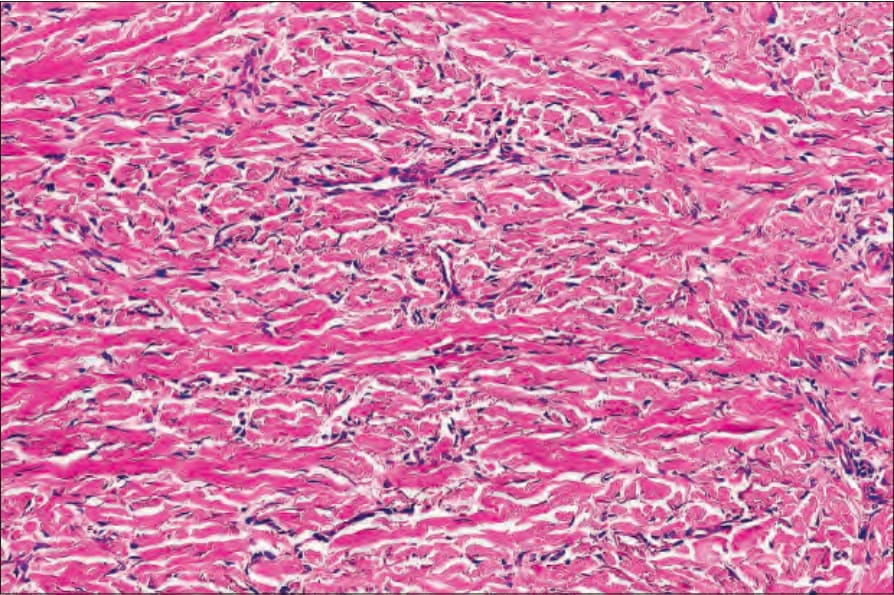
圖 35-251:萎縮性纖維組織細胞瘤 (atrophic fibrous histiocytoma):腫瘤細胞受膠原成分 (collagenous component) 壓迫。
Fig. 35.251 Atrophic fibrous histiocytoma: the tumor cells are compressed by the collagenous component.
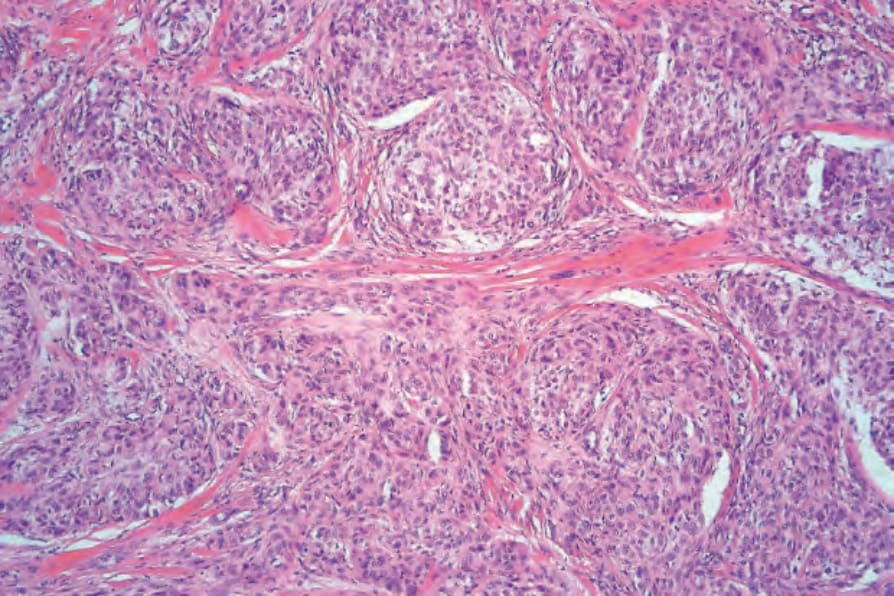
圖 35-252:細胞性神經鞘黏液瘤 (cellular neurothekeoma):腫瘤由嗜伊紅性細胞 (eosinophilic cells) 的巢與束組成。
Fig. 35.252 Cellular neurothekeoma: the tumor consists of nests and fascicles of eosinophilic cells.
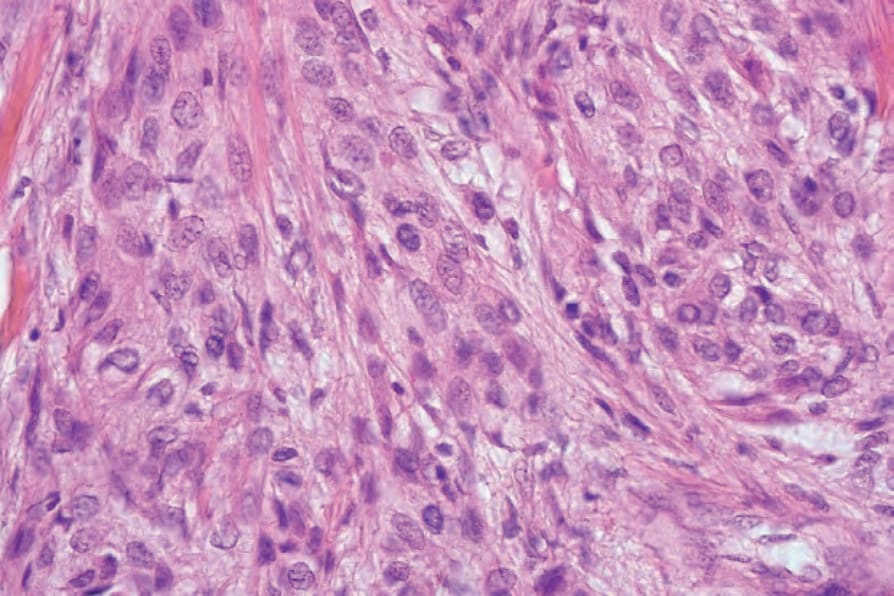
圖 35-253:細胞性神經鞘黏液瘤 (cellular neurothekeoma):細胞具有豐富的細胞質與囊泡狀核 (vesicular nuclei)。
Fig. 35.253 Cellular neurothekeoma: the cells have abundant cytoplasm and vesicular nuclei.
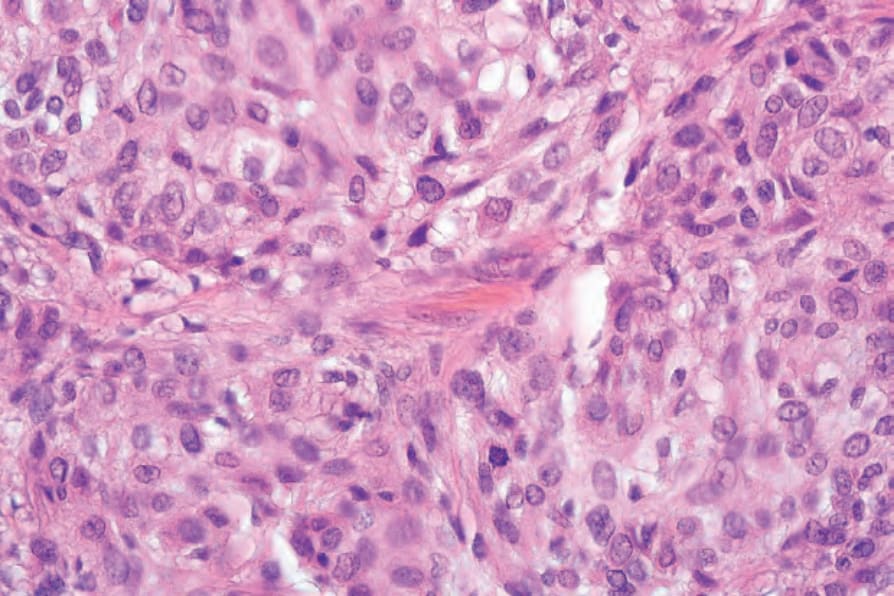
圖 35-254:細胞性神經鞘黏液瘤 (cellular neurothekeoma):有時可見有絲分裂相 (mitoses)。
Fig. 35.254 Cellular neurothekeoma: mitoses are sometimes present.
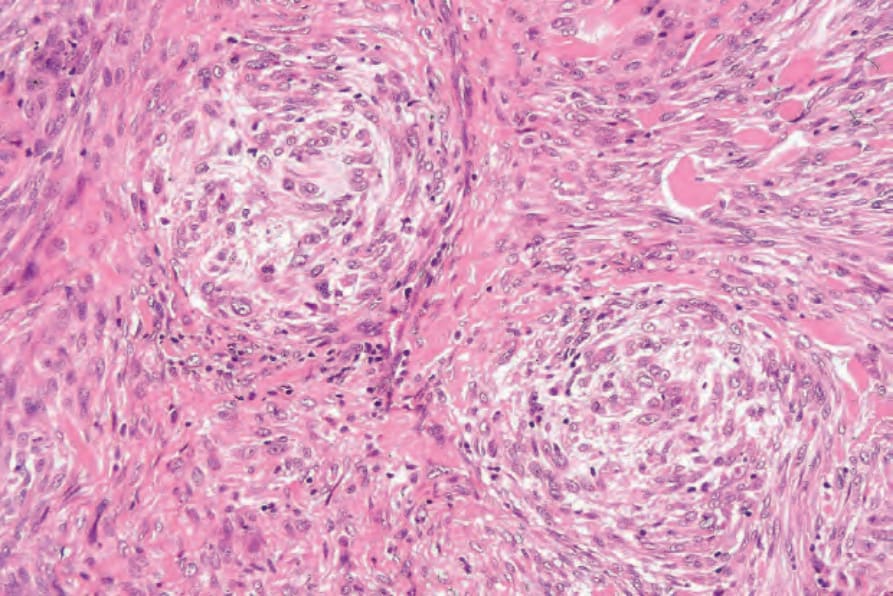
圖 35-255:非典型細胞性神經鞘黏液瘤 (atypical cellular neurothekeoma):腫瘤細胞大小不一,並有細胞學異型性 (cytologic atypia)。
Fig. 35.255 Atypical cellular neurothekeoma: tumor cells show variation in size and there is cytologic atypia.
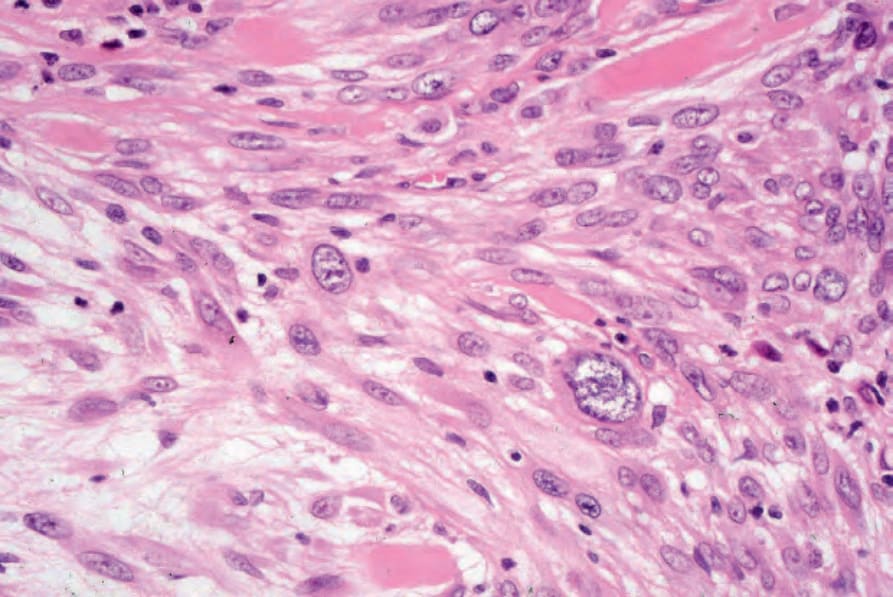
圖 35-256:非典型細胞性神經鞘黏液瘤 (atypical cellular neurothekeoma):高倍視野下,注意明顯的核多型性 (nuclear pleomorphism)。
Fig. 35.256 Atypical cellular neurothekeoma: at higher power, note the marked nuclear pleomorphism.
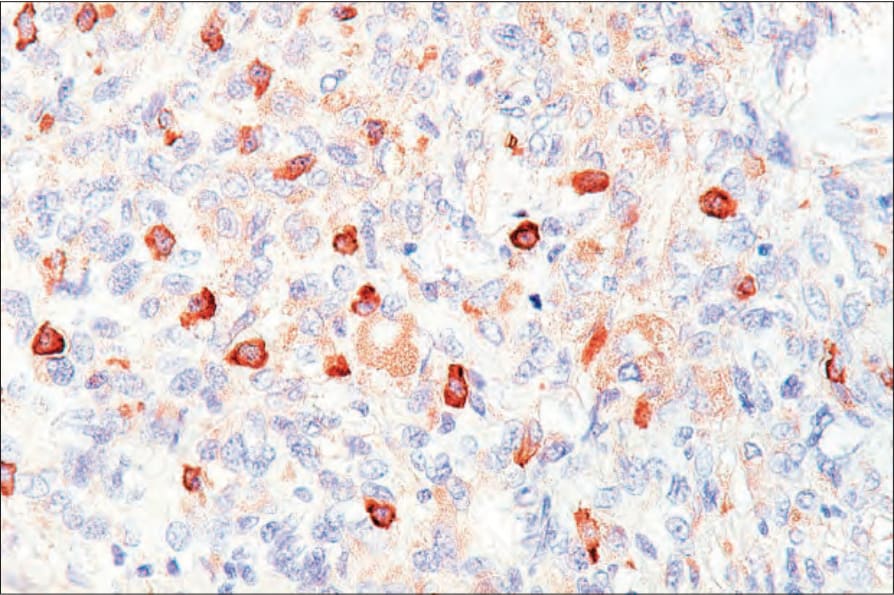
圖 35-257:細胞性神經鞘黏液瘤 (cellular neurothekeoma):腫瘤細胞表現 NKI-C3,但 S100 protein 陰性。
Fig. 35.257 Cellular neurothekeoma: the tumor cells express NKI-C3 but are S100 protein negative.
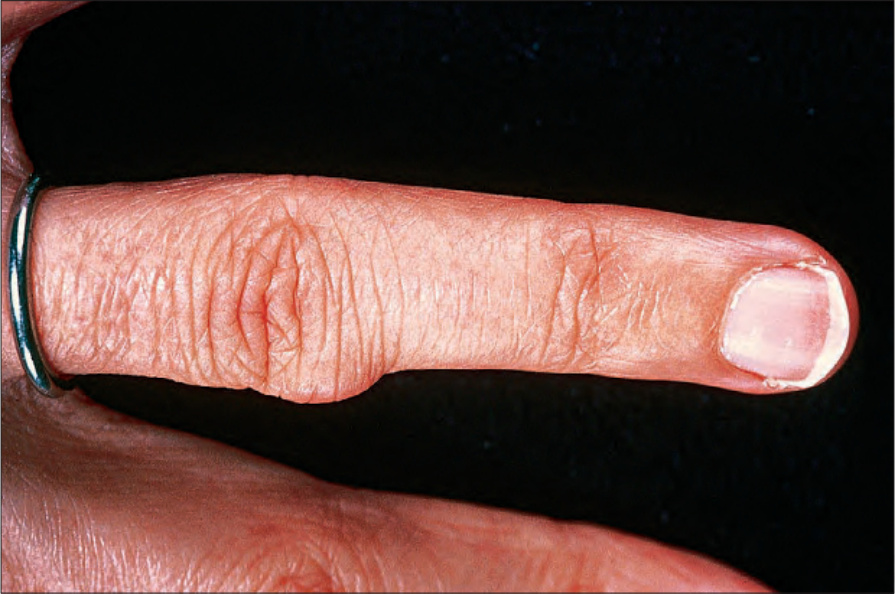
圖 35-258:腱鞘巨細胞瘤 (giant cell tumor of tendon sheath):此病灶表現為堅實的結節,最常侵犯手指。By courtesy of H. du P. Menagé, MD, Institute of Dermatology, London, UK.
Fig. 35.258 Giant cell tumor of tendon sheath: this lesion presents as a firm nodule that most often affects the finger. By courtesy of H. du P. Menagé, MD, Institute of Dermatology, London, UK.