Cellular neurothekeoma
Cellular neurothekeoma
Clinical features Cellular neurothekeoma usually presents on the head, neck and upper limbs followed by the trunk of children and young adults and shows predilection for females.1–8 Tumors in elderly patients are rare.9 Unusual sites of presentation include the maxilla, the bulbar conjunctiva, the oral cavity, the lip, the eyelid, hypopharynx, the ear and the vulva.10–20 Lesions are long-standing skin-colored papules, which usually measure less than 1 cm and in most cases less than 2 cm in diameter. Multiple lesions and eruptive cases are exceptional.8,21,22 A case in a patient with Guillain-Barre has been reported.23 Local recurrence is rare and the figure of around 7% reported in large series likely reflects a referral bias.7,8,24 Recurrent tumors are more common on the face.7,24 Some cases present with atypical features (see below), raising the possibility of malignancy.25–29 However, the behavior of these tumors is benign.
Hybrid tumors of perineurioma and cellular ‘neurothekeoma’ have been recently described (see below); the vast majority occur as a solitary papule on the lip.30–33
Pathogenesis and histologic features Cellular neurothekeoma is no longer considered a tumor of neural lineage. Its origin remains obscure and although an association with plexiform fibrohistiocytic tumor has been proposed, this is not likely.34
Lesions are poorly circumscribed and located in the reticular dermis with frequent focal extension into the subcutis. Atypical variants (see below) extend deeper into the subcutaneous tissue and an exceptional example with purely subcutaneous presentation has been documented.35 Facial tumors can focally involve the skeletal muscle. The tumor has a lobular growth pattern and consists of small nests and fascicles of epithelioid and short spindled cells with pale eosinophilic cytoplasm, vesicular nuclei and mild or no cytologic atypia (Figs 35.252 and 35.253). More prominent cytologic
1770 Connective tissue tumors
atypia can be seen in up to 25% of cases.7 Normal mitotic figures are fairly common and in some cases are prominent, and in exceptional instances atypical mitotic figures are found (Fig. 35.254).8 Multinucleated giant cells including osteoclast-like giant cells can be seen. The collagen around the tumor cells sometimes appears somewhat sclerotic. In some cases, the latter change is prominent and these lesions are regarded as desmoplastic.36–38 A predominantly plexiform pattern is very rare and in occasional cases larger lobules are identified.7,39 A fascicular and a sheet-like pattern is exceptional.28,40 Myxoid change is frequently observed and tends to be focal or more rarely predominant.7,29,41,42 Two rare tumors containing melanin have been documented.43
(Fig. 35.257).7,8,48 Although it has been reported that NKI/C3 tends to be negative in tumors in which spindle cells predominate this is not our personal experience.49 Although S100 protein is negative, S100A6 is positive in all reported cases.50 A proportion of cases are focally positive for SMA.2 PGP 9.5, microphthalmia transcription factor 1 (MITF-1) and podoplanin (D2–40) have also been reported as useful markers of cellular neurothekeoma.49,51,52 A single case was positive for desmin.7
Atypical cellular neurothekeoma is characterized by larger size, deep involvement, infiltrative growth pattern, vascular invasion, perineural invasion, high mitotic rate and marked cytologic atypia (Figs 35.255 and 35.256).7,25,28,44 Lymphocytic cuffing, xanthomatoid areas, a pseudonevoid appearance and chondroid stroma may be seen.28 A case with neuroendocrine differentiation has also been reported.45
The histogenesis of this tumor remains enigmatic.2–5 It has been suggested that the line of differentiation is fibroblastic/myofibroblastic and that it may represent part of the spectrum of plexiform fibrous histiocytoma.7,46,47 Immunohistochemistry is quite distinctive, as cases are consistently S100 protein and SOX10 negative and NSE, NKI/C3 (described originally as a melanoma marker and a very non-specific marker) and CD10 positive
Hybrid tumors with features of perineurioma and cellular neurothekeoma are well-circumscribed, unencapsulated plexiform lesions composed of nests/nodules of tumor cells in a focally myxoid stroma.30 Individual tumor cells are arranged in whorls or in a lamellar pattern. By immunohistochemistry most cells are strongly immunoreactive for S100A6, MITF1, NKI/C3, PGP9.5, EMA, and NSE. In some cases, there is weaker and focal positivity for CD34, claudin-1, and Glut-1. A biphasic non-plexiform hybrid tumor has also been reported.32
Differential diagnosis Although the overall growth pattern with nesting somewhat resembles a melanocytic lesion, there is no epidermal component and lesions are S100 protein, HMB-45 and Melan-A negative. Nerve sheath myxoma is a predominantly acral tumor lacking cellular areas and composed of myxoid
1771 Benign fibrohistiocytic tumors and tumorlike lesions
lobules of stellate cells which are positive for S100 protein and negative for NKI/C3.53 MITF1 positivity may be of help when a plexiform fibrohistiocytic tumor is considered in the differential diagnosis.54 PG9.5 is not a helpful marker as it has very low specificity.55
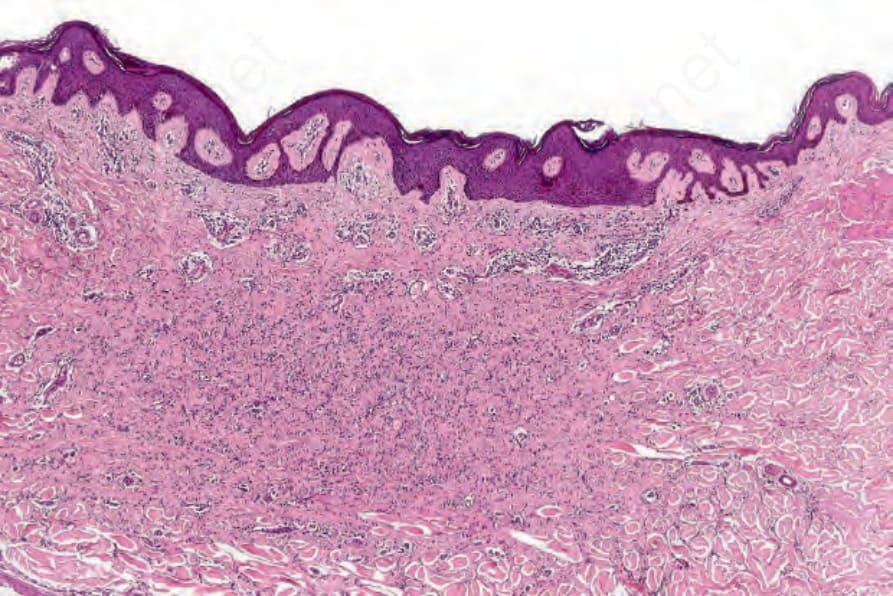
Fig. 35.250 Atrophic fibrous histiocytoma: this variant appears hypocellular and orientated parallel to the surface epithelium.
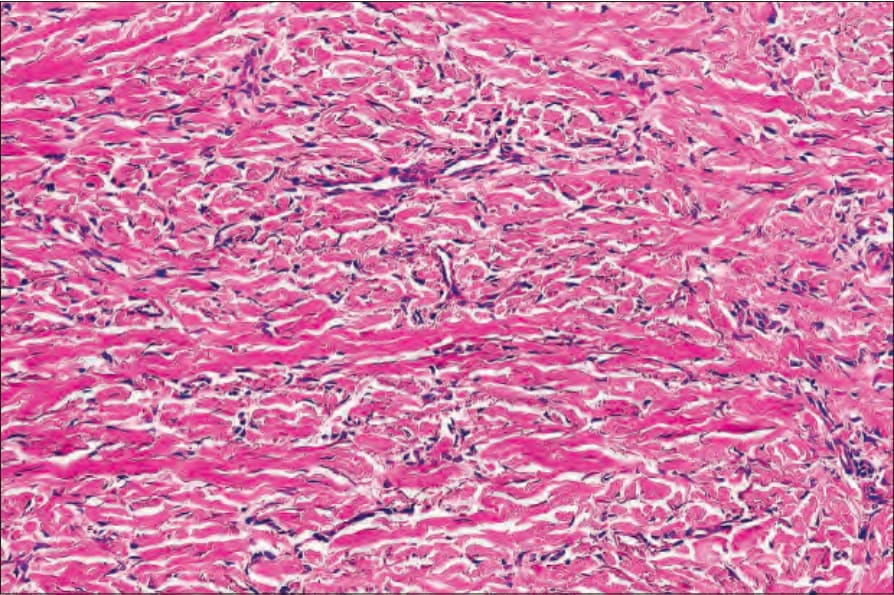
Fig. 35.251 Atrophic fibrous histiocytoma: the tumor cells are compressed by the collagenous component.
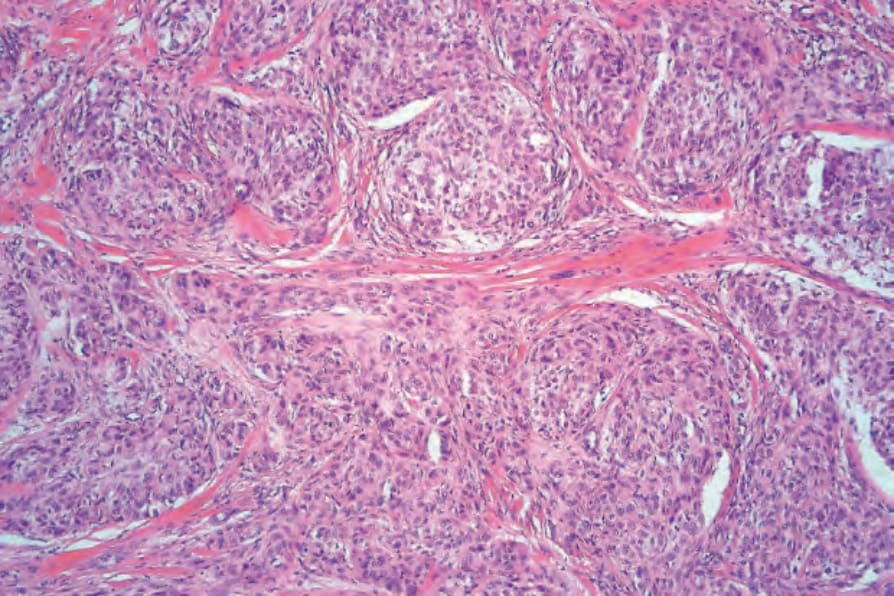
Fig. 35.252 Cellular neurothekeoma: the tumor consists of nests and fascicles of eosinophilic cells.
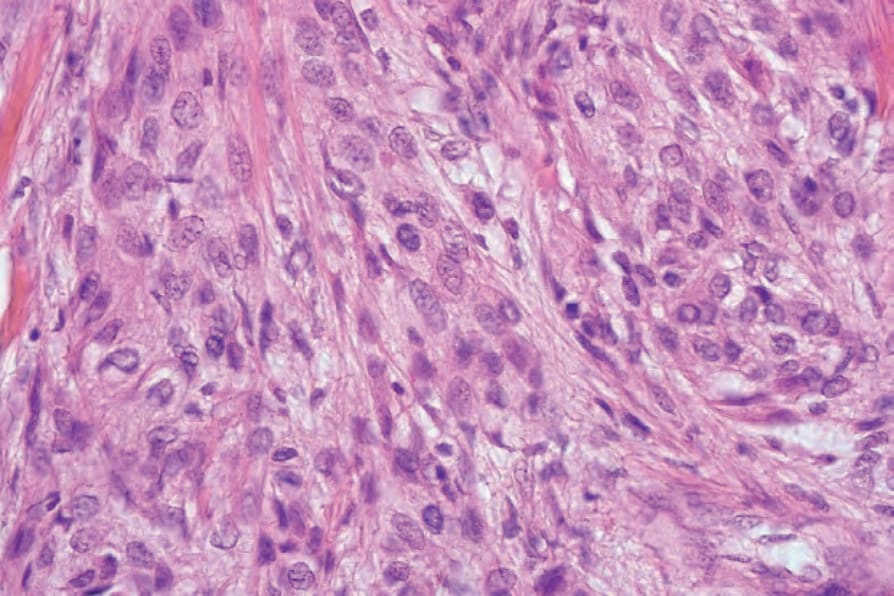
Fig. 35.253 Cellular neurothekeoma: the cells have abundant cytoplasm and vesicular nuclei.
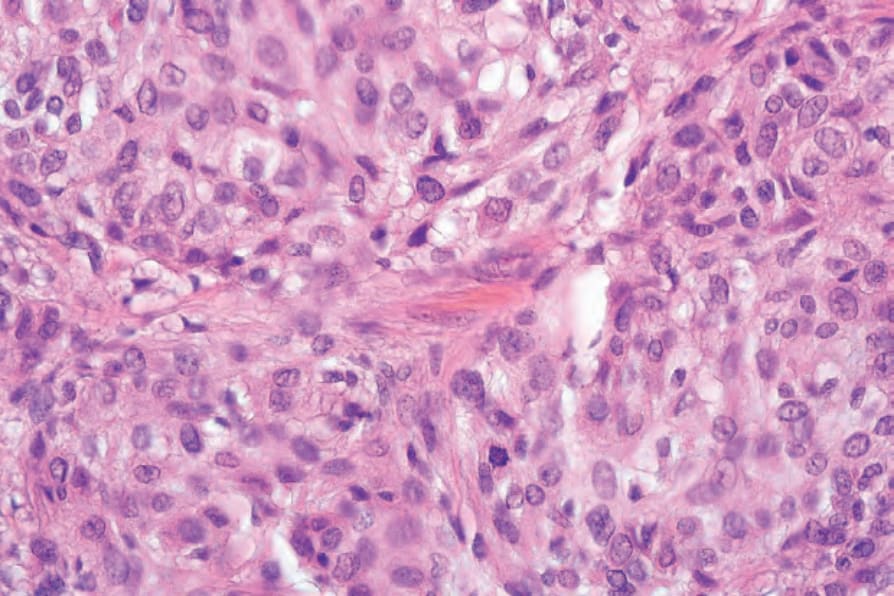
Fig. 35.254 Cellular neurothekeoma: mitoses are sometimes present.
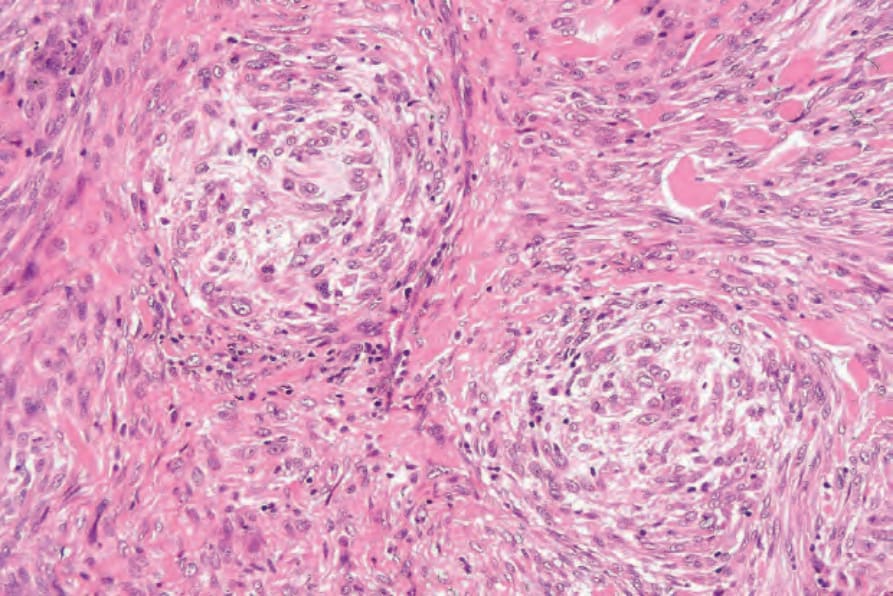
Fig. 35.255 Atypical cellular neurothekeoma: tumor cells show variation in size and there is cytologic atypia.
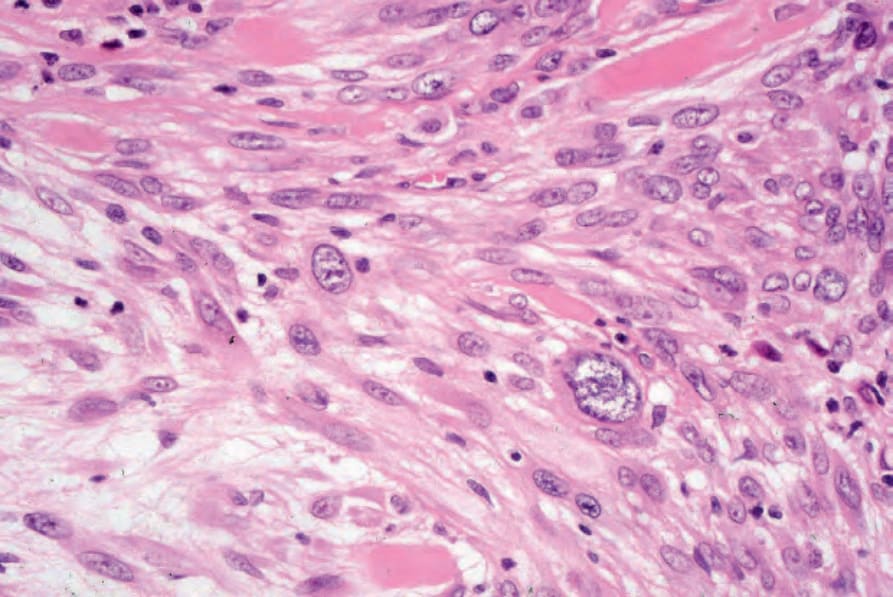
Fig. 35.256 Atypical cellular neurothekeoma: at higher power, note the marked nuclear pleomorphism.
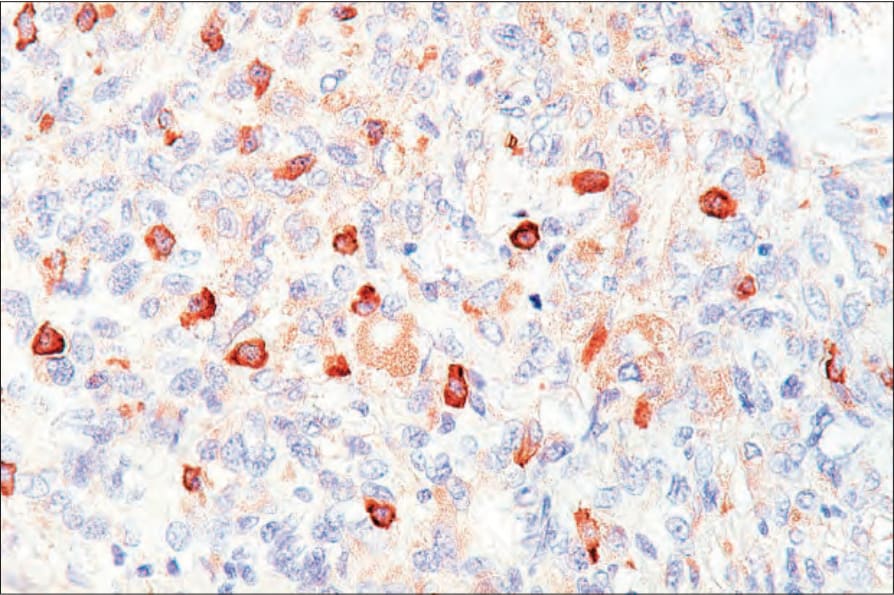
Fig. 35.257 Cellular neurothekeoma: the tumor cells express NKI-C3 but are S100 protein negative.
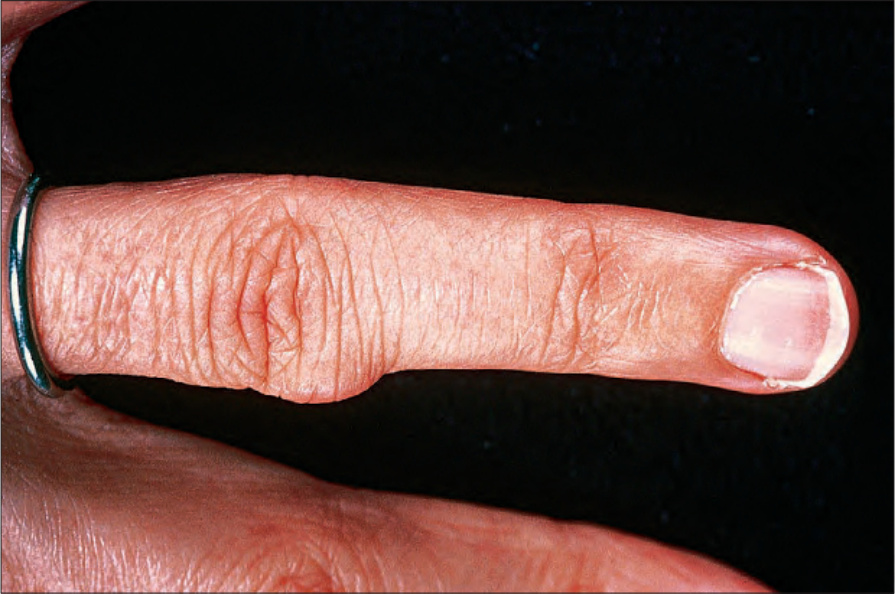
Fig. 35.258 Giant cell tumor of tendon sheath: this lesion presents as a firm nodule that most often affects the finger. By courtesy of H. du P. Menagé, MD, Institute of Dermatology, London, UK.