纖維組織球瘤/皮膚纖維瘤 (Fibrous histiocytoma / dermatofibroma)
纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma)
纖維組織球瘤 (fibrous histiocytoma;又稱 dermatofibroma、sclerosing hemangioma、histiocytoma cutis、nodular subepidermal fibrosis) 是最常見的良性皮膚軟組織腫瘤之一。1–5 多年來已描述出多種變異型,雖然這些變異型本質上是凸顯了可能造成診斷混淆的特定組織學特徵,但其中部分也與特徵性的臨床表現與行為相關6,7(見下文)。然而必須強調,數種變異型的組織學特徵可共存於同一個病灶中。8
臨床特徵 (Clinical Features)
纖維組織球瘤最常發生於中年人,並呈現輕微的女性優勢。多數病灶位於四肢,或(程度較低地)位於軀幹,表現為小型、隆起、過度角化 (hyperkeratotic) 的皮膚結節,直徑通常小於 1 cm,表面呈紅棕色 (Figs 35.207 and 35.208)。包括斑塊樣 (plaque-like) 變異型在內的巨大變異型極為罕見。9–12.
相當比例的病例據稱與先前的輕微局部創傷相關,尤其是昆蟲叮咬。它們生長緩慢且無痛,有時可為多發性。在免疫抑制 (immunosuppression)、HIV 感染以及高效能抗反轉錄病毒療法 (highly active antiretroviral therapy, HAART) 的情境下,已記載有爆發性 (eruptive) 病灶。13–19
多數皮膚纖維瘤呈現典型的皮膚鏡 (dermoscopy) 模式(周邊細緻的色素網與中央白色疤痕樣斑塊),但非典型模式可能模擬黑色素瘤 (melanoma)、血管性腫瘤、basal cell carcinoma、碰撞瘤 (collision tumor),甚至 psoriasis。31
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
致病機轉不明,但病灶在女性中遠較常見,且腫瘤細胞表現 estrogen receptor alpha,提示可能有荷爾蒙的病因角色。19 目前尚不清楚它是反應性 (reactive) 或腫瘤性 (neoplastic) 病變。17,20
表皮外觀無特殊變化。在淺層與中層真皮中可見小型、薄壁血管腔道的增生,每個腔道周圍環繞著一層周細胞 (pericytes) (Fig. 35.204)。周圍真皮含有散在的多核細胞,具有角狀的細胞質,背景為某種程度玻璃樣變 (hyalinized) 的膠原束 (Figs 35.205 and 35.206)。偶可見淋巴球。曾發現一個具有真皮神經腫大的例外病例。21 可能出現含鐵血黃素 (hemosiderin) 沉積。
這些多核細胞對 CD68 與 lysozyme 呈陽性,而間質細胞 (interstitial cells) 可能對 factor XIIIa 呈陽性。7,21
單純切除通常即可治癒,局部復發少見,除了某些變異型(見下文)以及發生於顏面的病灶(其報告之局部復發率為 20%)以外。20 在某些變異型(如 atypical、aneurysmal 與 cellular fibrous histiocytoma)以及例外的典型腫瘤中,曾報告罕見的轉移。21–28
這些病灶中有一小亞群起源於皮下脂肪或更深層結構(深部良性纖維組織球瘤,deep benign fibrous histiocytoma)。29,30
致病機轉與組織學特徵(續)
多年來曾認為皮膚纖維瘤代表一種反應性過程。可能的病因相關因素包括昆蟲叮咬,甚至如穿耳洞 (body-piercing) 之類的創傷。32 後來逐漸明確,該病灶代表一種腫瘤性過程。支持後者的臨床證據包括以下幾點:腫瘤不傾向自發性消退、某些變異型有不等程度的局部復發潛能,以及少數病例曾發生轉移。21–28,33 細胞遺傳學分析為此理論提供進一步支持。在某些 cellular fibrous histiocytoma 的例子中已證實有克隆性 (clonality)。34,35 較近期的研究透過 FISH 分析與 RNA 定序,在罕見的皮膚纖維組織球瘤亞型(cellular 與 aneurysmal)以及極例外的常規病灶與 deep fibrous histiocytoma 中證實了基因異常。36,37 在 regular、epithelioid、cellular 與 aneurysmal fibrous histiocytoma 中可見 protein kinase C 基因 (PRKCB 與 PRKCD) 的重排,而 ALK 重排僅見於 epithelioid 變異型。37 PRKC 與 ALK 的重排為互斥事件;這些基因的過度表現驅動啟動子交換 (promoter swapping),並與相當多樣的其他基因融合夥伴結合,包括 LAMTOR1、PDPN 與 CD63。在另一項研究中,
透過比較基因組雜交 (comparative genomic hybridization) 在轉移性腫瘤以及罕見的非轉移性 atypical 與 cellular 變異型病例中偵測到 DNA 拷貝數變化。27,38 在導致死亡的轉移性病例中,染色體異常較高。關於 aneurysmal fibrous histiocytoma,曾描述一個 t(12;19)(p12;q13) 易位,並有人提出 LAMTOR1-PRKCD 與 NUMA1-SFMBT1 的致病角色。39,40
常見變異型為一邊界不清的真皮病灶,可能延伸至淺層皮下脂肪 (Figs 35.209–35.213)。它大致由交織的纖細梭形細胞束組成,有時呈局部車輻狀 (storiform) 排列,位於疏鬆的膠原性(較少為黏液樣,myxoid)間質中。散布於梭形細胞之間的有泡沫狀組織球 (foamy histiocytes)、多核巨細胞與薄壁血管 (Figs 35.214–35.217)。常可見慢性發炎細胞灶(包括淋巴球與漿細胞)以及含鐵血黃素沉積。一個典型特徵是在病灶周邊處可見被腫瘤細胞包圍的單個玻璃樣膠原束。
長期存在的病灶呈現漸進性玻璃樣變與細胞密度降低,通常被稱為硬化性 (sclerosing) 或萎縮性 (atrophic) 皮膚纖維瘤。
所有這些腫瘤(包括變異型)都可能伴隨表覆表皮的棘層肥厚 (acanthosis),甚至假上皮瘤樣增生 (pseudoepitheliomatous hyperplasia),以及基底細胞層的色素增多 (hyperpigmentation) (Figs 35.218 and 35.219)。有人提出 epidermal growth factor 可能在表皮增生的致病機轉中扮演角色。41 通常存在一個乳頭真皮免受侵犯的 grenz zone (Fig. 35.220)。模擬脂漏性角化症 (seborrheic keratosis) 的變化很常見,其次為模擬透明細胞棘皮瘤 (clear cell acanthoma) 的透明細胞增生、密切類似毛母細胞瘤 (trichoblastoma) 的未成熟毛囊樣結構增生,以及有時呈網狀模式的皮脂腺誘導 (Fig. 35.221)。42,43 成熟毛囊罕被誘導;亦曾描述較不尋常的表皮變化,包括表皮鬆解性過度角化 (epidermolytic hyperkeratosis)、局部棘層鬆解 (focal acantholysis),甚至 Bowen disease。44,45 多數報告為 basal cell carcinoma 覆蓋於皮膚纖維瘤之上的病例,實際上代表未成熟毛囊結構的反應性誘導,而非碰撞瘤。
一部分腫瘤(尤其是 cellular 變異型)對 α-SMA 與 calponin 呈局部染色,提示肌纖維母細胞 (myofibroblastic) 分化 (Fig. 35.222)。有人提出此病灶起源於一種固定的真皮結締組織細胞,即真皮樹突細胞 (dermal dendrocyte),其對 factor XIIIa 呈陽性染色。46 雖然纖維組織球瘤內有許多細胞會與此標記反應(尤其朝向病灶邊緣處),但這些似乎是反應性細胞而非真正的腫瘤細胞。與 dermatofibrosarcoma 相反,CD34 表現通常並非其特徵,但 cellular 變異型除外。
在纖維組織球瘤中可見此標記(CD34)的局部陽性(見下文)。D2–40 在皮膚纖維瘤中呈瀰漫性陽性,而在 dermatofibrosarcoma protuberans 中僅呈非常局部的陽性或陰性。47
常見的皮膚纖維瘤通常容易診斷,鑑別診斷的問題一般只在其變異型時才出現。48
皮膚纖維瘤的變異型包括:
- cellular fibrous histiocytoma(細胞型纖維組織球瘤)
- aneurysmal fibrous histiocytoma(動脈瘤樣纖維組織球瘤)
- epithelioid fibrous histiocytoma(上皮樣纖維組織球瘤)
- atypical (pseudosarcomatous) fibrous histiocytoma(非典型/假肉瘤樣纖維組織球瘤)
- lipidized (‘ankle-type’) fibrous histiocytoma(脂質化/「踝部型」纖維組織球瘤)
- clear cell fibrous histiocytoma(透明細胞纖維組織球瘤)
- palisading cutaneous fibrous histiocytoma(柵欄狀皮膚纖維組織球瘤)
- atrophic dermatofibroma(萎縮性皮膚纖維瘤)。重要的是要注意,除了 epithelioid 變異型以外,皮膚纖維瘤的所有變異型在組織學上都可能彼此重疊。
變異型 (Variants)
Cellular fibrous histiocytoma(細胞型纖維組織球瘤)
Cellular benign fibrous histiocytoma 約佔皮膚纖維組織球瘤的近 5%。48–50 它最常見於年輕成人,尤其是男性,並好發於四肢以及頭頸部 (Figs 35.223 and 35.224)。這些病灶較常見的纖維組織球瘤大,且復發率高達 26%。少數病例曾報告轉移至區域淋巴結、軟組織與肺。22–28 亦曾描述衛星結節 (satellite nodules) 的形成。26 另有一病例發生指骨 (phalanx) 侵蝕。51 組織學特徵無法預測最終會轉移的病例。26 較可能轉移的病例似乎是那些早期復發且多次復發者。
組織學上,病灶高度富含細胞,具有更顯著的束狀 (fascicular) 生長模式 (Figs 35.225–35.228)。常侵犯淺層皮下組織。腫瘤細胞傾向具有較豐富的嗜伊紅細胞質,且常見正常的有絲分裂象 (mitotic figures) (Fig. 35.229)。某些病例(約 10%)可見中央壞死。曾在一例原發性 cellular fibrous histiocytoma 以及一個復發腫瘤中描述到多形性肉瘤 (pleomorphic sarcoma) 成分。27
免疫組織化學顯示對 SMA 呈可變的(通常為局部)染色(多數病例如此)以及 calponin,而對 CD34 呈陰性或僅局部染色 (Fig. 35.230)。當後者(CD34)存在時,其表現僅限於腫瘤的周邊部分。約三分之一的病例可見局部 desmin 陽性。52
與 leiomyosarcoma 的區別可藉由後者具有以下特徵來進行:細胞具有雪茄狀核 (cigar-shaped nuclei)、至少局部的細胞學非典型性、一致的束狀生長模式、對 SMA、desmin 與 H-caldesmon 呈瀰漫性陽性,以及常有對 keratin 的局部陽性。Dermatofibrosarcoma protuberans 則具有單調的車輻狀生長模式、單一形態的細胞,以及對 CD34 呈瀰漫性陽性。
Aneurysmal fibrous histiocytoma(動脈瘤樣纖維組織球瘤)
Aneurysmal benign fibrous histiocytoma 佔纖維組織球瘤不到 2%,表現為中年成人(尤其女性)四肢上的藍棕色結節 (Fig. 35.231)。53–56 由於廣泛出血可見快速生長,臨床上常與黑色素細胞性或血管性腫瘤混淆。復發率約為 19%。54 罕見病例以區域淋巴結侵犯表現。26,27,54
組織學上,最顯著的特徵是(尤其朝向病灶中央)出現出血性、不規則的裂隙樣與囊狀空間,模擬海綿狀血管腔道,但無內皮襯裡 (Figs 35.232 and 35.233)。鄰近的實性區域顯示良性纖維組織球瘤的常見特徵,但通常富含細胞。多灶性間質出血以及細胞內外的含鐵血黃素沉積很顯著,且常見正常的有絲分裂象 (Figs 35.234–35.236)。由於廣泛的次發性變化,此病灶常被診斷為血管性腫瘤,但纖維組織球瘤的典型特徵總是存在,且內皮標記僅在正常血管中呈陽性。
Aneurysmal fibrous histiocytoma 不應與 angiomatoid fibrous histiocytoma 混淆,後者是一種不相關的腫瘤,具有 EWSR1-CREB1 基因融合。後者通常位於皮下,由單一形態的梭形至卵圓形嗜伊紅細胞組成,這些細胞通常 desmin 陽性。常存在顯著的淋巴漿細胞 (lymphoplasmacytic) 浸潤。部分患有後者疾病的病人具有顯著的全身性症狀。
Hemosiderotic fibrous histiocytoma(含鐵血黃素性纖維組織球瘤)可能代表 aneurysmal fibrous histiocytoma 發展中的一個階段。
Epithelioid fibrous histiocytoma(上皮樣纖維組織球瘤)
Epithelioid fibrous histiocytoma 罕見,具有廣泛的年齡與解剖學分布(好發於下肢近端),常表現為息肉狀紅色結節,通常與小葉狀微血管血管瘤(lobular capillary hemangioma,即化膿性肉芽腫,pyogenic granuloma)混淆 (Fig. 35.237)。57–60 多發病灶極為例外,並曾報告一個發生於舌部的病灶。61,62 曾描述一個具有轉移性擴散的病例。26 組織學上,多數腫瘤位於淺層,但罕見例子可延伸至淺層皮下組織。常存在表皮環領 (epidermal collarette),腫瘤細胞為圓形,具有豐富的嗜伊紅細胞質與一個含小型嗜伊紅核仁的泡狀核 (vesicular nucleus) (Figs 35.238–35.241)。雙核或多核細胞很常見。罕見情況下,細胞可有顆粒細胞變化 (granular cell change)。63 偶可見正常的有絲分裂象。某些病灶較具黏液樣與血管性。曾報告一種罕見的腫瘤變異型,呈軟骨母細胞瘤樣 (chondroblastoma-like),由細胞周圍鈣化 (pericellular calcification) 組成。64 免疫組織化學顯示一群 CD34 陽性細胞,以及一群 factor XIIIa 陽性的樹突細胞。65 與 Spitz nevus 的區別可藉由缺乏交界處 (junctional) 成分或腫瘤細胞的巢狀排列,以及 S100 蛋白陰性來協助。與具上皮樣細胞變化的皮膚周邊神經瘤 (cutaneous perineurioma) 的區別,是藉由後者腫瘤中瀰漫性的 EMA 與 claudin-1 陽性。然而,局部膜性 EMA 陽性在 epithelioid fibrous histiocytoma 中是常見的發現。66 典型可見 ALK 表現(約 90% 的病例),並與多種夥伴基因(包括 SQSTM1、VCL、TMP3、EML4、PRKAR2A 等)的 ALK 重排相關 (Fig. 35.242)。67–69
Atypical (pseudosarcomatous) fibrous histiocytoma(非典型/假肉瘤樣纖維組織球瘤)
Atypical (pseudosarcomatous) fibrous histiocytoma 又稱為具有怪物細胞的皮膚纖維瘤 (dermatofibroma with monster cells)。21,70–73 臨床上,它好發於四肢,部分腫瘤發生於軀幹與頭頸部。病灶通常為丘疹狀或結節狀,但也可能為息肉狀,罕見腫瘤可大至數公分。21 少數病例有局部復發,轉移罕見發生,曾有一名病人因全身性擴散而死亡。21,26,27
組織學上,病灶主要位於真皮,但三分之一的病例延伸至淺層皮下組織。在某些區域,腫瘤呈現較典型纖維組織球瘤的特徵 (Fig. 35.243)。然而,腫瘤中有不等比例的細胞具有不規則、大型且多形性的核,並有顯著的核仁 (Fig. 35.244)。多形性 (pleomorphism) 可能很明顯。有絲分裂率不一,某些病例可能很高。有時可見非典型有絲分裂象。一個不尋常的特徵是局部壞死 (focal necrosis)。20 組織學特徵無法預測那些例外會轉移的腫瘤。26
Atypical fibrous histiocytoma 不應與 atypical fibroxanthoma 混淆。後者發生於完全不同的臨床情境(見下文),且通篇顯示瀰漫性多形性、細胞學非典型性與大量有絲分裂。
Lipidized (‘ankle-type’) fibrous histiocytoma(脂質化/「踝部型」纖維組織球瘤)
Lipidized (‘ankle-type’) fibrous histiocytoma 表現為小腿上的息肉狀黃色病灶。74 組織學上,以泡沫狀組織球為主,被豐富、幾近瘢痕疙瘩樣 (keloidal)、玻璃樣變的膠原束所包圍 (Figs 35.245–35.247)。
Palisading cutaneous fibrous histiocytoma(柵欄狀皮膚纖維組織球瘤)
Palisading cutaneous fibrous histiocytoma 指組織學上顯示顯著核柵欄狀排列 (nuclear palisading) 的病灶 (Figs 35.248 and 35.249)。80,81 它們似乎最常見於肢端 (acral) 部位。局部上,由於柵欄狀排列模擬 Verocay bodies,而與 schwannoma 相似。然而,病灶並無包膜,且腫瘤細胞 S100 陰性。
Clear cell fibrous histiocytoma(透明細胞纖維組織球瘤)
這是一種非常罕見的變異型,無特徵性臨床表現,整個病灶中具有大量的透明細胞變化。75–77 其整體結構與形態學特徵通常不是纖維組織球瘤的典型特徵,因此可能代表一種完全不相關的腫瘤。先前被描述為 clear cell fibrous histiocytoma 的腫瘤,很可能代表被報告為真皮透明細胞間葉性腫瘤 (dermal clear cell mesenchymal neoplasm) 的疾病。78,79 後者疾病僅有少數病例被描述於成人,好發於下肢。腫瘤由透明細胞片狀組成,具有泡狀核,佔據網狀真皮,並可延伸至皮下組織。細胞學非典型性與有絲分裂象罕見。腫瘤細胞對多數標記呈陰性,但 vimentin、NKI/C3 與有時 CD68 除外。其行為似乎為良性。
Atrophic dermatofibroma(萎縮性皮膚纖維瘤)
Atrophic dermatofibroma 很可能代表許多皮膚纖維瘤的終末期,臨床上以一處凹陷或牽縮 (retraction) 為特徵,常類似疤痕甚至萎縮斑 (anetoderma)。82–84 組織學上,病灶細胞稀少,並顯示顯著的膠原玻璃樣變 (Figs 35.250 and 35.251)。這些變化可能類似多核血管組織球瘤 (multinucleate angiohistiocytoma) 所見的變化,但後者通常以多發性臨床病灶表現。
Rare variants(罕見變異型)
極偶爾地,腫瘤可顯示顯著的破骨細胞樣巨細胞 (osteoclast-like giant cells)(偶伴骨化)、顆粒細胞變化、膽固醇沉積、局部平滑肌增生、明顯的黏液樣變化、瘢痕疙瘩樣變化、氣球細胞變化 (balloon cell change) 與印戒細胞變化 (signet-ring change)。85–102 腫瘤亦可能以苔癬樣 (lichenoid) 模式表現,並在單一病例中描述了胞質內嗜伊紅小球 (intracytoplasmic eosinophilic globules)。103,104 曾報告兩例具有散在色素性黑色素細胞、CD34 陽性,且在 Bednar tumor 與皮膚纖維瘤之間有重疊組織學特徵的腫瘤。105 遺憾的是,這些病例未進行細胞遺傳學研究。另有一例黑色素瘤覆蓋於皮膚纖維瘤之上的病例被報告。106 雖然發炎細胞是多數纖維組織球瘤的特徵,但生發中心 (germinal centers) 的形成罕見。107 亦曾描述具有血管瘢痕疙瘩樣 (angiokeloidal) 模式的病例。108
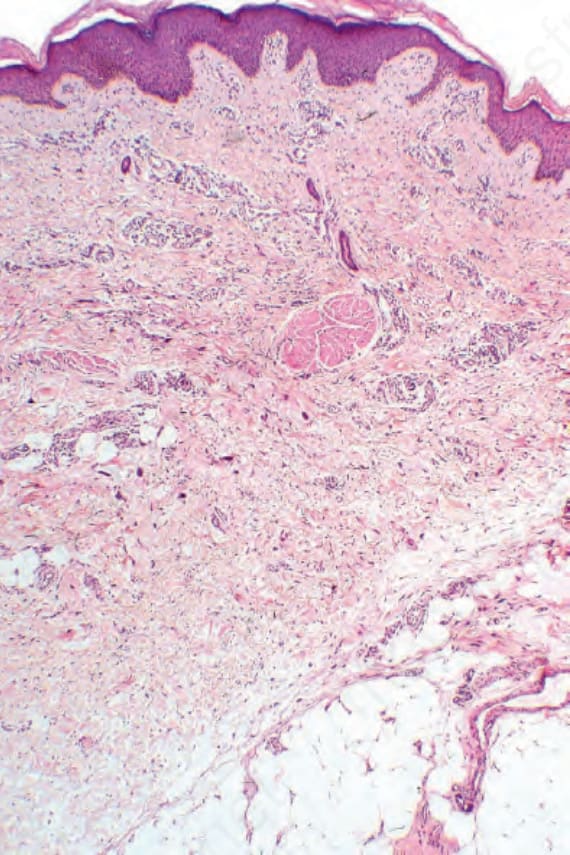
圖 35-204:多核細胞血管組織球瘤 (multinucleate cell angiohistiocytoma):真皮內有一血管性與膠原性的增生性病灶,伴顯著的多核巨細胞 (multinucleate giant cells)。
Fig. 35.204 Multinucleate cell angiohistiocytoma: within the dermis is a vascular and collagenous proliferative lesion with conspicuous multinucleate giant cells.
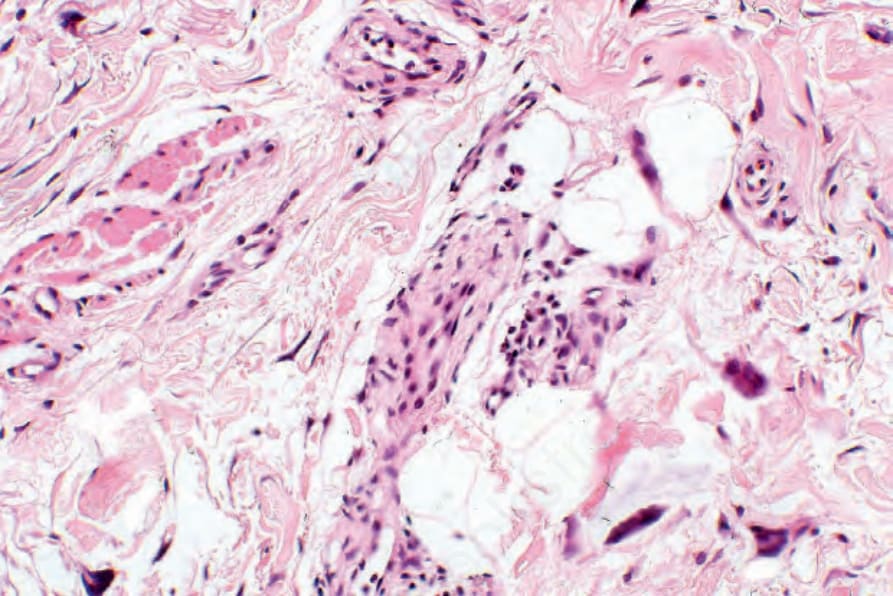
圖 35-205:多核細胞血管組織球瘤 (multinucleate cell angiohistiocytoma):中倍視野顯示血管伴巨細胞與周細胞 (pericytes)。
Fig. 35.205 Multinucleate cell angiohistiocytoma: medium-power view showing vessels with giant cells and pericytes.

圖 35-207:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):此腫瘤最常表現為紅斑性隆起病灶。表面鱗屑並不少見。From the collection of the late N.P. Smith, MD, The Institute of Dermatology, London, UK.
Fig. 35.207 Fibrous histiocytoma (dermatofibroma): this tumor most often presents as an erythematous raised lesion. Surface scaling is not uncommon. From the collection of the late N.P. Smith, MD, The Institute of Dermatology, London, UK.

圖 35-208:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):深棕色(由於含鐵血黃素 hemosiderin 沉積)病灶有時會被誤認為黑色素細胞性腫瘤,包括 melanoma。By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Fig. 35.208 Fibrous histiocytoma (dermatofibroma): dark brown (due to hemosiderin deposition) lesions are sometimes mistaken for melanocytic tumors, including melanoma. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
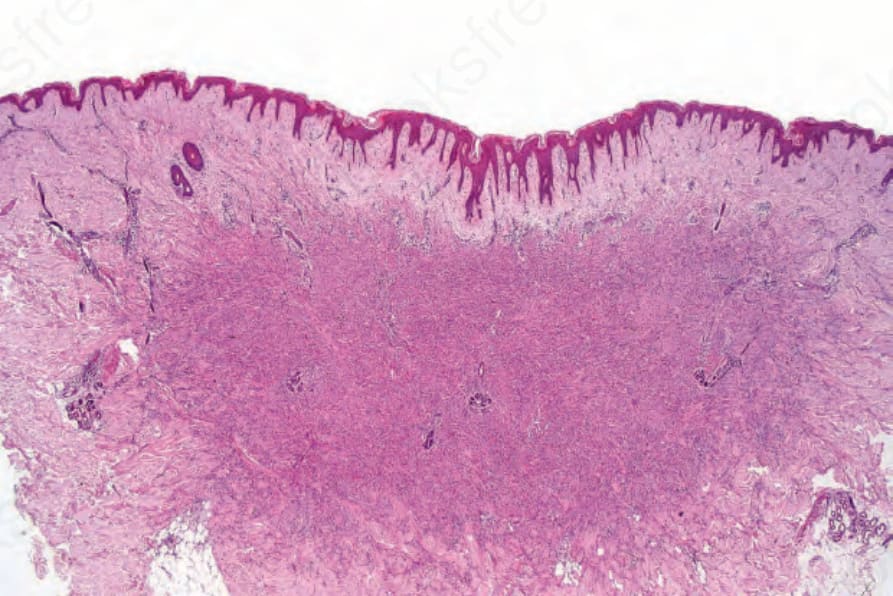
圖 35-209:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):掃描切面顯示特徵性結構。病灶的側緣與鄰近真皮交錯嵌合 (interdigitate)。表覆表皮有過度角化 (hyperkeratosis) 與棘層肥厚 (acanthosis)。
Fig. 35.209 Fibrous histiocytoma (dermatofibroma): scanning section showing the characteristic architecture. The lateral borders of the lesion interdigitate with the adjacent dermis. There is hyperkeratosis and acanthosis of the overlying epidermis.
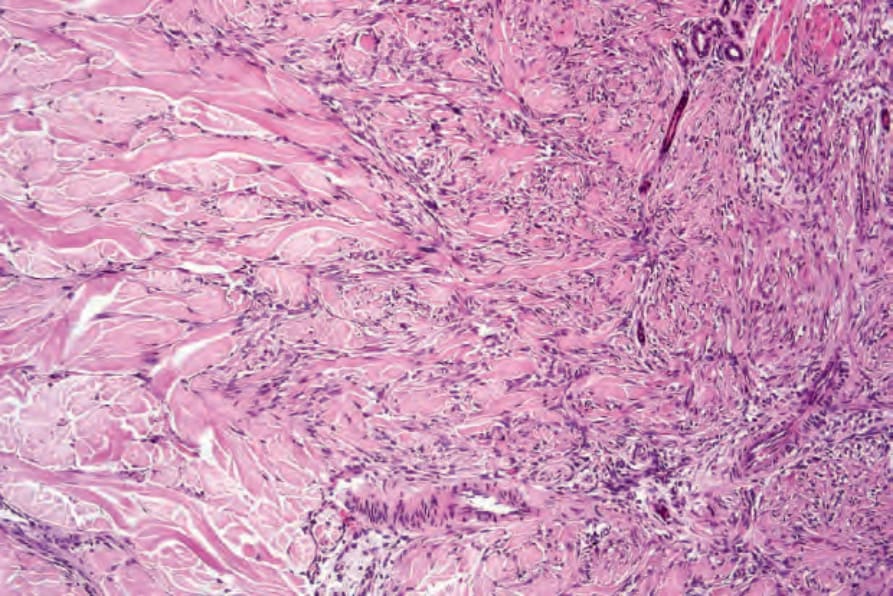
圖 35-210:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):腫瘤延伸至鄰近的正常真皮。
Fig. 35.210 Fibrous histiocytoma (dermatofibroma): the tumor extends into the adjacent normal dermis.
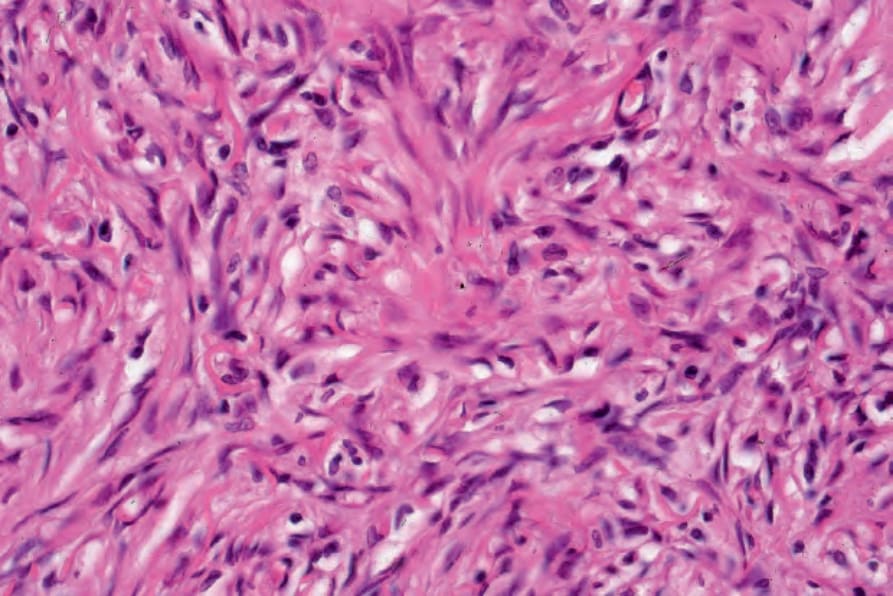
圖 35-211:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):高倍視野顯示車輻狀 (storiform) 生長模式。
Fig. 35.211 Fibrous histiocytoma (dermatofibroma): high-power view showing storiform growth pattern.
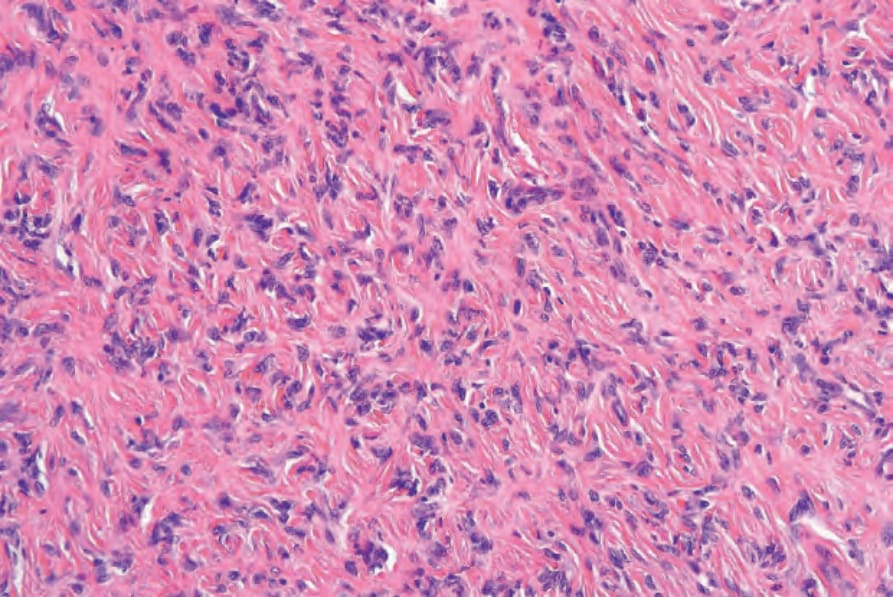
圖 35-212:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):腫瘤由均一、交織的梭形細胞組成,呈模糊的捲曲狀 (curlicue) 模式,嵌於玻璃樣膠原性間質中。
Fig. 35.212 Fibrous histiocytoma (dermatofibroma): the tumor is composed of uniform, interlacing spindle cells in a vaguely curlicue pattern embedded in a hyaline collagenous stroma.
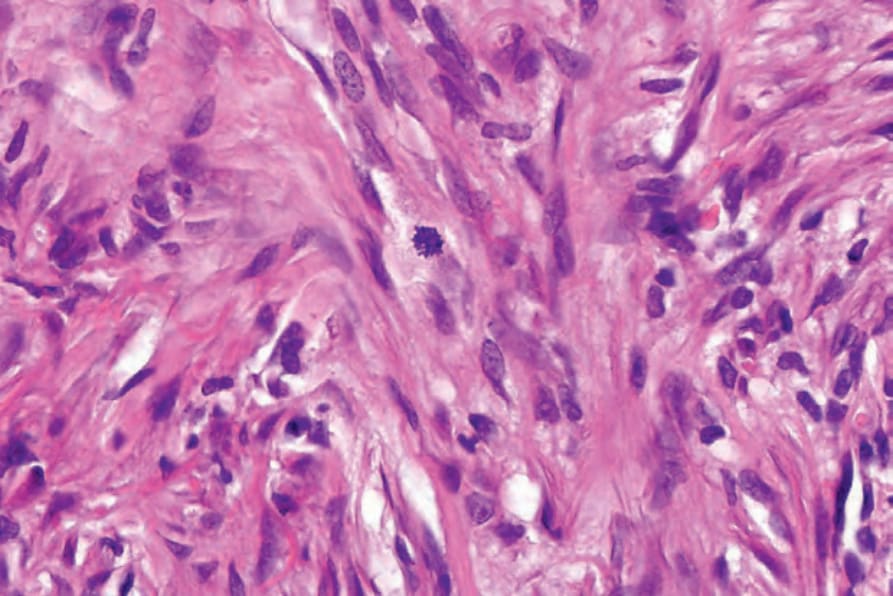
圖 35-213:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):偶可見正常的有絲分裂象 (mitotic figures)。
Fig. 35.213 Fibrous histiocytoma (dermatofibroma): occasional normal mitotic figures may be seen.
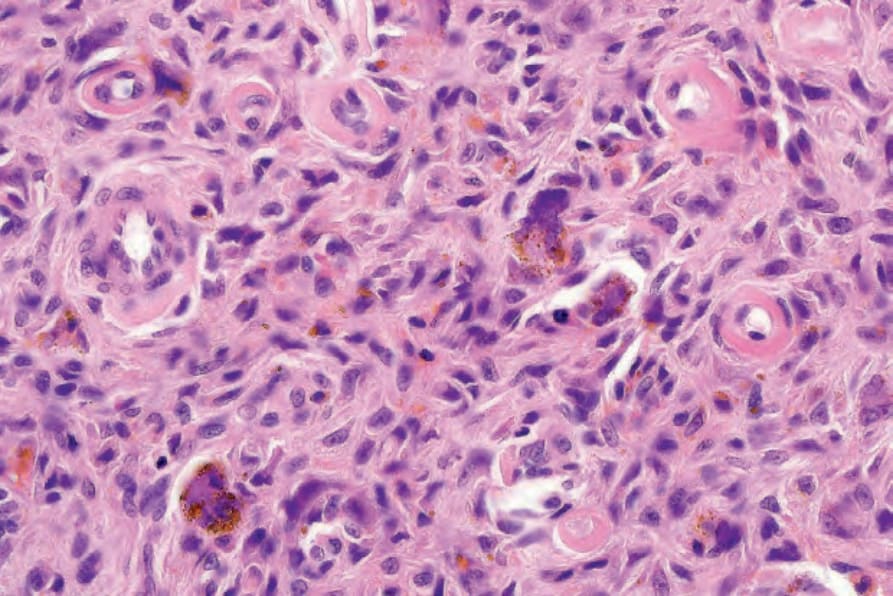
圖 35-214:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):散在的多核巨細胞是此病灶並不少見的特徵。注意含鐵血黃素 (hemosiderin) 色素。
Fig. 35.214 Fibrous histiocytoma (dermatofibroma): scattered multinucleated giant cells are a not infrequent feature of this lesion. Note the hemosiderin pigment.
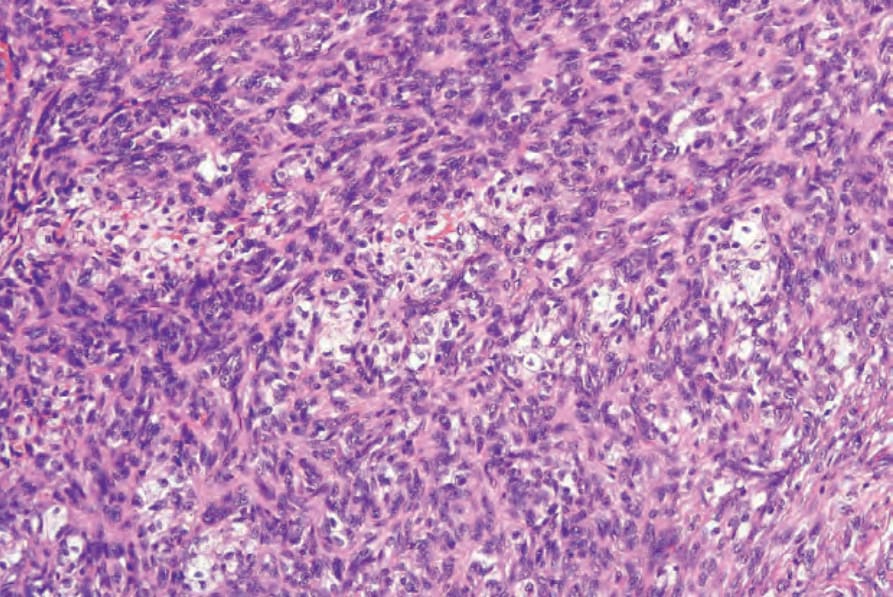
圖 35-215:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):常存在富含脂質的組織球 (lipid-laden histiocytes)。
Fig. 35.215 Fibrous histiocytoma (dermatofibroma): lipid-laden histiocytes are commonly present.
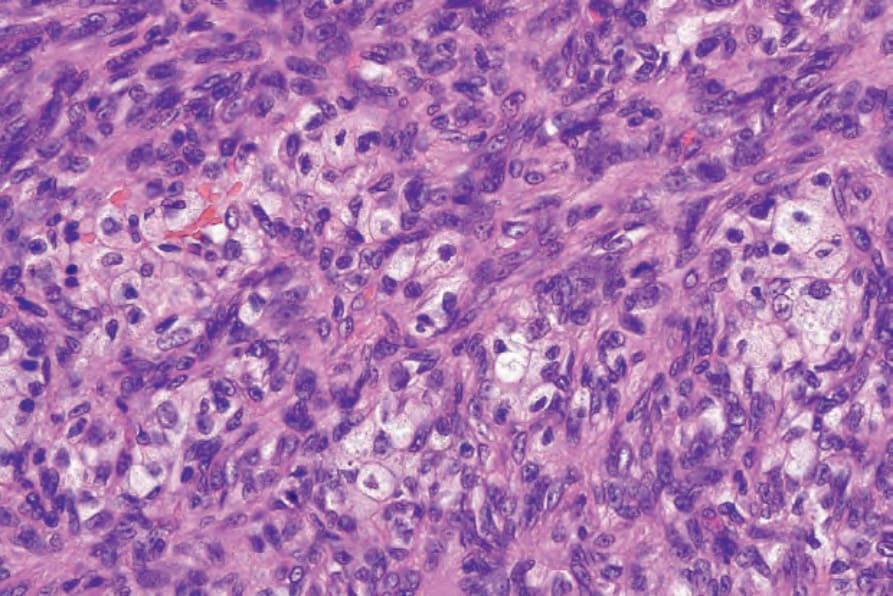
圖 35-216:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):高倍視野。
Fig. 35.216 Fibrous histiocytoma (dermatofibroma): high-power view.
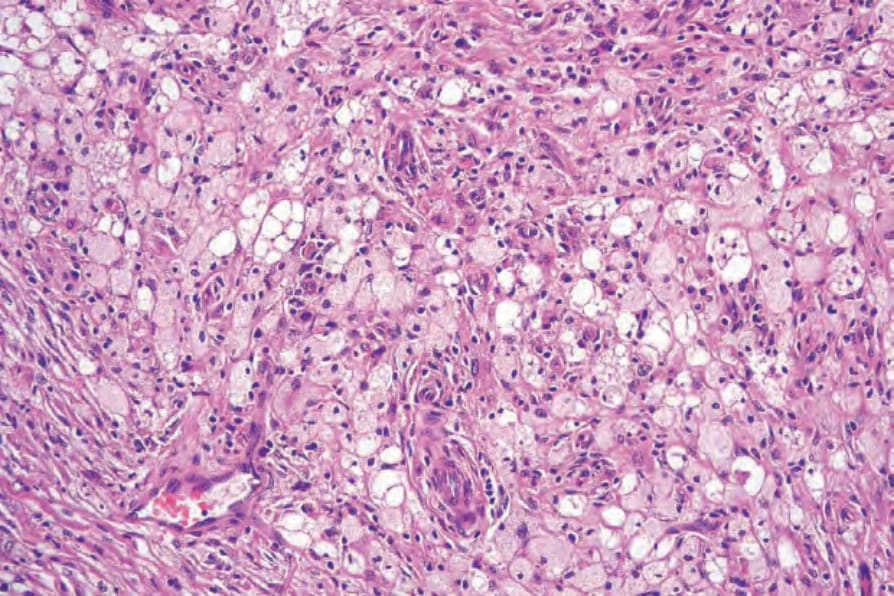
圖 35-217:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):當富含脂質的組織球眾多時,此病灶有時被稱為 histiocytoma cutis。
Fig. 35.217 Fibrous histiocytoma (dermatofibroma): when the lipid-laden histiocytes are numerous, this lesion is sometimes called histiocytoma cutis.
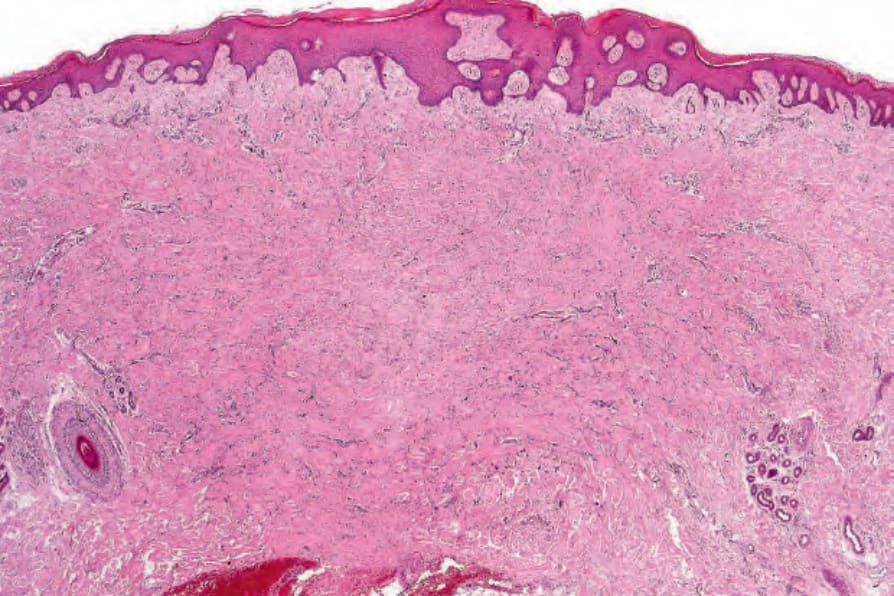
圖 35-218:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):覆蓋於腫瘤之上的上皮常呈棘層肥厚 (acanthotic)。
Fig. 35.218 Fibrous histiocytoma (dermatofibroma): the epithelium overlying the tumor is often acanthotic.
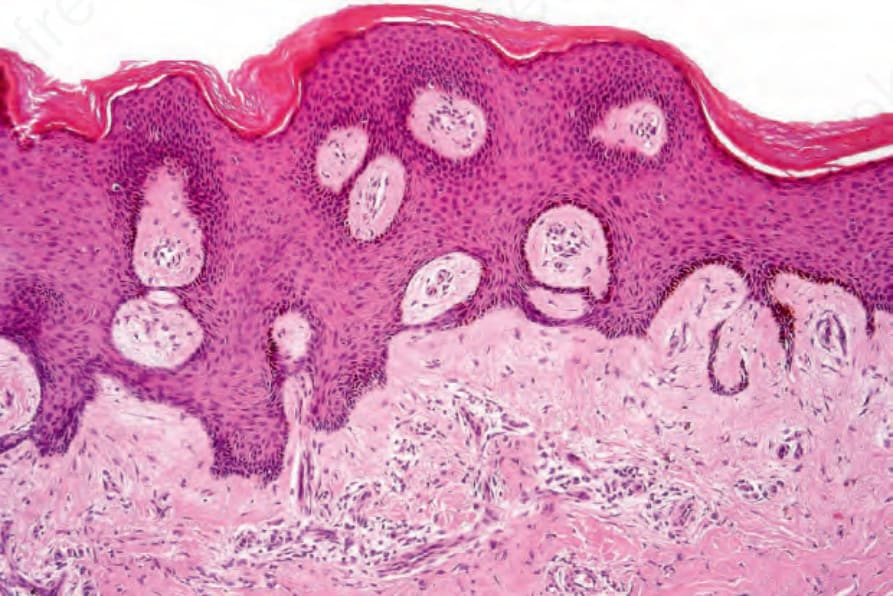
圖 35-219:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):腫瘤常被一個 grenz zone 與表皮分隔開。
Fig. 35.219 Fibrous histiocytoma (dermatofibroma): the tumor is often separated from the epidermis by a grenz zone.
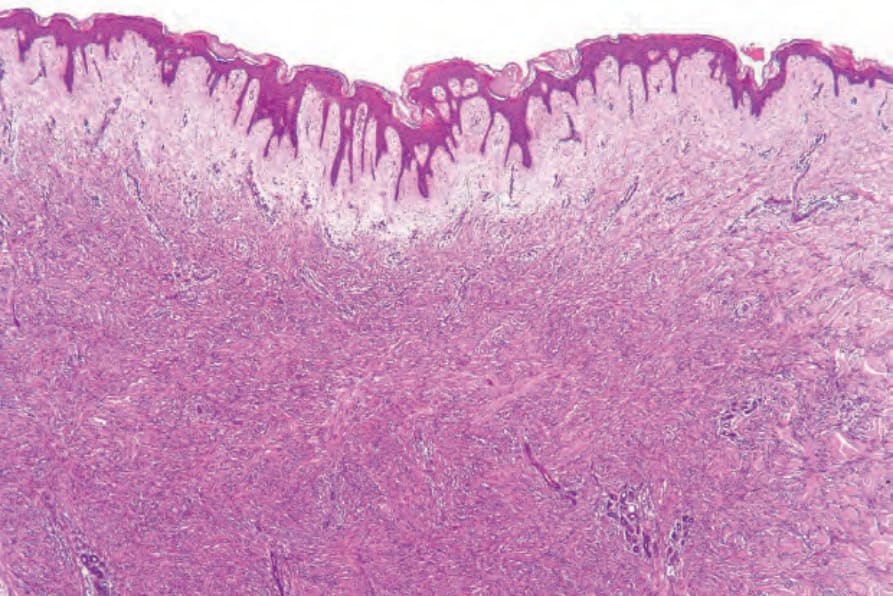
圖 35-220:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):在此例中,有一廣泛的 grenz zone。
Fig. 35.220 Fibrous histiocytoma (dermatofibroma): in this example, there is an extensive grenz zone.
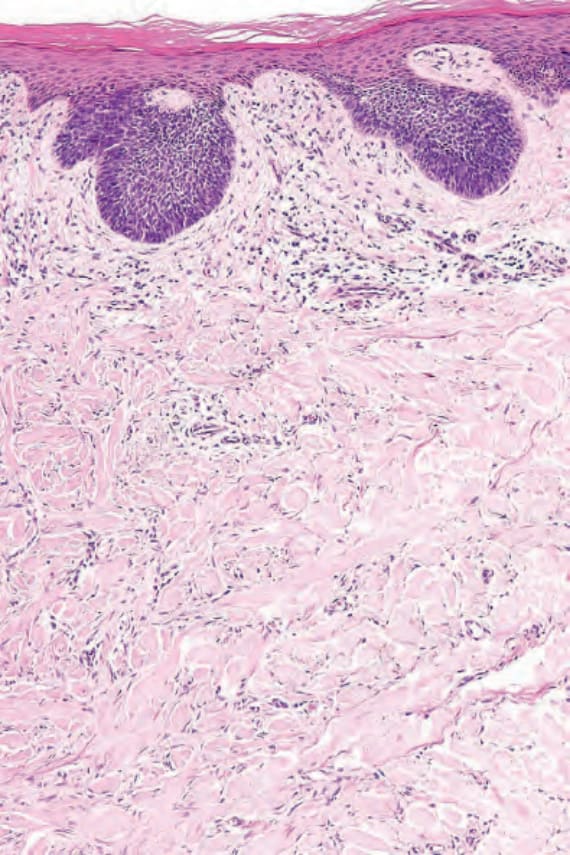
圖 35-221:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):類似毛母細胞瘤 (trichoblastoma) 的基底樣細胞 (basaloid cells) 增生。
Fig. 35.221 Fibrous histiocytoma (dermatofibroma): proliferation of basaloid cells reminiscent of trichoblastoma.
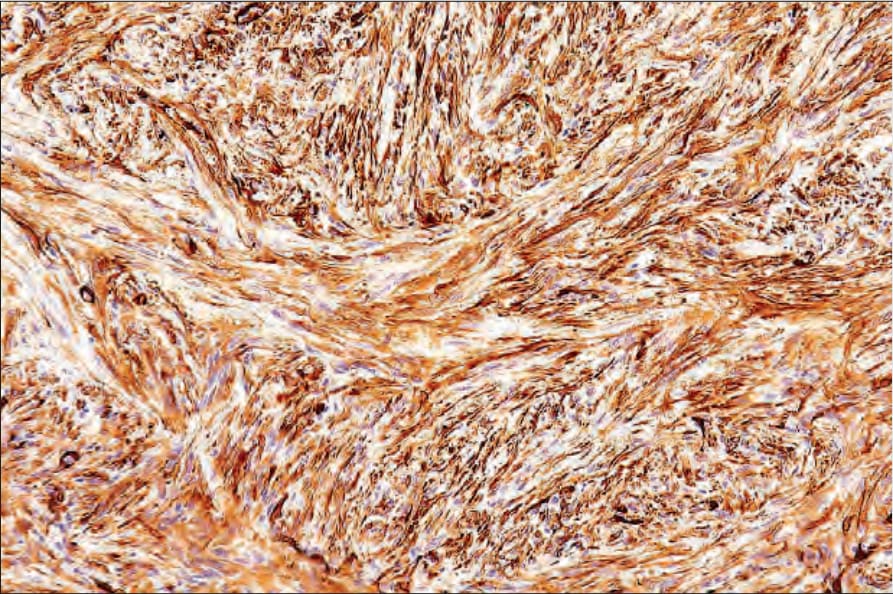
圖 35-222:纖維組織球瘤/皮膚纖維瘤 (fibrous histiocytoma / dermatofibroma):此例顯示強烈的 smooth muscle actin 表現。
Fig. 35.222 Fibrous histiocytoma (dermatofibroma): this example shows strong smooth muscle actin expression.

圖 35-223:細胞型纖維組織球瘤 (cellular fibrous histiocytoma):腫瘤可能很大,有時表現於不尋常部位,如此例所示。By courtesy of the Institute of Dermatology, London, UK.
Fig. 35.223 Cellular fibrous histiocytoma: tumors may be large and sometimes present at unusual sites, as in this example. By courtesy of the Institute of Dermatology, London, UK.

圖 35-224:細胞型纖維組織球瘤 (cellular fibrous histiocytoma):兒童罕受影響。潰瘍 (ulceration) 有時是其特徵。By courtesy of the Institute of Dermatology, London, UK.
Fig. 35.224 Cellular fibrous histiocytoma: children may rarely be affected. Ulceration is sometimes a feature. By courtesy of the Institute of Dermatology, London, UK.
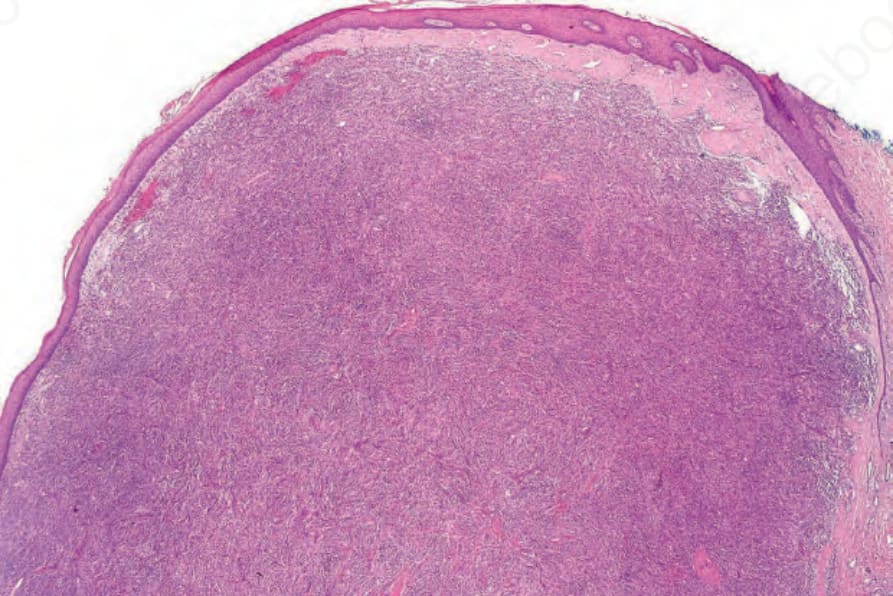
圖 35-225:細胞型纖維組織球瘤 (cellular fibrous histiocytoma):此皮膚纖維瘤變異型常是診斷混淆的來源。它較傳統型大,外觀更富細胞且有絲分裂活性更高。
Fig. 35.225 Cellular fibrous histiocytoma: this variant of dermatofibroma is often a source of diagnostic confusion. It is larger than the conventional form and appears more cellular and mitotically active.
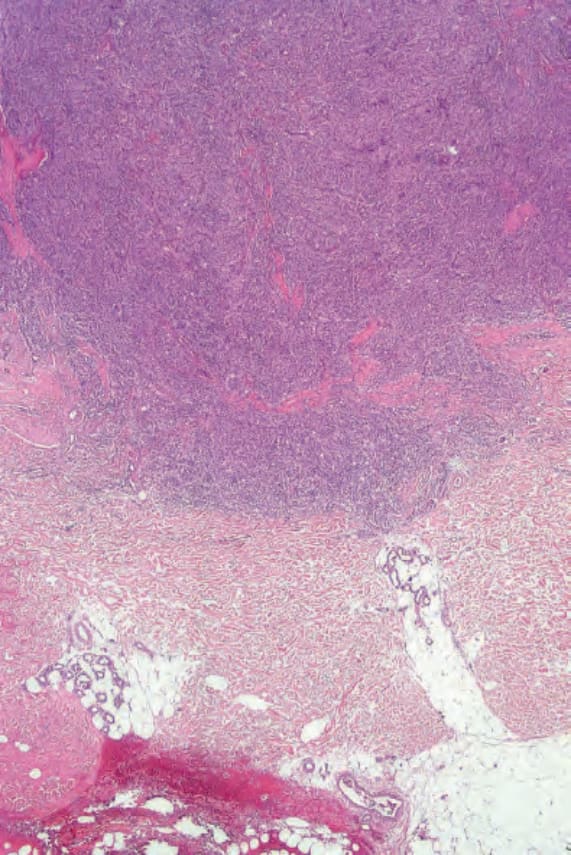
圖 35-226:細胞型纖維組織球瘤 (cellular fibrous histiocytoma):掃描視野顯示延伸至深層網狀真皮。
Fig. 35.226 Cellular fibrous histiocytoma: scanning view showing extension into the deep reticular dermis.
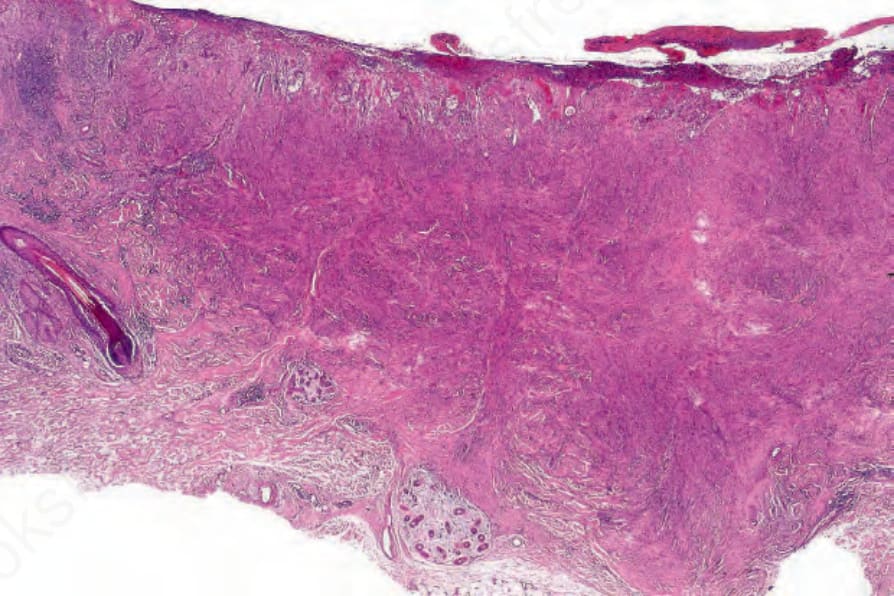
圖 35-227:細胞型纖維組織球瘤 (cellular fibrous histiocytoma):此例顯示驚人的細胞密度。
Fig. 35.227 Cellular fibrous histiocytoma: this example shows striking cellularity.
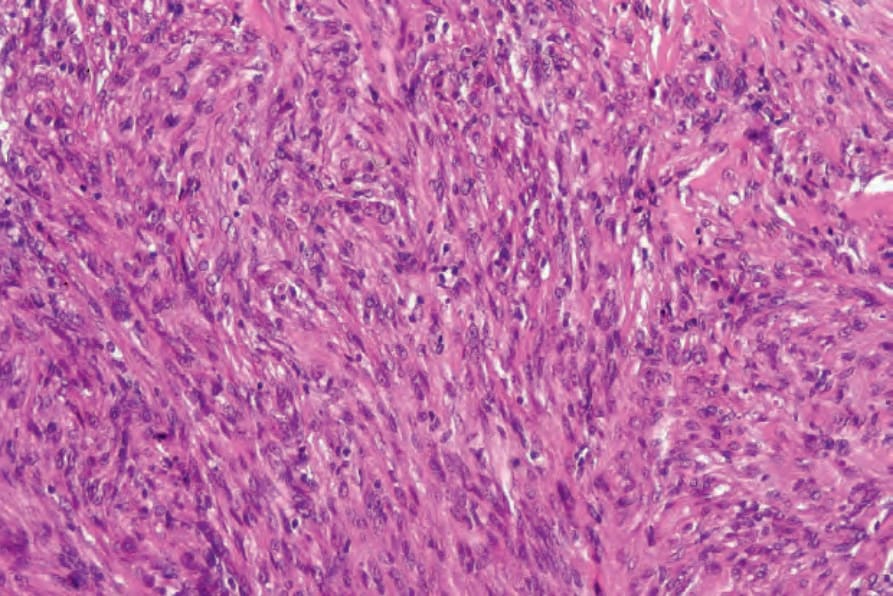
圖 35-228:細胞型纖維組織球瘤 (cellular fibrous histiocytoma):Figure 35.226 的高倍視野。
Fig. 35.228 Cellular fibrous histiocytoma: high-power view of Figure 35.226
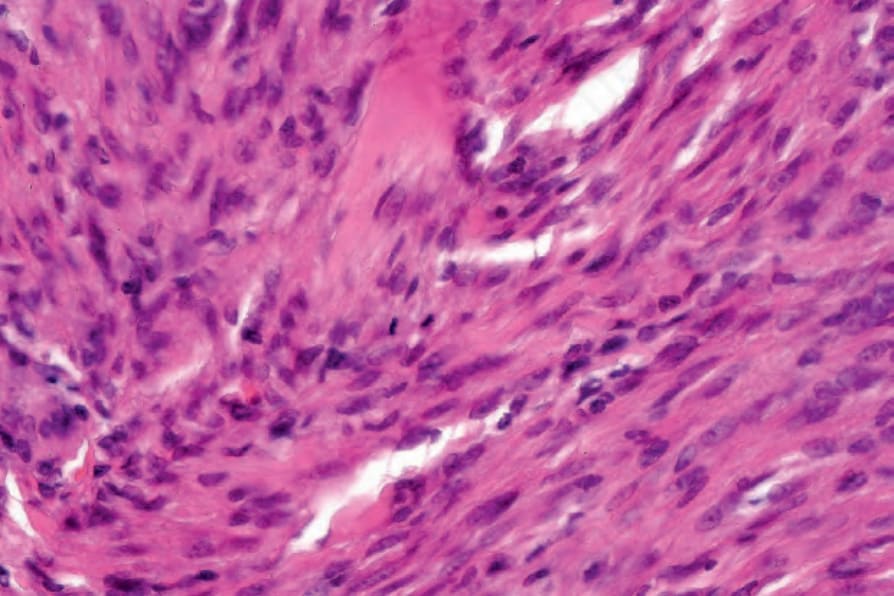
圖 35-229:細胞型纖維組織球瘤 (cellular fibrous histiocytoma):注意有絲分裂活性。
Fig. 35.229 Cellular fibrous histiocytoma: note the mitotic activity.
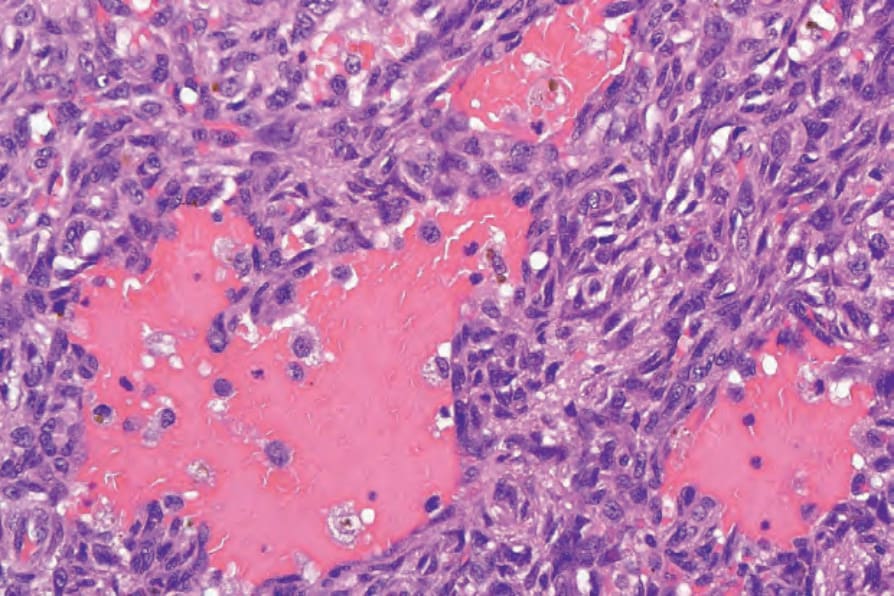
圖 35-233:動脈瘤樣纖維組織球瘤 (aneurysmal fibrous histiocytoma):出血性空間缺乏內皮襯裡。
Fig. 35.233 Aneurysmal fibrous histiocytoma: the hemorrhagic spaces are devoid of an endothelial lining.
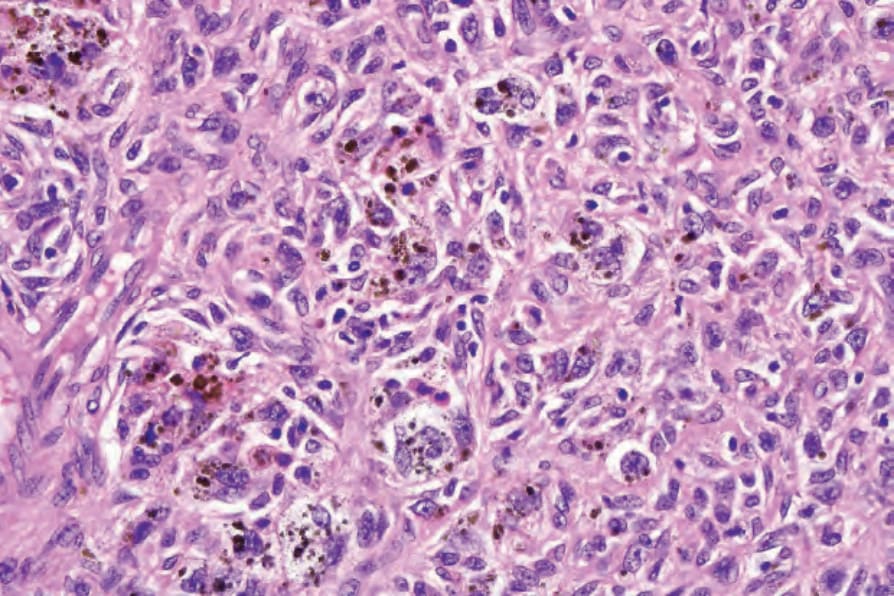
圖 35-235:含鐵血黃素性纖維組織球瘤 (hemosiderotic fibrous histiocytoma):此變異型有時亦稱為 sclerosing hemangioma。
Fig. 35.235 Hemosiderotic fibrous histiocytoma: this variant is also sometimes known as sclerosing hemangioma.
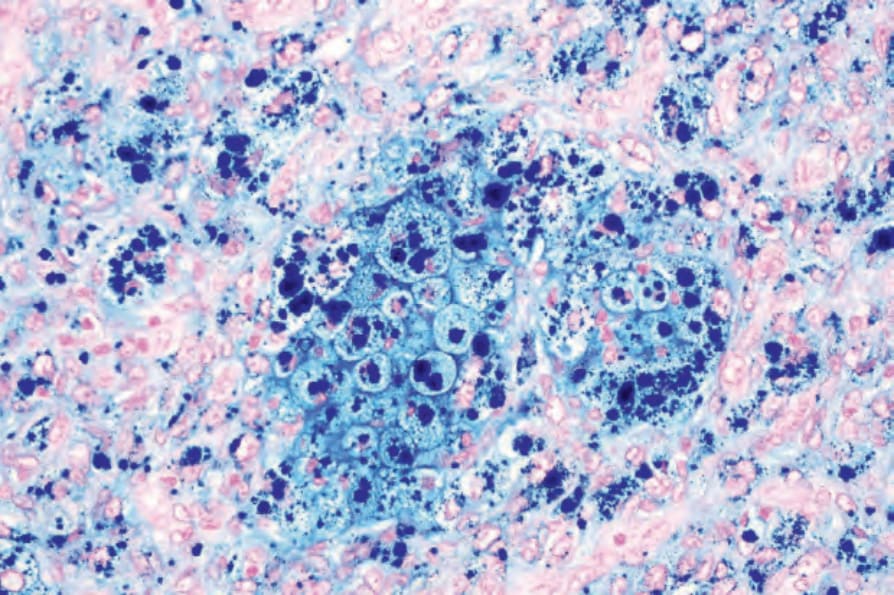
圖 35-236:含鐵血黃素性纖維組織球瘤 (hemosiderotic fibrous histiocytoma):Perl 染色 (Perl stain) 凸顯了含鐵血黃素 (hemosiderin)。
Fig. 35.236 Hemosiderotic fibrous histiocytoma: a Perl stain highlights the hemosiderin.
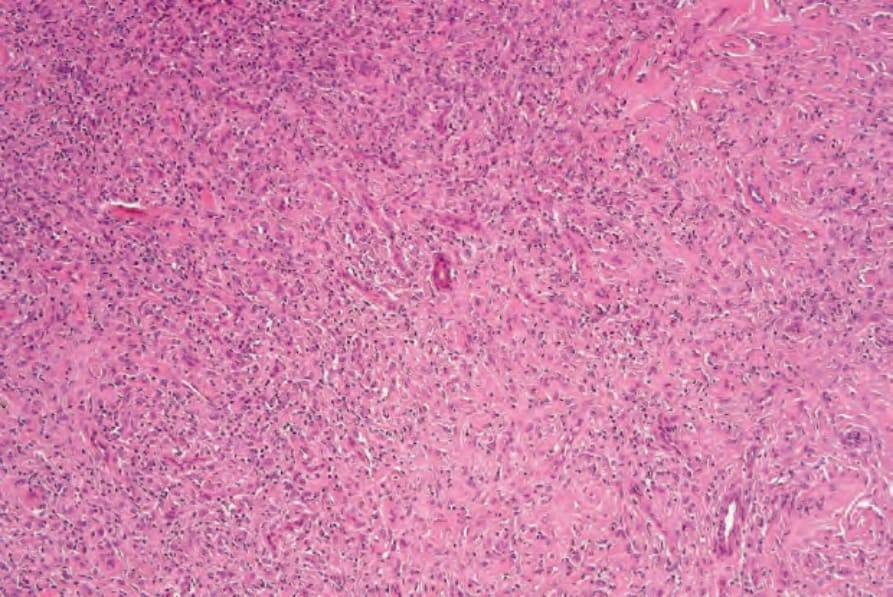
圖 35-239:上皮樣良性纖維組織球瘤 (epithelioid benign fibrous histiocytoma):腫瘤由具有豐富嗜伊紅細胞質的大型細胞組成。浸潤呈均一,與較典型的變異型形成對比。通常在標本他處可辨識出傳統的特徵。
Fig. 35.239 Epithelioid benign fibrous histiocytoma: the tumor is composed of large cells with abundant eosinophilic cytoplasm. The infiltrate is uniform, in contrast to the more typical variant. Often, conventional features are identifiable elsewhere in the specimen.
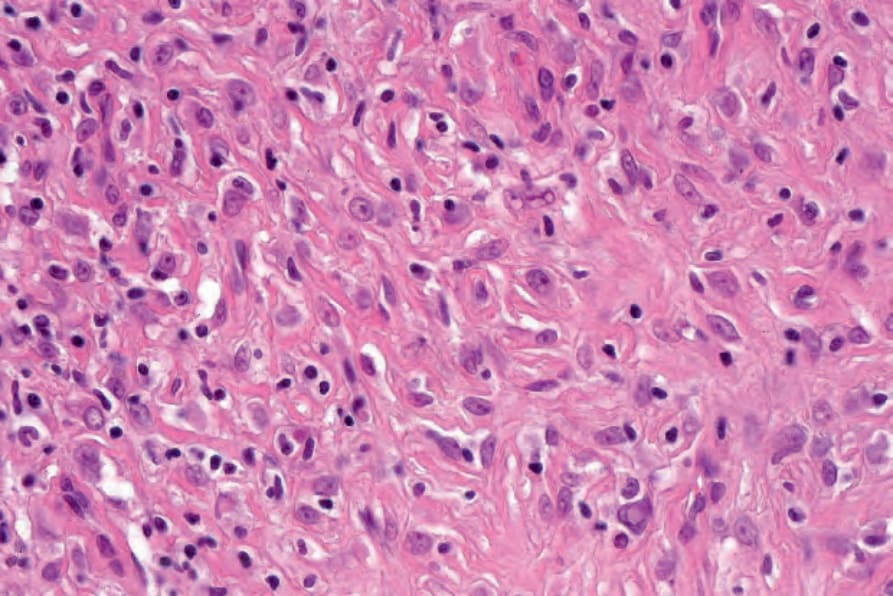
圖 35-240:上皮樣良性纖維組織球瘤 (epithelioid benign fibrous histiocytoma):高倍視野。
Fig. 35.240 Epithelioid benign fibrous histiocytoma: high-power view.
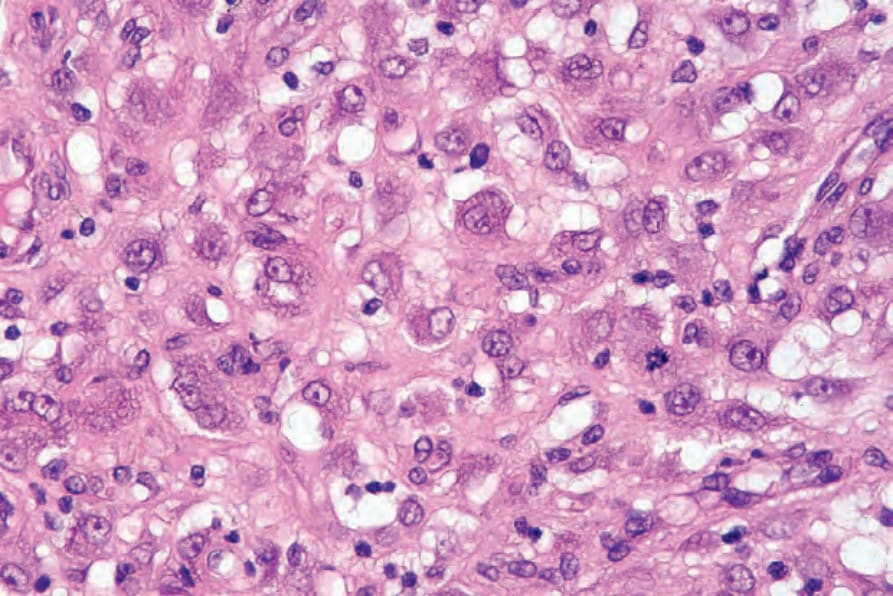
圖 35-241:上皮樣良性纖維組織球瘤 (epithelioid benign fibrous histiocytoma):偶可見正常的有絲分裂象。
Fig. 35.241 Epithelioid benign fibrous histiocytoma: occasional normal mitotic figures may be present.
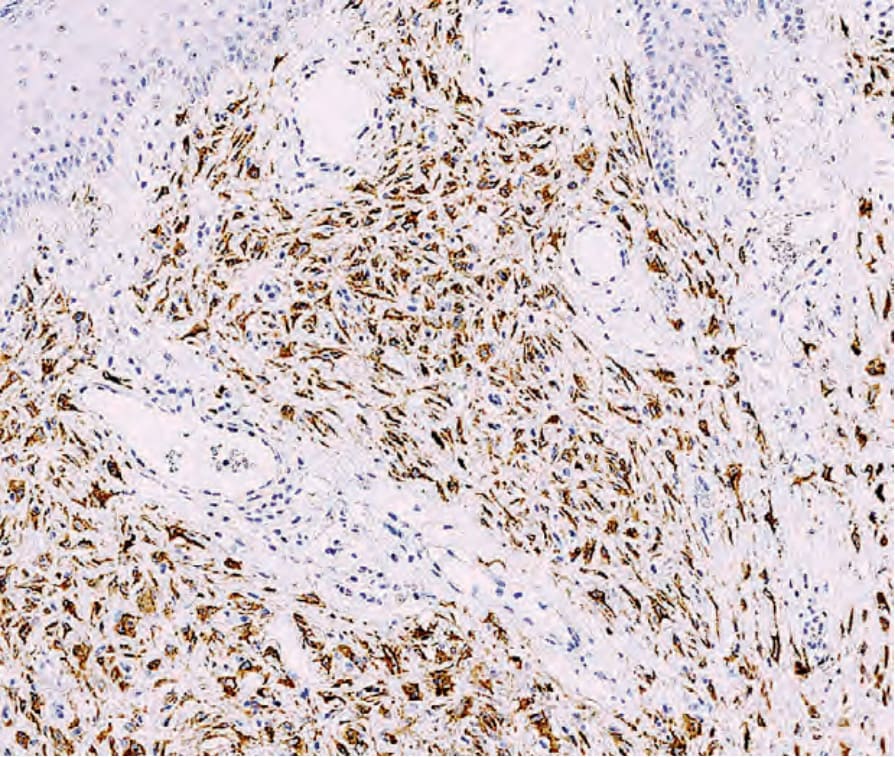
圖 35-242:上皮樣良性纖維組織球瘤 (epithelioid benign fibrous histiocytoma):腫瘤細胞常對 ALK1 呈陽性。
Fig. 35.242 Epithelioid benign fibrous histiocytoma: the tumor cells are often positive for ALK1.
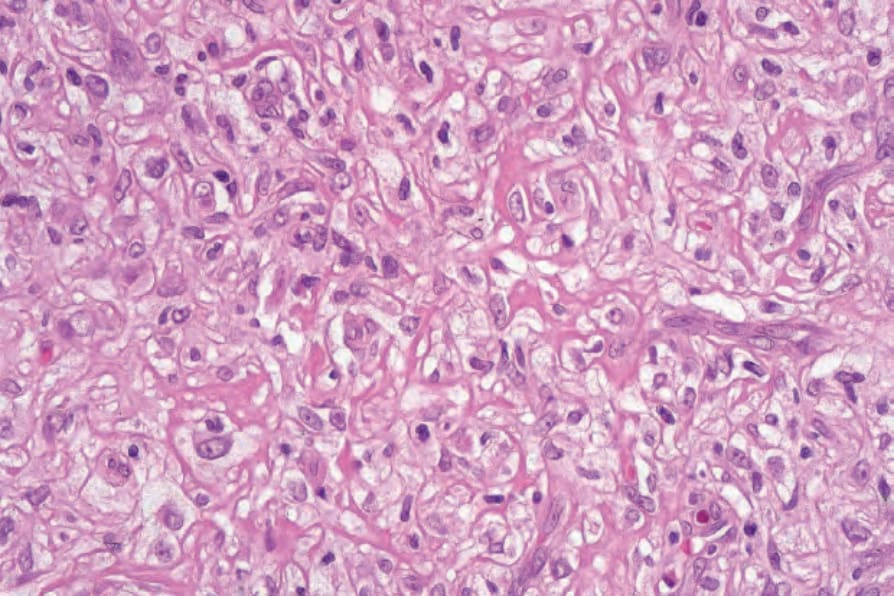
圖 35-246:脂質化(「踝部型」)纖維組織球瘤 (lipidized ‘ankle-type’ fibrous histiocytoma):泡沫狀組織球 (foamy histiocytes) 的高倍視野。By courtesy of R. Carr MD, Warwick Hospital, UK.
Fig. 35.246 Lipidized (‘ankle-type’) fibrous histiocytoma: high-power view of foamy histiocytes. By courtesy of R. Carr MD, Warwick Hospital, UK.
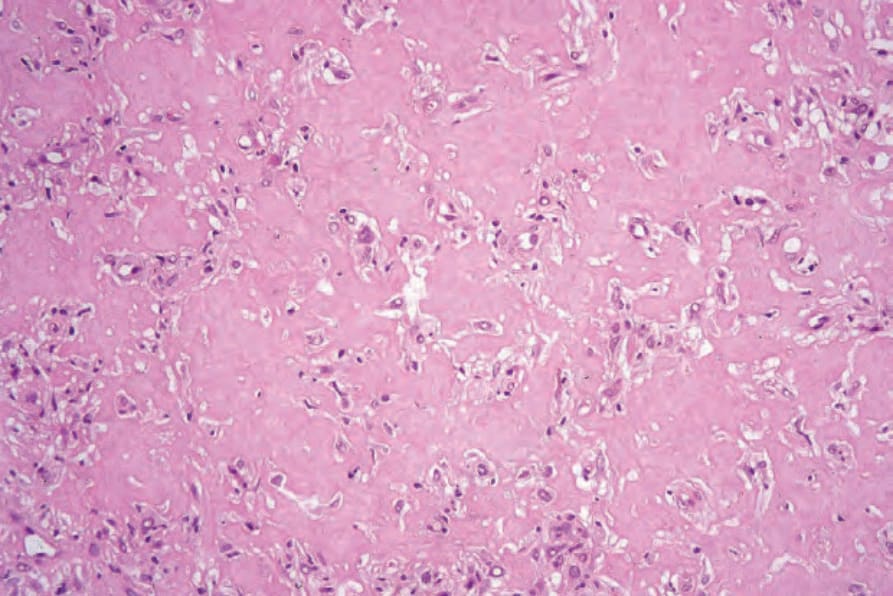
圖 35-247:脂質化(「踝部型」)纖維組織球瘤 (lipidized ‘ankle-type’ fibrous histiocytoma):此視野顯示密集玻璃樣變的膠原,類似類澱粉 (amyloid)。By courtesy of R. Carr MD, Warwick Hospital, UK.
Fig. 35.247 Lipidized (‘ankle-type’) fibrous histiocytoma: this field shows densely hyalinized collagen reminiscent of amyloid. By courtesy of R. Carr MD, Warwick Hospital, UK.
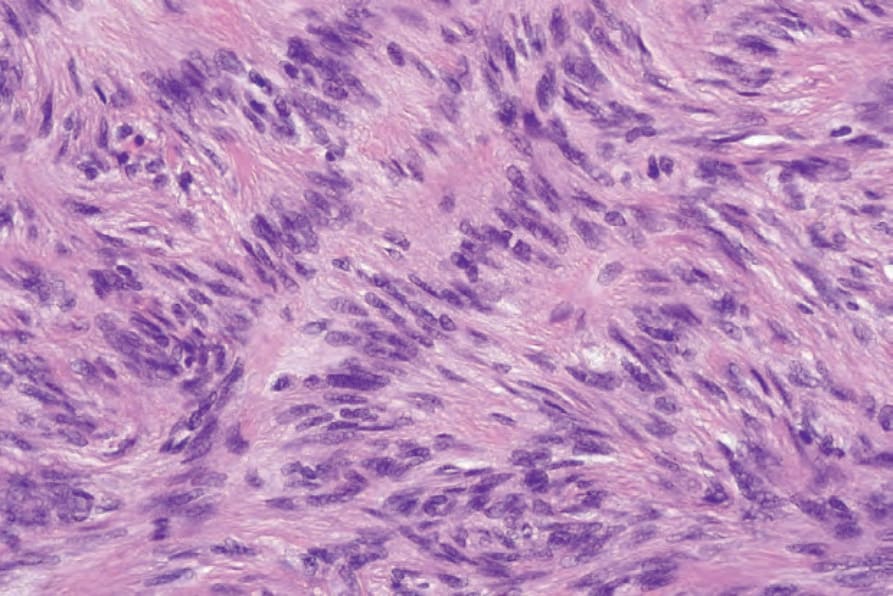
圖 35-249:柵欄狀纖維組織球瘤 (palisading fibrous histiocytoma):高倍視野。
Fig. 35.249 Palisading fibrous histiocytoma: high-power view.
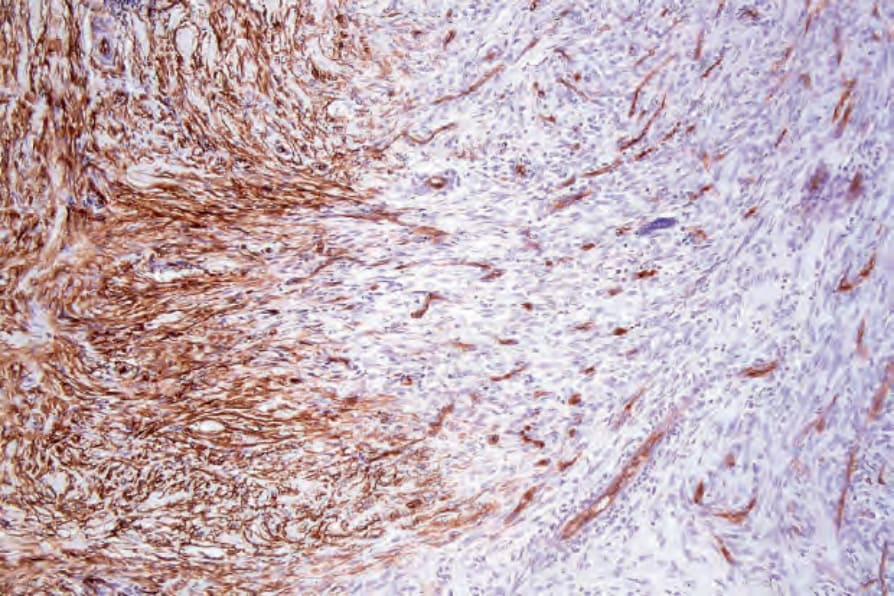
圖 35-230:細胞型纖維組織球瘤 (cellular fibrous histiocytoma):病灶邊緣的腫瘤細胞常表現 CD34。
Fig. 35.230 Cellular fibrous histiocytoma: the tumor cells at the edge of the lesion often express CD34.
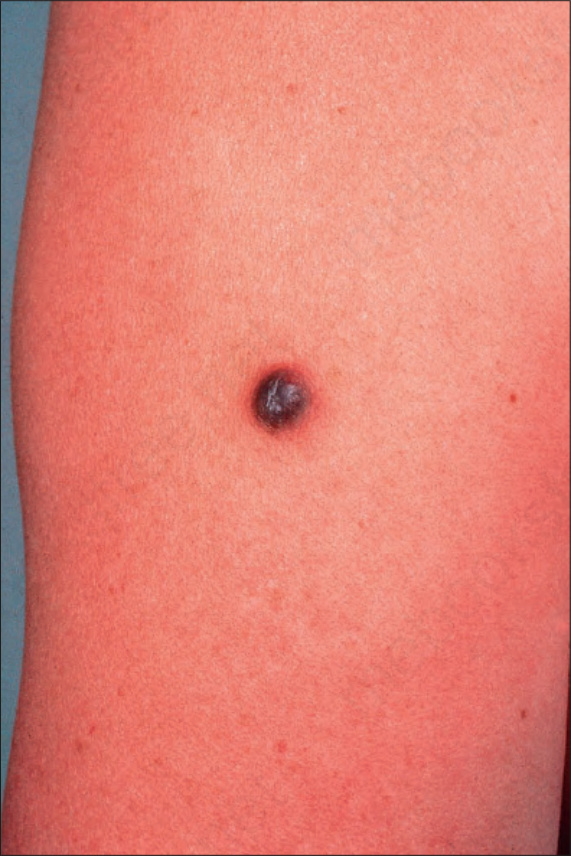
圖 35-231:動脈瘤樣纖維組織球瘤 (aneurysmal fibrous histiocytoma):此病灶表現為出血性結節。By courtesy of the Institute of Dermatology, London, UK.
Fig. 35.231 Aneurysmal fibrous histiocytoma: this lesion presents as a hemorrhagic nodule. By courtesy of the Institute of Dermatology, London, UK.
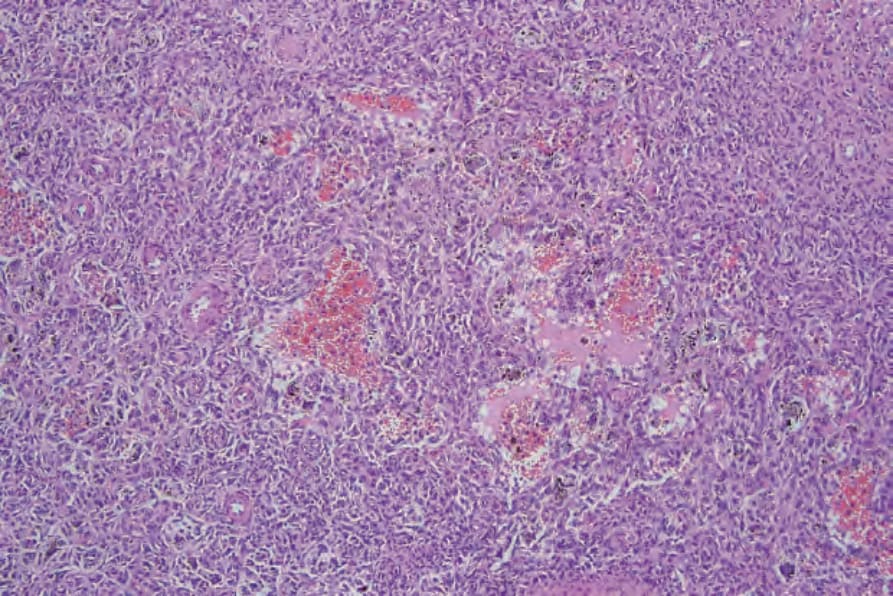
圖 35-232:動脈瘤樣纖維組織球瘤 (aneurysmal fibrous histiocytoma):較深層真皮中存在密集富細胞的浸潤。可見充血的囊狀空間。
Fig. 35.232 Aneurysmal fibrous histiocytoma: a densely cellular infiltrate is present in the deeper dermis. Blood-filled cystic spaces are evident.
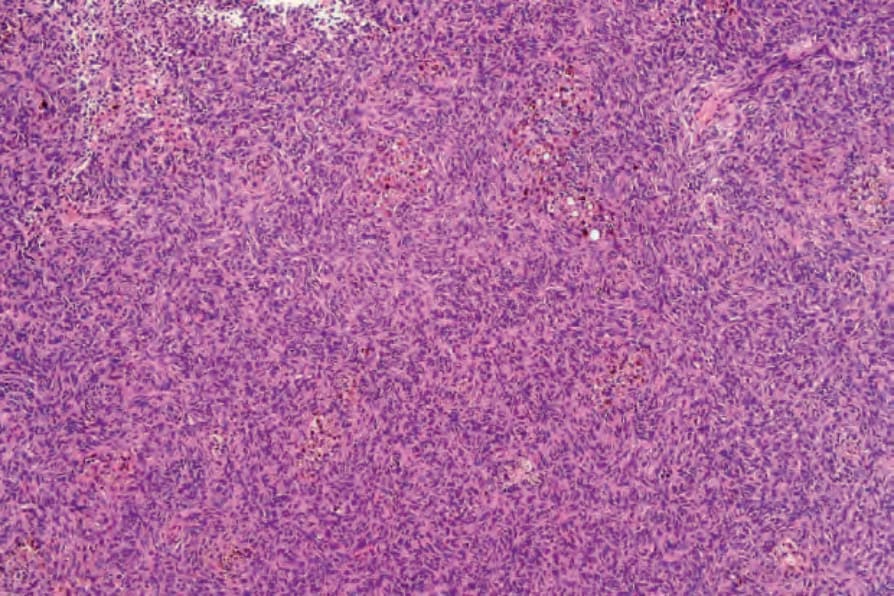
圖 35-234:含鐵血黃素性纖維組織球瘤 (hemosiderotic fibrous histiocytoma):此病灶有時可見的明顯血管增生與大量含鐵血黃素內容,賦予一種暗藍棕色調,臨床上可能造成與 melanoma 的混淆。
Fig. 35.234 Hemosiderotic fibrous histiocytoma: the marked vascularity and heavy hemosiderin content sometimes seen in this lesion gives a dark bluish-brown coloration, which clinically may cause confusion with melanoma.

圖 35-237:上皮樣良性纖維組織球瘤 (epithelioid benign fibrous histiocytoma):此變異型典型表現為紅斑性息肉狀病灶。By courtesy of the Institute of Dermatology, London, UK.
Fig. 35.237 Epithelioid benign fibrous histiocytoma: this variant typically presents as an erythematous polypoid lesion. By courtesy of the Institute of Dermatology, London, UK.
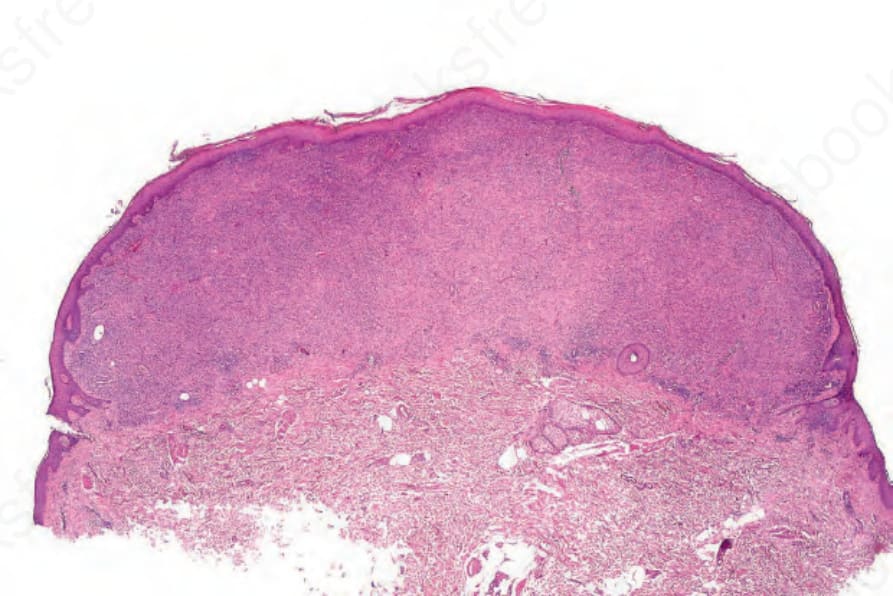
圖 35-238:上皮樣良性纖維組織球瘤 (epithelioid benign fibrous histiocytoma):此低倍視野顯示一淺層腫瘤結節伴一個相關的表皮環領 (epidermal collarette)。
Fig. 35.238 Epithelioid benign fibrous histiocytoma: this low-power view shows a superficial tumor nodule with an associated epidermal collarette.
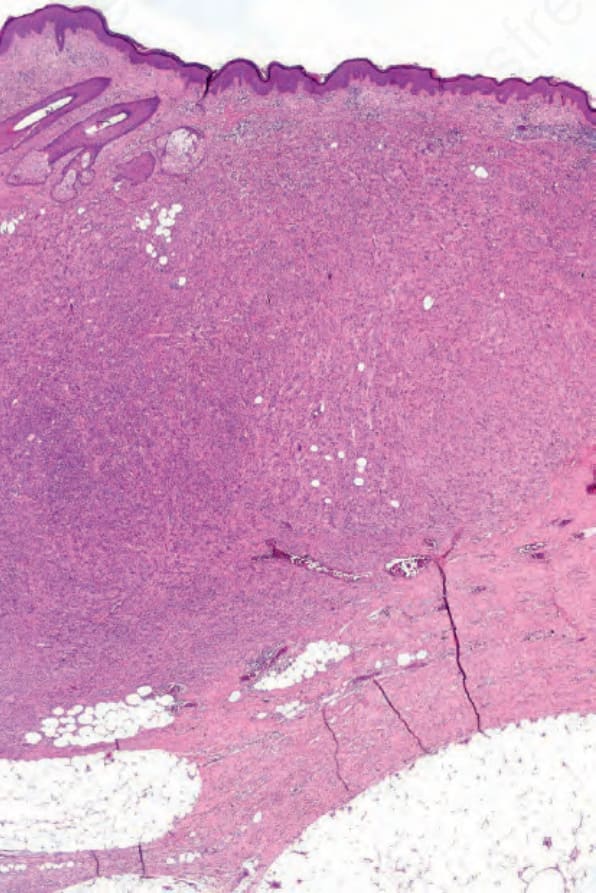
圖 35-243:非典型良性纖維組織球瘤 (atypical benign fibrous histiocytoma):此富細胞病灶延伸至皮下脂肪。
Fig. 35.243 Atypical benign fibrous histiocytoma: this cellular lesion extends into the subcutaneous fat.
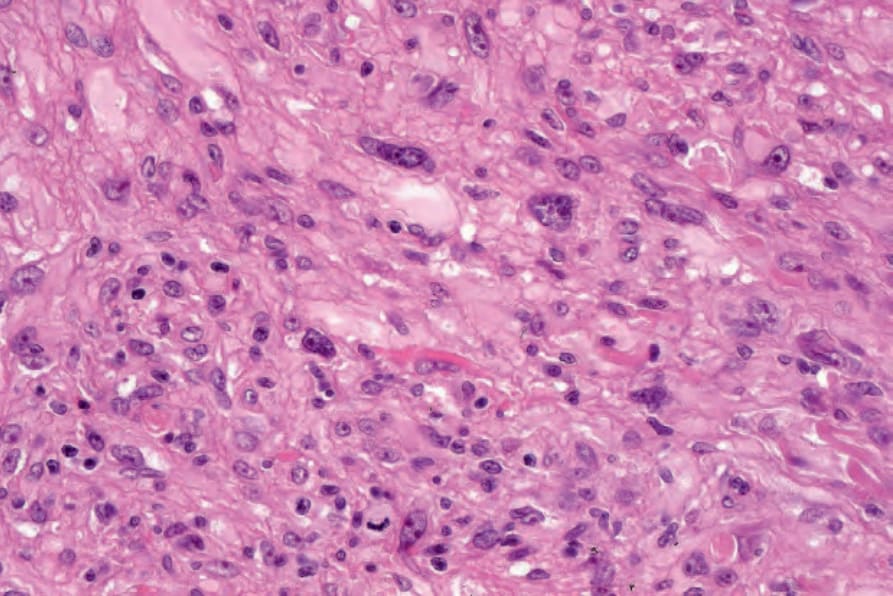
圖 35-244:非典型良性纖維組織球瘤 (atypical benign fibrous histiocytoma):有顯著的核多形性。注意有絲分裂象。protein. 與具上皮樣細胞變化的皮膚周邊神經瘤 (cutaneous perineurioma) 的區別,是藉由後者腫瘤中瀰漫性的 EMA 與 claudin-1 陽性。然而,局部膜性 EMA 陽性是 epithelioid fibrous histiocytoma 的常見發現。66 典型可見 ALK 表現(約 90% 的病例),並與多種夥伴基因(包括 SQSTM1、VCL、TMP3、EML4、PRKAR2A 等)的 ALK 重排相關 (Fig. 35.242)。67–69
Fig. 35.244 Atypical benign fibrous histiocytoma: there is striking nuclear pleomorphism. Note the mitotic figure. protein. Distinction from a cutaneous perineurioma with epithelioid cell change is made by the presence of diffuse EMA and claudin-1 positivity in the latter tumor. However, focal membranous EMA positivity is a frequent finding in epithelioid fibrous histiocytoma.66 ALK expression is typically seen (in roughly 90% of cases) and is correlated with ALK rearrangements with a variety of partner genes including SQSTM1, VCL, TMP3, EML4, PRKAR2A, and others (Fig. 35.242).67–69
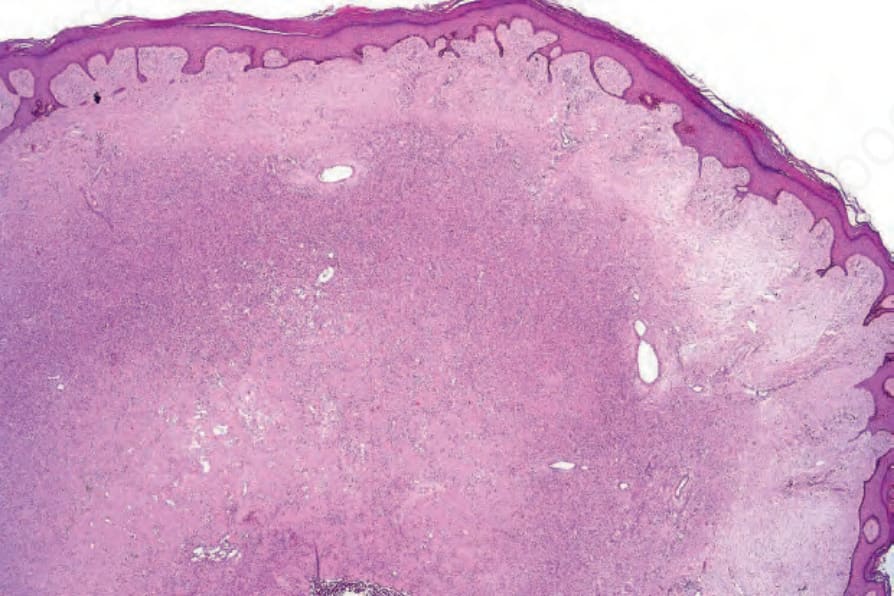
圖 35-245:脂質化(「踝部型」)纖維組織球瘤 (lipidized ‘ankle-type’ fibrous histiocytoma):這是一個獨特的形態學亞群,以黃瘤細胞 (xanthoma cells) 為主,伴顯著的間質玻璃樣變。By courtesy of R. Carr MD, Warwick Hospital, UK.
Fig. 35.245 Lipidized (‘ankle-type’) fibrous histiocytoma: this is a distinctive morphological subset characterized by a predominance of xanthoma cells associated with marked stromal hyalinization. By courtesy of R. Carr MD, Warwick Hospital, UK.
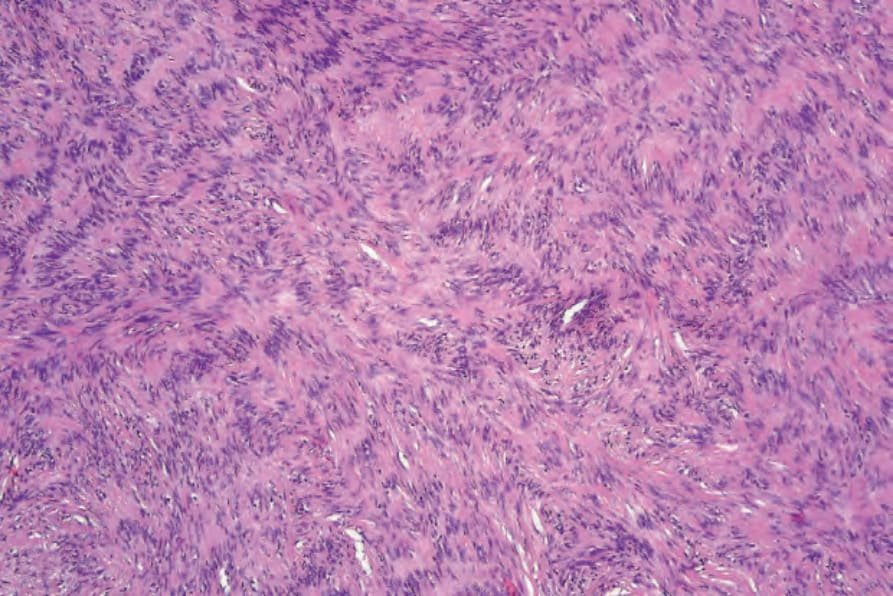
圖 35-248:柵欄狀纖維組織球瘤 (palisading fibrous histiocytoma):偶爾,模擬 Verocay bodies 的柵欄狀排列可為其特徵。
Fig. 35.248 Palisading fibrous histiocytoma: occasionally, palisading mimicking Verocay bodies may be a feature.
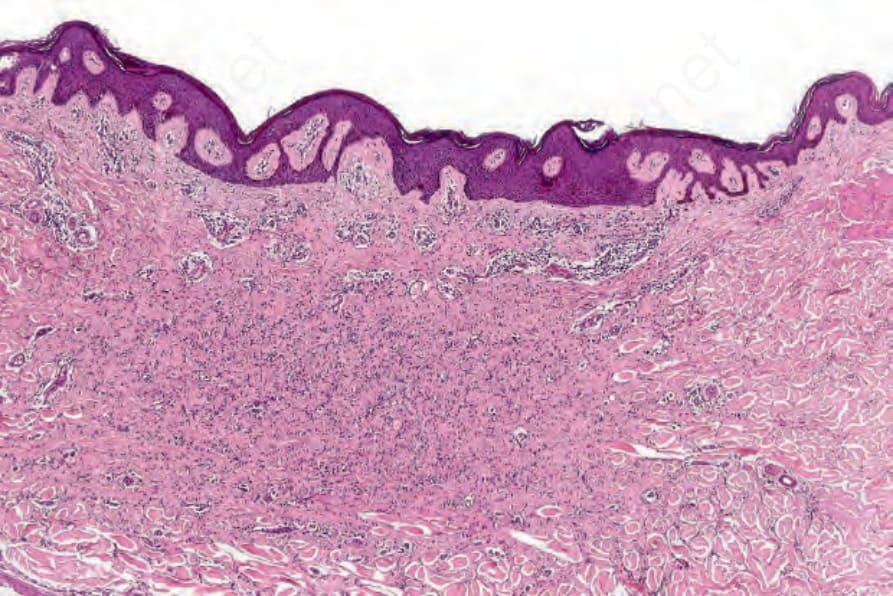
圖 35-250:萎縮性纖維組織球瘤 (atrophic fibrous histiocytoma):此變異型外觀細胞稀少,並與表面上皮平行排列。
Fig. 35.250 Atrophic fibrous histiocytoma: this variant appears hypocellular and orientated parallel to the surface epithelium.