Fibrous histiocytoma (dermatofibroma)
Fibrous histiocytoma (dermatofibroma)
Fibrous histiocytoma (dermatofibroma, sclerosing hemangioma, histiocytoma cutis, nodular subepidermal fibrosis) represents one of the most common benign cutaneous soft tissue tumors.1–5 Over the years a number of variants have been described, and although they essentially highlight specific histologic features that can cause diagnostic confusion, some of them also correlate with characteristic clinical findings and behavior6,7 (see below). However, it must be emphasized that the histologic features of several variants can coexist in the same lesion.8
Clinical features Fibrous histiocytoma occurs most often in the middle aged and shows a slight female predominance. The majority of lesions are located on the limbs or (to a lesser degree) the trunk, and present as small, raised, hyperkeratotic cutaneous nodules usually less than 1 cm in diameter with a reddish-brown surface (Figs 35.207 and 35.208). Giant variants including a plaque-like variant are very rare.9–12.
Pathogenesis and histologic features The pathogenesis is unknown but the lesions are much more common in females and the tumor cells express estrogen receptor alpha, suggesting a possible hormonal etiological role.19 It is not clear whether it is a reactive or neoplastic condition.17,20
The epidermis appears unremarkable. In the superficial and mid dermis there is a proliferation of small, thin-walled vascular channels, each of which is surrounded by a layer of pericytes (Fig. 35.204). The surrounding dermis contains scattered multinucleate cells with angulated cytoplasm and a background of somewhat hyalinized collagen bundles (Figs 35.205 and 35.206). Occasional lymphocytes are also seen. An exceptional case with enlarged dermal nerves has been identified.21 Hemosiderin deposition may be present.
The multinucleate cells are positive for CD68 and lysozyme while the interstitial cells may be positive for factor XIIIa.7,21
A significant proportion of cases are said to be associated with previous minor local trauma, especially insect bites. They are slow growing and painless, and may sometimes be multiple. Eruptive lesions have been documented in the context of immunosuppression, HIV infection and highly active antiretroviral therapy (HAART).13–19
Simple excision is usually curative and local recurrence is exceptional except for some of the variants (see below) and in lesions occurring on the face, where the reported rate of local recurrence is 20%.20 In some variants (e.g., atypical, aneurysmal, and cellular fibrous histiocytoma) and exceptional classic tumors, rare metastases have been reported.21–28
A small subgroup of these lesions originates in subcutaneous fat or in deeper structures (deep benign fibrous histiocytoma).29,30
Most fibrous histiocytomas show a typical dermoscopy pattern (peripheral delicate pigment network and a central white scar-like patch) but atypical patterns may mimic melanoma, vascular tumors, basal cell carcinoma, a collision tumor and even psoriasis.31
1760 Connective tissue tumors
Pathogenesis and histologic features For years, it was suggested that dermatofibroma represents a reactive process. Possible etiological associations included insect bites and even trauma such as body-piercing.32 In later years it has become clear that the lesion represents a neoplastic process. Clinical evidence supporting the latter includes the following: tumors do not tend to regress spontaneously, in some variants there is variable potential for local recurrence, and a small number of cases have metastasized.21–28,33 Cytogenetic analysis has provided further support to this theory. Clonality has been demonstrated in some examples of cellular fibrous histiocytoma.34,35 More recently, further studies have demonstrated genetic aberrations by FISH analysis and RNA sequencing in rare examples of subsets of cutaneous fibrous histiocytoma (cellular and aneurysmal) and very exceptionally in regular lesions and deep fibrous histiocytoma.36,37 Rearrangements of the protein kinase C genes (PRKCB and PRKCD) are seen in regular, epithelioid, cellular, and aneurysmal fibrous histiocytoma, and ALK rearrangements are only seen in the epithelioid variant.37 Rearrangements of PRKC and ALK are mutually exclusive events; overexpression of these genes drives promoter swapping with a considerable variety of other gene fusion partners including LAMTOR1, PDPN and CD63. In another study,
DNA copy number changes by comparative genomic hybridization were detected in metastatic tumors and rare cases of nonmetastatic atypical and cellular variants.27,38 The chromosomal aberrations were higher in metastatic cases resulting in death. With regards to aneurysmal fibrous histiocytoma, a translocation t(12;19)(p12;q13) was described and a pathogenetic role for LAMTOR1-PRKCD and NUMA1-SFMBT1 has been suggested.39,40
The common variant is an ill-defined dermal lesion that may extend into superficial subcutaneous fat (Figs 35.209–35.213). It is largely composed of interlacing fascicles of slender spindled cells, sometimes in a focal storiform arrangement, set within a loose collagenous or (less often) myxoid stroma. Scattered between the spindled cells are foamy histiocytes, multinucleated giant cells and thin-walled blood vessels (Figs 35.214–35.217). Foci of chronic inflammatory cells, including lymphocytes and plasma cells, and hemosiderin deposition are frequently seen. A typical feature is the presence of individual hyaline collagen bundles surrounded by tumor cells in the periphery of the lesions.
Long-standing lesions show progressive hyalinization and decreased cellularity and are usually referred to as sclerosing or atrophic dermatofibroma.
All of these tumors, including the variants, may be associated with acanthosis or even pseudoepitheliomatous hyperplasia of the overlying epidermis
1761 Benign fibrohistiocytic tumors and tumorlike lesions
1762 Connective tissue tumors
and hyperpigmentation of the basal cell layer (Figs 35.218 and 35.219). It has been suggested that epidermal growth factor may play a role in the pathogenesis of the epidermal hyperplasia.41 A grenz zone of papillary dermal sparing is usually present (Fig. 35.220). Changes simulating seborrheic keratosis are common, followed by proliferation of clear cells mimicking a clear cell acanthoma, and proliferation of immature hair follicle-like structures closely resembling a trichoblastoma, and induction of sebaceous glands sometimes in a reticulate pattern (Fig. 35.221) 42,43 Mature hair follicles are rarely induced and more unusual epidermal changes including, epidermolytic hyperkeratosis, focal acantholysis and even Bowen disease, have also been described.44,45 Most cases reported as basal cell carcinoma overlying dermatofibroma actually represent reactive induction of immature follicular structures rather than collision tumors.
of fibrous histiocytoma where focal positivity for this marker may be seen (see below). D2–40 is diffusely positive in dermatofibromas and only very focally positive or negative in dermatofibrosarcoma protuberans.47
Common dermatofibroma is usually easy to diagnose and problems with differential diagnosis generally only arise with its variants.48
A proportion of tumors, especially the cellular variant, stain focally for α-SMA and calponin, suggesting myofibroblastic differentiation (Fig. 35.222). It has been proposed that this lesion arises from a fixed dermal connective tissue cell, the dermal dendrocyte, which stains positively for factor XIIIa.46 Although a number of cells within fibrous histiocytomas react with this marker, especially towards the edges of the lesion, these appear to be reactive cells and not true tumor cells. In contrast to dermatofibrosarcoma, CD34 expression is not usually a feature except in the cellular variant
Variants of dermatofibroma include:
• cellular fibrous histiocytoma,
• aneurysmal fibrous histiocytoma,
• epithelioid fibrous histiocytoma,
• atypical (pseudosarcomatous) fibrous histiocytoma,
• lipidized (‘ankle-type’) fibrous histiocytoma,
• clear cell fibrous histiocytoma,
• palisading cutaneous fibrous histiocytoma,
• atrophic dermatofibroma. It is important to note that all variants of dermatofibroma except the epithelioid variant may overlap histologically.
Cellular fibrous histiocytoma Cellular benign fibrous histiocytoma accounts for almost 5% of cutaneous fibrous histiocytomas.48–50 It is most common in young adults, especially males, and has a predilection for the limbs and head and neck area (Figs
1763 Benign fibrohistiocytic tumors and tumorlike lesions
35.223 and 35.224). These lesions are larger than common fibrous histiocytoma and have a high recurrence rate of up to 26%. Metastasis to regional lymph nodes, soft tissues and lungs has been reported in a small number of cases.22–28 Development of satellite nodules has also been described.26 In a further case, erosion of the phalanx occurred.51 Histologic features do not allow prediction of those cases that ultimately metastasize.26 Cases that may be more likely to metastasize appear to be those that recur early and on multiple occasions.
Histologically, lesions are highly cellular with a more prominent fascicular growth pattern (Figs 35.225–35.228). Frequently there is involvement of the superficial subcutis. Tumor cells tend to have more abundant eosinophilic cytoplasm, and normal mitotic figures are common (Fig. 35.229). Central necrosis is seen in some cases (about 10%). A pleomorphic sarcoma component has been described in a case of primary cellular fibrous histiocytoma and in a recurrent tumor.27
Immunohistochemistry shows variable (usually focal) staining for SMA (in most cases) and calponin and negative or only focal staining for CD34
1764 Connective tissue tumors
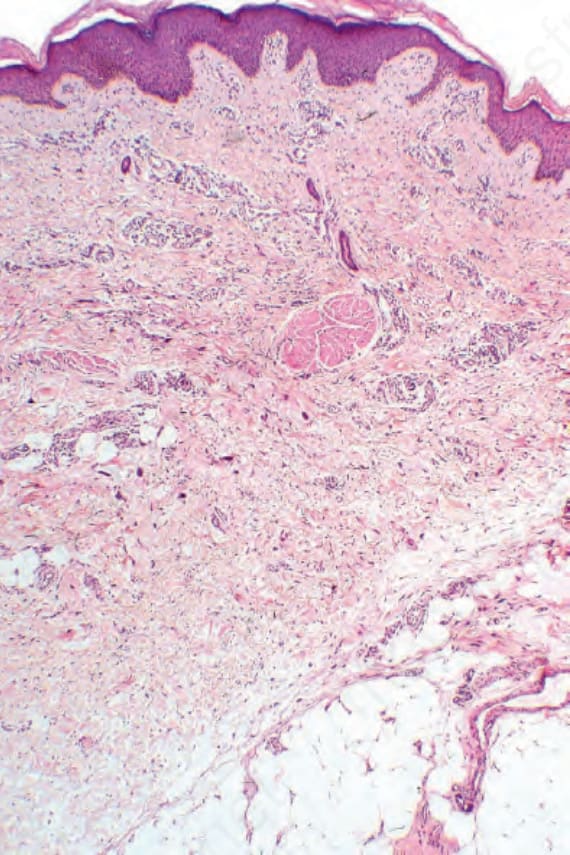
Fig. 35.204 Multinucleate cell angiohistiocytoma: within the dermis is a vascular and collagenous proliferative lesion with conspicuous multinucleate giant cells.
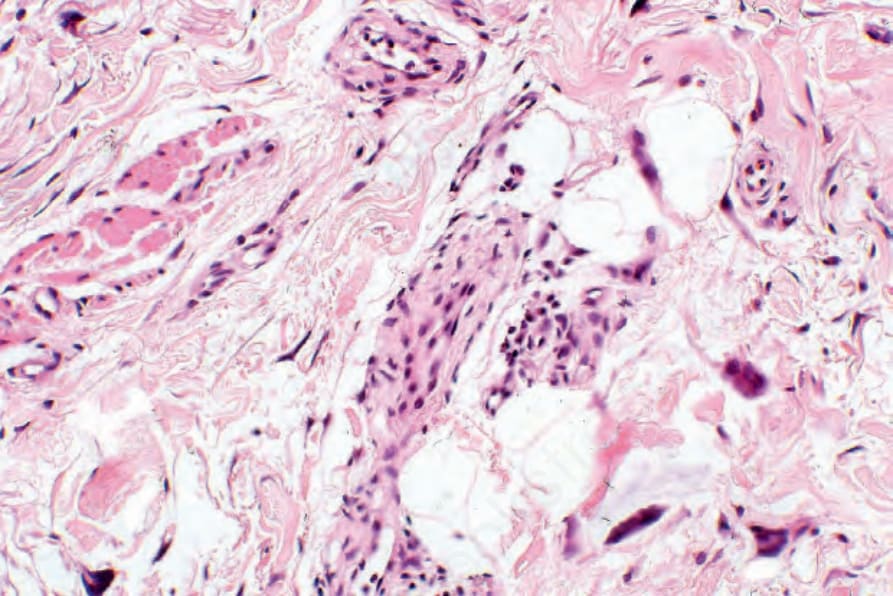
Fig. 35.205 Multinucleate cell angiohistiocytoma: medium-power view showing vessels with giant cells and pericytes.

Fig. 35.207 Fibrous histiocytoma (dermatofibroma): this tumor most often presents as an erythematous raised lesion. Surface scaling is not uncommon. From the collection of the late N.P. Smith, MD, The Institute of Dermatology, London, UK.

Fig. 35.208 Fibrous histiocytoma (dermatofibroma): dark brown (due to hemosiderin deposition) lesions are sometimes mistaken for melanocytic tumors, including melanoma. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
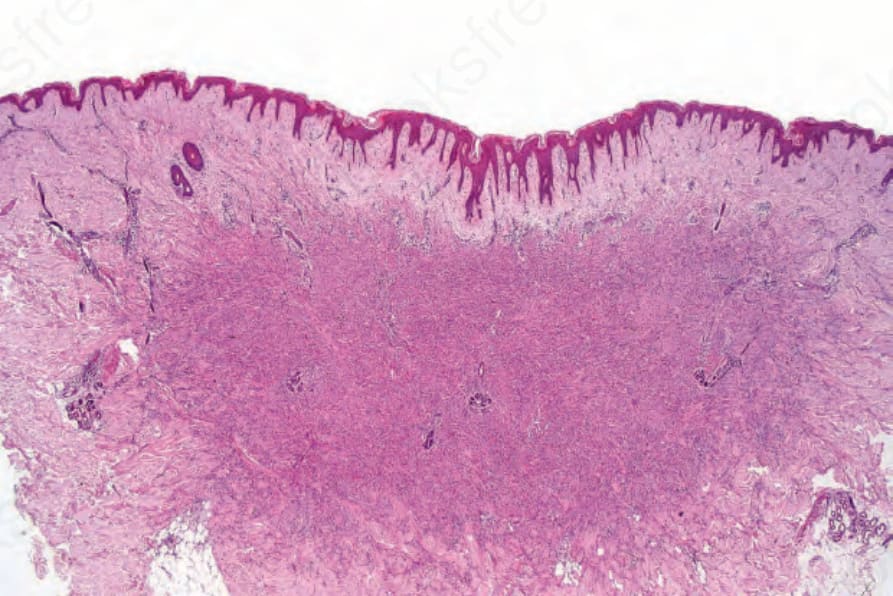
Fig. 35.209 Fibrous histiocytoma (dermatofibroma): scanning section showing the characteristic architecture. The lateral borders of the lesion interdigitate with the adjacent dermis. There is hyperkeratosis and acanthosis of the overlying epidermis.
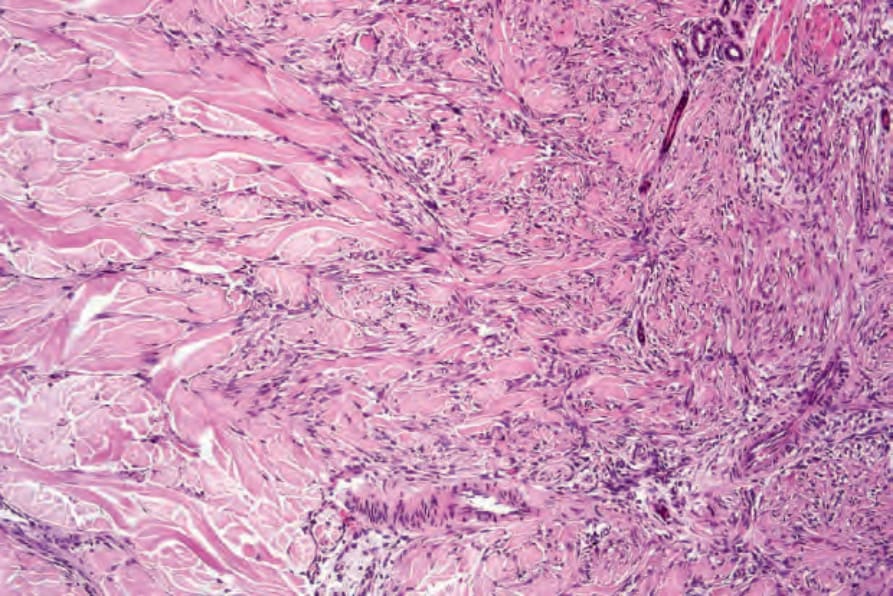
Fig. 35.210 Fibrous histiocytoma (dermatofibroma): the tumor extends into the adjacent normal dermis.
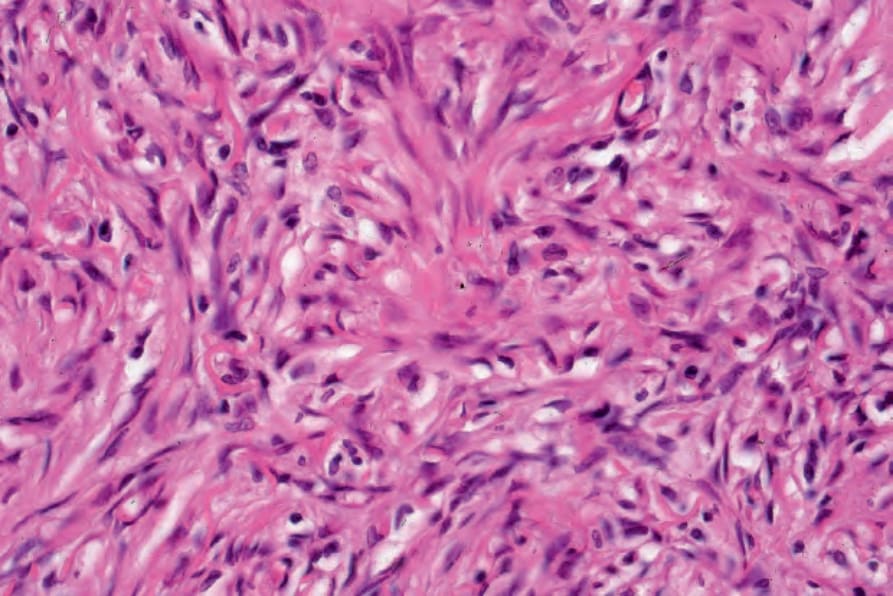
Fig. 35.211 Fibrous histiocytoma (dermatofibroma): high-power view showing storiform growth pattern.
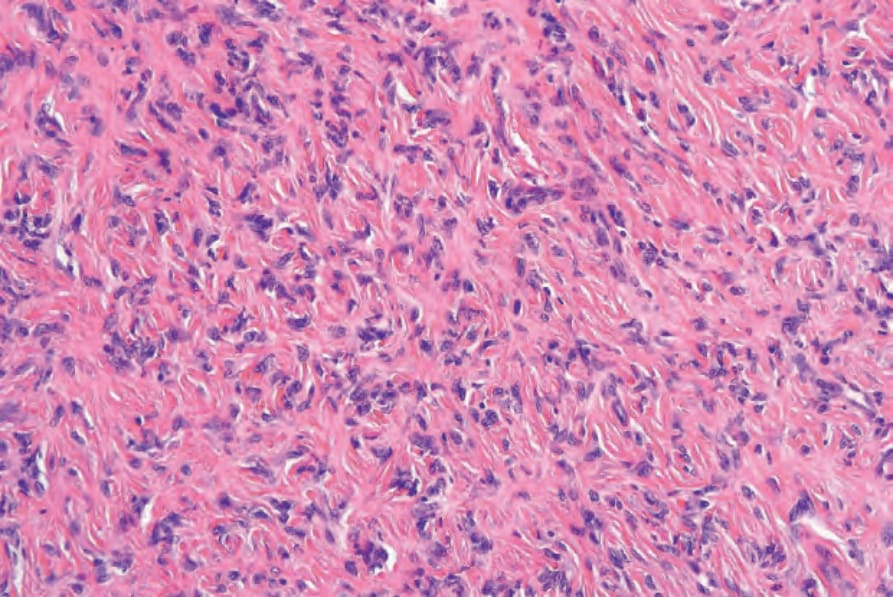
Fig. 35.212 Fibrous histiocytoma (dermatofibroma): the tumor is composed of uniform, interlacing spindle cells in a vaguely curlicue pattern embedded in a hyaline collagenous stroma.
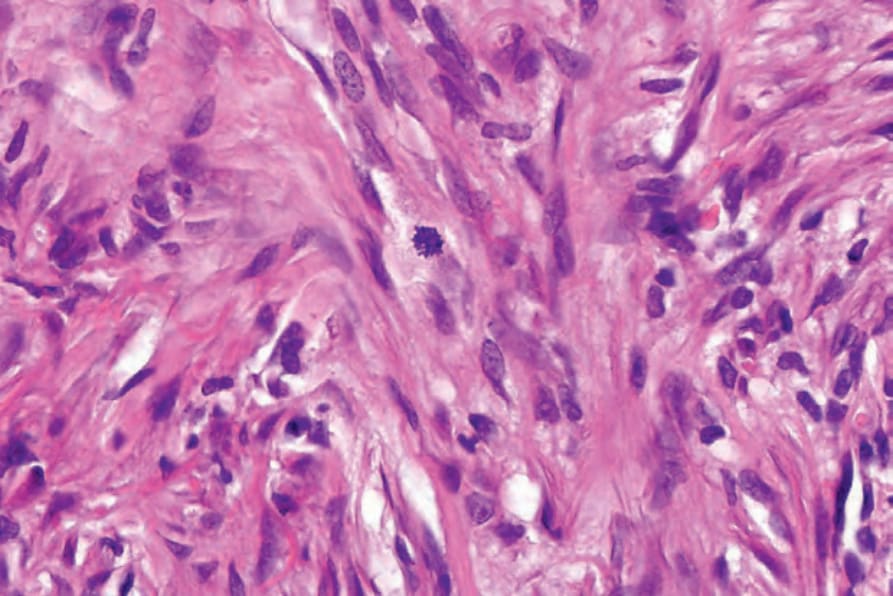
Fig. 35.213 Fibrous histiocytoma (dermatofibroma): occasional normal mitotic figures may be seen.
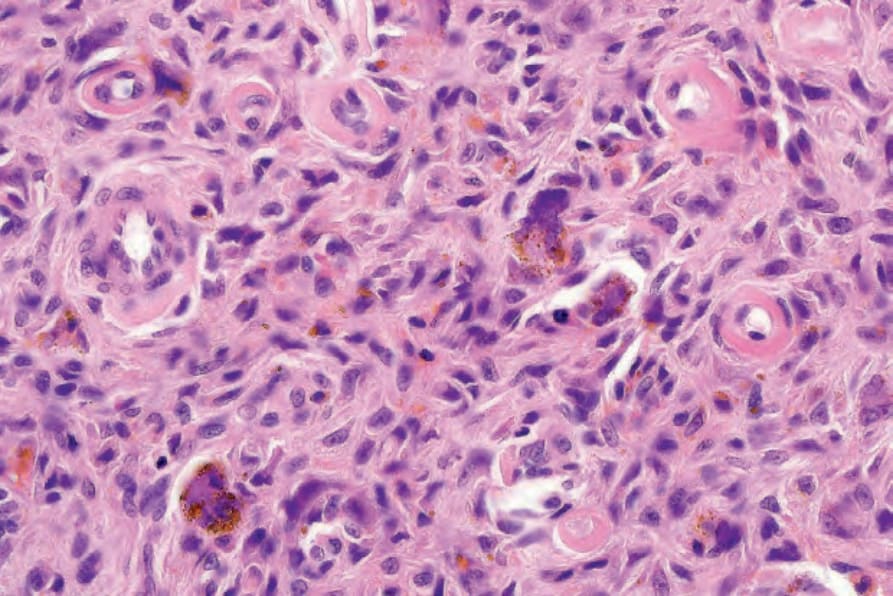
Fig. 35.214 Fibrous histiocytoma (dermatofibroma): scattered multinucleated giant cells are a not infrequent feature of this lesion. Note the hemosiderin pigment.
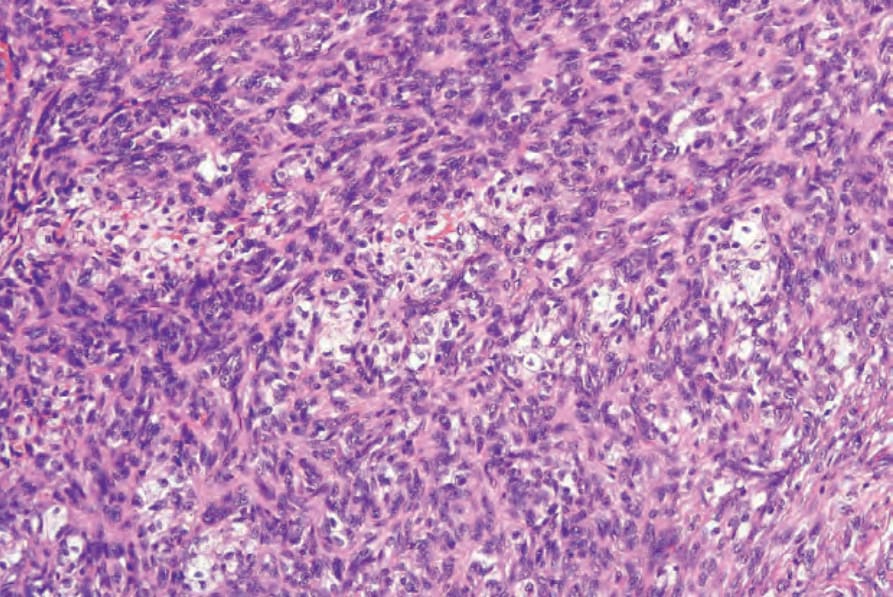
Fig. 35.215 Fibrous histiocytoma (dermatofibroma): lipid-laden histiocytes are commonly present.
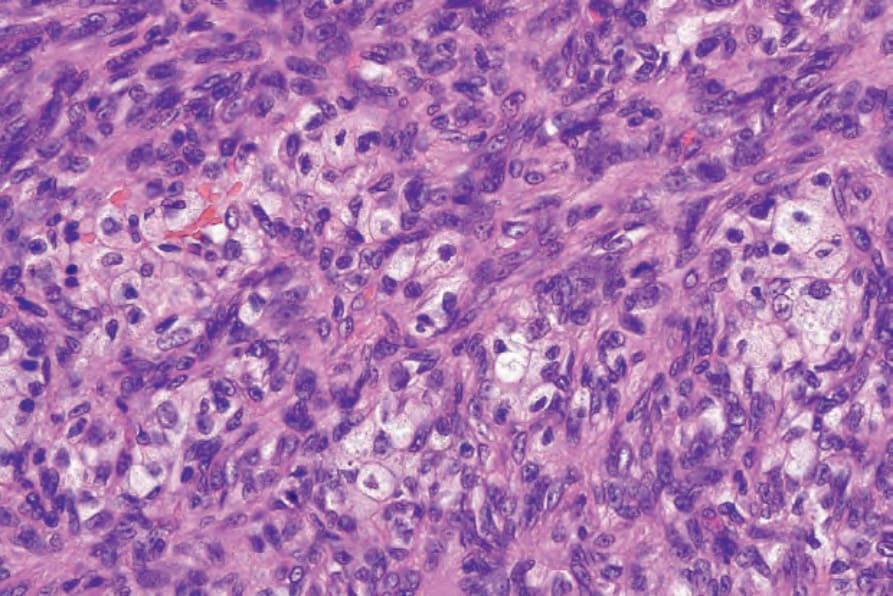
Fig. 35.216 Fibrous histiocytoma (dermatofibroma): high-power view.
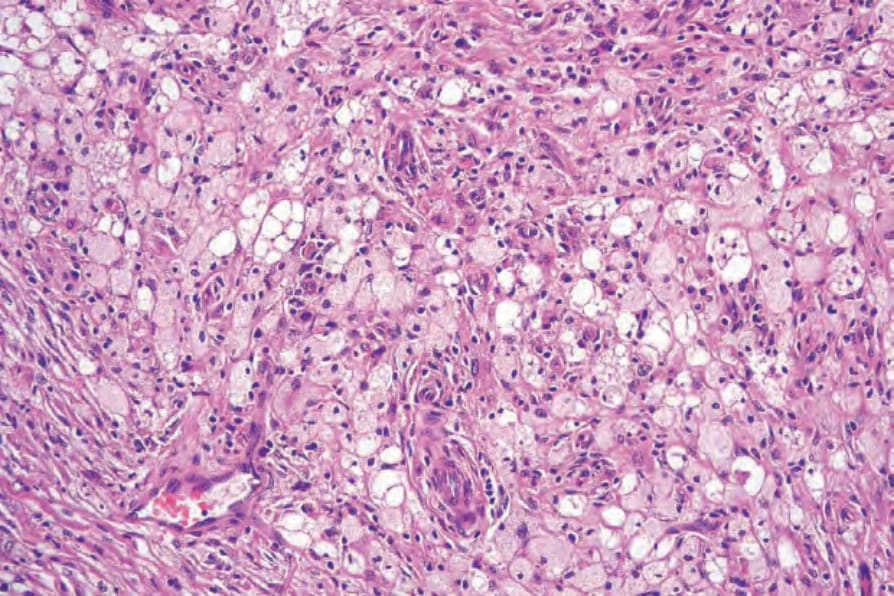
Fig. 35.217 Fibrous histiocytoma (dermatofibroma): when the lipid-laden histiocytes are numerous, this lesion is sometimes called histiocytoma cutis.
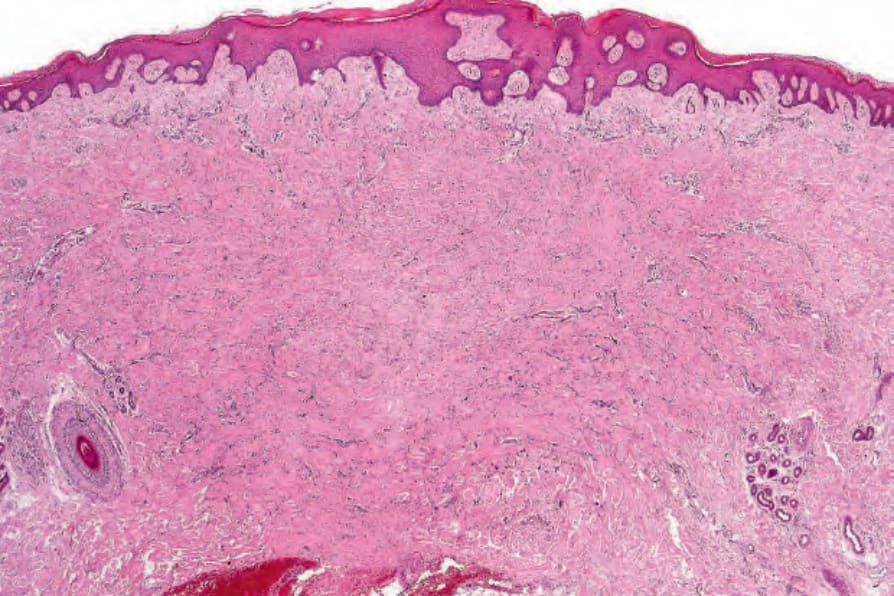
Fig. 35.218 Fibrous histiocytoma (dermatofibroma): the epithelium overlying the tumor is often acanthotic.
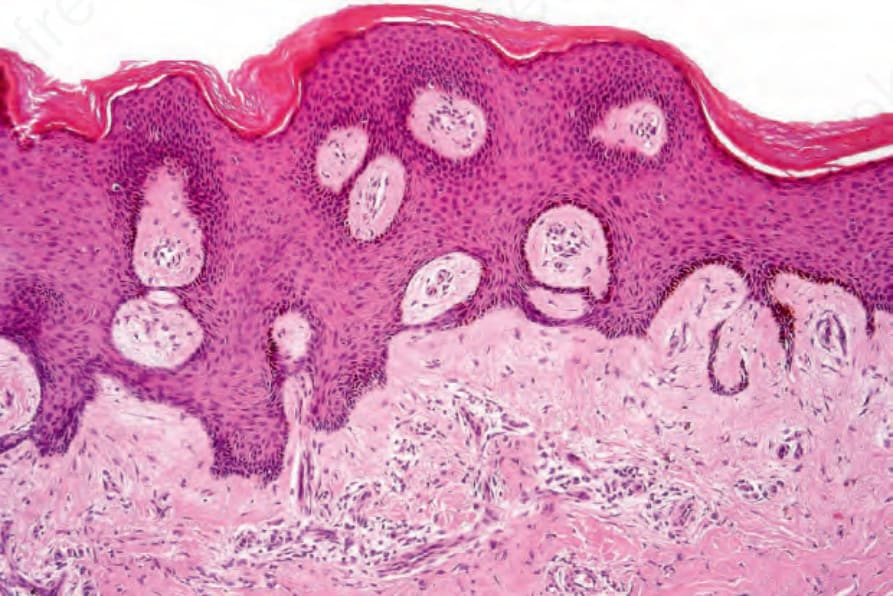
Fig. 35.219 Fibrous histiocytoma (dermatofibroma): the tumor is often separated from the epidermis by a grenz zone.
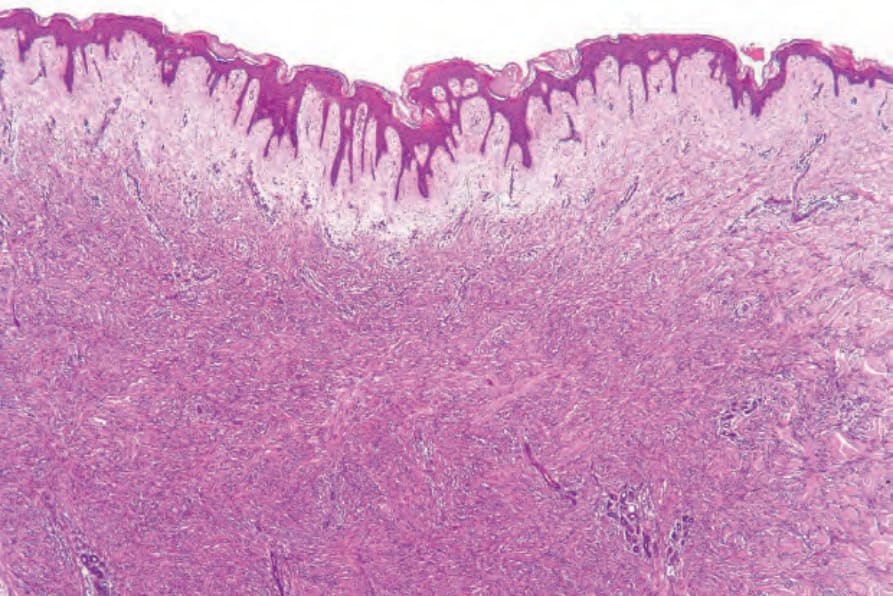
Fig. 35.220 Fibrous histiocytoma (dermatofibroma): in this example, there is an extensive grenz zone.
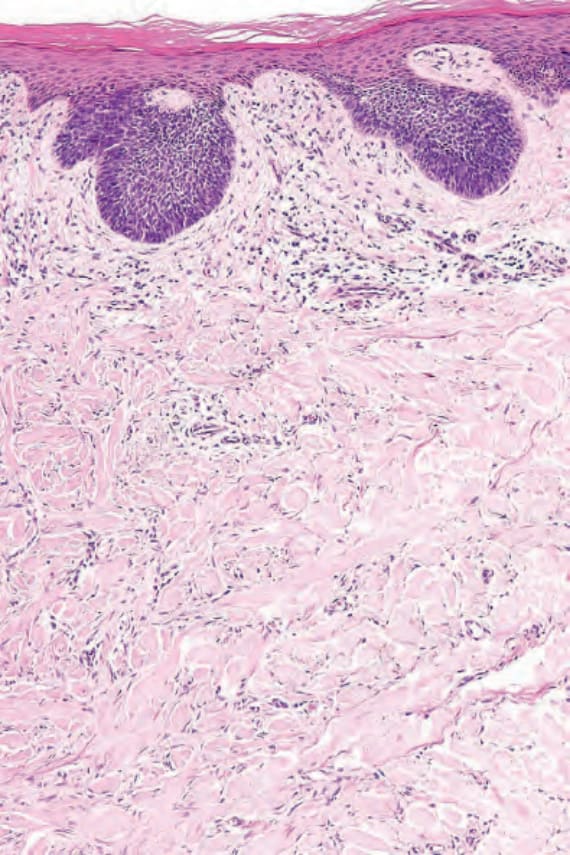
Fig. 35.221 Fibrous histiocytoma (dermatofibroma): proliferation of basaloid cells reminiscent of trichoblastoma.
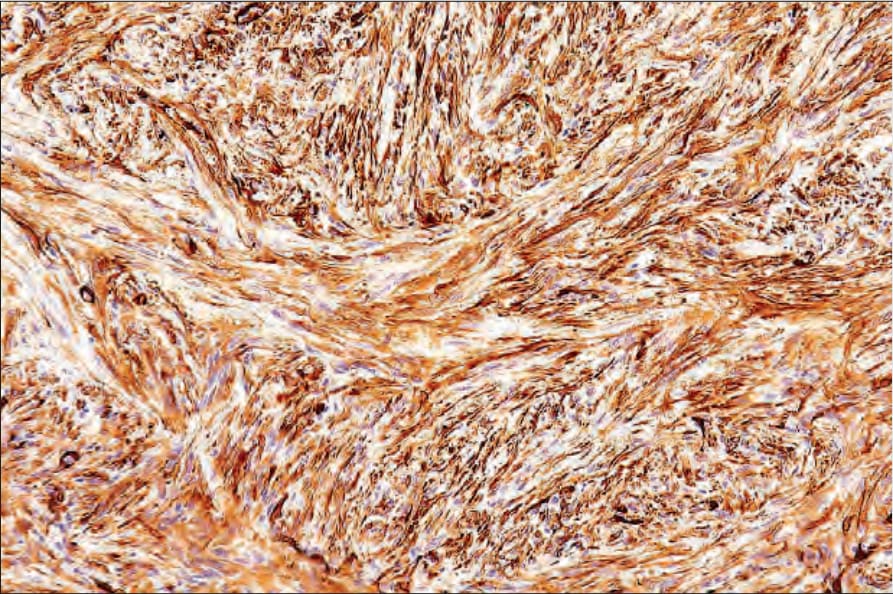
Fig. 35.222 Fibrous histiocytoma (dermatofibroma): this example shows strong smooth muscle actin expression.

Fig. 35.223 Cellular fibrous histiocytoma: tumors may be large and sometimes present at unusual sites, as in this example. By courtesy of the Institute of Dermatology, London, UK.

Fig. 35.224 Cellular fibrous histiocytoma: children may rarely be affected. Ulceration is sometimes a feature. By courtesy of the Institute of Dermatology, London, UK.
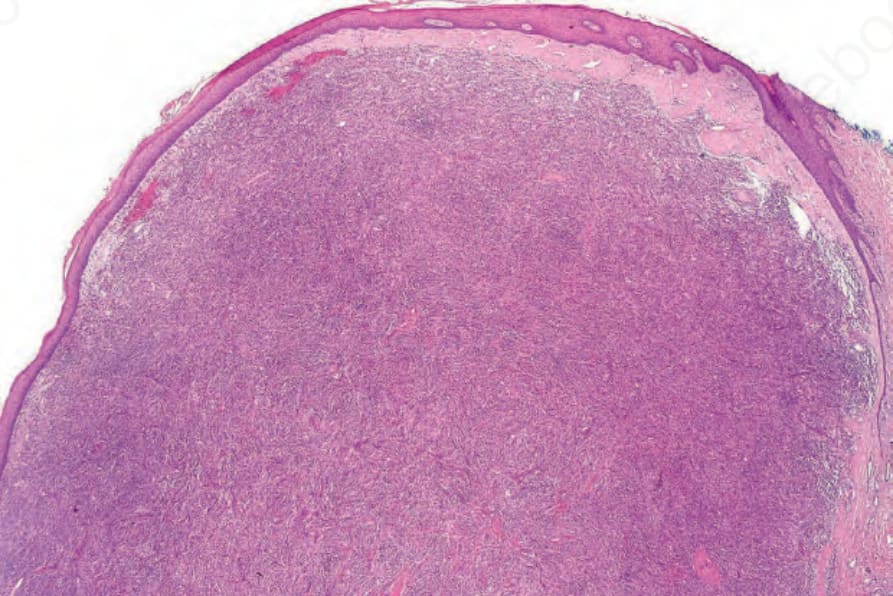
Fig. 35.225 Cellular fibrous histiocytoma: this variant of dermatofibroma is often a source of diagnostic confusion. It is larger than the conventional form and appears more cellular and mitotically active.
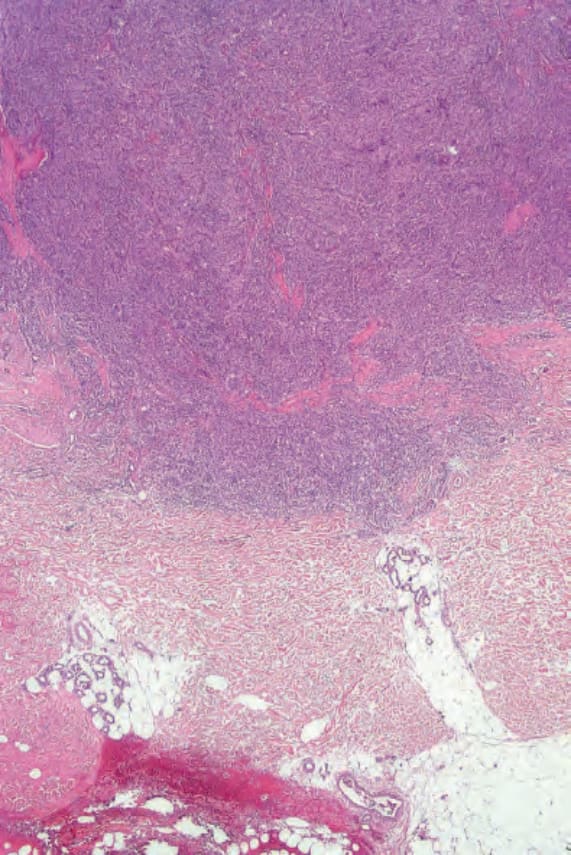
Fig. 35.226 Cellular fibrous histiocytoma: scanning view showing extension into the deep reticular dermis.
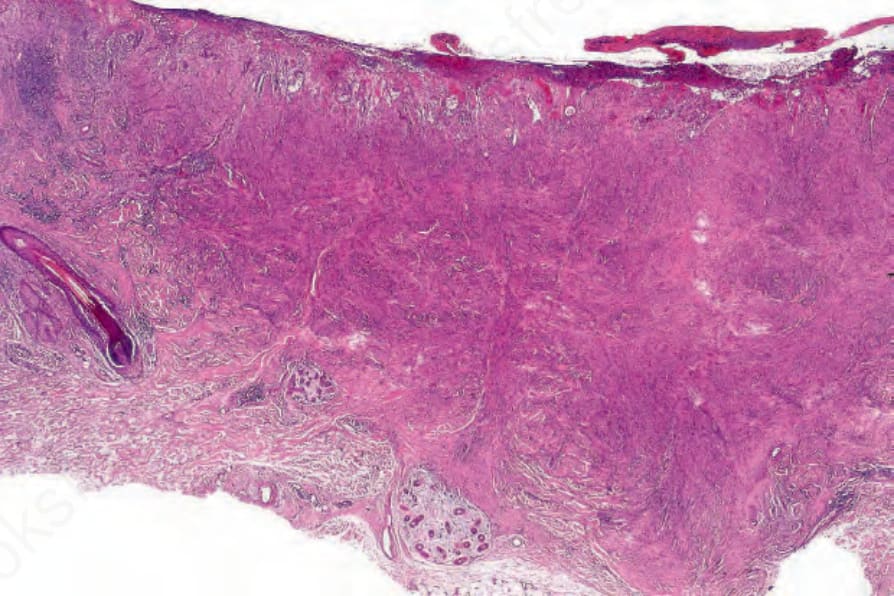
Fig. 35.227 Cellular fibrous histiocytoma: this example shows striking cellularity.
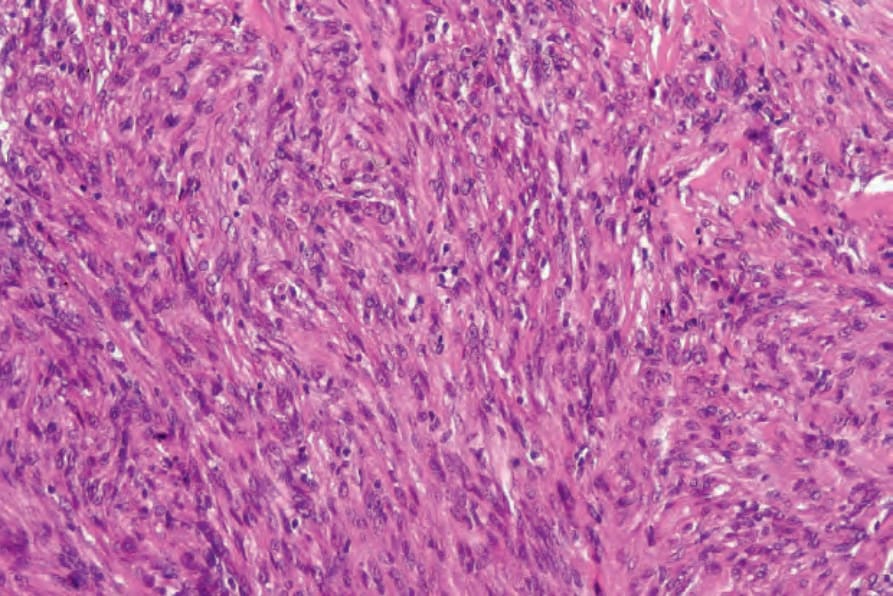
Fig. 35.228 Cellular fibrous histiocytoma: high-power view of Figure 35.226
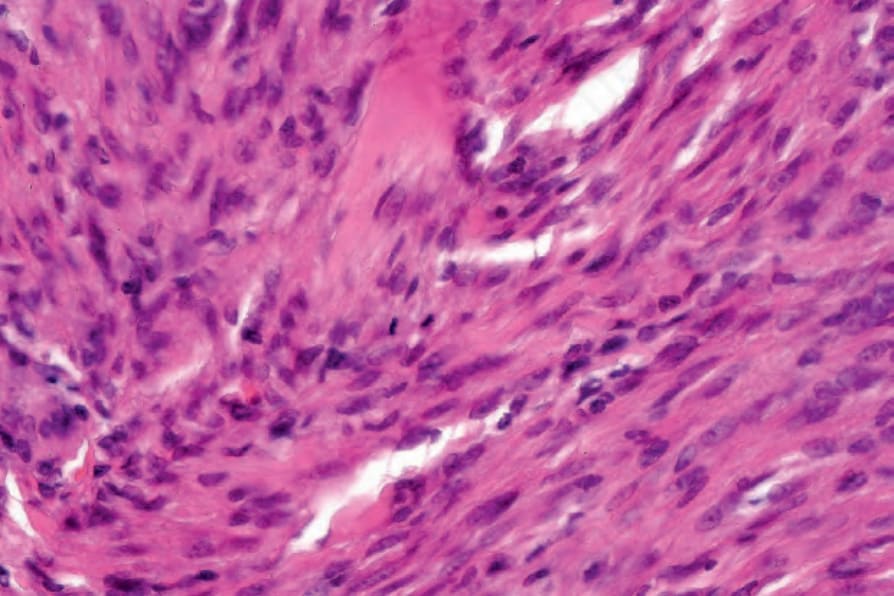
Fig. 35.229 Cellular fibrous histiocytoma: note the mitotic activity.
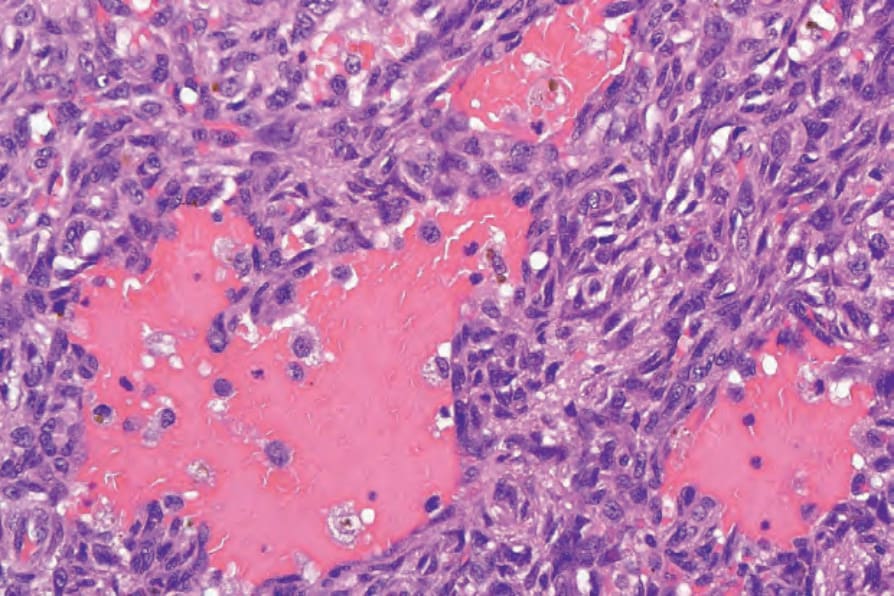
Fig. 35.233 Aneurysmal fibrous histiocytoma: the hemorrhagic spaces are devoid of an endothelial lining.
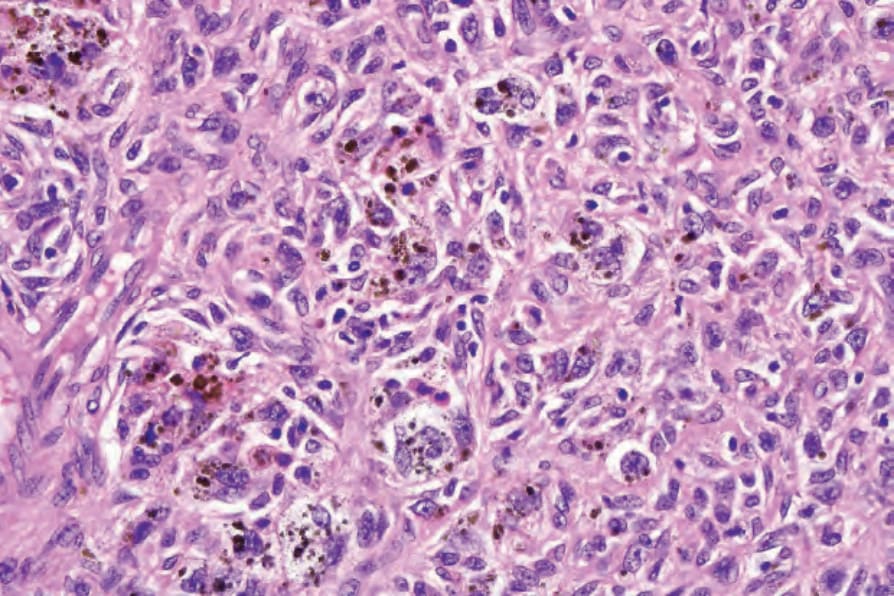
Fig. 35.235 Hemosiderotic fibrous histiocytoma: this variant is also sometimes known as sclerosing hemangioma.
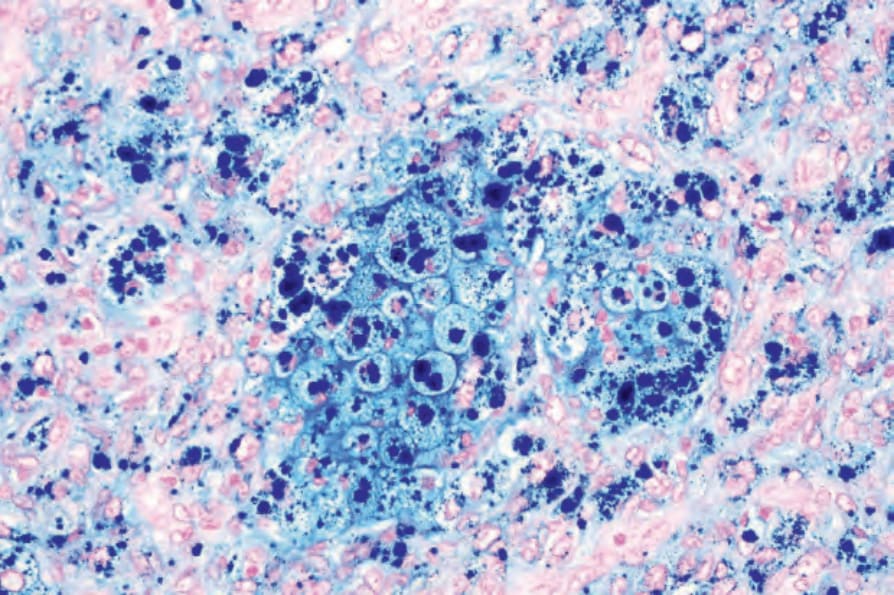
Fig. 35.236 Hemosiderotic fibrous histiocytoma: a Perl stain highlights the hemosiderin.
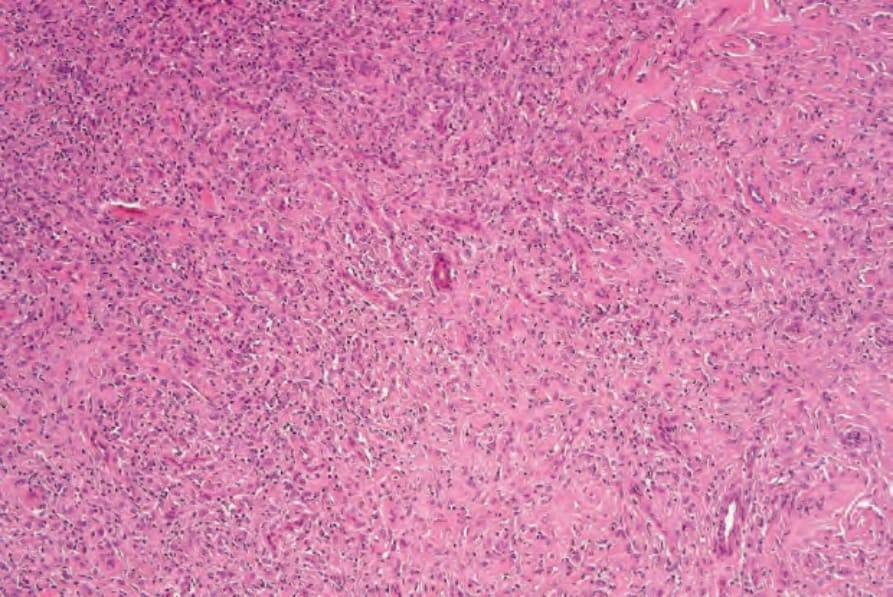
Fig. 35.239 Epithelioid benign fibrous histiocytoma: the tumor is composed of large cells with abundant eosinophilic cytoplasm. The infiltrate is uniform, in contrast to the more typical variant. Often, conventional features are identifiable elsewhere in the specimen.
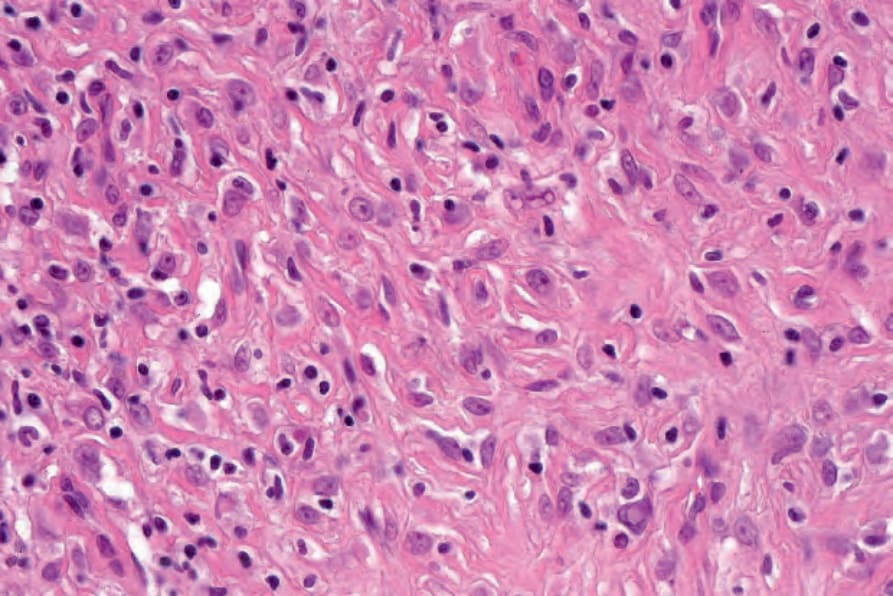
Fig. 35.240 Epithelioid benign fibrous histiocytoma: high-power view.
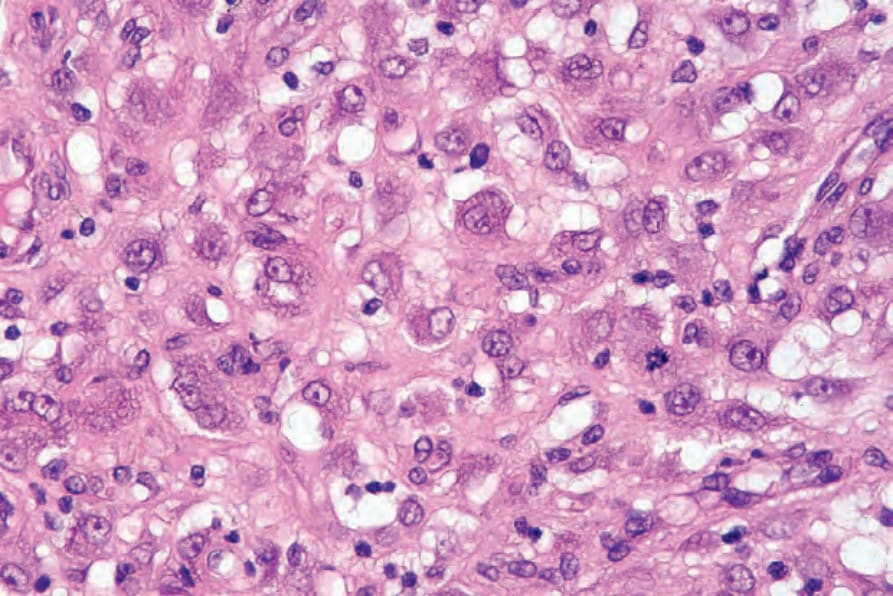
Fig. 35.241 Epithelioid benign fibrous histiocytoma: occasional normal mitotic figures may be present.
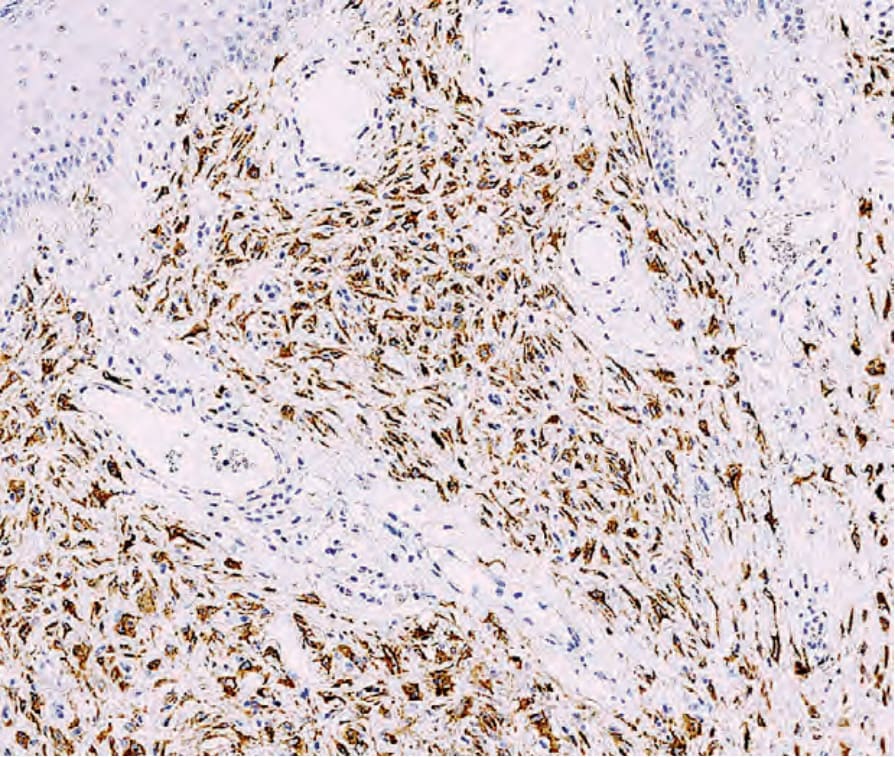
Fig. 35.242 Epithelioid benign fibrous histiocytoma: the tumor cells are often positive for ALK1.
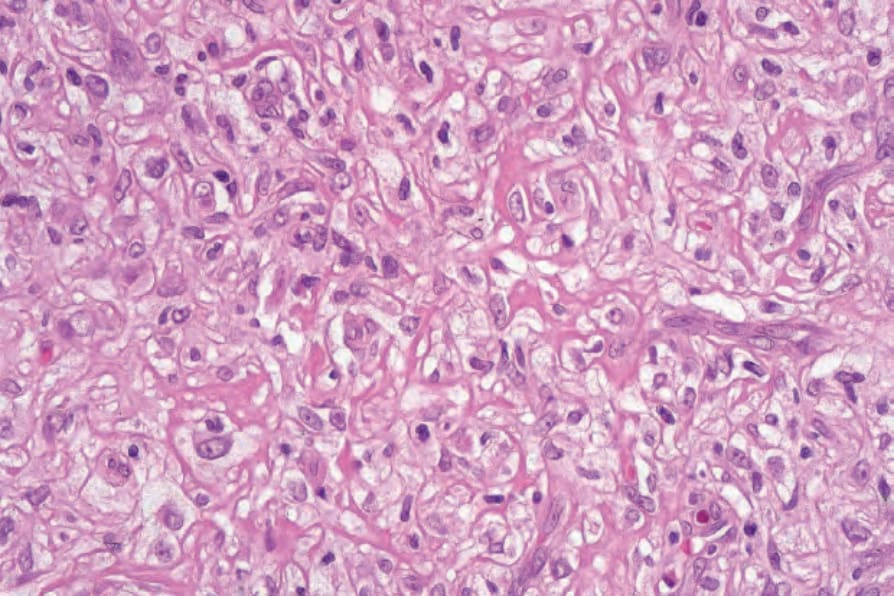
Fig. 35.246 Lipidized (‘ankle-type’) fibrous histiocytoma: high-power view of foamy histiocytes. By courtesy of R. Carr MD, Warwick Hospital, UK.
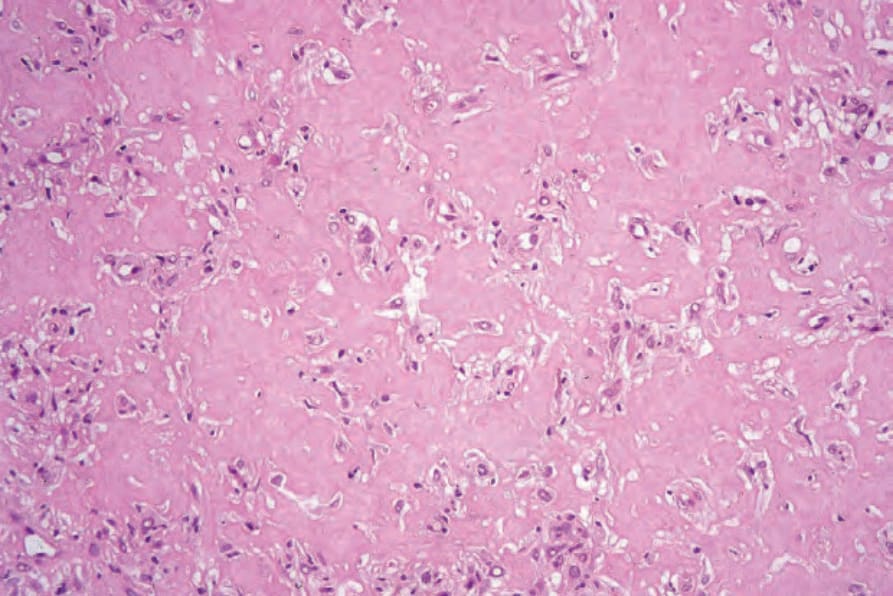
Fig. 35.247 Lipidized (‘ankle-type’) fibrous histiocytoma: this field shows densely hyalinized collagen reminiscent of amyloid. By courtesy of R. Carr MD, Warwick Hospital, UK.
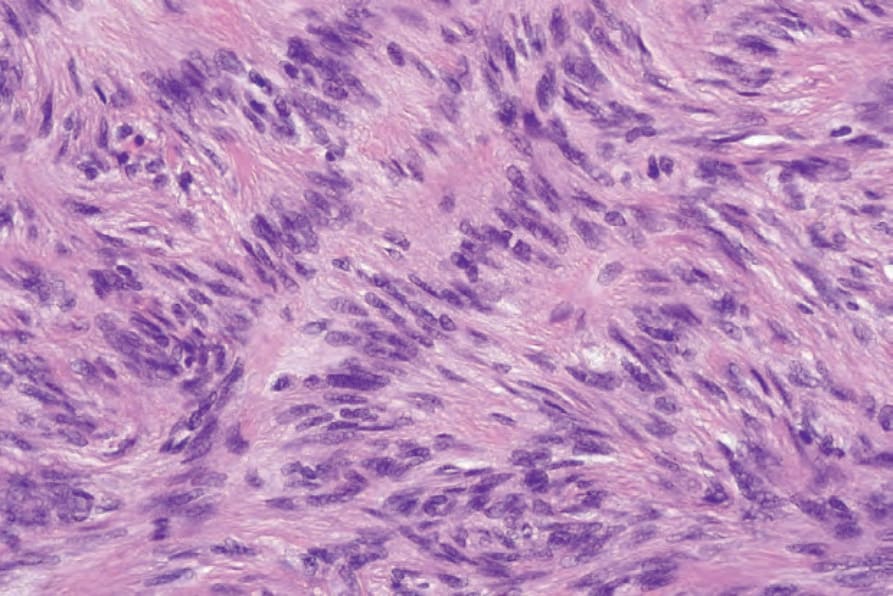
Fig. 35.249 Palisading fibrous histiocytoma: high-power view.
(Fig. 35.230). When the last is present, expression is limited to peripheral parts of the tumor. Focal desmin positivity may be seen in around a third of cases.52
Distinction from leiomyosarcoma is possible by the presence in the latter of cells with cigar-shaped nuclei, at least focal cytologic atypia, a uniform fascicular growth pattern, diffuse positivity for SMA, desmin and H-caldesmon and frequent focal positivity for keratin. Dermatofibrosarcoma protuberans has a monotonous, storiform growth pattern, monomorphous cells and diffuse positivity for CD34.
Aneurysmal fibrous histiocytoma Aneurysmal benign fibrous histiocytoma represents less than 2% of fibrous histiocytomas and presents as a blue–brown nodule on the limbs of middle-aged adults, especially females (Fig. 35.231).53–56 Rapid growth can be seen due to extensive hemorrhage, and clinical confusion with a melanocytic or vascular tumor is common. The rate of recurrence is around 19%.54 Rare cases present with regional lymph node involvement.26,27,54
1765 Benign fibrohistiocytic tumors and tumorlike lesions
Histologically, the most striking feature is the presence (especially towards the center of the lesion) of hemorrhagic irregular cleft-like and cystic spaces mimicking cavernous vascular channels, but without endothelial lining (Figs 35.232 and 35.233). Adjacent solid areas show the usual features of benign fibrous histiocytoma, but are often very cellular. Multifocal interstitial hemorrhage and intra- and extracellular hemosiderin deposition are prominent and normal mitotic figures are common (Figs 35.234–35.236). Due to the extensive secondary changes this lesion is frequently diagnosed as a vascular tumor, but typical features of fibrous histiocytoma are always present and endothelial markers are only positive in normal blood vessels.
Aneurysmal fibrous histiocytoma should not be confused with angiomatoid fibrous histiocytoma, the latter being an unrelated neoplasm with EWSR1-CREB1 gene fusion. The latter is usually subcutaneous and is composed of monomorphic spindle-to-ovoid eosinophilic cells, which are usually desmin positive. A prominent lymphoplasmacytic infiltrate is commonly present. Some patients with the latter condition have striking systemic symptoms.
1766 Connective tissue tumors
Hemosiderotic fibrous histiocytoma probably represents a stage in the development of aneurysmal fibrous histiocytoma.
Epithelioid fibrous histiocytoma Epithelioid fibrous histiocytoma is rare, has a wide age and anatomical distribution (with predilection for the proximal lower limb), and often presents as a polypoid red nodule, which is usually confused with a lobular capillary hemangioma (pyogenic granuloma) (Fig. 35.237).57–60 Multiple lesions are exceptional and a lesion has been reported in the tongue.61,62 A case with metastatic spread has been described.26 Histologically, most tumors are superficial, but rare examples extend into the superficial subcutis. An epidermal collarette is often present and tumor cells are rounded with abundant eosinophilic cytoplasm and a vesicular nucleus with small eosinophilic nucleoli (Figs 35.238–35.241). Binucleate or multinucleate cells are common. Rarely, cells may have granular cell change.63 Occasional normal mitotic figures may be evident. Some lesions are more myxoid and vascular. A rare variant of the tumor has been reported as chondroblastoma-like and consisting of pericellular calcification.64 Immunohistochemistry reveals a population of CD34 positive cells and a population of factor XIIIa-positive dendritic cells.65 Distinction from Spitz nevus is facilitated by the absence of a junctional component or nesting of tumor cells and negativity for S100
1767 Benign fibrohistiocytic tumors and tumorlike lesions
Atypical (pseudosarcomatous) fibrous histiocytoma Atypical (pseudosarcomatous) fibrous histiocytoma is also known as dermatofibroma with monster cells.21,70–73 Clinically, it has a predilection for the limbs with some tumors occurring on the trunk and head and neck. Lesions are usually papular or nodular but may be polypoid, and rare tumors measure up to several centimeters.21 There is local recurrence in a minority of cases, and metastasis rarely occur with one patient dying as a result of systemic spread.21,26,27
Histologically, the lesion is mainly dermal but extends into the superficial subcutis in one-third of cases. In some areas, the tumor shows the features of a more typical fibrous histiocytoma (Fig. 35.243). However, a variable proportion of cells in the tumor have irregular, large and pleomorphic nuclei with prominent nucleoli (Fig. 35.244). Pleomorphism may be marked. The mitotic rate varies and may be high in some cases. Atypical mitotic figures are sometimes seen. An unusual feature is that of focal necrosis.20 Histologic features do not allow prediction of the exceptional tumors that metastasize.26
Atypical fibrous histiocytoma should not be confused with atypical fibroxanthoma. The latter occurs in a completely different clinical setting (see below) and shows diffuse pleomorphism, cytologic atypia and numerous mitoses throughout.
1768 Connective tissue tumors
Lipidized (‘ankle-type’) fibrous histiocytoma Lipidized (‘ankle-type’) fibrous histiocytoma presents as a polypoid yellow lesion on the lower leg.74 Histologically, there is a predominance of foamy histiocytes surrounded by abundant, almost keloidal, hyalinized collagen bundles (Figs 35.245–35.247).
Palisading cutaneous fibrous histiocytoma Palisading cutaneous fibrous histiocytoma refers to lesions that histologically show prominent nuclear palisading (Figs 35.248 and 35.249).80,81 They appear to present most often on acral sites. Focally, there is a resemblance to schwannoma as the palisading mimics Verocay bodies. However, lesions are not encapsulated and tumor cells are S100 negative.
Clear cell fibrous histiocytoma This is a very rare variant with no distinctive clinical features and with massive clear cell change throughout the lesion.75–77 The overall architecture and morphological features are not usually typical of a fibrous histiocytoma and thus may represent an altogether unrelated tumor. It is likely that tumors previously described as clear cell fibrous histiocytoma represent the entity reported as dermal clear cell mesenchymal neoplasm.78,79 Only a handful of cases of the latter entity have been described in adults with predilection for the lower limbs. Tumors consist of sheets of clear cells with vesicular nuclei that occupy the reticular dermis and may extend into the subcutaneous tissue. Cytologic atypia and mitotic figures are rare. Tumor cells are negative for most markers except vimentin, NKI/C3 and sometimes CD68. Behavior appears to be benign.
Atrophic dermatofibroma Atrophic dermatofibroma probably represents the end stage of many dermatofibromas and is characterized clinically by an area of depression or retraction, often resembling a scar or even anetoderma.82–84 Histologically, lesions are hypocellular and show prominent hyalinization of collagen (Figs 35.250 and 35.251). The changes may resemble those seen in multinucleate angiohistiocytoma but the latter usually presents with multiple clinical lesions.
Rare variants Very occasionally, tumors can show prominent osteoclast-like giant cells (occasionally with ossification), granular cell change, cholesterol deposition, focal smooth muscle proliferation, marked myxoid change, keloidal change,
1769 Benign fibrohistiocytic tumors and tumorlike lesions
balloon cell change and signet-ring change.85–102 Tumors may also present with a lichenoid pattern and in a single case intracytoplasmic eosinophilic globules were described.103,104 Two cases of a tumor with scattered pigmented melanocytes, with CD34 positivity and overlapping histologic features between Bednar tumor and dermatofibroma have been reported.105 Unfortunately, no cytogenetic studies were performed in these cases. A further case of a melanoma overlying a dermatofibroma has been reported.106 Although inflammatory cells are a feature of most fibrous histiocytomas, formation of germinal centers is rare.107 Cases with an angiokeloidal pattern have also been described.108
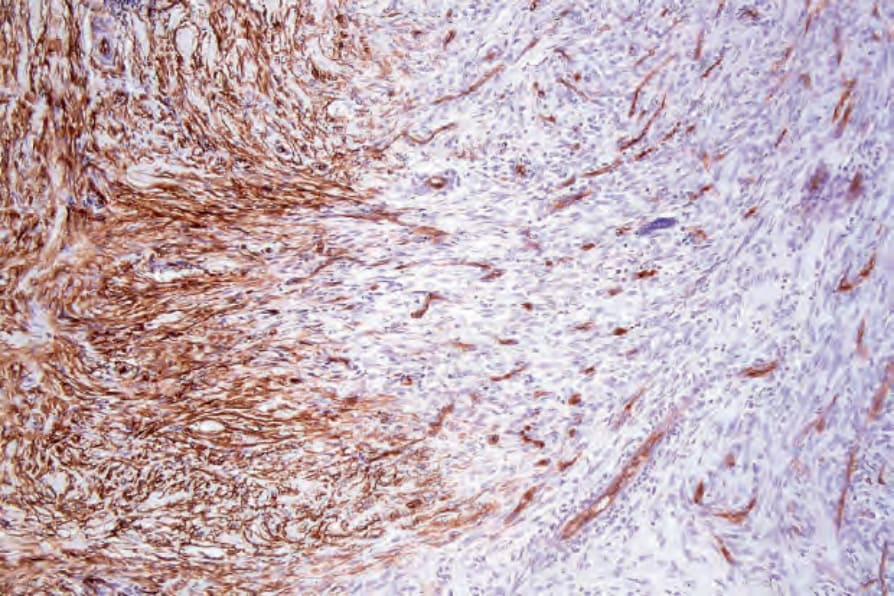
Fig. 35.230 Cellular fibrous histiocytoma: the tumor cells at the edge of the lesion often express CD34.
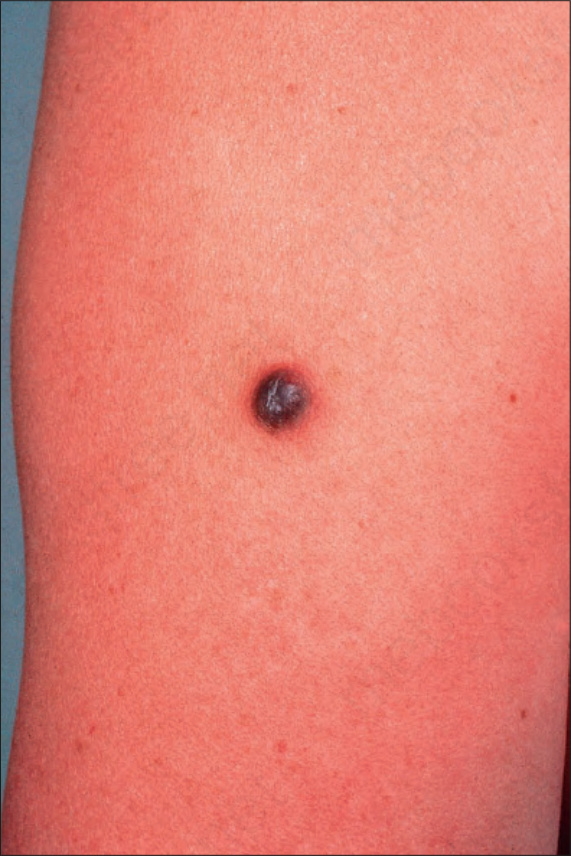
Fig. 35.231 Aneurysmal fibrous histiocytoma: this lesion presents as a hemorrhagic nodule. By courtesy of the Institute of Dermatology, London, UK.
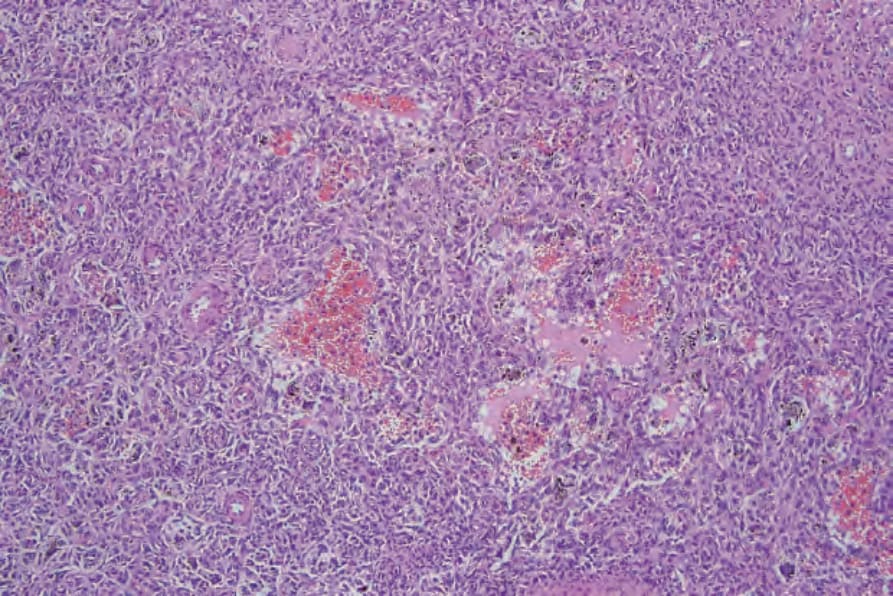
Fig. 35.232 Aneurysmal fibrous histiocytoma: a densely cellular infiltrate is present in the deeper dermis. Blood-filled cystic spaces are evident.
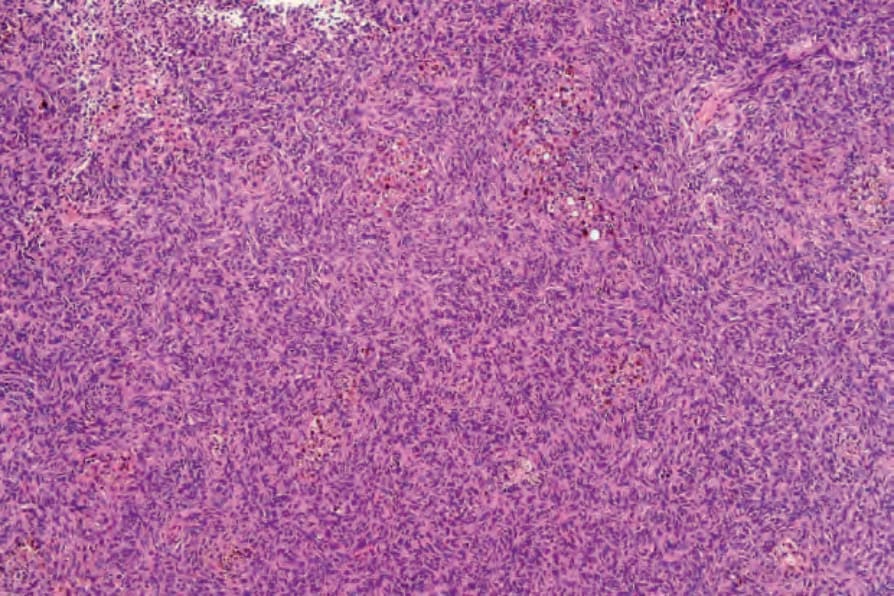
Fig. 35.234 Hemosiderotic fibrous histiocytoma: the marked vascularity and heavy hemosiderin content sometimes seen in this lesion gives a dark bluish-brown coloration, which clinically may cause confusion with melanoma.

Fig. 35.237 Epithelioid benign fibrous histiocytoma: this variant typically presents as an erythematous polypoid lesion. By courtesy of the Institute of Dermatology, London, UK.
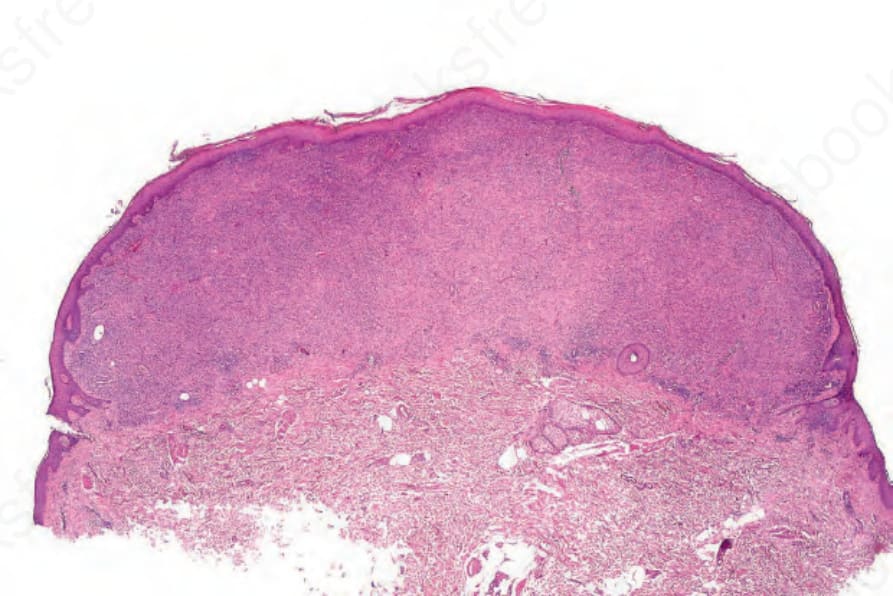
Fig. 35.238 Epithelioid benign fibrous histiocytoma: this low-power view shows a superficial tumor nodule with an associated epidermal collarette.
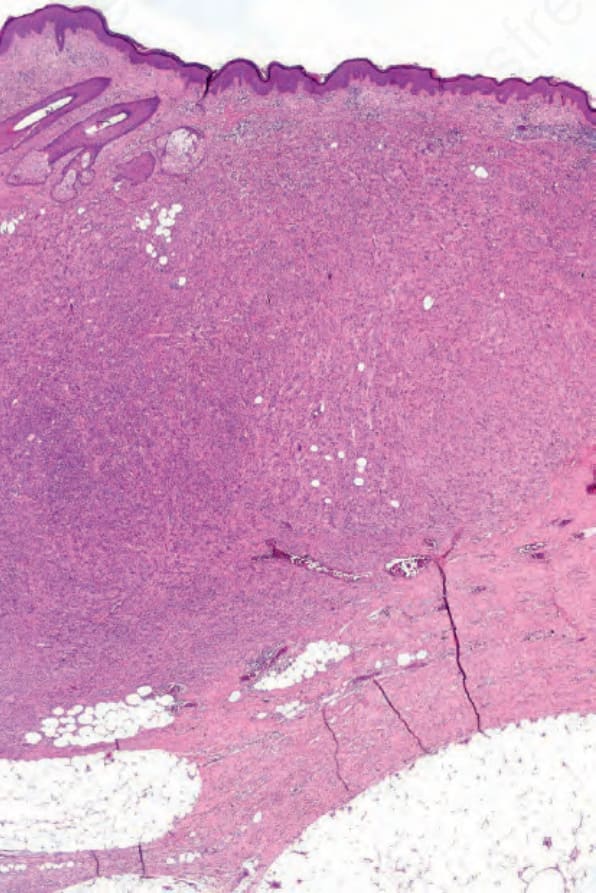
Fig. 35.243 Atypical benign fibrous histiocytoma: this cellular lesion extends into the subcutaneous fat.
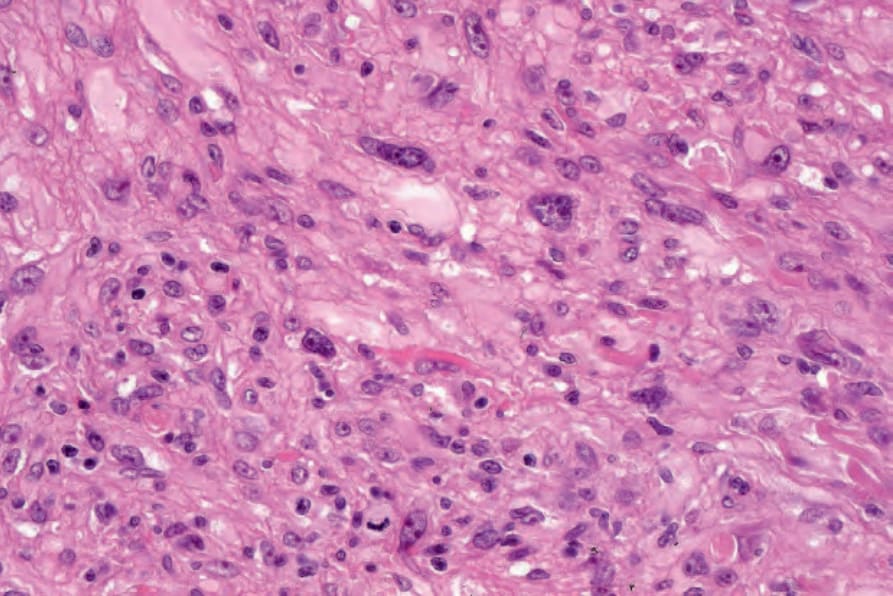
Fig. 35.244 Atypical benign fibrous histiocytoma: there is striking nuclear pleomorphism. Note the mitotic figure. protein. Distinction from a cutaneous perineurioma with epithelioid cell change is made by the presence of diffuse EMA and claudin-1 positivity in the latter tumor. However, focal membranous EMA positivity is a frequent finding in epithelioid fibrous histiocytoma.66 ALK expression is typically seen (in roughly 90% of cases) and is correlated with ALK rearrangements with a variety of partner genes including SQSTM1, VCL, TMP3, EML4, PRKAR2A, and others (Fig. 35.242).67–69
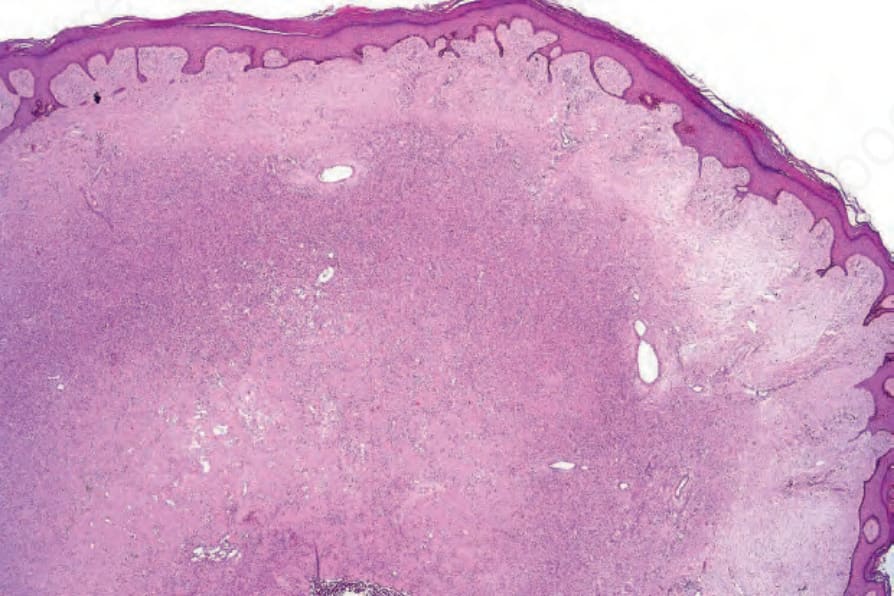
Fig. 35.245 Lipidized (‘ankle-type’) fibrous histiocytoma: this is a distinctive morphological subset characterized by a predominance of xanthoma cells associated with marked stromal hyalinization. By courtesy of R. Carr MD, Warwick Hospital, UK.
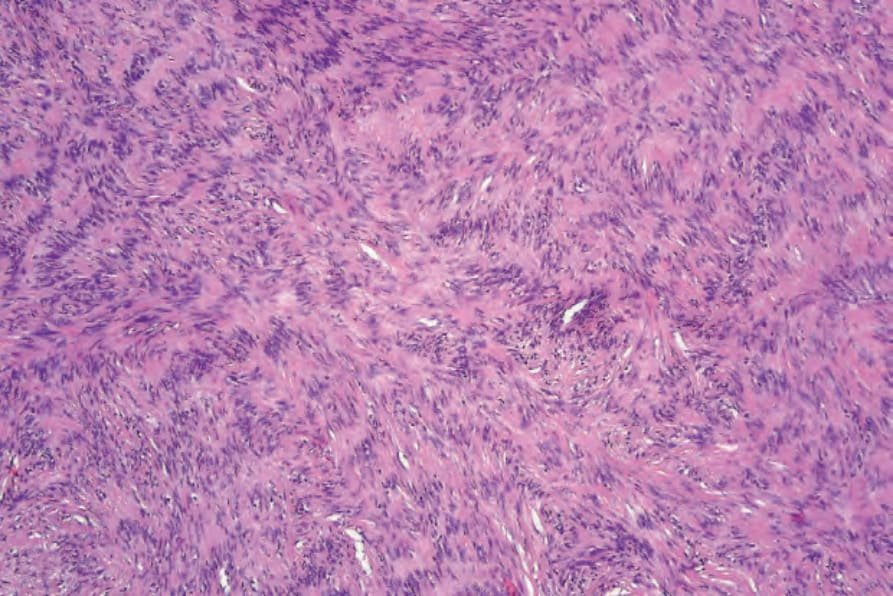
Fig. 35.248 Palisading fibrous histiocytoma: occasionally, palisading mimicking Verocay bodies may be a feature.
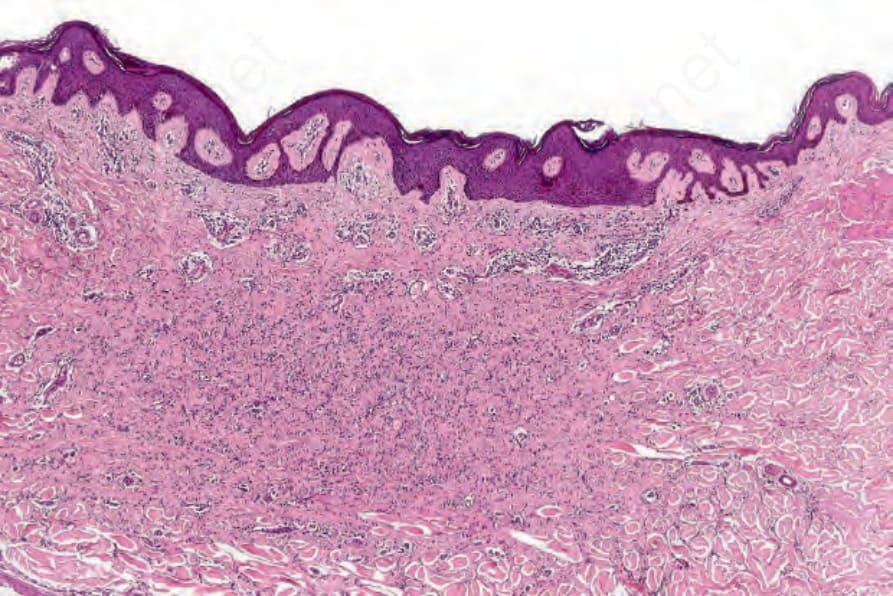
Fig. 35.250 Atrophic fibrous histiocytoma: this variant appears hypocellular and orientated parallel to the surface epithelium.