腦膜異位 (Meningeal Heterotopias)
疾病定義與分類
- 出現於皮膚的腦膜病灶 (meningeal lesions) 通常被稱為「皮膚腦膜瘤 (cutaneous meningiomas)」。此名稱傾向暗示一種腫瘤性 (neoplastic) 起源;然而本組大多數病灶可能屬於錯構瘤性 (hamartomatous) 或發育缺陷 (developmental defect) 的結果,因此我們偏好使用腦膜異位 (meningeal heterotopias) 此一名稱。
- 將皮膚腦膜病灶分為三型 (type I、type II、type III) 較為方便。然而各型之間有極大程度的重疊,尤其在組織學上 type I 與 type II 病灶之間更是如此,它們很可能代表同一錯構瘤性過程 (hamartomatous process) 的不同變異型。
臨床特徵 (Clinical Features)
- Type I 病灶亦曾被描述為異位性腦膜上皮錯構瘤 (ectopic meningothelial hamartoma) 以及隔離型或退化型腦膜膨出 (sequestrated or rudimentary meningocele)。雖然它們屬於先天性 (congenital),但有時要到兒童期與青春期才被辨識出來。其性別發生率相等,臨床表現為頭皮 (scalp)(尤其枕部 occipital area)上一個外觀不顯著的皮膚或皮下結節或斑塊,較少見於背部沿中線分布 (Fig. 35.378)。它們常於臨床上被診斷為囊腫 (cysts)。其下方並無骨骼異常。可見禿髮 (alopecia) 與先天性皮膚缺損 (aplasia cutis)。
- Type II 病灶主要在成年期出現於頭頸部,主要圍繞口、鼻、眼與耳,但偶可發生於兒童。曾有一例與妊娠 (pregnancy) 相關、另一例與顱周竇 (sinus pericranii) 相關的個案被報告。
組織病理特徵 (Histopathology)
- 可見對 NSE、podoplanin、NKIC3 呈陽性,較少見對 Glut-1 與 PR 陽性。局部可見細胞包繞於透明化的膠原束 (hyalinized collagen bundles) 周圍,伴有鈣化 (calcification) 或砂粒體 (psammoma body) 形成 (Figs 35.383 與 35.384)。偶可見多核細胞 (multinucleated cells) 為一特徵。基質呈纖維化 (fibrotic stroma),但有時可相當明顯,在部分個案中可見黏液樣變性 (myxoid change)。整個腫瘤中正常血管數目增加,真皮內可見脂肪組織。有時可辨識出真皮黑色素細胞 (dermal melanocytes)。可見與腦組織 (brain tissue) 或異位性室管膜囊腫 (heterotopic ependymal cyst) 相關。
- Type II 病灶的特徵為存在少量更為界限分明且較大的腦膜上皮細胞 (meningothelial cells) 實性巢。曾有一例腦膜瘤 (meningioma) 顯然由退化型腦膜膨出 (rudimentary meningocele) 發展而來的個案被記載。
- 曾報告一例 8 歲男孩同時合併黑色素細胞增多症 (melanocytosis) 與血管畸形 (vascular malformation) 的個案。
- Type III 病灶呈現顱內腦膜瘤 (intracranial meningioma) 的特徵,包括退行發育型 (anaplastic forms)。它們由紡錘狀與卵圓形腦膜上皮細胞組成,伴有程度不一的纖維膠原性基質 (fibrocollagenous stroma) (Figs 35.385 與 35.386)。漩渦狀 (whorled) 或席紋狀 (storiform) 排列型態常見,有時腫瘤細胞排列成小葉 (lobules) 或細胞團 (packets)。不少見的是,較大的卵圓形細胞具有不清晰的細胞邊界,呈片狀分布,呈現合胞體樣外觀 (syncytial appearance)。砂粒體 (psammoma bodies) 常出現。
免疫組化與特殊染色 (Immunohistochemistry & Special Stains)
- Type II 與 III 對 EMA 與 p63 呈陽性,但對 CK5/6、S100 與 CD31 呈陰性。
鑑別診斷 (Differential Diagnosis)
- 由於其偽血管樣外觀 (pseudovascular appearance),type I 病灶可能與血管肉瘤 (angiosarcoma) 混淆。然而後者一般發生於年紀較大的病人,且典型上呈現細胞學異型性 (cytologic atypia)、多層化 (multilayering)、有絲分裂象 (mitotic figures),以及對血管標記 (vascular markers) 呈陽性表現,但對 EMA 不表現。
- 當考慮原發性上皮性或附屬器腫瘤 (primary epithelial or adnexal tumor) 時,對 cytokeratins、尤其是對 CK5/6 呈陰性是有幫助的特徵。
- 轉移性癌 (metastatic carcinoma) 可藉由病史短、存在細胞學異型性、有絲分裂與 keratin 陽性而與 type I 及 type II 病灶區分。
- CT 與 MRI 掃描(尤其是後者)是首選的放射學檢查,但與血管瘤 (hemangioma) 的區分可能有困難。在此類個案中,超音波 (ultrasound) 或都卜勒血流檢查 (Doppler flow studies) 或可提供區分。產前診斷 (prenatal diagnosis) 可藉由超音波進行。對此類病人若不謹慎處置,有時會導致腦脊髓液 (cerebrospinal fluid) 滲漏、腦膜炎 (meningitis) 與腦膿瘍 (cerebral abscess)。
組織學特徵 (Histologic Features)
- 顯微鏡下外觀具特徵性,典型表現為界限清楚的結節,主要由位於皮下組織內、處於疏鬆神經原纖維基質 (loose neurofibrillar stroma) 中的分化良好星形膠質細胞 (well-differentiated astrocytes) 所組成 (Figs 35.388 與 35.389)。寡突膠質細胞 (oligodendrocytes) 可局部辨識出來,且在罕見個案中可見可辨認的神經元成分 (neuronal component) (Fig. 35.390)。與腦膨出 (encephalocele) 的組織學區分並不可能,因為即使是異位 (heterotopias) 也可顯示具神經元 (neurons) 與室管膜管 (ependymal canals) 的層狀大腦皮質 (laminated cerebral cortex) (Fig. 35.391)。有時可見局部鈣化 (focal calcifications) 與輕度發炎。曾有一例描述相關小汗腺導管 (eccrine sweat ducts) 的增生。在年紀較大的病人中,病灶可能幾乎完全被纖維化 (fibrosis) 取代,使辨識變得非常困難。診斷可藉由 GFAP 與 S100 protein 的表現加以確認。

圖 35-378:異位性腦膜上皮錯構瘤 (ectopic meningothelial hamartoma):頭皮 (scalp) 是常見的受侵部位。承蒙 Institute of Dermatology, London, UK 惠予提供。
Fig. 35.378 Ectopic meningothelial hamartoma: the scalp is a commonly affected site. By courtesy of the Institute of Dermatology, London, UK.
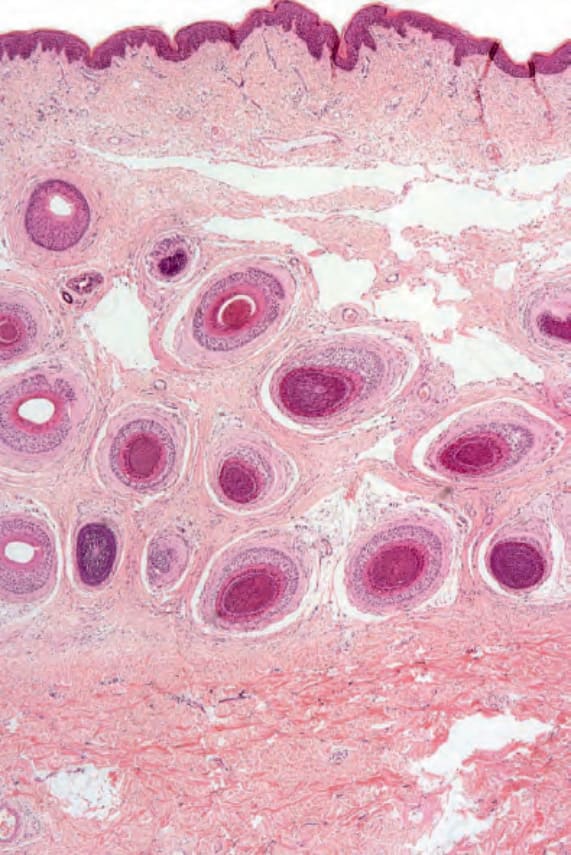
圖 35-379:異位性腦膜上皮錯構瘤 (ectopic meningothelial hamartoma):此病灶由襯覆腦膜上皮細胞 (meningothelial cells) 的偽血管樣裂隙 (pseudovascular clefts) 所組成。
Fig. 35.379 Ectopic meningothelial hamartoma: this lesion is composed of pseudovascular clefts lined by meningothelial cells.
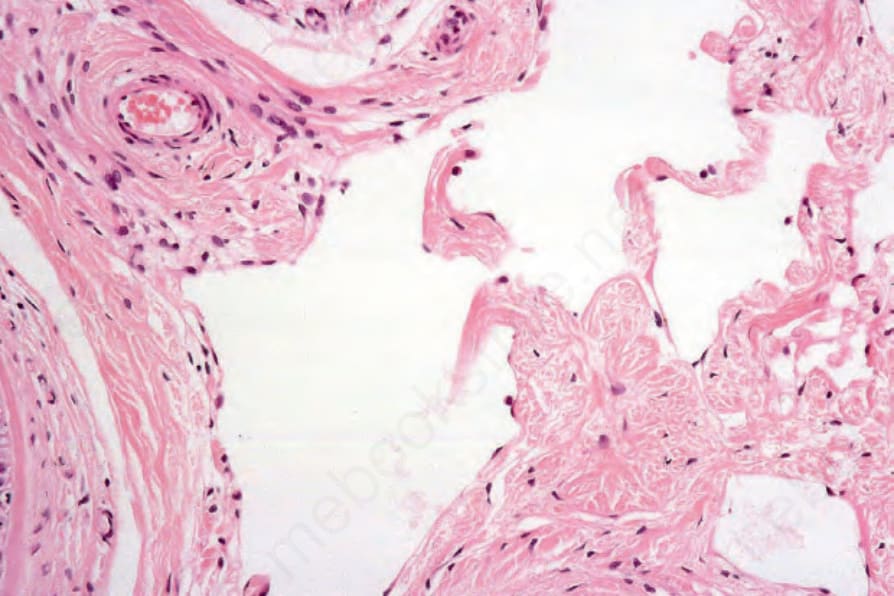
圖 35-380:異位性腦膜上皮錯構瘤 (ectopic meningothelial hamartoma):高倍視野顯示腦膜上皮細胞 (meningothelial cells) 襯覆於囊狀腔隙。
Fig. 35.380 Ectopic meningothelial hamartoma: high-power view showing meningothelial cells lining the cystic spaces.
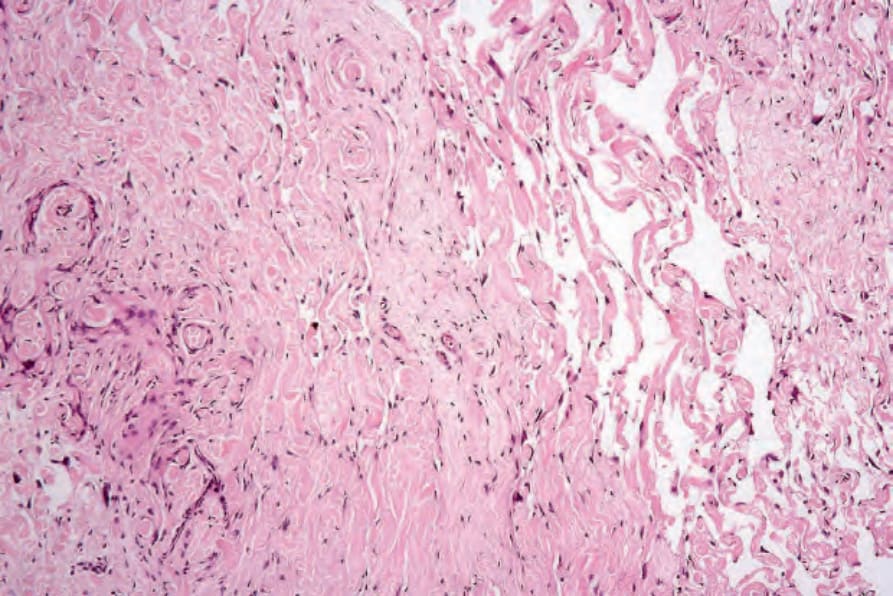
圖 35-381:異位性腦膜上皮錯構瘤 (ectopic meningothelial hamartoma):偽血管樣腔隙 (pseudovascular spaces) 與緻密纖維組織 (dense fibrous tissue) 相關。
Fig. 35.381 Ectopic meningothelial hamartoma: the pseudovascular spaces are associated with dense fibrous tissue.
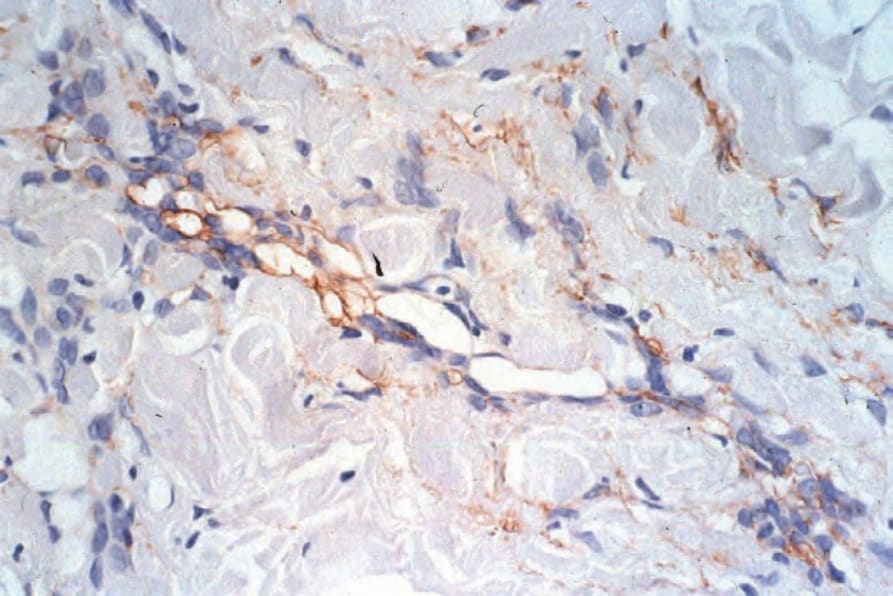
圖 35-382:異位性腦膜上皮錯構瘤 (ectopic meningothelial hamartoma):腫瘤細胞表現 epithelial membrane antigen。
Fig. 35.382 Ectopic meningothelial hamartoma: the tumor cells express epithelial membrane antigen.
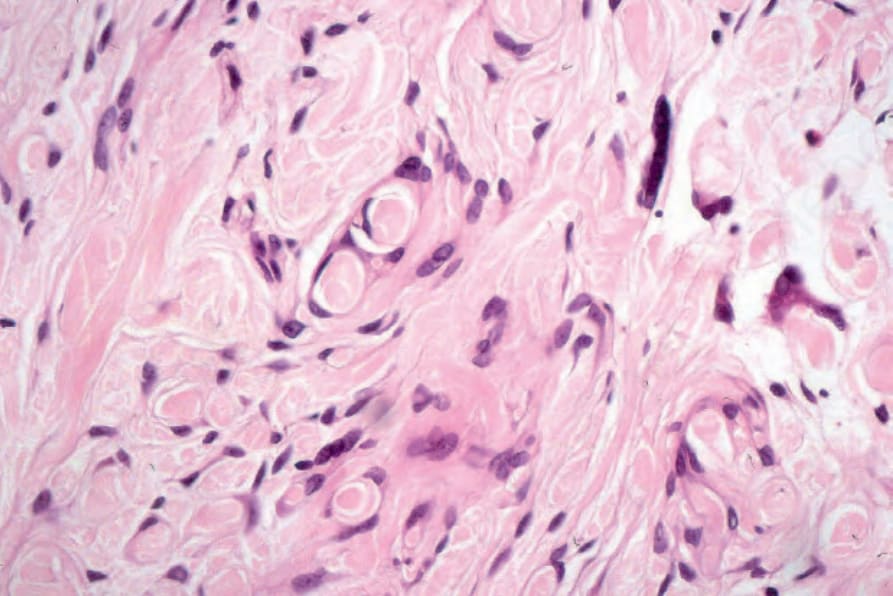
圖 35-383:異位性腦膜上皮錯構瘤 (ectopic meningothelial hamartoma):腫瘤細胞特徵性地包繞陷入膠原 (collagen)。
Fig. 35.383 Ectopic meningothelial hamartoma: the tumor cells characteristically entrap collagen.
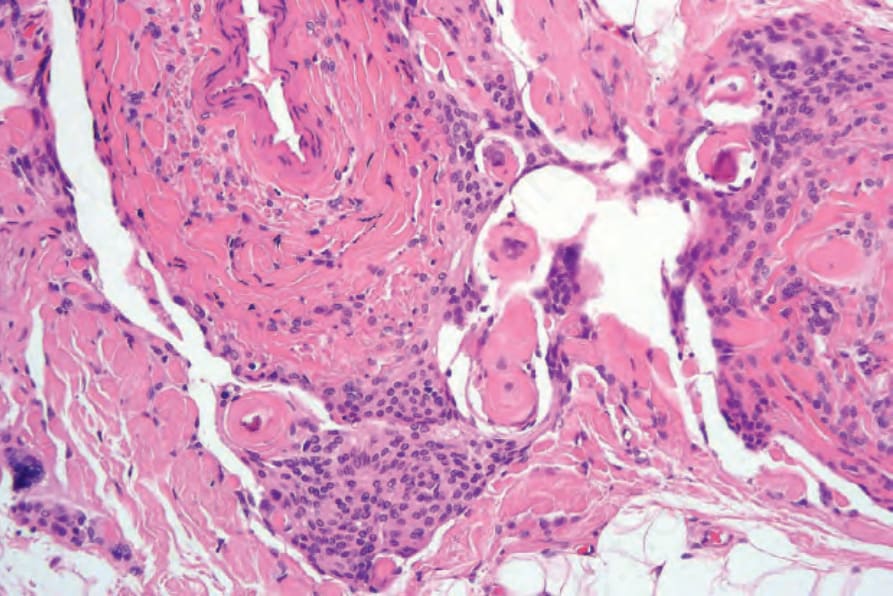
圖 35-384:異位性腦膜上皮錯構瘤 (ectopic meningothelial hamartoma):砂粒體 (psammoma bodies) 有時為一特徵。注意明顯的腦膜上皮增生 (meningothelial proliferation)。
Fig. 35.384 Ectopic meningothelial hamartoma: psammoma bodies are sometimes a feature. Note the conspicuous meningothelial proliferation.
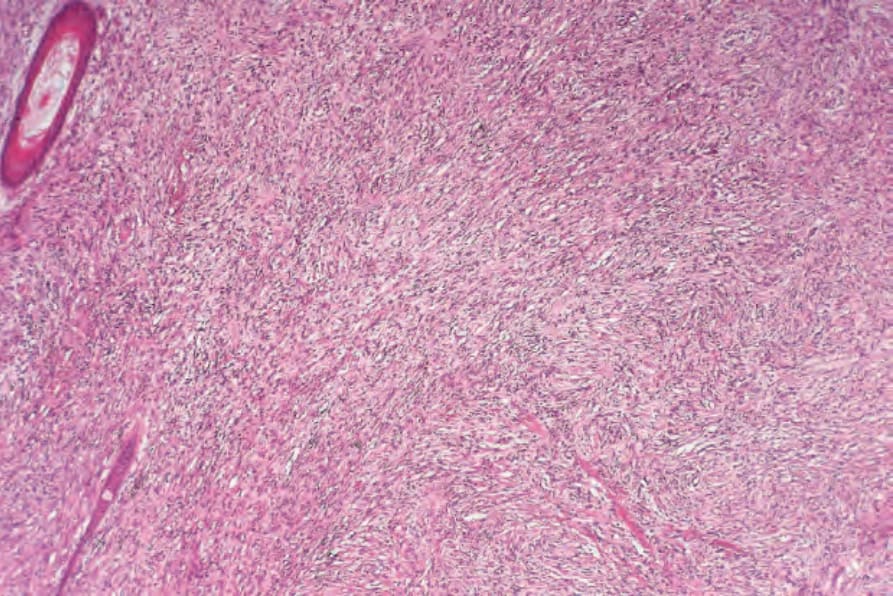
圖 35-385:皮膚「轉移性」腦膜瘤 (cutaneous ‘metastatic’ meningioma):真皮被一紡錘細胞腫瘤 (spindle cell tumor) 瀰漫性浸潤。
Fig. 35.385 Cutaneous ‘metastatic’ meningioma: the dermis is diffusely infiltrated by a spindle cell tumor.
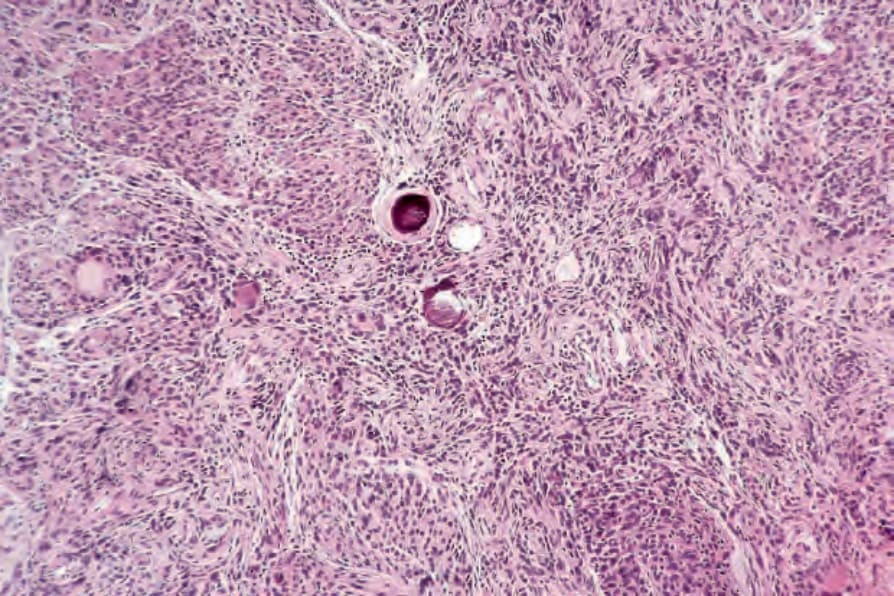
圖 35-386:皮膚「轉移性」腦膜瘤 (cutaneous ‘metastatic’ meningioma):此例中可見發育良好的嗜鹼性砂粒體 (basophilic psammoma bodies)。
Fig. 35.386 Cutaneous ‘metastatic’ meningioma: in this example well-developed basophilic psammoma bodies are evident.

圖 35-387:鼻神經膠質瘤 (nasal glioma):鼻是最常見的受侵部位。承蒙 Institute of Dermatology, London, UK 惠予提供。
Fig. 35.387 Nasal glioma: the nose is the most commonly affected site. By courtesy of the Institute of Dermatology, London, UK.
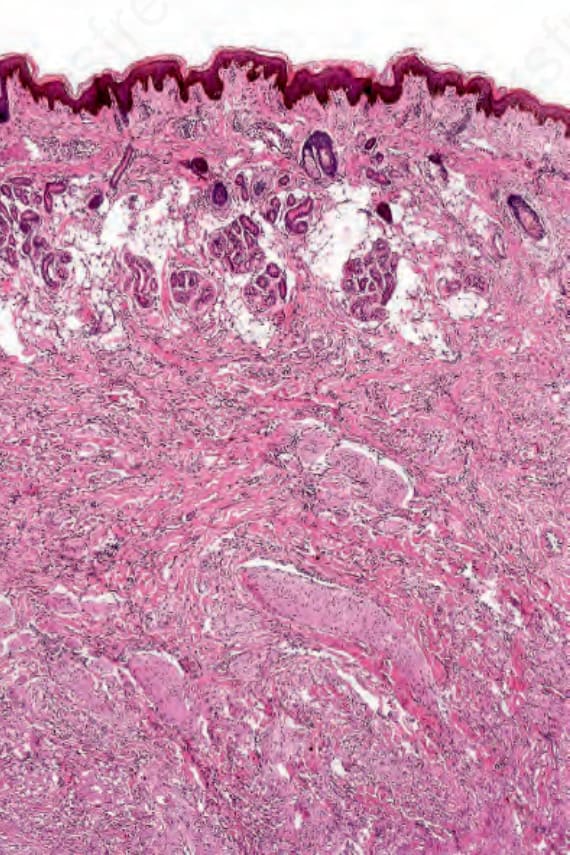
圖 35-388:鼻神經膠質瘤 (nasal glioma):取自一名 2 歲女孩鼻樑的此切片,顯示一界限不清的腫瘤腫塊位於受壓迫的皮下脂肪深處。
Fig. 35.388 Nasal glioma: this section from the bridge of the nose of a 2-year-old girl shows an ill-defined tumor mass deep to the compressed subcutaneous fat.
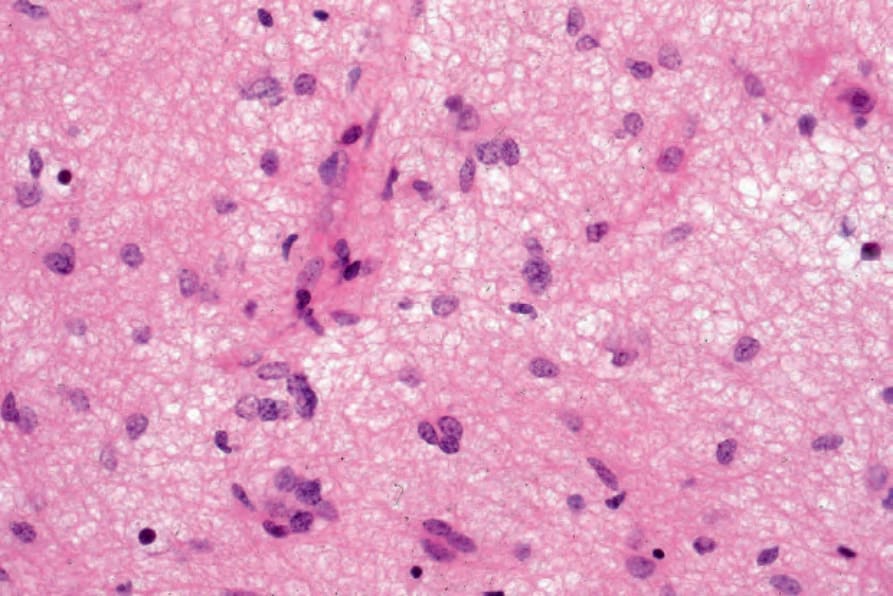
圖 35-390:鼻神經膠質瘤 (nasal glioma):結節主要由具圓形空泡狀核 (round vesicular nuclei) 的星形膠質細胞 (astrocytes) 組成。具小型深染核 (small hyperchromatic nuclei) 的細胞為寡突膠質細胞 (oligodendrocytes)。
Fig. 35.390 Nasal glioma: the nodules are composed predominantly of astrocytes with round vesicular nuclei. The cells with small hyperchromatic nuclei are oligodendrocytes.
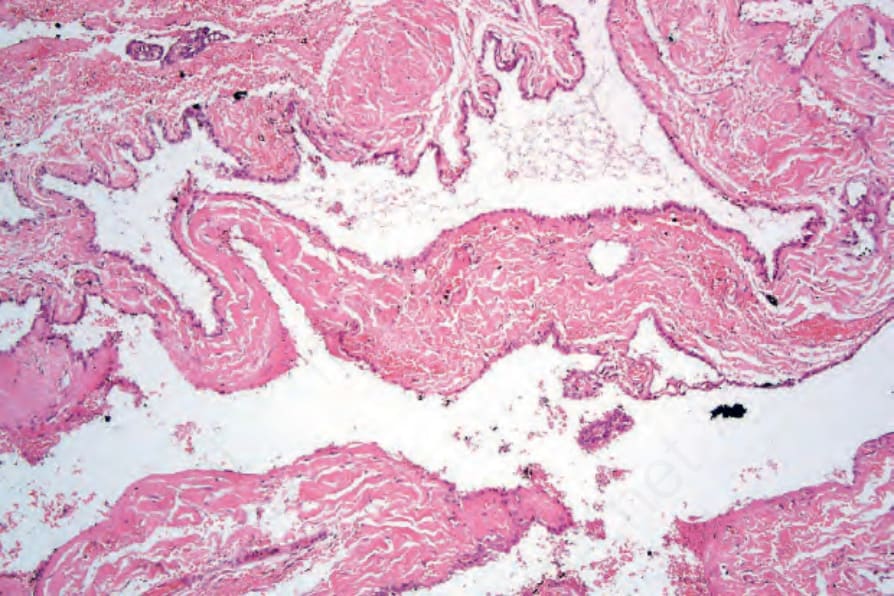
圖 35-391:腦膨出 (encephalocele):此囊狀腔隙襯覆室管膜細胞 (ependymal cells),並與一顱內成分相通。
Fig. 35.391 Encephalocele: this cystic cavity is lined by ependymal cells and communicated with an intracranial component.