Meningeal heterotopias
Meningeal heterotopias
Meningeal lesions presenting in the skin are usually known as ‘cutaneous meningiomas.’ The use of this term tends to imply a neoplastic origin and since most lesions in this group are probably hamartomatous or the result of developmental defect, we prefer the designation meningeal heterotopias. It is convenient to classify cutaneous meningeal lesions into three types.1 However, there is a great degree of overlap, especially histologically, between type I and type II lesions and they probably represent variants of a similar hamartomatous process.
Clinical features Type I lesions have also been described as ectopic meningothelial hamartoma and sequestrated or rudimentary meningocele.2–9 Although they are congenital, they are sometimes only recognized during childhood and adolescence. There is an equal sex incidence and presentation is that of a nondescript cutaneous or subcutaneous nodule or plaque on the scalp (especially the occipital area) or less commonly on the back along the midline (Fig. 35.378). Often, they are diagnosed clinically as cysts. There is no underlying bone abnormality. Alopecia and aplasia cutis can be seen.9,10
Type II lesions present mainly in adulthood on the head and neck mainly around mouth, nose, eyes, and ears but may rarely occur in children.11–13 A case associated with pregnancy and one with a sinus pericranii have been
1805 Heterotopias
Positivity for NSE, podoplanin, NKIC3 and less commonly for Glut-1 and PR may be seen.9 Focally, cells wrap around hyalinized collagen bundles with calcification or psammoma body formation (Figs 35.383 and 35.384). Occasional multinucleated cells may be a feature. A fibrotic stroma but may be prominent and in some cases the is myxoid change.9 Throughout the tumor there is an increase in the number of normal blood vessels, and fatty tissue may be evident within the dermis. Dermal melanocytes are sometimes identified.9 The association with brain tissue or a heterotopic ependymal cyst may be seen.9
Type II lesions are characterized by the presence of small numbers of more discrete and larger solid nests of meningothelial cells. A case of meningioma apparently developing from a rudimentary meningocele has been documented.21
A case associated with melanocytosis and a vascular malformation in an 8-year-old boy has been reported.22
Type III lesions show the features of an intracranial meningioma including anaplastic forms.23 They are composed of spindle-shaped and ovoid meningothelial cells, with a variable fibrocollagenous stroma (Figs 35.385 and 35.386). A whorled or storiform pattern is common and sometimes the tumor cells are arranged in lobules or packets. Not infrequently, the larger
1806 Connective tissue tumors
ovoid cells, which have indistinct cell borders, are distributed in sheets, giving rise to a syncytial appearance. Psammoma bodies are often present.
Type II and III are positive for EMA and p63 but negative for CK5/6, S100, and CD31.24
Differential diagnosis Due to the pseudovascular appearance, type I lesions may be confused with angiosarcoma. The latter, however, generally occurs in older patients and typically shows cytologic atypia, multilayering, mitotic figures and positive expression for vascular markers, but not for EMA.
When a primary epithelial or adnexal tumor is considered negativity for cytokeratins and especially for CK5/6 are helpful features.16,25
Metastatic carcinoma can be distinguished from type I and type II lesions by a short history and the presence of cytologic atypia, mitosis and keratin positivity.
CT and MRI scans (particularly the latter) are the preferred radiological studies but distinction from a hemangioma may be difficult. In such cases ultrasound or Doppler flow studies may afford the distinction.18 Prenatal diagnosis may be made by ultrasound.19,20 Incautious treatment of such patients sometimes results in leakage of cerebrospinal fluid, meningitis and cerebral abscess.
Histologic features The microscopic appearances are characteristic, being typified by well-circumscribed nodules composed largely of well-differentiated astrocytes in a loose neurofibrillar stroma situated in the subcutaneous tissues (Figs 35.388 and 35.389). Oligodendrocytes may be focally identified and, in rare cases, there may be a demonstrable neuronal component (Fig. 35.390). Histologic distinction from an encephalocele is not possible since even heterotopias may show laminated cerebral cortex with neurons and ependymal canals (Fig. 35.391).12 Focal calcifications and mild inflammation are sometimes seen.5 Proliferation of associated eccrine sweat ducts has been described in a case.21 In older patients, lesions may be almost completely replaced by fibrosis, making recognition very difficult.12 Diagnosis can be confirmed by the expression of GFAP and S100 protein.3,5

Fig. 35.378 Ectopic meningothelial hamartoma: the scalp is a commonly affected site. By courtesy of the Institute of Dermatology, London, UK.
Fig. 35.379 Ectopic meningothelial hamartoma: this lesion is composed of pseudovascular clefts lined by meningothelial cells.
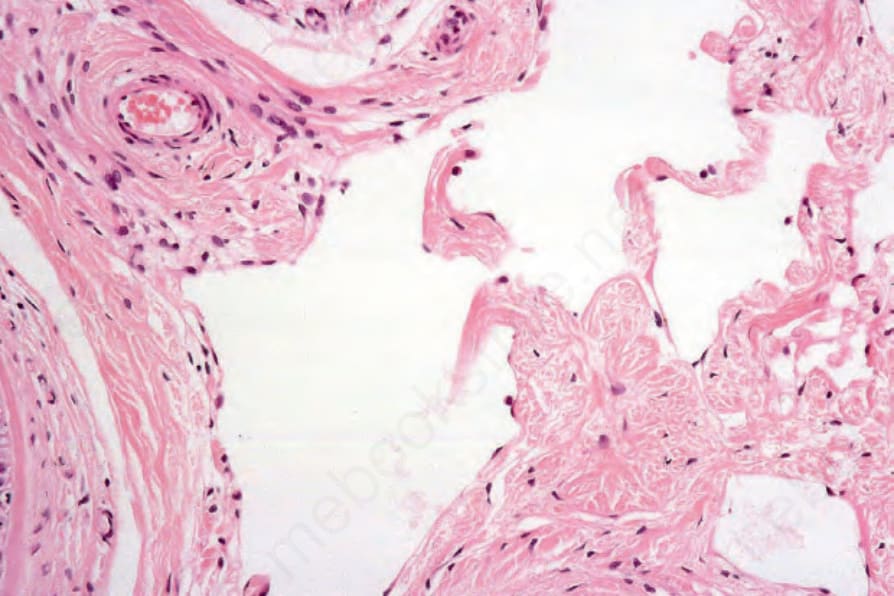
Fig. 35.380 Ectopic meningothelial hamartoma: high-power view showing meningothelial cells lining the cystic spaces.
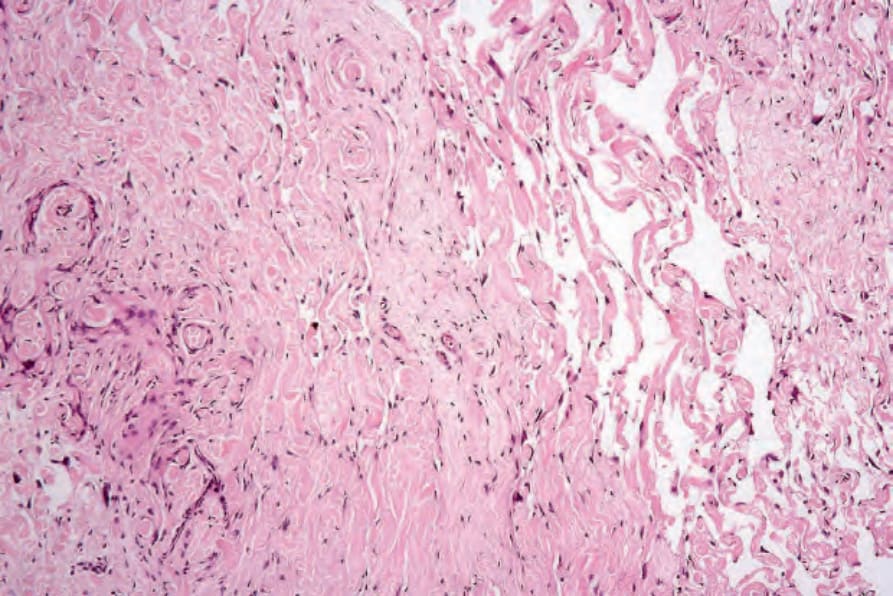
Fig. 35.381 Ectopic meningothelial hamartoma: the pseudovascular spaces are associated with dense fibrous tissue.
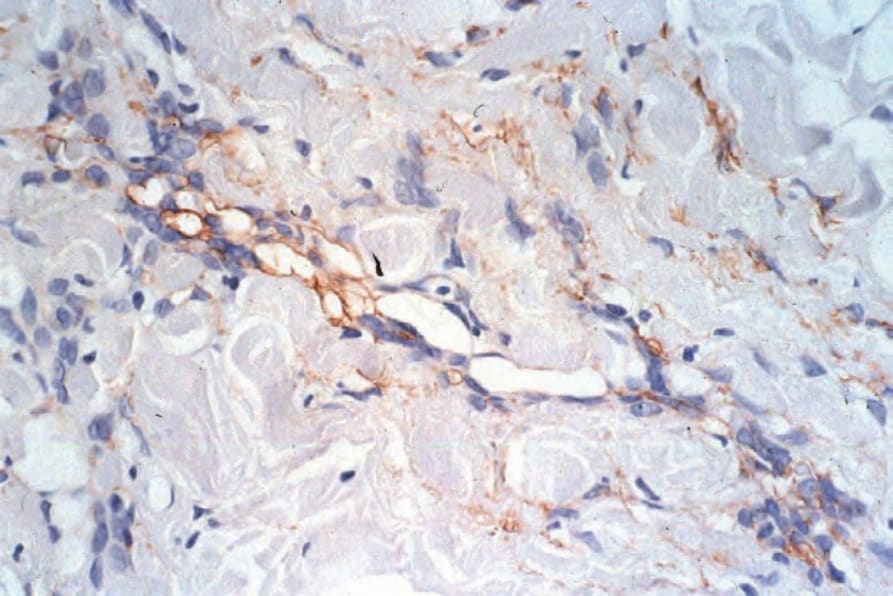
Fig. 35.382 Ectopic meningothelial hamartoma: the tumor cells express epithelial membrane antigen.
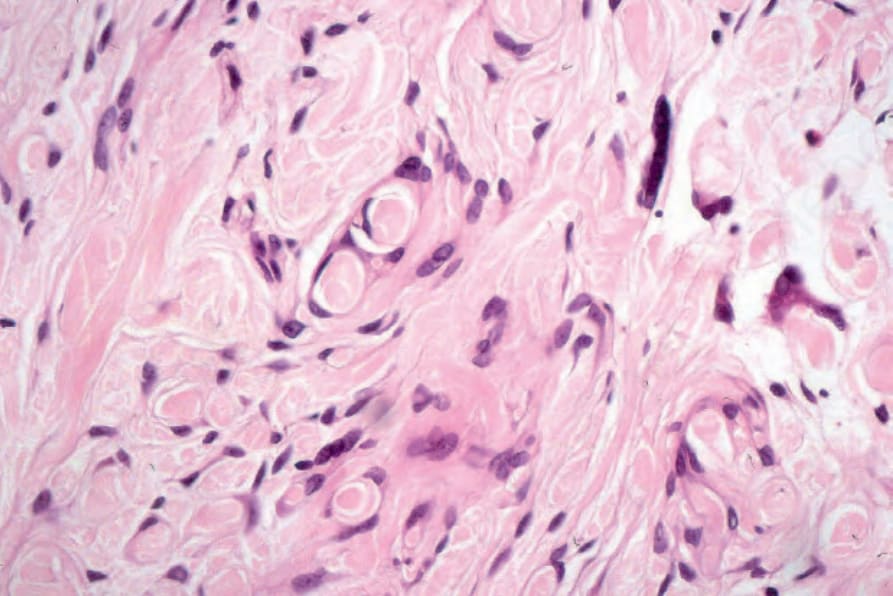
Fig. 35.383 Ectopic meningothelial hamartoma: the tumor cells characteristically entrap collagen.
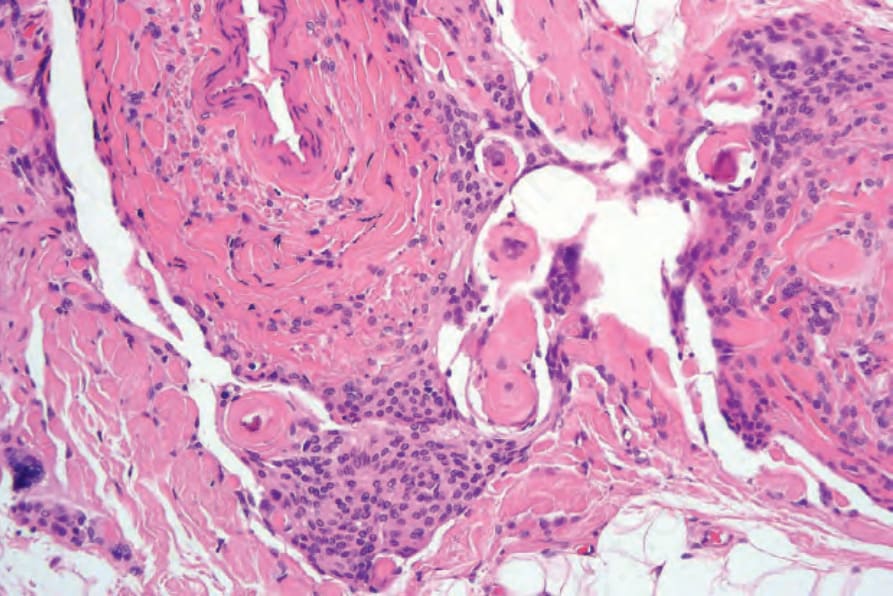
Fig. 35.384 Ectopic meningothelial hamartoma: psammoma bodies are sometimes a feature. Note the conspicuous meningothelial proliferation.
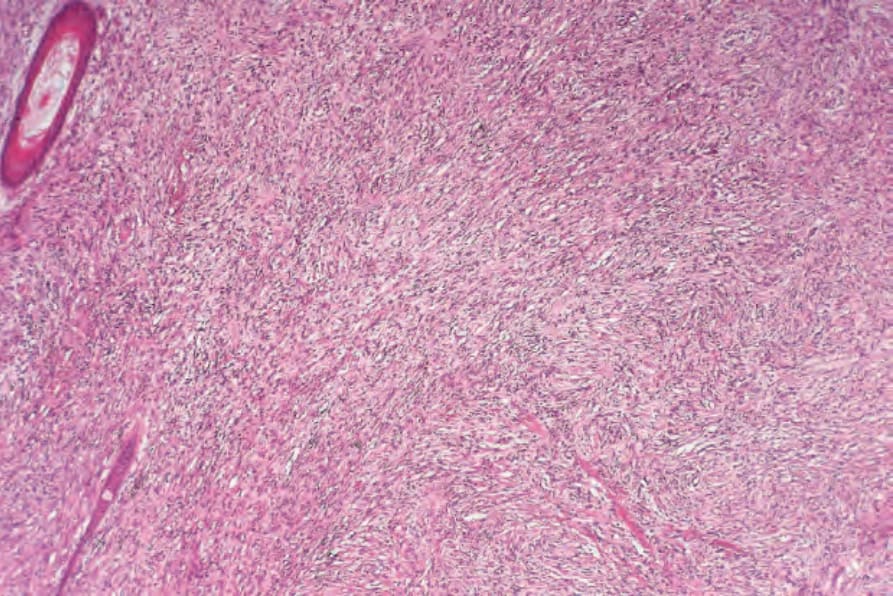
Fig. 35.385 Cutaneous ‘metastatic’ meningioma: the dermis is diffusely infiltrated by a spindle cell tumor.
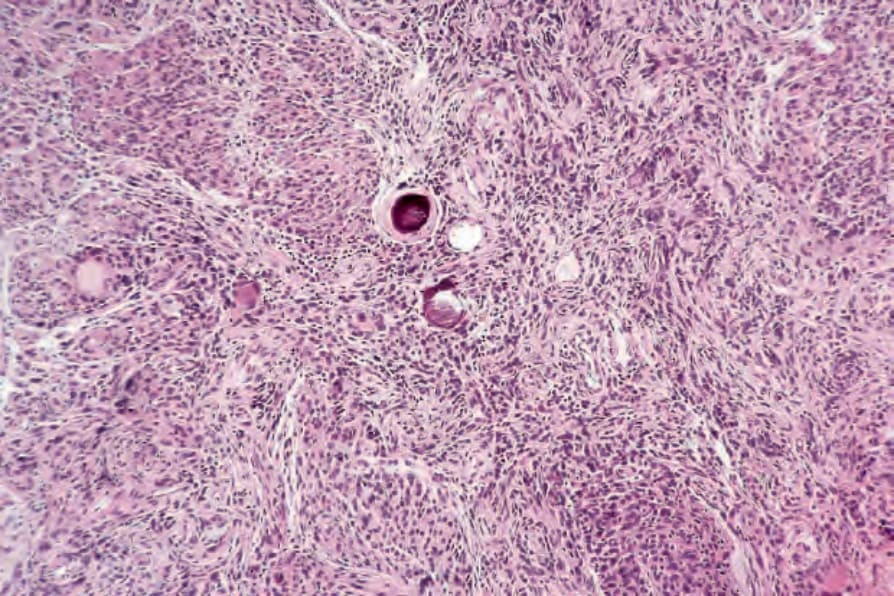
Fig. 35.386 Cutaneous ‘metastatic’ meningioma: in this example well-developed basophilic psammoma bodies are evident.

Fig. 35.387 Nasal glioma: the nose is the most commonly affected site. By courtesy of the Institute of Dermatology, London, UK.
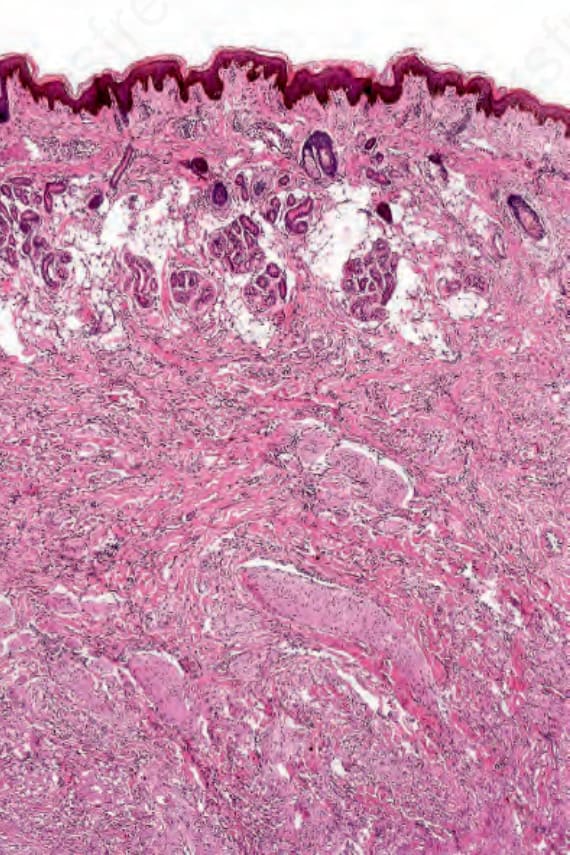
Fig. 35.388 Nasal glioma: this section from the bridge of the nose of a 2-year-old girl shows an ill-defined tumor mass deep to the compressed subcutaneous fat.
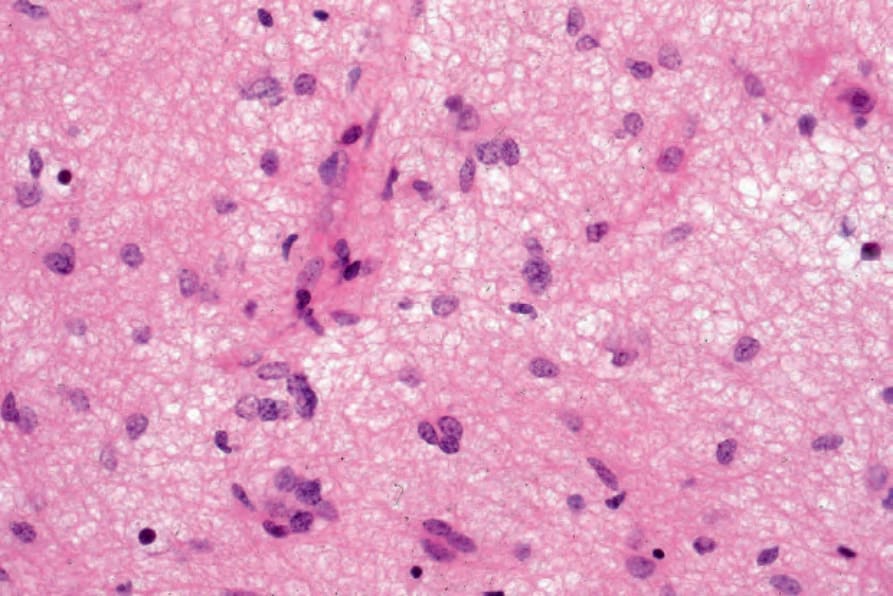
Fig. 35.390 Nasal glioma: the nodules are composed predominantly of astrocytes with round vesicular nuclei. The cells with small hyperchromatic nuclei are oligodendrocytes.
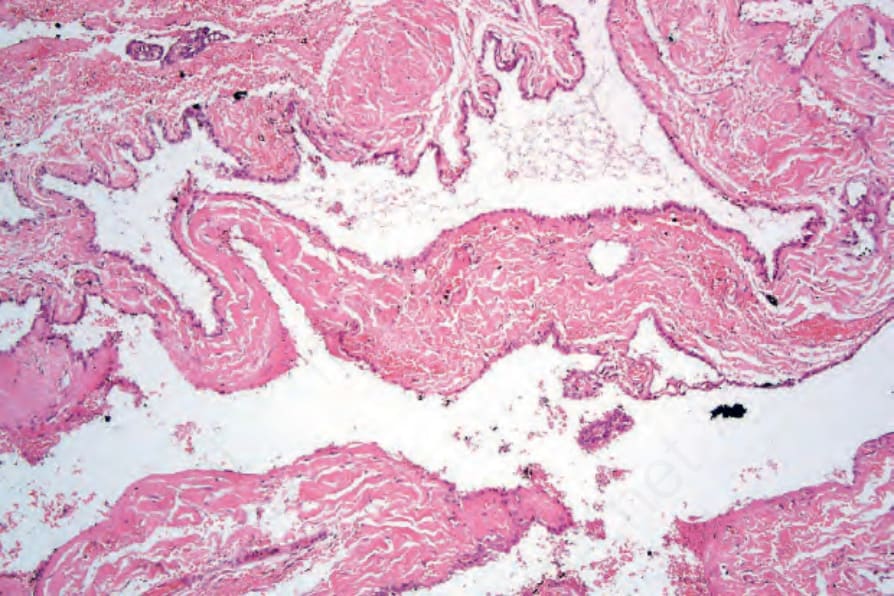
Fig. 35.391 Encephalocele: this cystic cavity is lined by ependymal cells and communicated with an intracranial component.