Fibrofolliculoma
臨床特徵 (Clinical Features)
- 纖維毛囊瘤 (fibrofolliculoma) 極少以單發性的臉部丘疹 (solitary facial papule) 形式表現。較常見的是出現多發性病灶 (multiple lesions),可代表一種孤立性的情況,或一種體染色體顯性遺傳症候群 (autosomal dominant syndrome)。
- 曾有一例報告:一系列患有多發性 fibrofolliculoma 的病人合併家族性甲狀腺髓質癌 (familial thyroid medullary carcinoma)。多發性 fibrofolliculoma 的出現也曾被描述與結締組織痣 (connective tissue nevus) 有關。fibrofolliculoma 亦曾被報告與脂肪瘤性痣 (nevus lipomatosis) 相關,以及出現於一名結節性硬化症 (tuberous sclerosis) 的病人。患有多發性 fibrofolliculoma 的病人可能同時具有多發性的毛盤瘤 (trichodiscomas) 與軟纖維瘤 (acrochorda)(即 Birt-Hogg-Dubé syndrome)。
- Fibrofolliculoma 表現為圓頂狀 (dome-shaped)、淡黃色或白色的丘疹,直徑 2–4 mm,好發於頭皮、前額、臉部與頸部(圖 31.140)。病灶也可見於胸部與背部,以及肘前窩 (antecubital fossa) 與膕窩 (popliteal fossa)。有些丘疹中央凹陷 (umbilicated) 並帶有角質栓 (keratinous plug),有些則含有毛髮。最常於人生的第三個十年 (third decade) 出現。
組織病理特徵 (Histopathology)
- Fibrofolliculoma 是一種良性的錯構瘤性 (hamartomatous) 病變,合併了毛囊周圍纖維鞘 (perifollicular fibrous sheath) 與外根鞘 (external root sheath) 的增生。它具有獨特且十分有特徵性的組織學外觀,並以漏斗部 (infundibulum) 為中心。
- 通過丘疹中央的切片可見一個發育良好的毛囊,常呈囊狀擴張 (cystically dilated),內含角質碎屑或一根毛幹 (hair shaft)(圖 31.141)。圍繞著漏斗部的是界限分明的疏鬆結締組織增生,內含細緻的膠原 (fine collagen) 與過量的玻尿酸 (hyaluronic acid)。罕見情況下,其中可含有外觀怪異的多核間質細胞 (bizarre-appearing multinucleated stromal cells),產生一種「古老型 (ancient-type)」或「假肉瘤樣 (pseudosarcomatous)」的外觀。彈性纖維 (elastic fibers) 缺如。
- 上皮條索 (epithelial strands),厚 2–4 個細胞,自漏斗部發出、相互吻合 (anastomose) 並重新匯回漏斗部,或與皮脂腺 (sebaceous gland) 的生發層 (stratum germinativum) 相連結,呈現出一種令人聯想到鷹架 (scaffolding) 的外觀(圖 31.142)。殘留的皮脂腺常被整合入此痣中。有些丘疹顯示出合併 fibrofolliculoma 與 trichodiscoma 的組織學特徵。acrochorda 則可能顯示纖維上皮性息肉 (fibroepithelial polyp) 或局灶性纖維毛囊瘤樣變化 (focal fibrofolliculomatous change) 的特徵。
[本段原文承接前文 acrochorda 之描述,OCR 順序略有錯置,依原文逐字保留:] acrochorda 最初於 1977 年被描述,現稱為 Birt-Hogg-Dubé syndrome。此種體染色體顯性的遺傳性皮膚病 (autosomal dominant genodermatosis) 在臨床上的特徵為臉部、頸部與軀幹的多發性堅實丘疹;也可能出現類似 acrochorda 的有蒂病灶 (pedunculated lesions)(圖 31.143–31.145)。重要的是,它與內臟疾病 (internal disease) 有關,特別是腎臟腫瘤 (renal tumors) 與肺部疾病,包括反覆性自發性氣胸 (recurrent spontaneous pneumothorax)、肺囊腫 (lung cysts) 與大泡性肺氣腫 (bullous emphysema)。腎臟腫瘤常為雙側性 (bilateral),並以顯性方式共分離 (cosegregate)。在組織學上,其範圍除了乳頭狀腎細胞癌 (papillary renal cell carcinoma) 之外,還涵蓋嗜酸細胞瘤 (oncocytoma) 與嫌色細胞型 (chromophobe)。曾有人提出它與腸道息肉 (intestinal polyps) 與腸道惡性腫瘤 (intestinal malignancy) 的關聯,但迄今仍不確定這是否真正屬於此症候群的一部分,因為尚未記錄到明確的證據。亦曾報告許多其他全身性表現,包括甲狀腺髓質癌 (medullary thyroid carcinoma)、甲狀腺濾泡腺瘤 (follicular adenoma of the thyroid)、甲狀腺多結節性甲狀腺腫 (multinodular goiter of the thyroid)、腮腺嗜酸細胞瘤 (oncocytoma of the parotid gland)、脈絡視網膜瘢痕 (chorioretinal scars)、多發性脂肪瘤 (multiple lipomata) 與血管脂肪瘤 (angiolipomata)、神經腫瘤 (neural tumors)、副甲狀腺腺瘤 (parathyroid adenoma)、結締組織痣 (connective tissue nevus),以及多發性臉部血管纖維瘤 (multiple facial angiofibromas)。這些關聯的意義尚不明確。
Trichodiscoma、Birt-Hogg-Dubé 與 Hornstein-Knickenberg 症候群
臨床特徵 (Clinical Features)
- 毛盤瘤 (trichodiscoma) 是毛盤 (hair disc,haarscheibe) 中胚層成分 (mesodermal component) 的錯構瘤性增生,毛盤代表一種慢適應性的機械受器 (slowly adapting mechanoreceptor)。病人表現為數以百計的小型 (1–5 mm)、無症狀、圓形、界限銳利、堅實、圓頂狀或扁平、膚色的丘疹,廣泛分布於全身。病灶有時與毳毛 (vellus hairs) 相關。並無相關的全身性異常。
- 在某些病人中,此病以體染色體顯性 (autosomal dominant) 方式遺傳。多發性 trichodiscoma 合併 fibrofolliculoma 與 [acrochorda 的關聯——OCR 順序錯置,依原文承接:]
[以下段落 OCR 順序略有錯置,依原文逐字保留:] Hornstein-Knickenberg syndrome 令人聯想到 Birt-Hogg-Dubé syndrome。其特徵為臉部、頸部與軀幹出現多發性的毛囊周圍纖維瘤 (perifollicular fibromas),表現為眾多丘疹,並合併結腸的腺瘤性息肉 (adenomatous polyps) 與腺癌 (adenocarcinoma of the colon)。較近期的資料顯示,perifollicular fibroma 與 fibrofolliculoma/trichodiscoma 很可能代表一種形態學上的連續譜 (morphological spectrum),而 Hornstein-Knickenberg syndrome 與 Birt-Hogg-Dubé syndrome 則是同一種疾病的不同表現。
致病機轉與組織病理特徵 (Pathogenesis and Histologic Features)
- 近期研究已排除了若干 Birt-Hogg-Dubé syndrome 的候選基因 (candidate genes),而易感基因座 (susceptibility locus) 已定位至第 17 號染色體 17p11.2。候選基因 (BHD) 近期已被鑑定出來,其編碼一種新型蛋白質——folliculin。雖然其確切功能與作用機轉仍屬未知,folliculin 很可能是一種腫瘤抑制基因 (tumor suppressor gene),並如同其他錯構瘤症候群 (hamartoma syndromes) 一樣,參與哺乳動物雷帕黴素標靶 (mammalian target of rapamycin,mTOR) 路徑。在 Birt-Hogg-Dubé syndrome 病人中已鑑定出 folliculin 基因的多種突變,包括插入 (insertions)、缺失 (deletions)、移碼 (frame shift) 與剪接位點突變 (splice site mutations),以及錯義 (missense) 與無義 (nonsense) 突變。
- Trichodiscoma 在地形學上總是與毛囊相關,但可能需要多張切片才能確認此點。其上覆的表皮扁平化,但在側緣有一圈領圈 (collarette)(圖 31.146)。
- 它由一種無包膜 (unencapsulated)、橢圓形、疏鬆編織的膠原、網狀纖維 (reticulin) 與細彈性纖維的混合物構成,富含酸性黏多醣 (acid mucopolysaccharides),並含有外觀溫和的梭形細胞 (bland-appearing spindle cells)(圖 31.147)。間質區偶爾可顯示脂肪瘤樣化生 (lipomatous metaplasia),並可能含有非典型間質細胞 (atypical stromal cells)。有時可見到局灶性玻璃樣變 (focal hyalinization)。一個常見的特徵是腫瘤實質內存在多條薄壁血管 (thin-walled blood vessels),並具有 PAS 陽性的基底膜 (PAS-positive basement membranes)(圖 31.148)。一條管腔狹窄、內皮細胞明顯的厚壁血管 (thick-walled vessel) 常進入腫瘤,通常自毛囊附近接近。小型梭形與星狀細胞 (fusiform and stellate cells,推測為 Schwann cells) 內的黑色素 (melanin pigment) 是其特徵。偶爾可見多核細胞 (multinucleate cells)。檢查連續切片有時可見一條周邊神經 (peripheral nerve) 進入病灶。與毛盤 (hair disc) 不同,trichodiscoma 中並無 Merkel cells。
- 以免疫組織化學而言,梭形細胞可能與 CD34 抗體反應,但對 S100、SMA、EMA 與 desmin 呈陰性。
神經毛囊性錯構瘤 (Neurofollicular Hamartoma,梭形細胞為主型 trichodiscoma)
臨床特徵 (Clinical Features)
- 神經毛囊性錯構瘤 (neurofollicular hamartoma) 是一種罕見的良性腫瘤,位於 trichodiscoma 與 fibrofolliculoma 的譜系範圍內。儘管其名稱如此,真正的神經分化 (true neural differentiation) 並非其特徵,近期已有人提出「梭形細胞為主型 trichodiscoma (spindle cell predominant trichodiscoma)」一詞以反映此點。此腫瘤現在被認為代表與 trichodiscoma 形態學連續譜中的細胞性末端 (cellular end)。
- 臨床上表現為一個小型、膚色、圓頂狀、堅實的丘疹,直徑小於 1 cm。病灶幾乎無一例外地位於臉部,並強烈好發於鼻部 (nose) 或鼻唇溝 (nasolabial fold)。成人受影響者主要在第四或第五個十年 (fourth or fifth decade),並無性別好發傾向。臨床鑑別診斷通常包括纖維性丘疹 (fibrous papule)、基底細胞癌 (basal cell carcinoma) 與真皮痣 (dermal nevus)。
組織病理特徵 (Histopathology)
- 神經毛囊性錯構瘤是一種界限分明、以真皮為基底 (dermal-based) 的腫瘤,由上皮性 (epithelial) 與間葉性 (mesenchymal) 成分構成。
- 上皮成分由扭曲且增生的毛囊皮脂腺單位 (pilosebaceous units) 構成,伴有顯著的皮脂腺,並伴隨基底樣上皮 (basaloid epithelium) 與導管上皮 (ductal epithelium) 的增生。圍繞並包埋此上皮成分的是略呈黏液樣 (myxoid) 且纖維性 (fibrillary) 的間質,內含排列成疏鬆束狀 (loosely formed fascicles) 的長形波浪狀梭形細胞 (elongate and wavy spindle cells)。可能出現局灶性柵欄狀排列 (focal palisading),並可注意到間質細胞的非典型性,即所謂的「古老型 (ancient-type)」或「假肉瘤樣 (pseudosarcomatous)」變化。其間散布著小神經分支 (small nerve twigs),肥大細胞 (mast cells) 有時很顯著。間質與上皮成分顯得緊密相關。神經毛囊性錯構瘤的特徵令人聯想到 trichodiscoma 與 fibrofolliculoma,這些病變實體可能代表一種形態學連續譜。
免疫組化 (Immunohistochemistry)
- 這些腫瘤內可鑑定出 S100 蛋白的不定表現 (variable expression)。然而,S100 的陽性很可能是存在於病灶內的 S100 陽性樹突細胞 (S100-positive dendritic cells),而非病灶的梭形細胞。此外,並無 NSE、synaptophysin、GFAP、NFP、EMA 或 Leu-7 的顯著表現,這與真正的神經分化相悖。梭形細胞表現 CD13 與 CD34,以及 CD10,而對 actin、desmin、Melan-A 與 factor XIIIa 呈陰性。
請至 ExpertConsult.com 取得完整的參考文獻清單。
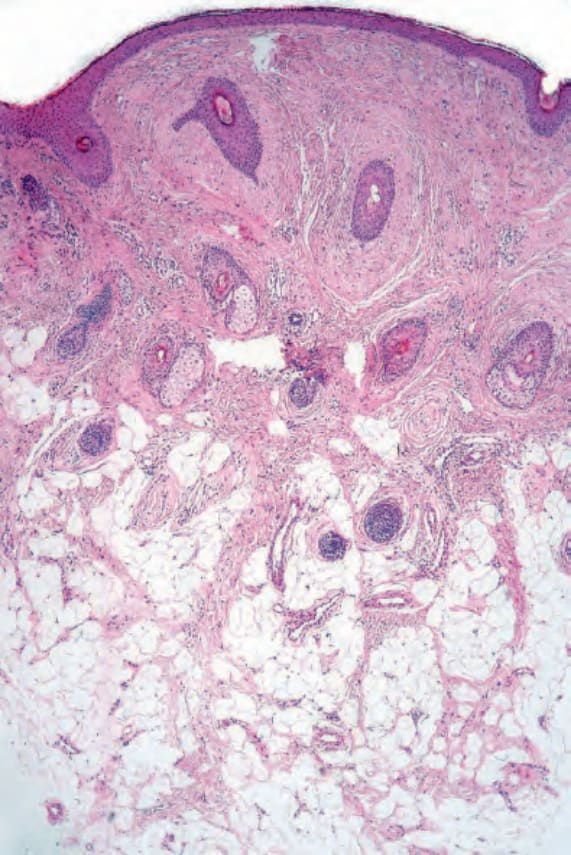
圖 31.138 毛囊周圍纖維瘤 (perifollicular fibroma):毛囊被一層緻密的結締組織鞘 (dense connective tissue sheath) 所圍繞。注意收縮假象 (retraction artifact)。
Fig. 31.138 Perifollicular fibroma: the hair follicles are surrounded by a dense connective tissue sheath. Note the retraction artifact.
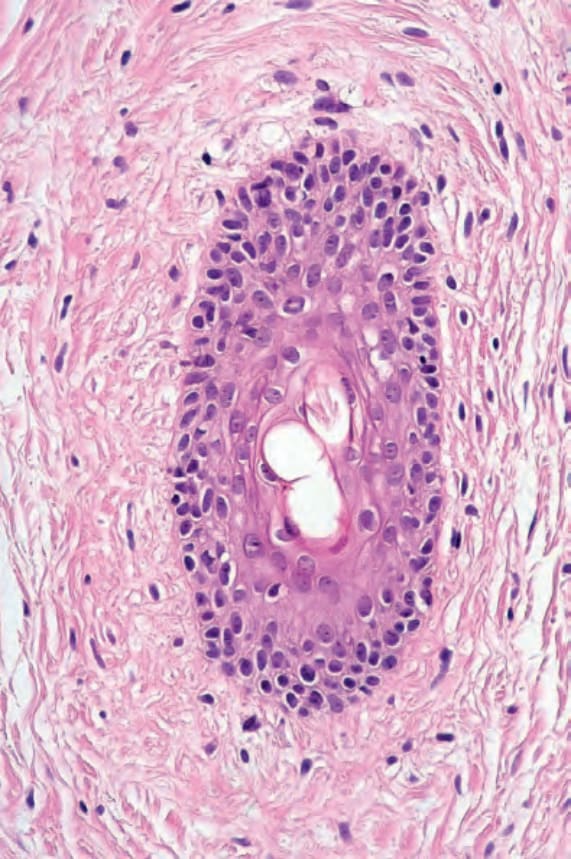
圖 31.139 毛囊周圍纖維瘤 (perifollicular fibroma):除了纖維組織之外,還有過量的醣胺聚醣 (glycosaminoglycans)。
Fig. 31.139 Perifollicular fibroma: in addition to fibrous tissue, there are excessive glycosaminoglycans.

圖 31.140 纖維毛囊瘤 (fibrofolliculoma):注意眾多淡色的臉部丘疹。By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Fig. 31.140 Fibrofolliculoma: note the numerous pale facial papules. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
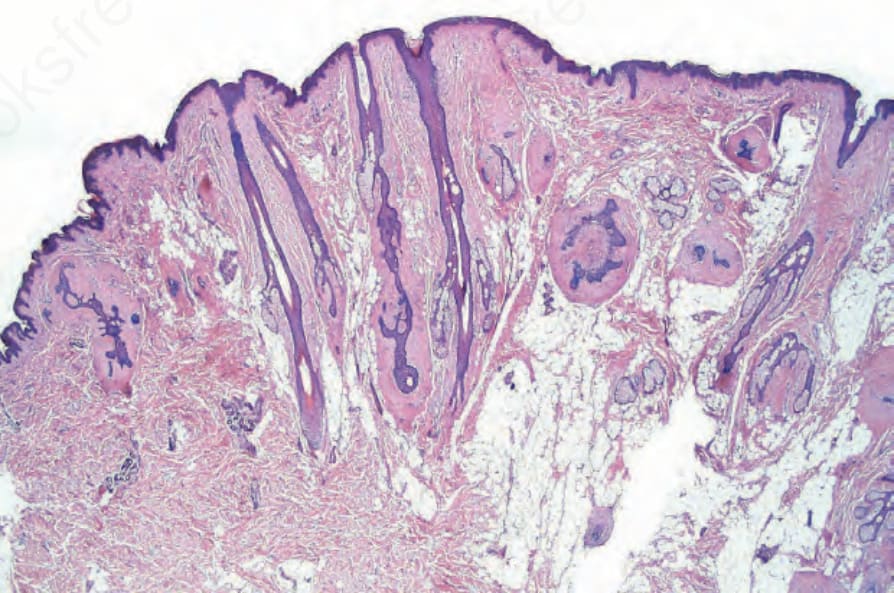
圖 31.141 纖維毛囊瘤 (fibrofolliculoma):這種外根鞘 (outer root sheath) 與毛囊周圍纖維鞘 (perifollicular fibrous sheath) 增生的組合具有特徵性診斷意義 (pathognomonic)。
Fig. 31.141 Fibrofolliculoma: this combination of outer root sheath and perifollicular fibrous sheath proliferation is pathognomonic.
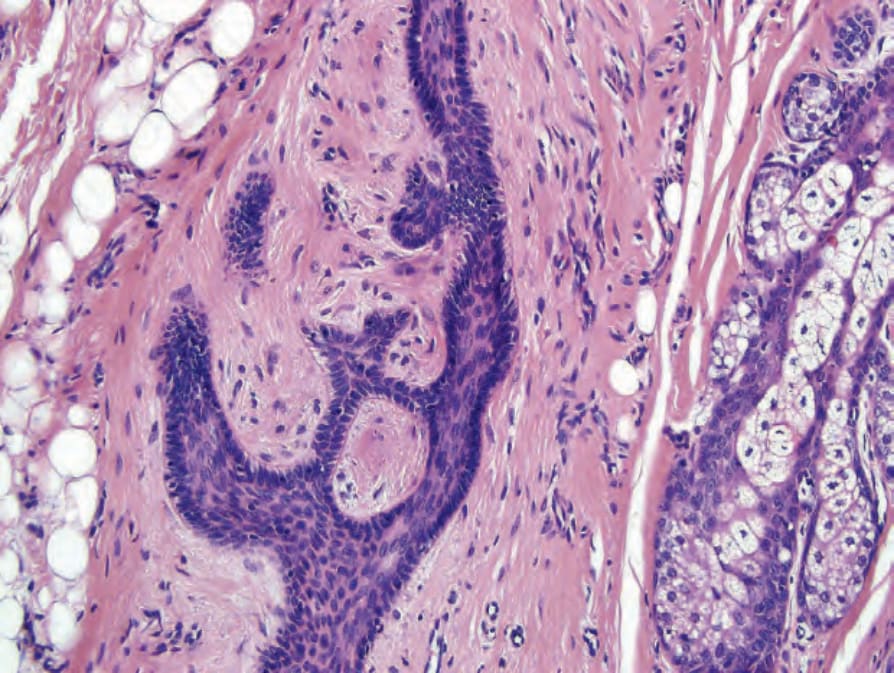
圖 31.142 纖維毛囊瘤 (fibrofolliculoma):高倍視野。
Fig. 31.142 Fibrofolliculoma: high-power view.

圖 31.143 Birt-Hogg-Dubé syndrome:注意多發性臉部丘疹。From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
Fig. 31.143 Birt-Hogg-Dubé syndrome: note multiple facial papules. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 31.144 Birt-Hogg-Dubé syndrome:可見丘疹,部分具有 acrochorda 的特徵。From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
Fig. 31.144 Birt-Hogg-Dubé syndrome: neurosis papules are seen some with features of acrochorda. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 31.145 Birt-Hogg-Dubé syndrome:丘疹性病灶可能數量眾多且融合 (confluent)。From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
Fig. 31.145 Birt-Hogg-Dubé syndrome: papular lesions can be numerous and confluent. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 31.146 毛盤瘤 (trichodiscoma):掃描視野顯示隆起的丘疹與側緣的領圈 (lateral collarette)。By courtesy of V. Liu, MD, Harvard Medical School, Boston, and E. Page, MD, Lahey Clinic, Burlington, USA.
Fig. 31.146 Trichodiscoma: scanning view showing the raised papule with lateral collarette. By courtesy of V. Liu, MD, Harvard Medical School, Boston, and E. Page, MD, Lahey Clinic, Burlington, USA.
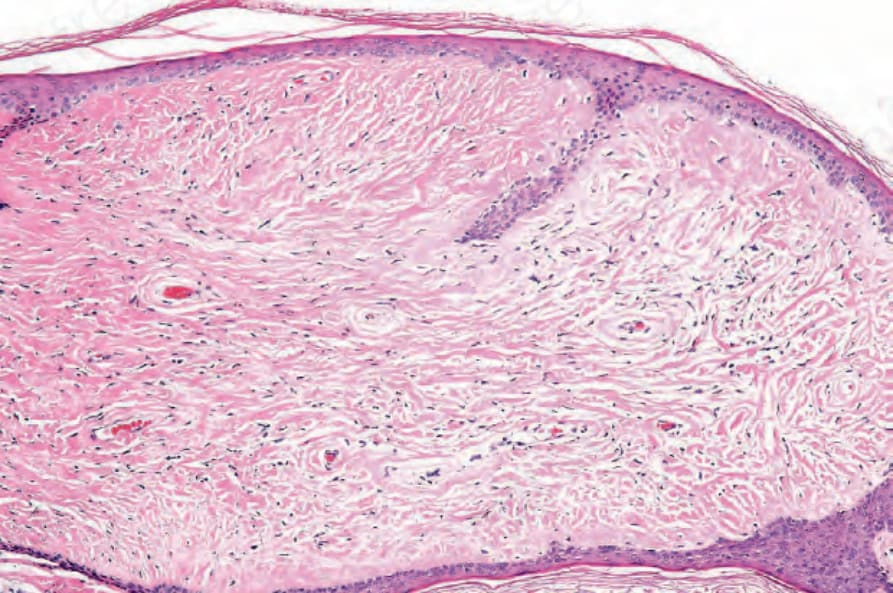
圖 31.147 毛盤瘤 (trichodiscoma):病灶的核心由水腫的結締組織 (edematous connective tissue) 構成。By courtesy of V. Liu, MD, Harvard Medical School, Boston, and E. Page, MD, Lahey Clinic, Burlington, USA.
Fig. 31.147 Trichodiscoma: the core of the lesion consists of edematous connective tissue. By courtesy of V. Liu, MD, Harvard Medical School, Boston, and E. Page, MD, Lahey Clinic, Burlington, USA.
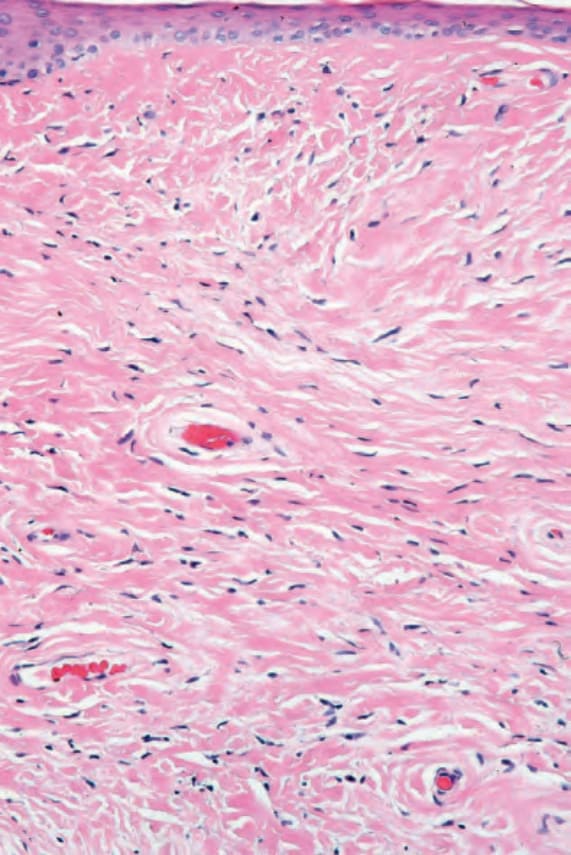
圖 31.148 毛盤瘤 (trichodiscoma):腫瘤特徵性地含有混雜的薄壁與厚壁血管 (thin- and thick-walled blood vessels)。By courtesy of V. Liu, MD, Harvard Medical School, Boston, and E. Page, MD, Lahey Clinic, Burlington, USA.
Fig. 31.148 Trichodiscoma: the tumor characteristically contains admixed thin- and thickwalled blood vessels. By courtesy of V. Liu, MD, Harvard Medical School, Boston, and E. Page, MD, Lahey Clinic, Burlington, USA.