Fibrofolliculoma
Fibrofolliculoma
Clinical features Fibrofolliculoma very rarely presents as a solitary facial papule.1,2 More often, multiple lesions are seen, which represent either an isolated condition or an autosomal dominant syndrome.1,3,4 In one instance, a series of patients with multiple fibrofolliculomas had familial thyroid medullary carcinoma.5 The presence of multiple fibrofolliculomas has also been described in association with a connective tissue nevus.6 Fibrofolliculoma has been reported in association with nevus lipomatosis and in a patient with tuberous sclerosis.7,8 Patients with multiple fibrofolliculomas may have multiple trichodiscomas and acrochorda (Birt-Hogg-Dubé syndrome).9–12
Fibrofolliculomas present as dome-shaped, pale yellow or white papules, 2–4 mm in diameter, with a predilection for the scalp, forehead, face, and neck (Fig. 31.140). Lesions may also be found on the chest and back, and antecubital and popliteal fossae.3 Some papules are umbilicated with a keratinous plug, while others contain hairs. Presentation is most common in the third decade of life.3,6,9
Histologic features Fibrofolliculoma is a benign hamartomatous condition combining proliferation of the perifollicular fibrous and external root sheaths.1,13 It has a unique and very distinctive histologic appearance, which is centered on the infundibulum. A section through the middle of a papule reveals a well-formed hair follicle, which is often cystically dilated and contains keratinous debris or a hair shaft (Fig. 31.141). Surrounding the infundibulum is a circumscribed proliferation of loose connective tissue containing fine collagen and excess hyaluronic acid. Rarely, this may contain bizarre-appearing multinucleated stromal cells, giving rise to an ancient-type or pseudosarcomatous appearance.14 Elastic fibers are absent.3,6 Epithelial strands, 2–4 cells thick, arise from the infundibulum, anastomose and rejoin the infundibulum or unite with the stratum germinativum of the sebaceous gland, to give an
1586 Tumors of the hair follicle
appearance reminiscent of scaffolding (Fig. 31.142). Residual sebaceous glands are often incorporated into the nevus. Some papules show histologic features combining fibrofolliculoma with trichodiscoma. The acrochorda may show features of a fibroepithelial polyp or focal fibrofolliculomatous change.
acrochorda was originally described in 1977 and is now referred to as the Birt-Hogg-Dubé syndrome.4,5 This autosomal dominant genodermatosis is clinically characterized by multiple firm papules on the face, neck, and trunk; pedunculated lesions resembling acrochorda may also be present (Figs 31.143–31.145). Importantly, there is an association with internal disease, especially renal tumors and lung disease including recurrent spontaneous pneumothorax, lung cysts, and bullous emphysema.6–13 Renal tumors are frequently bilateral and cosegregate in a dominant fashion. Histologically, their spectrum encompasses oncocytoma and chromophobe in addition to papillary renal cell carcinoma.7–9,14–16 An association with intestinal polyps and intestinal malignancy has been proposed, but to date it is uncertain whether this truly represents part of the syndrome since no unequivocal evidence has been documented.7,17–20 A number of other systemic manifestations have been reported including medullary thyroid carcinoma, follicular adenoma of the thyroid, multinodular goiter of the thyroid, oncocytoma of the parotid gland, chorioretinal scars, multiple lipomata and angiolipomata, neural tumors, parathyroid adenoma, connective tissue nevus, and multiple facial angiofibromas.4,6,8,17–27 The significance of these associations is unclear.
Trichodiscoma, Birt-Hogg-Dubé, and Hornstein-Knickenberg syndromes
Clinical features Trichodiscoma is a hamartomatous proliferation of the mesodermal component of the hair disc (haarscheibe), which represents a slowly adapting mechanoreceptor.1 Patients present with hundreds of small (1–5 mm) asymptomatic, round, sharply circumscribed, firm, dome-shaped or flat, flesh-colored papules, which are widely distributed about the body.1,2 Lesions are sometimes associated with vellus hairs. There are no associated systemic abnormalities.
In some patients, the condition is inherited as an autosomal dominant.3 The association of multiple trichodiscomas with fibrofolliculomas and
Hornstein-Knickenberg syndrome is reminiscent of Birt-Hogg-Dubé syndrome. It is characterized by the presence of multiple perifollicular fibromas presenting as numerous papules on the face, neck, and trunk in association
1587 Trichodiscoma, Birt-Hogg-Dubé, and Hornstein-Knickenberg syndromes
with adenomatous polyps and adenocarcinoma of the colon.28–30 More recent data suggest that perifollicular fibroma and fibrofolliculoma/trichodiscoma likely represent a morphological spectrum and that Hornstein-Knickenberg syndrome and Birt-Hogg-Dubé syndrome are manifestations of the same condition.20,31–33
Pathogenesis and histologic features Recent studies have excluded a number of candidate genes for Birt-Hogg- Dubé syndrome, and the susceptibility locus has been mapped to chromosome 17p11.2.34–37 The candidate gene (BHD) has recently been identified, and this encodes for a novel protein, folliculin.37 Although its precise function and mechanism of action remain unknown, folliculin is likely a tumor suppressor gene and involved in the mammalian target of rapamycin (mTOR) pathway similar to other hamartoma syndromes.38–40 Multiple mutations in the folliculin gene have been identified in patients with Birt-Hogg-Dubé syndrome including insertions, deletions, frame shift, and splice site mutations as well as missense and nonsense mutations.41–49
Trichodiscoma is always topographically related to a hair follicle, although multiple sections may be necessary to confirm this.1 The overlying epidermis is flattened, but laterally there is a collarette (Fig. 31.146).
It is composed of an unencapsulated, elliptical, loosely woven admixture of collagen, reticulin, and thin elastic fibers with abundant acid mucopolysaccharides and containing bland-appearing spindle cells (Fig. 31.147).1–3 Occasionally, the stromal compartment may show lipomatous metaplasia, and it may contain atypical stromal cells.50 Focal hyalinization may sometimes be evident.3 A regular feature is the presence of multiple thin-walled blood vessels with PAS-positive basement membranes within the substance of the tumor (Fig. 31.148).2 A thick-walled vessel with a narrow lumen and conspicuous endothelial cells often enters the tumor, usually approaching from the vicinity of a hair follicle. Melanin pigment within small fusiform and stellate cells (presumably Schwann cells) is characteristic. Occasionally, multinucleate cells are evident.3 Examination of serial sections sometimes
1588 Tumors of the hair follicle
reveals a peripheral nerve entering the lesion. In contrast to the hair disc, Merkel cells are not present in trichodiscoma.
By immunohistochemistry, spindle cells may react with CD34 antibodies but are negative for S100, SMA, EMA, and desmin.51,52
Neurofollicular hamartoma (spindle cell predominant trichodiscoma)
Clinical features Neurofollicular hamartoma is a rare benign tumor that lies within the spectrum of trichodiscoma and fibrofolliculoma. Despite its name, true neural differentiation is not a feature, and more recently the term ‘spindle cell predominant trichodiscoma’ has been proposed to reflect this.1 The tumor is now thought to represent the cellular end of a morphological spectrum with trichodiscoma.1 It presents clinically as a small, skin-colored, dome-shaped, firm papule, less than 1 cm in diameter.2–5 Lesions are almost invariably located on the face, with a strong predilection for the nose or nasolabial fold.2–5 Adults are affected predominantly in the fourth or fifth decade, and there is no gender predilection. The clinical differential diagnosis typically includes fibrous papule, basal cell carcinoma, and dermal nevus.
component consists of distorted and hyperplastic pilosebaceous units with prominent sebaceous glands accompanied by a proliferation of basaloid and ductal epithelium. Surrounding and embedding this epithelial component is a somewhat myxoid and fibrillary stroma containing elongate and wavy spindle cells arranged in loosely formed fascicles. Focal palisading may be present, and atypia of the stromal cells, so-called ancient-type or pseudosarcomatous change, may be noted.6,7 Small nerve twigs are interspersed and mast cells are sometimes prominent.2–5 The stromal and epithelial components appear intimately associated. The features of neurofollicular hamartoma are reminiscent of trichodiscoma and fibrofolliculoma, and these entities possibly represent a morphological spectrum.3
Histologic features Neurofollicular hamartoma is a well-circumscribed, dermal-based tumor composed of epithelial and mesenchymal components.2–5 The epithelial
Variable expression of S100 protein is identified within these tumors.2–5 However, S100 positivity is likely present within intralesional S100-positive dendritic cells rather than the lesional spindle cells.1,3 Furthermore, there is no significant expression of NSE, synaptophysin, GFAP, NFP, EMA, or Leu-7, arguing against true neural differentiation.1–5 Spindle cells express CD13 and CD34 as well as CD10 and are negative for actin, desmin, Melan-A, and factor XIIIa.1,8
Access ExpertConsult.com for the complete list of references
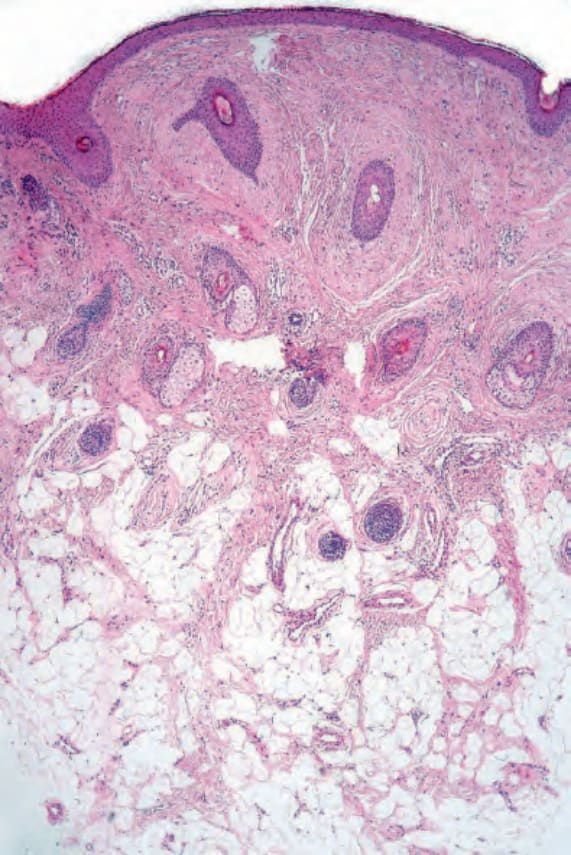
Fig. 31.138 Perifollicular fibroma: the hair follicles are surrounded by a dense connective tissue sheath. Note the retraction artifact.
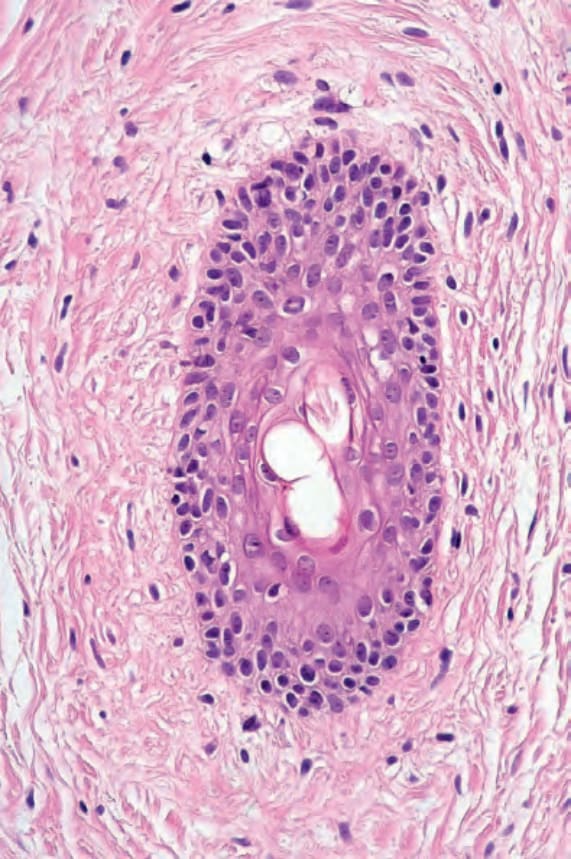
Fig. 31.139 Perifollicular fibroma: in addition to fibrous tissue, there are excessive glycosaminoglycans.

Fig. 31.140 Fibrofolliculoma: note the numerous pale facial papules. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
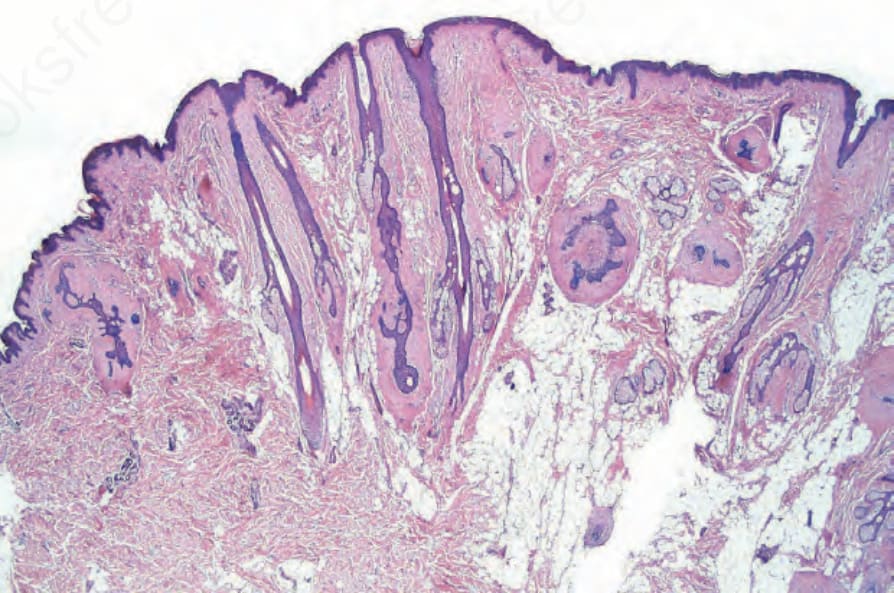
Fig. 31.141 Fibrofolliculoma: this combination of outer root sheath and perifollicular fibrous sheath proliferation is pathognomonic.
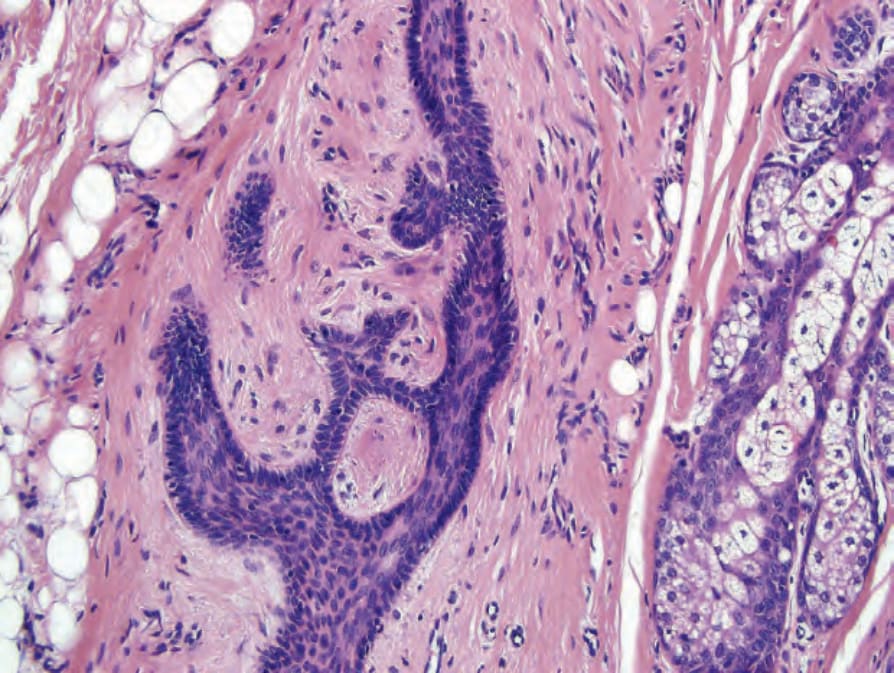
Fig. 31.142 Fibrofolliculoma: high-power view.

Fig. 31.143 Birt-Hogg-Dubé syndrome: note multiple facial papules. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 31.144 Birt-Hogg-Dubé syndrome: neurosis papules are seen some with features of acrochorda. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 31.145 Birt-Hogg-Dubé syndrome: papular lesions can be numerous and confluent. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 31.146 Trichodiscoma: scanning view showing the raised papule with lateral collarette. By courtesy of V. Liu, MD, Harvard Medical School, Boston, and E. Page, MD, Lahey Clinic, Burlington, USA.
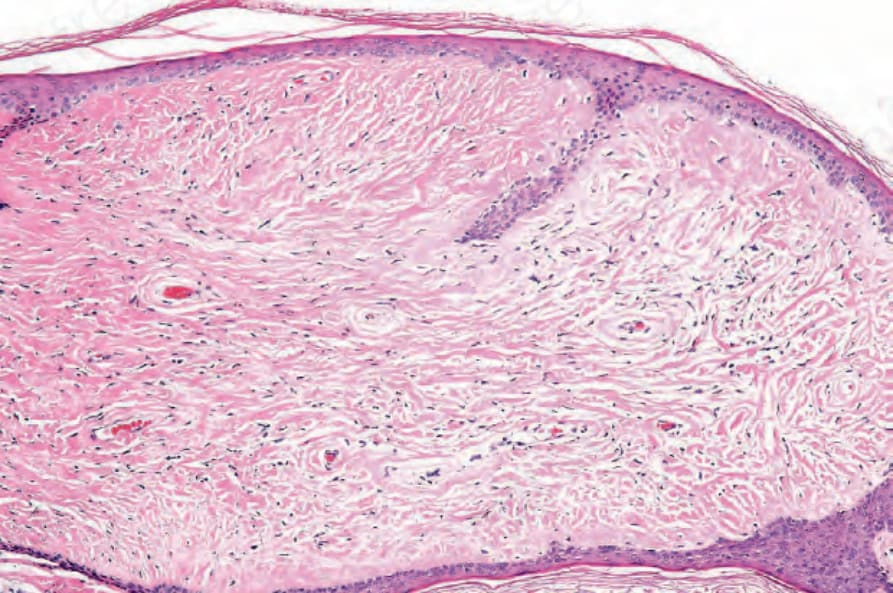
Fig. 31.147 Trichodiscoma: the core of the lesion consists of edematous connective tissue. By courtesy of V. Liu, MD, Harvard Medical School, Boston, and E. Page, MD, Lahey Clinic, Burlington, USA.
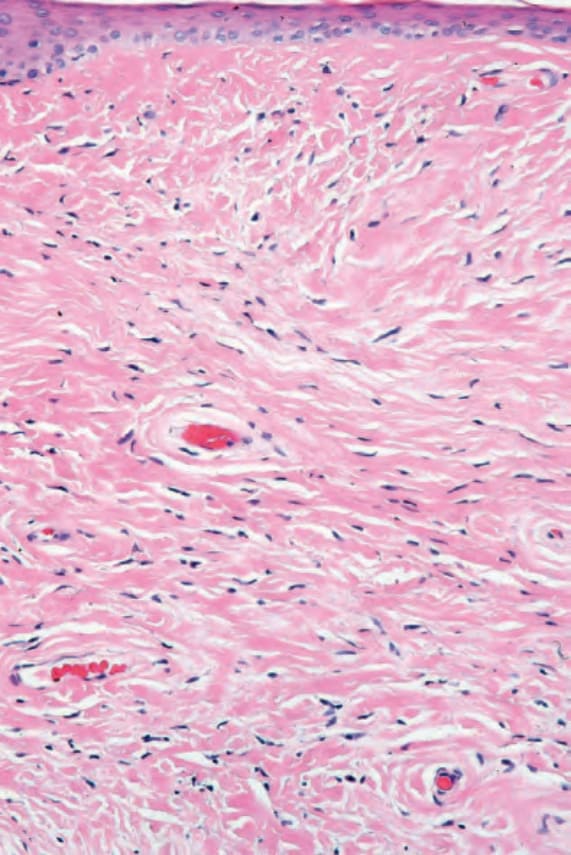
Fig. 31.148 Trichodiscoma: the tumor characteristically contains admixed thin- and thickwalled blood vessels. By courtesy of V. Liu, MD, Harvard Medical School, Boston, and E. Page, MD, Lahey Clinic, Burlington, USA.