毛上皮瘤 (Trichoepithelioma)
疾病定義與分類
毛上皮瘤 (trichoepithelioma) 是一種錯構瘤性 (hamartomatous) 病變,其毛囊分化程度低於毛囊瘤 (trichofolliculoma)。病灶可為多發且具家族性,亦可為單發。
臨床特徵 (Clinical Features)
多發性家族性毛上皮瘤 (Multiple familial trichoepithelioma) 多發性家族性毛上皮瘤(epithelioma adenoides cysticum [Brooke])以體染色體顯性 (autosomal dominant) 方式遺傳,男性表現減弱,發病時間在青春期。患者表現為多發、小型、膚色丘疹,呈大致對稱分布,主要位於臉部(圖 31.89 與 31.90)。最常侵犯鼻唇溝、眉部、眼瞼與兩頰。其他部位包括頭皮、頸部、四肢、臀部與生殖器區域亦可受侵犯。病灶通常無症狀,起初為半透明的膚色丘疹,有時表面可見輕微微血管擴張 (telangiectasia)。它們緩慢增大,最大直徑約達 0.5 cm。罕見情況下會發生潰瘍,通常發生於非常晚期。病灶偶爾呈色素沉著。亦曾報告呈線狀與皮節 (dermatomal) 分布。
epithelioma adenoides cysticum 患者鮮少發生任何明顯的全身性表現。然而,曾有報告與腎臟及肺臟囊腫,以及腮腺 (parotid gland) 的惡性淋巴上皮病變 (malignant lymphoepithelial lesion) 有所關聯。極為罕見的情況下,可發現並存的基底細胞癌 (basal cell carcinoma)。
雖然最初的基因連鎖分析 (genetic linkage analysis) 將本病定位至第 9 號染色體 9p21 區域,但後續研究未能證實此一觀察。取而代之的是,在多個家族中持續發現第 16 號染色體 16q12-q13 上 CYLD 基因 (CYLD gene) 的突變,與 Brooke-Spiegler syndrome 相似。這些資料強調,多發性家族性毛上皮瘤可能確實代表一個疾病譜系的一部分,此譜系亦包括家族性圓柱瘤病 (familial cylindromatosis) 與 Brooke-Spiegler syndrome。
Rombo 症候群 (Rombo syndrome) Rombo syndrome 包含多發性毛上皮瘤、粟粒疹 (milia)、蠕蟲狀萎縮 (vermiculate atrophy)、基底細胞癌、毳毛囊腫 (vellus hair cysts)、周邊血管擴張 (peripheral vasodilatation) 與發紺 (cyanosis)。此為極為罕見之疾病,可能為體染色體顯性遺傳模式。皮膚病灶在兒童期出現,基底細胞癌則於成年早期發生。
另有一種家族性型態與指甲營養不良 (nail dystrophy)、禿髮 (alopecia) 與重症肌無力 (myasthenia gravis) 有所關聯。
單發性毛上皮瘤 (Solitary trichoepithelioma) 單發性毛上皮瘤通常表現為成人臉部一個直徑 0.5 cm、無症狀、膚色的結節。偶爾見於其他部位,包括頭皮、頸部、背部、外陰 (vulva)、陰阜 (mons pubis) 與四肢近端。
Brooke-Spiegler 症候群 (Brooke-Spiegler syndrome) 體染色體顯性的 Brooke-Spiegler syndrome(家族性圓柱瘤病 [familial cylindromatosis] 或頭巾瘤症候群 [turban tumor syndrome])的特徵為多發性圓柱瘤 (cylindromas),外加螺旋腺瘤 (spiradenomas)、多發性毛上皮瘤與粟粒疹。雖然外顯率 (penetrance) 很高,但患者間的表現變異甚大。在同一家族中,有些患者可能僅表現多發性圓柱瘤或毛上皮瘤,或兩者兼具。患者於成年早期出現皮膚病灶,並有女性偏好。圓柱瘤典型出現於頭皮,可長至大型且融合(頭巾瘤 [turban tumor]),而多發性毛上皮瘤則主要位於臉部中央。腫瘤常顯示混合特徵,如螺旋腺圓柱瘤 (spiradenocylindromas),皮脂腺分化 (sebaceous differentiation) 亦可能為一項特徵。患者亦會發生其他毛囊腫瘤,如毛母細胞瘤 (trichoblastoma) 與皮膚淋巴腺瘤 (cutaneous lymphadenoma)。額外的汗管瘤 (syringomas) 罕見,可能為偶發性關聯。腮腺腫瘤如膜性型基底細胞腺瘤 (membranous-type basal cell adenoma)——圓柱瘤的組織學擬態——亦罕見發生,乳腺實質的圓柱瘤亦然。唾液腺腫瘤以及圓柱瘤皆偶爾發生惡性變化。在 Brooke-Spiegler syndrome 與多發性家族性毛上皮瘤患者中,亦曾記錄毛上皮瘤的惡性轉化(高惡性度毛母細胞癌 [high-grade trichoblastic carcinoma])與癌肉瘤 (carcinosarcoma) 的發生。
毛上皮瘤偶爾與黑色素細胞性 (melanocytic)(普通型 [banal] 或藍色 [blue])及表皮 (epidermal) 母斑 (nevi) 有所關聯。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
Brooke-Spiegler syndrome 近期被定位至第 16 號染色體 16q12-13 位點,候選基因被鑑定為腫瘤抑制基因 (tumor suppressor gene) CYLD。曾報告導致 CYLD 基因失活的突變,腫瘤顯示野生型 (wild-type) 拷貝的異質性喪失 (loss of heterozygosity),此為腫瘤抑制基因的特徵性發現。CYLD 突變現亦在多發性家族性毛上皮瘤與家族性圓柱瘤病的家族中被鑑定出,顯示同一潛在疾病的表現型變異 (phenotypic variation)。然而,迄今尚未出現基因型—表現型 (genotype–phenotype) 的相關性。
更近期,對 CYLD 分子功能的見解已有所進展。CYLD 是一種去泛素化蛋白 (deubiquinating protein),藉由標靶多個重要的訊號分子如 TRAF2(tumor necrosis factor receptor-associated factor 2,腫瘤壞死因子受體相關因子 2)、NEMO 以及 bcl-3 等,干擾 tumor necrosis factor alpha (TNF-α)/NF-κb 路徑。因此 CYLD 參與調節多種重要功能,包括發炎、細胞存活、增殖與腫瘤生成 (tumorigenesis)。CYLD 缺乏導致組成型 (constitutive) NF-κb 路徑活化以及凋亡 (apoptosis) 減少。然而,NF-κb 路徑活化如何參與腫瘤生成的確切機制,目前尚未完全明瞭。
毛上皮瘤的角蛋白表現譜 (keratin expression profiles) 顯示朝向外毛根鞘 (outer root sheath) 的分化。與多發性家族性毛上皮瘤及 Brooke-Spiegler syndrome 的資料相反,Shh 訊號路徑 (Shh signaling pathway) 似乎參與單發性毛上皮瘤的致病機轉。與基底細胞癌相似,在一部分毛上皮瘤中偵測到 patched 基因 (PTCH) 的體細胞突變 (somatic mutations) 與異質性喪失。過度表現 GLI-1(一種參與 Shh 訊號路徑的蛋白)的轉殖基因小鼠 (transgenic mice) 會發生基底細胞癌以及讓人聯想到毛上皮瘤與圓柱瘤的附屬器腫瘤 (adnexal tumors),且在基底細胞癌與毛上皮瘤中皆偵測到高 GLI-1 轉錄本 (transcript) 水平。
腫瘤有時顯示與表皮的連續性,該表皮可能呈現正常,或輕度角化過度 (hyperkeratotic) 且變薄,並喪失表皮突 (rete ridge) 樣式。然而,潰瘍極為罕見。典型的毛上皮瘤特徵為真皮內以及基底樣細胞 (basaloid cells) 小葉內出現多數游離的角質囊腫 (horn cysts)(圖 31.91 與 31.92)。與角質囊腫混雜的是與基底細胞癌無法區分的腫瘤細胞小葉,呈嗜鹼性 (basophilic)、胞質極少並顯示周邊柵欄狀排列 (peripheral palisading)(圖 31.93)。然而,在毛上皮瘤中,小葉周圍的結締組織鞘 (perilobular connective tissue sheath) 較為顯著,且常伴隨形成上皮旁 (juxtaepithelial) 的圓形或卵圓形纖維母細胞聚集——乳頭狀間質體 (papillary mesenchymal bodies)(圖 31.94)。一般認為這些代表原始的乳頭狀間質 (primitive papillary mesenchyme)。它們有時會凹陷壓迫小葉,產生毛球樣 (hair bulblike) 外觀。基底樣細胞小葉常伴隨纖細的上皮樣條索 (epithelioid strands),造成葉狀 (frondlike) 外觀(圖 31.95)。毛上皮瘤不算少見地對游離角蛋白顯示異物巨細胞反應 (foreign body giant cell reaction),偶爾可見鈣化灶。澱粉樣物質沉積 (amyloid deposits) 不常見。
然而,有些毛上皮瘤可能顯示極少的角蛋白囊腫形成。取而代之的是,腫瘤由一個相當界限分明的病變組成,其中離散的基底樣細胞小葉廣泛散布於豐富的結締組織間質 (connective tissue stroma) 中(圖 31.96 與 31.97)。具此特定樣式的腫瘤可能發生於臉部以外的部位。罕見情況下,曾在腫瘤小葉中觀察到上皮巨細胞與多核形態。

圖 31.101:促結締組織增生性毛上皮瘤 (desmoplastic trichoepithelioma):在此例中,毛囊起源 (follicular origin) 明顯可見。
Fig. 31.101 Desmoplastic trichoepithelioma: in this example, a follicular origin is evident.
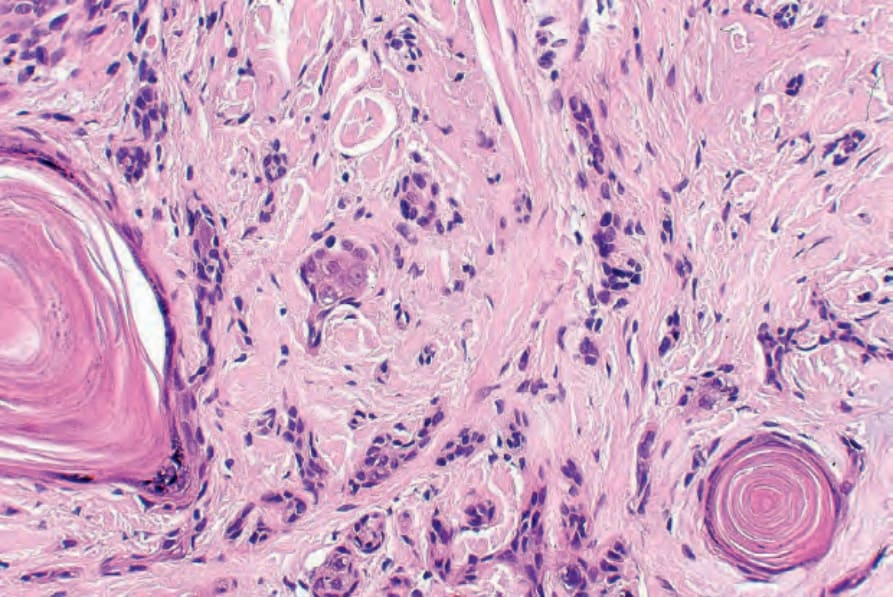
圖 31.103:促結締組織增生性毛上皮瘤 (desmoplastic trichoepithelioma):囊腫顯示表皮樣角化 (epidermoid keratinization)。
Fig. 31.103 Desmoplastic trichoepithelioma: the cysts show epidermoid keratinization.
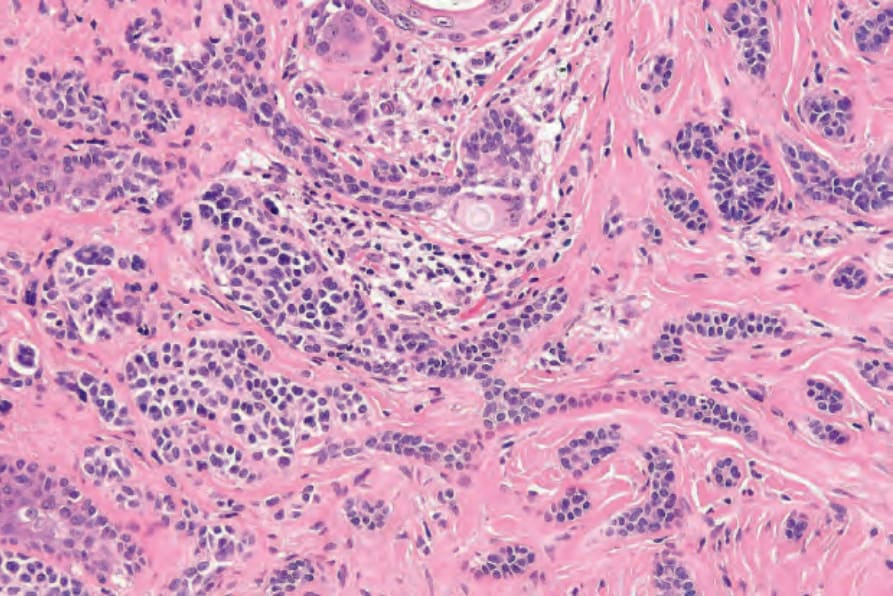
圖 31.106:促結締組織增生性毛上皮瘤 (desmoplastic trichoepithelioma):高倍視野。
Fig. 31.106 Desmoplastic trichoepithelioma: high-power view.

圖 31.87:正中鼻部皮樣瘻管 (median nasal dermoid fistula):突出的白色毛髮之存在為其特徵。承蒙 D. Shuttleworth, MD, University of Wales, Cardiff, UK 提供。
Fig. 31.87 Median nasal dermoid fistula: the presence of protruding white hairs is characteristic. By courtesy of D. Shuttleworth, MD, University of Wales, Cardiff, UK.
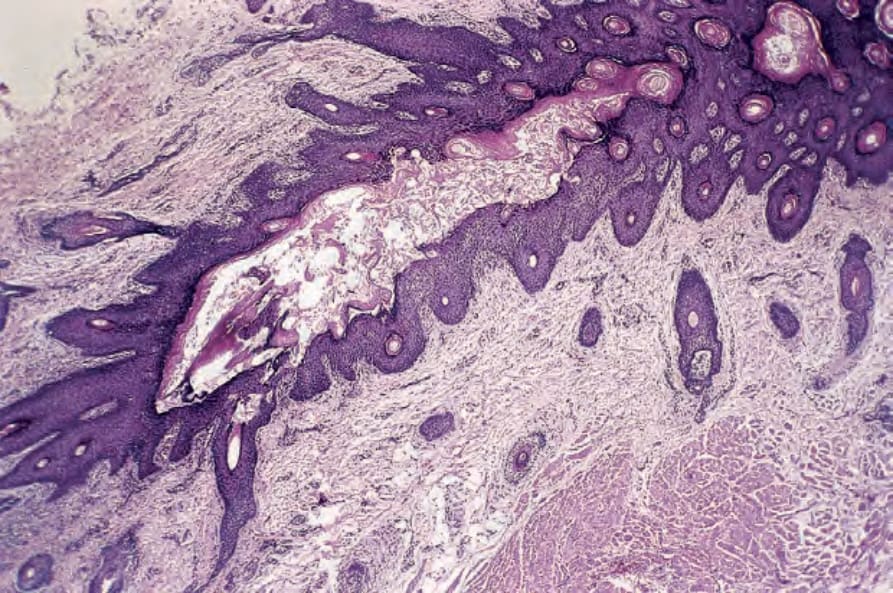
圖 31.88:正中鼻部皮樣瘻管 (median nasal dermoid fistula):此瘻管與表面表皮相通,襯以含毛上皮 (hair-bearing epithelium)。承蒙 D. Shuttleworth, MD, University of Wales, Cardiff, UK 提供。
Fig. 31.88 Median nasal dermoid fistula: the fistula, which communicates with the surface epidermis, is lined by hair-bearing epithelium. By courtesy of D. Shuttleworth, MD, University of Wales, Cardiff, UK.
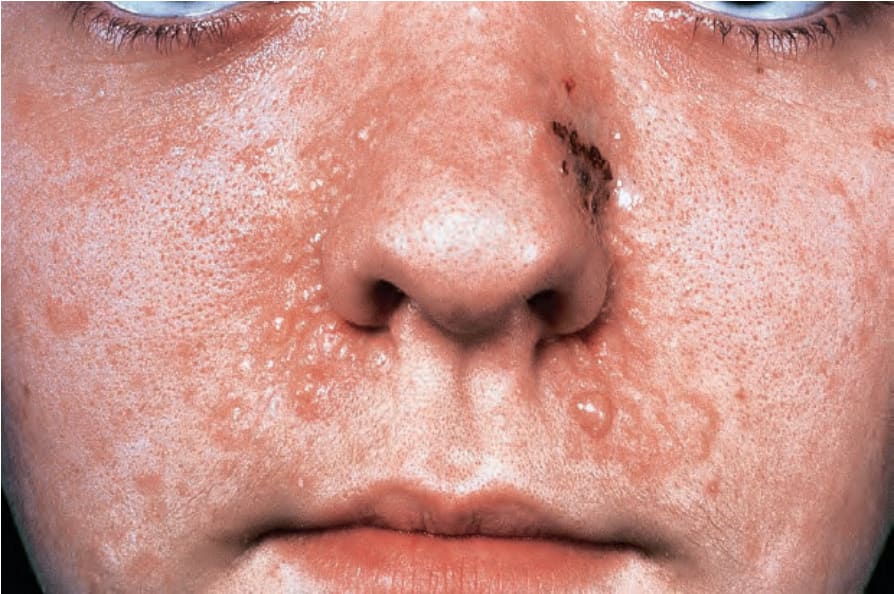
圖 31.89:毛上皮瘤 (trichoepithelioma):此患者有家族性多發性毛上皮瘤。注意鼻唇溝周圍存在多發的膚色丘疹。承蒙 the Institute of Dermatology, London, UK 提供。
Fig. 31.89 Trichoepithelioma: this patient has familial multiple trichoepitheliomas. Note the presence of multiple skin-colored papules about the nasolabial folds. By courtesy of the Institute of Dermatology, London, UK.

圖 31.90:毛上皮瘤 (trichoepitheliomas):注意此女孩頭皮與前額上眾多的膚色丘疹與結節。承蒙 R.A. Marsden, MD, St George’s Hospital, London, UK 提供。
Fig. 31.90 Trichoepitheliomas: note the numerous skin-colored papules and nodules on this girl’s scalp and forehead. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
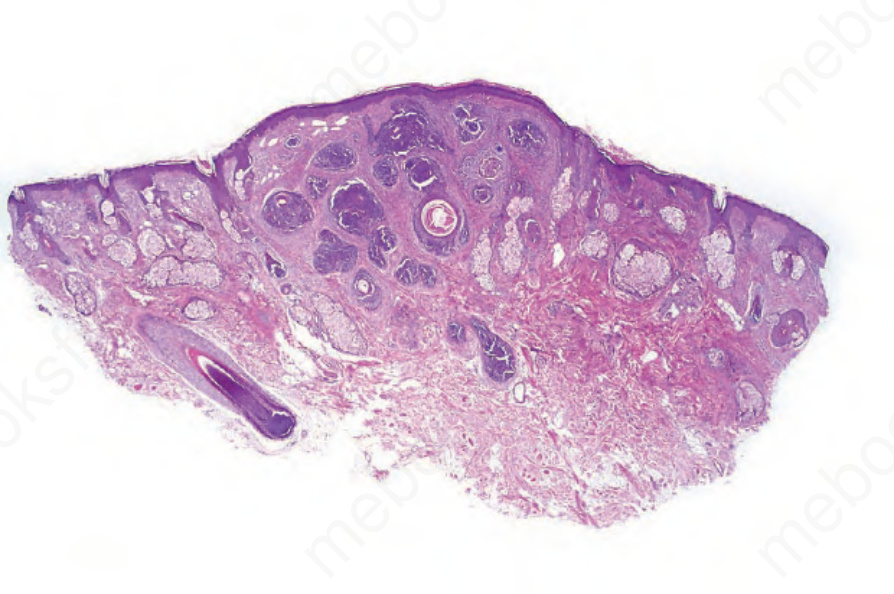
圖 31.91:毛上皮瘤 (trichoepithelioma):此掃描視野顯示基底樣細胞小葉與角質囊腫 (keratocysts) 的典型外觀。
Fig. 31.91 Trichoepithelioma: this scanning view shows the typical appearances of lobules of basaloid cells and keratocysts.
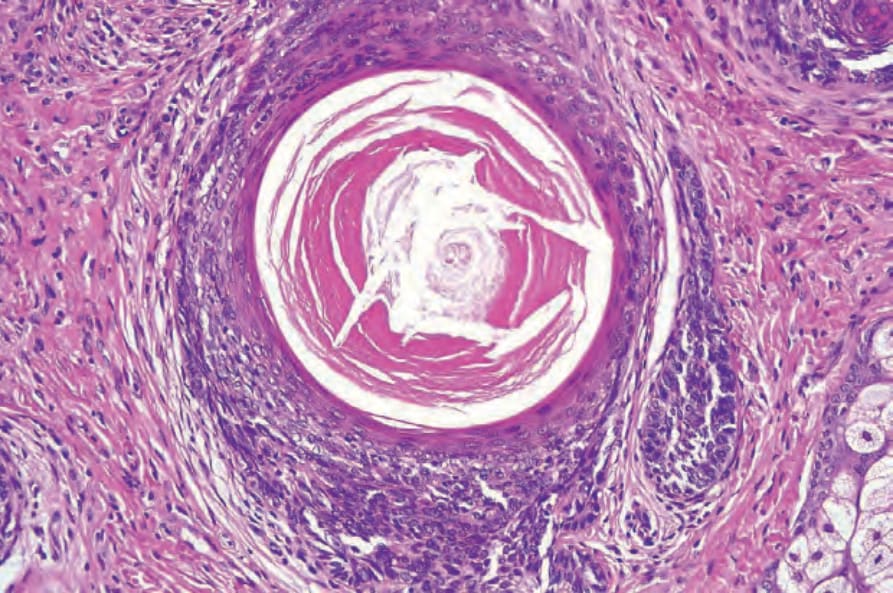
圖 31.92:毛上皮瘤 (trichoepithelioma):角質囊腫顯示漏斗部角化 (infundibular keratinization)。
Fig. 31.92 Trichoepithelioma: the keratocysts show infundibular keratinization.
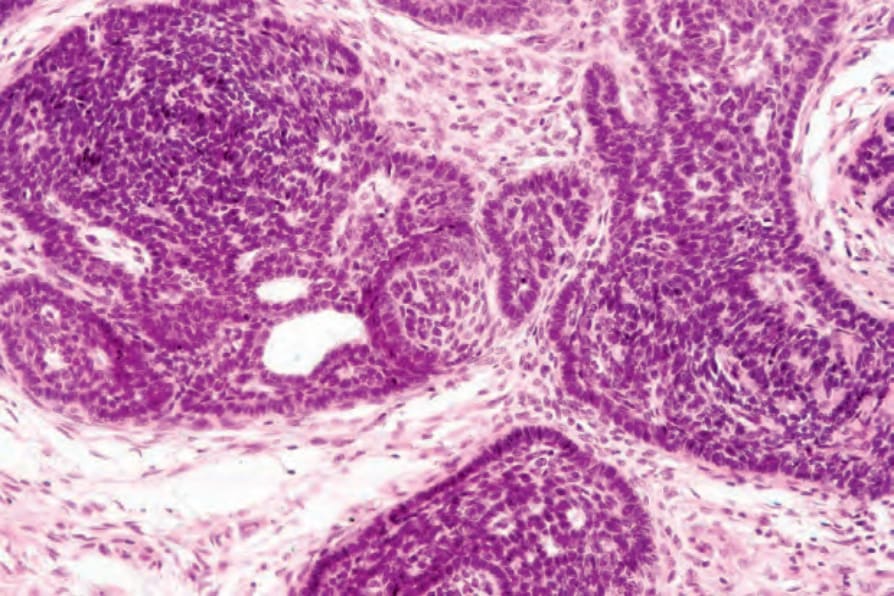
圖 31.93:毛上皮瘤 (trichoepithelioma):在此區域,腫瘤小葉顯示顯著的周邊柵欄狀排列 (peripheral palisading),並被緻密的結締組織鞘包覆。視野中央可見一乳頭狀間質體 (papillary mesenchymal body)。
Fig. 31.93 Trichoepithelioma: in this area, the tumor lobules show conspicuous peripheral palisading and are enveloped in a dense connective tissue sheath. A papillary mesenchymal body is evident in the center of the field.
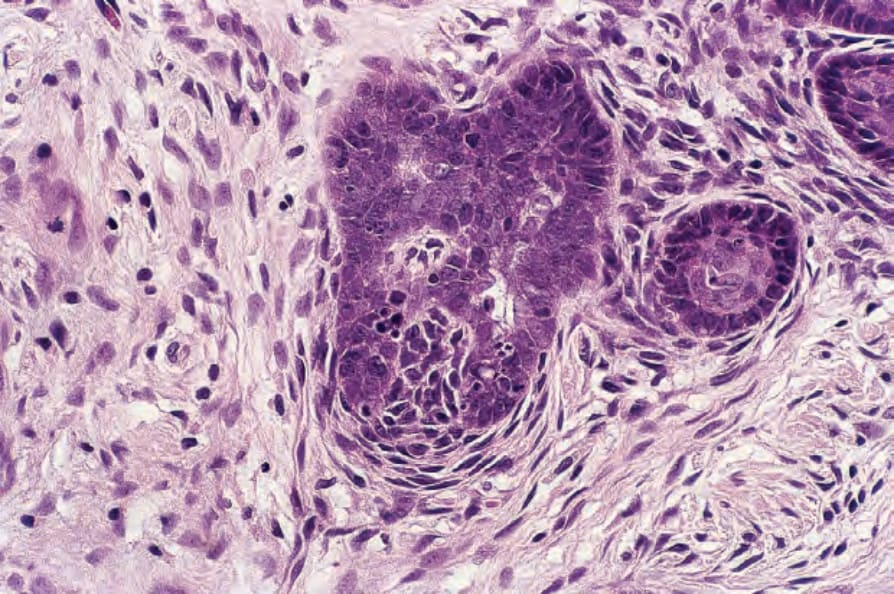
圖 31.94:毛上皮瘤 (trichoepithelioma):乳頭狀間質體 (papillary mesenchymal body) 的高倍視野。
Fig. 31.94 Trichoepithelioma: high-power view of a papillary mesenchymal body.
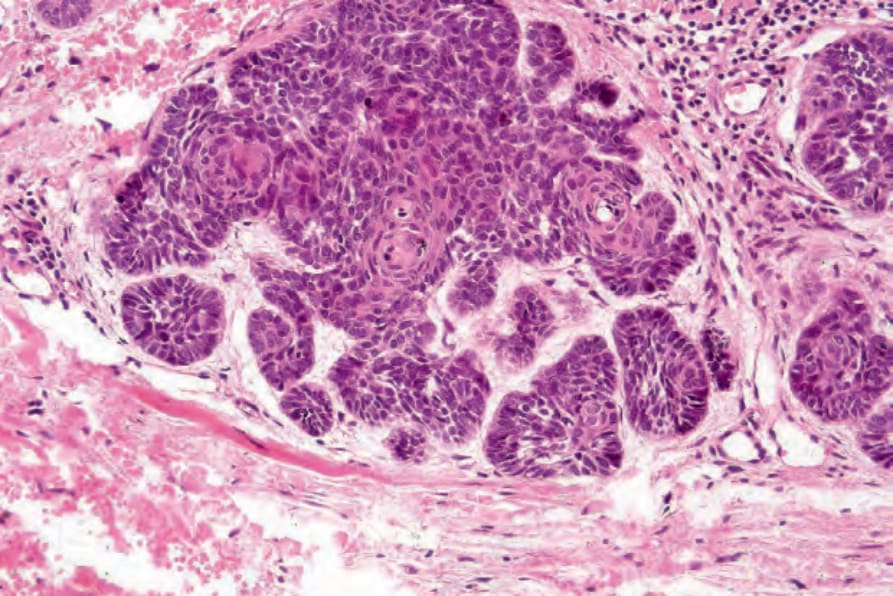
圖 31.95:毛上皮瘤 (trichoepithelioma):在此視野中,腫瘤呈現精緻的葉狀 (frondlike) 樣式。
Fig. 31.95 Trichoepithelioma: in this view, the tumor has a delicate frondlike pattern.
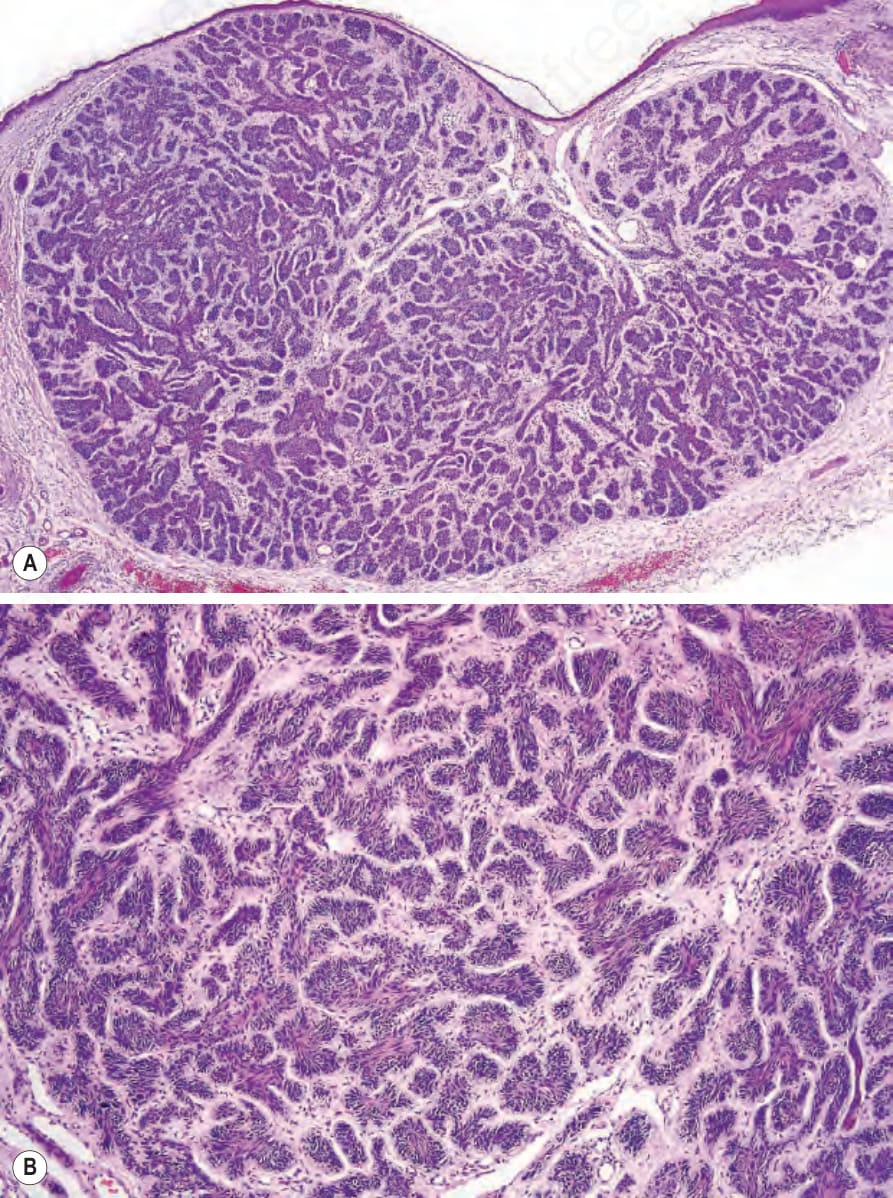
圖 31.96 (A, B):毛上皮瘤 (trichoepithelioma):在此例中,腫瘤由被緻密纖維性間質包圍的小型嗜鹼性小葉構成。並無角質囊腫 (keratocysts) 存在。
Fig. 31.96 (A, B) Trichoepithelioma: in this example, the tumor is composed of small basophilic lobules surrounded by a dense fibrous stroma. Keratocysts are not present.
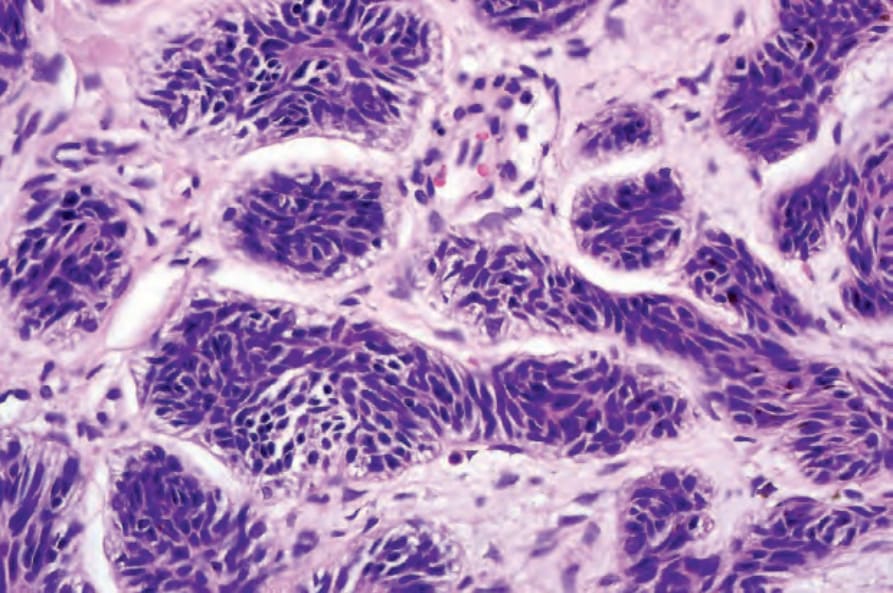
圖 31.97:毛上皮瘤 (trichoepithelioma):腫瘤由具有均勻深染細胞核的小細胞構成。
Fig. 31.97 Trichoepithelioma: the tumor is composed of small cells with uniform darkly staining nuclei.

圖 31.99:促結締組織增生性毛上皮瘤 (desmoplastic trichoepithelioma):此鼻部之病例表現為一個凹陷的瘢痕區域。承蒙 the Institute of Dermatology, London, UK 提供。
Fig. 31.99 Desmoplastic trichoepithelioma: this example on the nose presented as a depressed area of scarring. By courtesy of the Institute of Dermatology, London, UK.
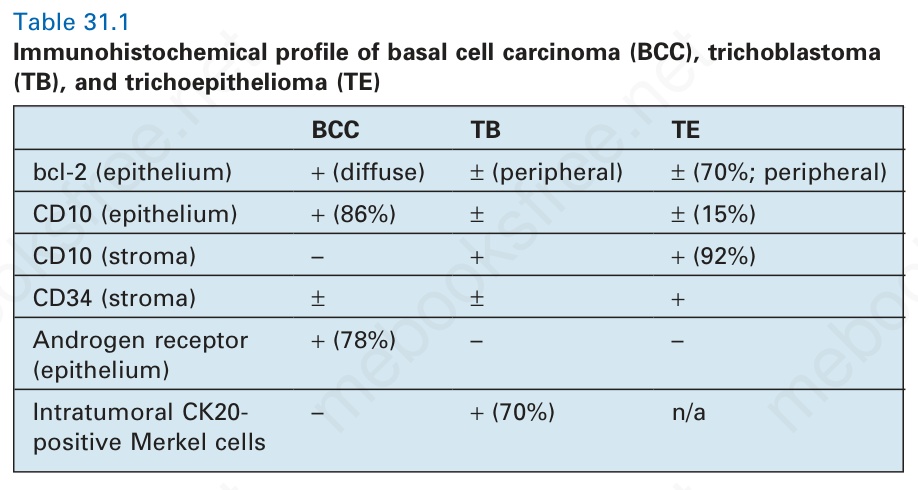
表 31.1:基底細胞癌 (basal cell carcinoma, BCC)、毛母細胞瘤 (trichoblastoma, TB) 與毛上皮瘤 (trichoepithelioma, TE) 之免疫組織化學特徵 (immunohistochemical profile)。
Table 31.1 Immunohistochemical profile of basal cell carcinoma (BCC), trichoblastoma (TB), and trichoepithelioma (TE)
毛上皮瘤與毛母細胞瘤 (trichoblastoma) 顯示相當大的組織學重疊,事實上有些作者可能將其歸類為毛母細胞瘤。
鑑別診斷 (Differential Diagnosis)
有時候毛上皮瘤的組織學外觀難以與角化型基底細胞癌 (keratotic basal cell carcinoma) 區分。潰瘍的存在和(或)伴有黏液 (mucin) 沉積的顯著腫瘤—間質回縮假象 (tumor–stroma retraction artifact) 支持後者(基底細胞癌),而顯著的上皮葉狀形成,尤其是伴有毛球形成的乳頭狀間質體 (papillary mesenchymal body),則指向前者(毛上皮瘤)。有絲分裂象 (mitotic figures) 與凋亡細胞 (apoptotic cells) 在兩種情況中皆可能存在。免疫組織化學 (immunohistochemistry) 在鑑別診斷中可能扮演有用的角色,雖然細胞角蛋白 (cytokeratin, CK) 的表現樣式大致相似。只有 CK15——在大多數毛上皮瘤中表現但不在基底細胞癌中表現——似乎具有某種價值。bcl-2 的表現在基底細胞癌中一貫為瀰漫性 (diffuse),而在毛上皮瘤中則主要為周邊性 (peripheral)。PHLDA1 在大多數毛上皮瘤中表現,而在基底細胞癌中則常喪失。與毛上皮瘤相比,基底細胞癌的 MIB-1 增殖指數 (proliferative index) 與 p53 核染色增加,且雄性素受體 (androgen receptor) 表現見於大多數基底細胞癌,而在毛上皮瘤中則不存在。此外,毛上皮瘤周圍的間質含有 CD34+ 細胞,而這些在基底細胞癌中則大致缺乏。毛上皮瘤中的 CD10 染色主要位於間質而非上皮成分,基底細胞癌則相反(表 31.1)。然而,上述免疫組織化學染色皆無法在鑑別診斷中完全可靠地使用,不應依賴。眾多臉部小丘疹的臨床病史高度提示 epithelioma adenoides cysticum。若病灶為單發且診斷有疑慮,將其當作角化型基底細胞癌處理,可能最符合患者的安全利益。
促結締組織增生性毛上皮瘤(硬化性上皮錯構瘤)(Desmoplastic trichoepithelioma [sclerosing epithelial hamartoma])
疾病定義與分類
促結締組織增生性毛上皮瘤 (Desmoplastic trichoepithelioma) 最初被認為代表毛上皮瘤的汗管樣 (syringoid) 變異型。其後同時被描述為 desmoplastic trichoepithelioma 與 sclerosing epithelial hamartoma。
促結締組織增生性毛上皮瘤並不見於患有多發性毛上皮瘤症候群 (multiple trichoepithelioma syndromes) 的患者,且家族性發生極為例外。
臨床特徵 (Clinical Features)
促結締組織增生性毛上皮瘤是一種無症狀、緩慢生長的病變,通常出現於年輕成人的臉部或頸部,好發部位為兩頰、下巴與前額(圖 31.98 與 31.99)。先天性表現罕見。病灶通常為單發,雖然偶爾有患有多發性腫瘤的患者被記錄。它顯示女性偏好(4:1)。腫瘤直徑為 3–8 mm、堅硬且環狀,呈白色或黃色,具凹陷或萎縮的中心與隆起的邊緣。典型上,病灶不潰瘍。偶爾亦可見粟粒疹 (milia)。
組織學特徵 (Histologic Features)
促結締組織增生性毛上皮瘤與傳統的毛上皮瘤相當不同。它由三聯徵 (triad) 構成:狹窄的上皮條索 (narrow epithelial strands)、角質囊腫 (keratinous cysts) 與促結締組織增生性間質 (desmoplastic stroma)(圖 31.100 與 31.101)。
表皮可能正常、萎縮或輕度棘層肥厚 (acanthotic)。顯著的假性上皮瘤樣增生 (pseudoepitheliomatous hyperplasia) 是罕見的發現。偶爾可見中央凹陷。位於真皮上部與中部的是線狀與分支狀上皮條索與角化囊腫的不定混合,鑲嵌於緻密的纖維性、常為膠原性 (collagenous) 的間質中(圖 31.102 與 31.103)。囊腫由周邊一圈具有顯著細胞核與稀少胞質的小型立方狀基底細胞 (cuboidal basal cells) 構成。這些細胞成熟形成鱗狀上皮 (squamous epithelium),後者再進行表皮樣角化 (epidermoid keratinization)。上皮條索有時從囊壁出芽。因角蛋白釋出造成的異物巨細胞反應 (foreign body giant cell reaction) 非常常見。鈣化亦常見,偶爾發生骨形成 (bone formation)(圖 31.104)。
上皮條索(有時與表皮相連)由排列成 1–3 個細胞厚之層的小型立方狀基底樣細胞構成。有絲分裂活性極為罕見,多形性 (pleomorphism) 從不為其特徵。周邊柵欄狀排列 (peripheral palisading) 缺如。偶爾可見鬼影細胞 (ghost cells) 聚集。腫瘤細胞 PAS 陰性。腫瘤間質緻密且常呈現玻璃樣化 (hyalinized)。Merkel cells 可見,並代表腫瘤的一個整合性組成成分。
促結締組織增生性毛上皮瘤中罕見神經周圍浸潤 (perineural infiltration)。
P53 與 bcl-2 不表現,且 MIB-1 增殖指數極低。與硬皮病樣 (morpheaform) 基底細胞癌相反,病灶周圍纖維母細胞 (perilesional fibroblasts) 並無基質金屬蛋白酶 stromelysin-3 (matrix metalloproteinase stromelysin-3) 的表現,且周圍間質含有 CD34+ 細胞。
促結締組織增生性毛上皮瘤偶爾與真皮內母斑 (intradermal nevus)(包括藍色母斑 [blue nevus])並存(圖 31.105 與 31.106)。此為偶然,或如曾有人提出的代表黑色素細胞誘發的上皮增生 (melanocyte-induced epithelial hyperplasia),目前尚不確定。然而,它發生得夠頻繁,足以提示此關聯並非隨機。促結締組織增生性毛上皮瘤亦曾在水痘瘢痕 (varicella scar) 中被描述。
鑑別診斷 (Differential Diagnosis)
促結締組織增生性毛上皮瘤最可能與硬皮病樣基底細胞癌 (morpheaform basal cell carcinoma) 混淆。它的不同之處在於其對稱性,以及缺乏周邊柵欄狀排列、壞死、回縮假象與有絲分裂活性。促結締組織增生性毛上皮瘤鮮少潰瘍。硬皮病樣 (morpheic) 基底細胞癌通常不伴隨角質囊腫形成。藉由免疫組織化學,CK20 陽性的 Merkel cells 可在大多數促結締組織增生性毛上皮瘤中被鑑定,但僅在一小部分基底細胞癌中可見。P75 神經滋養因子受體 (p75 neurotrophin receptor) 與 PHLDA1 在促結締組織增生性毛上皮瘤中表現,但在浸潤型 (infiltrative) 或硬皮病樣基底細胞癌中表現較不頻繁。相對地,纖維母細胞活化蛋白 (fibroblast activation protein) 由浸潤型與硬皮病樣基底細胞癌的腫瘤周圍間質細胞表現,但不由促結締組織增生性毛上皮瘤表現。大多數促結締組織增生性毛上皮瘤病例的雄性素受體 (androgen receptor) 為陰性。與基底細胞癌相似,促結締組織增生性毛上皮瘤對 Ber-EP4 染色呈陽性,且此標記在與基底細胞癌的區分上並無用處。
偶爾,特別是當僅有小型切片可供研究時,促結締組織增生性毛上皮瘤可能被誤認為汗管瘤 (syringoma)、微囊性附屬器癌 (microcystic adnexal carcinoma) 或外分泌腺上皮瘤(外分泌腺汗管樣癌 [eccrine epithelioma (eccrine syringoid carcinoma)])。藉由 diastase–PAS 染色或評估 EMA 與 CEA 免疫組織化學所確定的導管形成 (duct formation) 或胞質內管腔 (intracytoplasmic lumina) 之存在,可排除毛囊分化的腫瘤(圖 31.107)。此外,在微囊性附屬器癌中有絲分裂較常見、CK19 表現較常見,且促結締組織增生性毛上皮瘤中未鑑定出 CD23 表現。
具有釉質瘤樣 (adamantinoid) 特徵。由於其獨特的形態學特徵,將另行討論。
臨床特徵 (Clinical Features)
毛母細胞瘤 (Trichoblastoma) 臨床上表現為一個緩慢生長、單發、界限分明的結節,主要位於頭頸部,好發於頭皮,但其他解剖部位包括軀幹、四肢近端、肛周與生殖器區域亦可受侵犯(圖 31.108)。病灶罕見表現為浸潤性斑塊 (infiltrative plaques),而這些幾乎一律位於臉部,尤其是兩頰,在此處被稱為毛母細胞纖維瘤 (trichoblastic fibroma) 的「斑塊變異型」(plaque-variant)。毛母細胞瘤在初次切片前常已存在多年,且通常生長至大型——直徑 3 cm 或更大;某些病例已達 8–10 cm 寬。任何年齡層(除幼童外)皆可能受影響,但患者最常見於第五至第七十年(fifth to seventh decades)。腫瘤在男性與女性中發生率相等,斑塊樣臉部病灶除外,後者有顯著的女性優勢 9:1.5。它與家族性多發性毛上皮瘤無關聯,但毛母細胞瘤曾在一位 Birt-Hogg-Dubé syndrome 患者以及一位 Curry-Jones syndrome 患者中被描述,後者的特徵為涉及腦部與顱骨異常、多指併指畸形 (polysyndactyly),以及眼、皮膚與胃腸道缺陷的多發性畸形。病灶典型呈膚色,雖然亦曾記錄色素沉著的變異型。它們鮮少與擴張的毛孔 (dilated pore) 相關。毛母細胞瘤以及基底細胞癌的發生,曾被報告為頭皮癬菌感染 (ringworm infection) 放射治療的併發症。
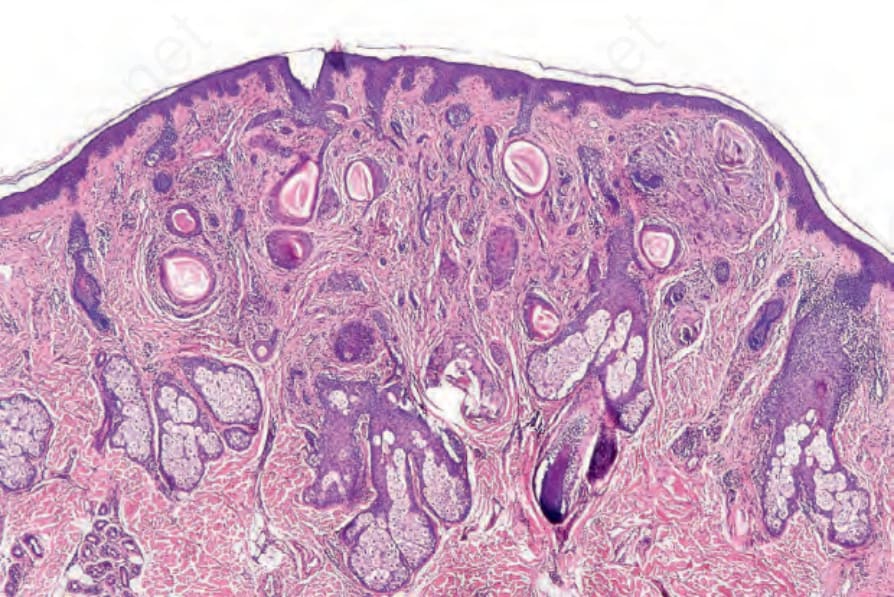
圖 31.100:促結締組織增生性毛上皮瘤 (desmoplastic trichoepithelioma):低倍視野顯示其典型特徵。注意鑲嵌於緻密纖維性間質中的角質囊腫 (keratocysts) 與上皮條索。
Fig. 31.100 Desmoplastic trichoepithelioma: low-power view showing the typical features. Note the keratocysts and epithelial strands embedded in a dense fibrous stroma.
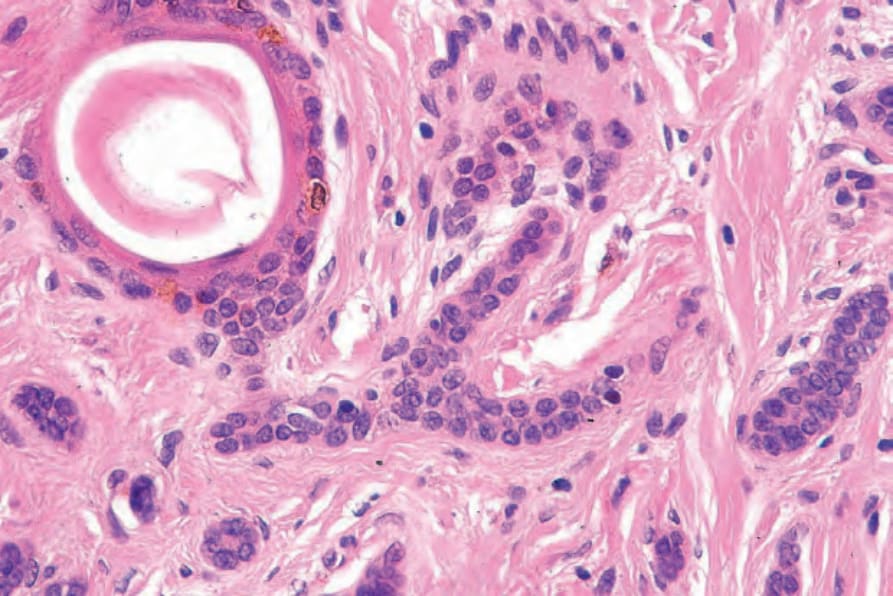
圖 31.102:促結締組織增生性毛上皮瘤 (desmoplastic trichoepithelioma):注意鑲嵌於緻密膠原性間質中的狹窄小型嗜鹼性細胞條索。
Fig. 31.102 Desmoplastic trichoepithelioma: note the narrow strands of small basophilic cells embedded in a dense collagenous stroma.
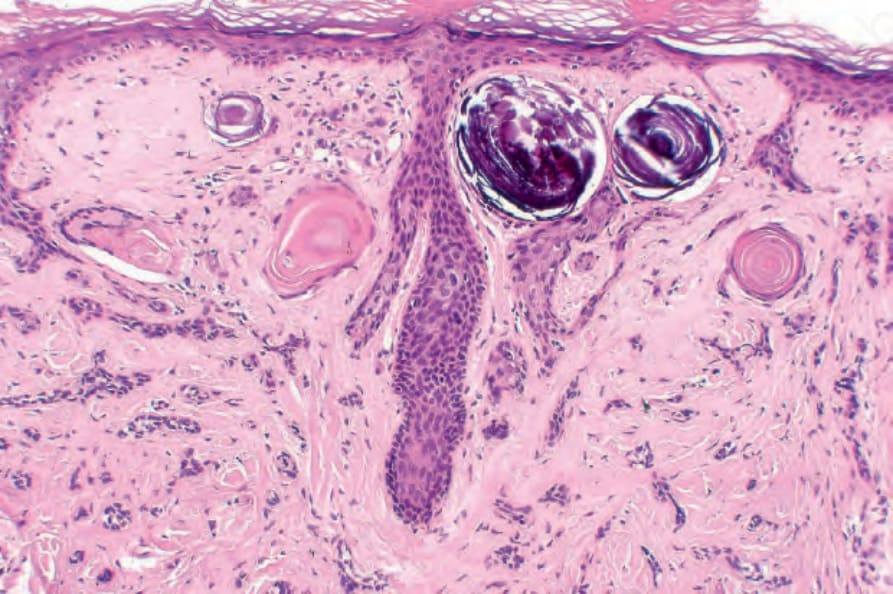
圖 31.104:促結締組織增生性毛上皮瘤 (desmoplastic trichoepithelioma):如此視野所示的局灶性鈣化 (focal calcification) 是非常常見的特徵。
Fig. 31.104 Desmoplastic trichoepithelioma: focal calcification as shown in this field is a very common feature.
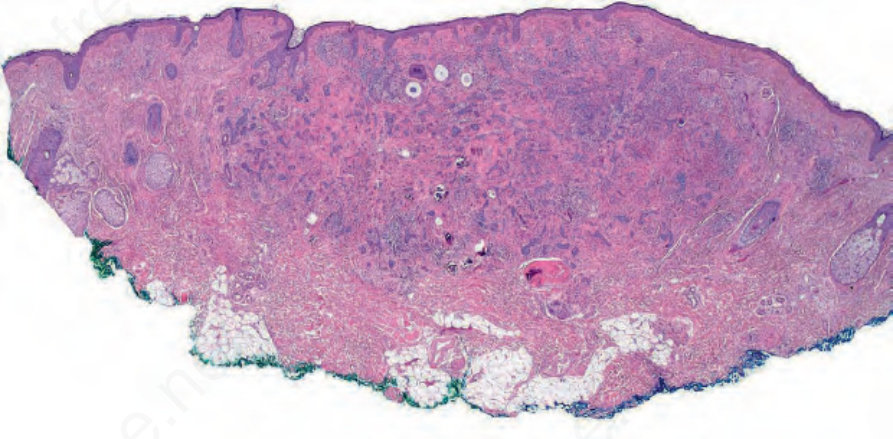
圖 31.105:促結締組織增生性上皮瘤 (desmoplastic epithelioma):此例顯示並存的真皮母斑 (dermal nevus)。
Fig. 31.105 Desmoplastic epithelioma: this example shows a coexistent dermal nevus.
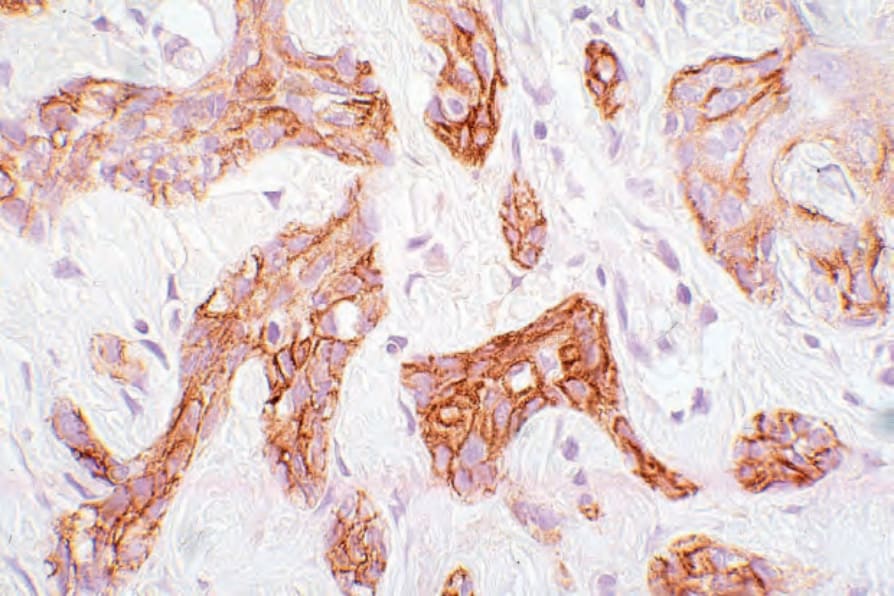
圖 31.107:促結締組織增生性毛上皮瘤 (desmoplastic trichoepithelioma):腫瘤細胞表現 EMA,但無導管分化 (ductal differentiation) 的證據。
Fig. 31.107 Desmoplastic trichoepithelioma: the tumor cells express EMA, but there is no evidence of ductal differentiation.

圖 31.108:毛母細胞瘤 (trichoblastoma):此潰瘍性、息肉狀病灶位於兩臀之間,為其特徵性部位之一。承蒙 E. Wilson Jones, MD, Institute of Dermatology, London, UK 提供。
Fig. 31.108 Trichoblastoma: this ulcerated, polypoid lesion is present between the buttocks, one of the characteristic sites. By courtesy of E. Wilson Jones, MD, Institute of Dermatology, London, UK.
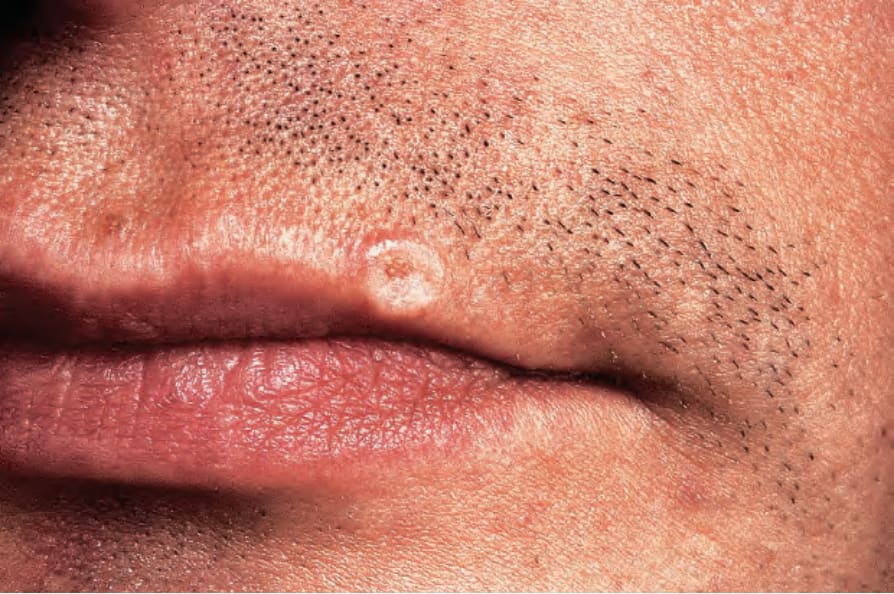
圖 31.98:促結締組織增生性毛上皮瘤 (desmoplastic trichoepithelioma):有一個白色環狀病灶,具有讓人聯想到基底細胞癌的捲起上緣。承蒙 the Institute of Dermatology, London, UK 提供。
Fig. 31.98 Desmoplastic trichoepithelioma: there is a white annular lesion with a rolled upper border reminiscent of basal cell carcinoma. By courtesy of the Institute of Dermatology, London, UK.