Trichoepithelioma
Trichoepithelioma
Clinical features Trichoepithelioma is a hamartomatous condition that shows less follicular differentiation than a trichofolliculoma. The lesion may be multiple and familial or solitary.
Multiple familial trichoepithelioma Multiple familial trichoepithelioma (epithelioma adenoides cysticum [Brooke]) is inherited in an autosomal dominant fashion with diminished expression in males and onset during puberty.1 Patients present with multiple, small, skin-colored papules in a roughly symmetrical distribution located predominantly on the face (Figs 31.89 and 31.90).2 The nasolabial folds, eyebrows, eyelids, and cheeks are most commonly involved.2,3 Other sites including the scalp, neck, extremities, buttocks, and genital area may also be affected.2,4–9 The lesions are usually asymptomatic and commence as translucent skin-colored papules, which sometimes show slight surface telangiectasia. They slowly enlarge to reach a maximum diameter of about 0.5 cm. Rarely, ulceration occurs, usually at a very late stage. Lesions are occasionally pigmented. A linear and dermatomal distribution has also been reported.5
Patients with epithelioma adenoides cysticum rarely develop any significant systemic manifestations. An association with renal and pulmonary cysts and with malignant lymphoepithelial lesion of the parotid gland has,
1571 Trichoepithelioma
large size and confluence (turban tumor), the multiple trichoepitheliomas are largely located centrofacially.2 Tumors frequently show hybrid features such as spiradenocylindromas, and sebaceous differentiation may be a feature.55 Patients also develop other hair follicle tumors such as trichoblastoma and cutaneous lymphadenoma.55 Additional syringomas are rare and may be an incidental association.56 Parotid gland tumors such as membranous-type basal cell adenoma, a histologic mimic of cylindroma, may rarely develop as well as cylindroma of the breast parenchyma.57–64 Both the salivary gland tumor as well as the cylindromas infrequently undergo malignant change.31,58,65–67 Malignant transformation in trichoepithelioma (high-grade trichoblastic carcinoma) and development of a carcinosarcoma have also been documented in patients with Brooke-Spiegler syndrome and multiple familial trichoepithelioma.68–70
however, been documented.10,11 Very rarely, a coexistent basal cell carcinoma may be found.12–16
Although initial genetic linkage analysis mapped the disease to a region on chromosome 9p21, subsequent studies have failed to confirm this observation. Instead, mutations in the CYLD gene on chromosome 16q12-q13 have been consistently identified in multiple families, analogous to Brooke-Spiegler syndrome.17–28 These data emphasize that multiple familial trichoepithelioma may indeed represent part of a disease spectrum that also includes familial cylindromatosis and Brooke-Spiegler syndrome.
Rombo syndrome Rombo syndrome comprises multiple trichoepitheliomas, milia, vermiculate atrophy, basal cell carcinoma, vellus hair cysts, peripheral vasodilatation, and cyanosis.71 It is an exceedingly rare condition, with a possible autosomal dominant mode of inheritance.72 Skin lesions present in childhood and basal cell carcinomas develop in early adulthood.72
A further familial form has been associated with nail dystrophy, alopecia, and myasthenia gravis.73–76
Solitary trichoepithelioma Solitary trichoepithelioma usually presents as a 0.5-cm-diameter, asymptomatic, flesh-colored nodule on the face of an adult. It is occasionally seen at other sites, including the scalp, neck, back, vulva, mons pubis, and proximal extremities.2,77,78
Brooke-Spiegler syndrome The autosomal dominant Brooke-Spiegler syndrome (familial cylindromatosis or turban tumor syndrome) is characterized by multiple cylindromas in addition to spiradenomas, multiple trichoepitheliomas, and milia.29–54 While penetrance is high, there is great variability in presentation among patients. Within the same family some patients may present with either multiple cylindromas or trichoepitheliomas only, or a combination of both. Patients present with skin lesions in early adulthood, and there is a female predilection. While cylindromas typically present on the scalp and may grow to
Trichoepithelioma is occasionally associated with melanocytic (banal or blue) and epidermal nevi.79–82
Pathogenesis and histologic features The Brooke-Spiegler syndrome has recently been mapped to chromosome locus 16q12-13, and the candidate gene identified as the tumor suppressor gene CYLD.47–52 Mutations resulting in inactivation of the CYLD gene have been reported, with tumors showing loss of heterozygosity for the wild-type copy, a characteristic finding for tumor suppressor genes.32,33,35,47 CYLD mutations have now also been identified in families with multiple familial trichoepithelioma and familial cylindromatosis, suggesting phenotypic variation of the same underlying disease.18,19,21–28,30,83 However, no genotype– phenotype correlation has emerged thus far.
More recently, insights into the molecular function of CYLD have been gained. CYLD is a deubiquinating protein that interferes with the
1572 Tumors of the hair follicle
tumor necrosis factor alpha (TNF-α)/NF-κb pathway by targeting multiple important signaling molecules such as TRAF2 (tumor necrosis factor receptor-associated factor 2), NEMO as well as bcl-3, among others. CYLD is therefore involved in the regulation of various important functions including inflammation, cell survival, proliferation, and tumorigenesis.84–86 Lack of CYLD results in constitutive NF-κb pathway activation as well as decreased apoptosis.87–91 The precise mechanism detailing how NF-κb pathway activation is involved in tumorigenesis is, however, not fully understood.
Keratin expression profiles in trichoepithelioma demonstrate differentiation toward the outer root sheath.92 In contrast to data on multiple familial trichoepithelioma and the Brooke-Spiegler syndrome, the Shh signaling pathway appears to be involved in the pathogenesis of solitary trichoepithelioma. Analogous to basal cell carcinoma, somatic mutations and loss of heterozygosity of the patched gene (PTCH) have been detected in a subset of trichoepitheliomas.93,94 Transgenic mice overexpressing GLI-1, a protein involved in the Shh signaling pathway, develop basal cell carcinoma as well as adnexal tumors reminiscent of trichoepithelioma and cylindroma, and high GLI-1 transcript levels have been detected in both basal cell carcinomas as well as trichoepitheliomas.95,96
The tumor sometimes shows continuity with the epidermis, which may appear normal or slightly hyperkeratotic and thinned with loss of the rete ridge pattern. Ulceration, however, is exceedingly rare. Typical trichoepithelioma is characterized by numerous horn cysts free within the dermis and within lobules of basaloid cells (Figs 31.91 and 31.92).2 Admixed with the horn cysts are lobules of tumor cells indistinguishable from those of basal cell carcinoma, being basophilic with minimal cytoplasm and showing peripheral palisading (Fig. 31.93). In trichoepithelioma, however, the perilobular connective tissue sheath is more conspicuous and is frequently associated with the formation of juxtaepithelial round or oval fibroblastic aggregates – papillary mesenchymal bodies (Fig. 31.94).97 These are believed to represent primitive papillary mesenchyme. Sometimes they indent the lobules to produce a hair bulblike appearance. The lobules of basaloid cells are frequently associated with thin epithelioid strands resulting in a frondlike appearance (Fig. 31.95). Trichoepitheliomas not uncommonly show a foreign body giant cell reaction to free keratin, and occasionally foci of calcification are evident. Amyloid deposits are uncommon.98–100
Some trichoepitheliomas, however, may show little keratin cyst formation.2 Instead, the tumor is composed of a rather circumscribed lesion in which discrete lobules of basaloid cells are widely dispersed throughout an abundant connective tissue stroma (Figs 31.96 and 31.97). Tumors with this particular pattern are likely to have arisen at extrafacial sites. Rarely, epithelial giant cells and multinucleated forms have been observed in tumor lobules.101
1573 Trichoepithelioma
BCC TB TE
bcl-2 (epithelium) + (diffuse) ± (peripheral) ± (70%; peripheral)
CD10 (epithelium) + (86%) ± ± (15%)
CD10 (stroma) – + + (92%)
CD34 (stroma) ± ± +
- (78%) – –
Androgen receptor (epithelium)
– + (70%) n/a
Intratumoral CK20- positive Merkel cells
A
Differential diagnosis Sometimes the histologic appearances of trichoepithelioma are difficult to distinguish from those of keratotic basal cell carcinoma. The presence of ulceration and/or a marked tumor–stroma retraction artifact with mucin deposits argue in favor of the latter, whereas marked epithelial frond formation, and more particularly, papillary mesenchymal body with hair bulb formation, are indicative of the former.98 Mitotic figures and apoptotic cells may be present in both conditions.98 Immunohistochemistry may play a useful role in the differential diagnosis although the cytokeratin (CK) expression pattern is largely similar.97,102 Only CK15, which is expressed in most trichoepitheliomas but not in basal cell carcinoma, appears to be of some value.103,104 Expression of bcl-2 is consistently found to be diffuse in basal cell carcinoma while it is predominantly peripheral in trichoepithelioma.102,105 PHLDA1 is expressed in the majority of trichoepitheliomas while it is frequently lost in basal cell carcinoma.106 The MIB-1 proliferative index and p53 nuclear staining are increased in basal cell carcinoma compared to trichoepithelioma, and androgen receptor expression is observed in the majority of basal cell carcinomas while it is absent in trichoepitheliomas.107,108 In addition, the stroma surrounding trichoepithelioma contains CD34+ cells, whereas these are largely absent in basal cell carcinoma.109 CD10 staining in trichoepithelioma is predominantly located in the stromal rather than the epithelial component while the opposite is true for basal cell carcinoma (Table 31.1).110 However, none of the above-mentioned immunohistochemical stains can be used with complete confidence in the differential diagnosis and should not be relied on.111 A clinical history of numerous small facial papules is highly suggestive of epithelioma adenoides cysticum. If the lesion is solitary and the diagnosis is in doubt, it is probably in the patient’s safest interest to treat it as a keratotic basal cell carcinoma.

Fig. 31.101 Desmoplastic trichoepithelioma: in this example, a follicular origin is evident.
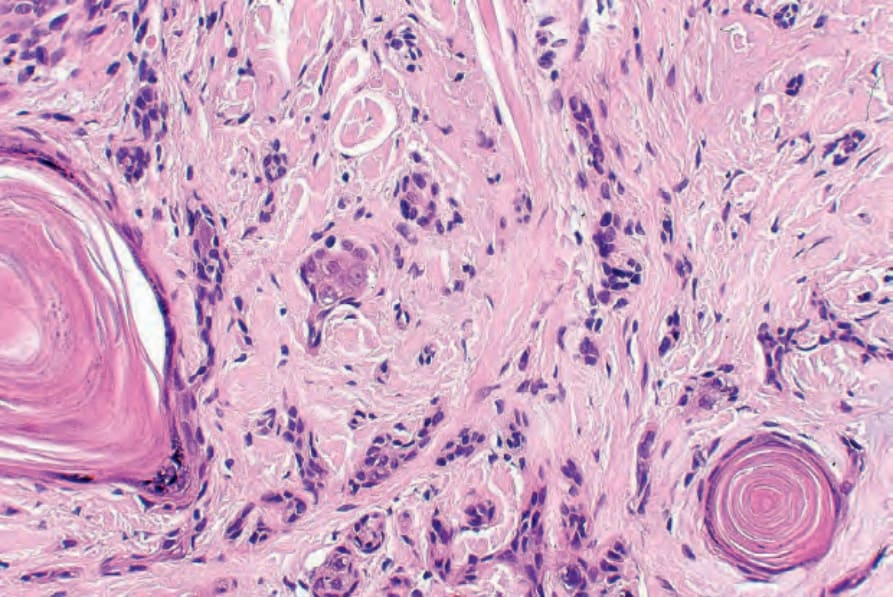
Fig. 31.103 Desmoplastic trichoepithelioma: the cysts show epidermoid keratinization.
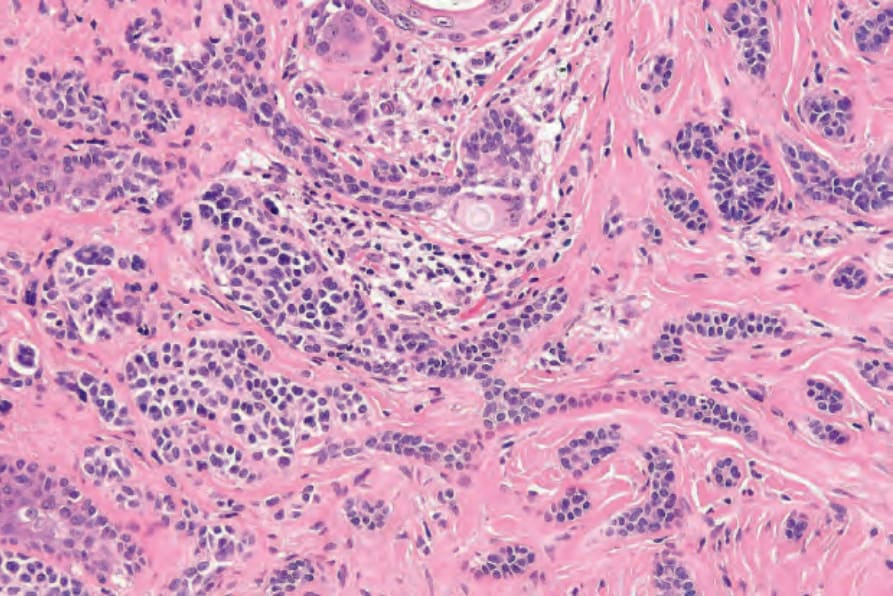
Fig. 31.106 Desmoplastic trichoepithelioma: high-power view.

Fig. 31.87 Median nasal dermoid fistula: the presence of protruding white hairs is characteristic. By courtesy of D. Shuttleworth, MD, University of Wales, Cardiff, UK.
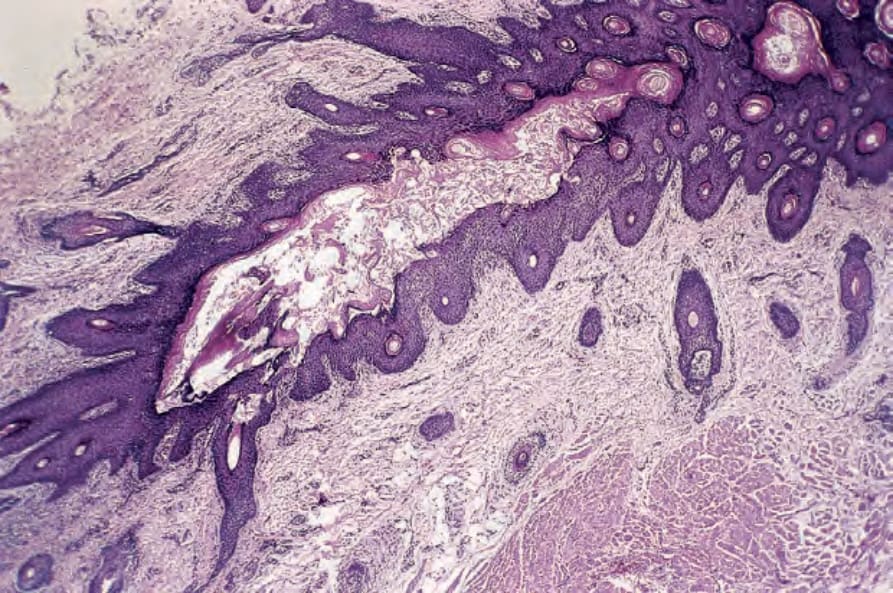
Fig. 31.88 Median nasal dermoid fistula: the fistula, which communicates with the surface epidermis, is lined by hair-bearing epithelium. By courtesy of D. Shuttleworth, MD, University of Wales, Cardiff, UK.
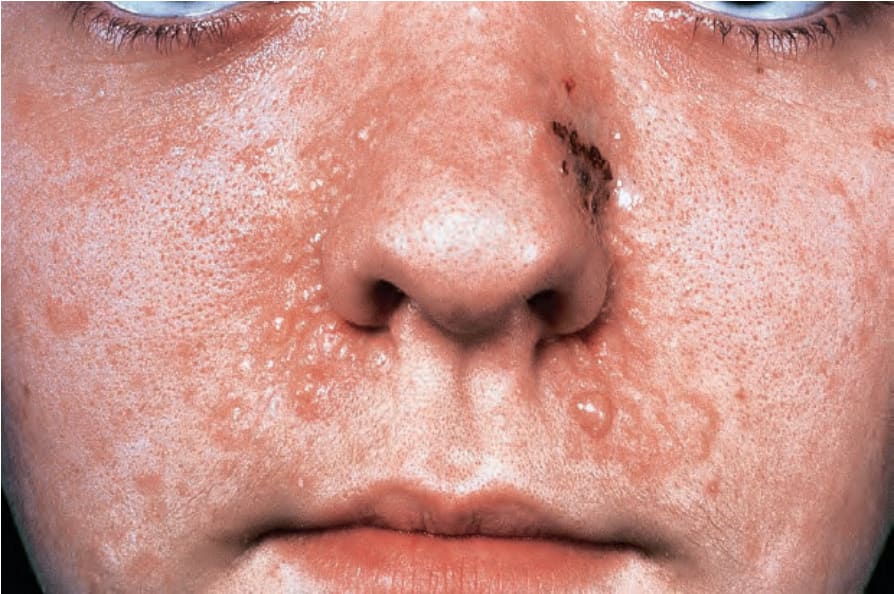
Fig. 31.89 Trichoepithelioma: this patient has familial multiple trichoepitheliomas. Note the presence of multiple skin-colored papules about the nasolabial folds. By courtesy of the Institute of Dermatology, London, UK.

Fig. 31.90 Trichoepitheliomas: note the numerous skin-colored papules and nodules on this girl’s scalp and forehead. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
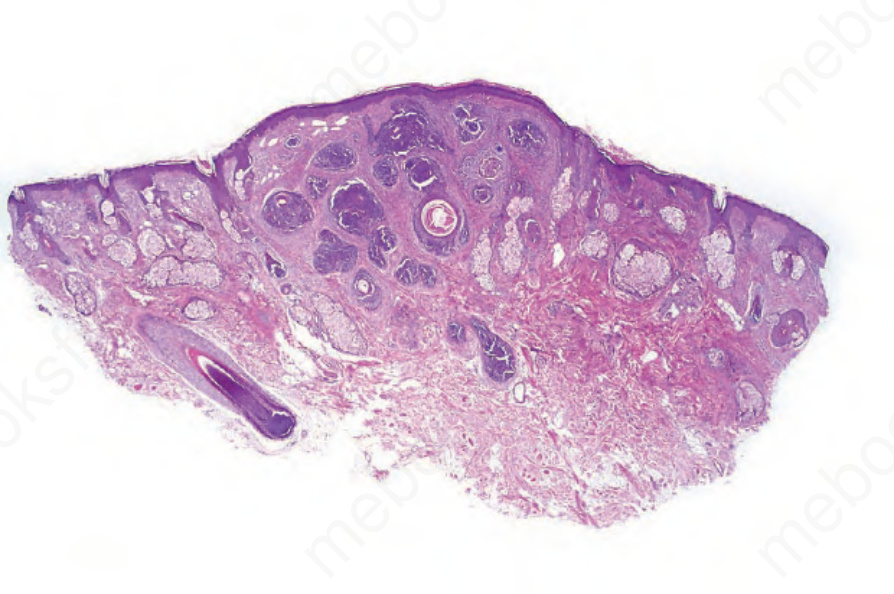
Fig. 31.91 Trichoepithelioma: this scanning view shows the typical appearances of lobules of basaloid cells and keratocysts.
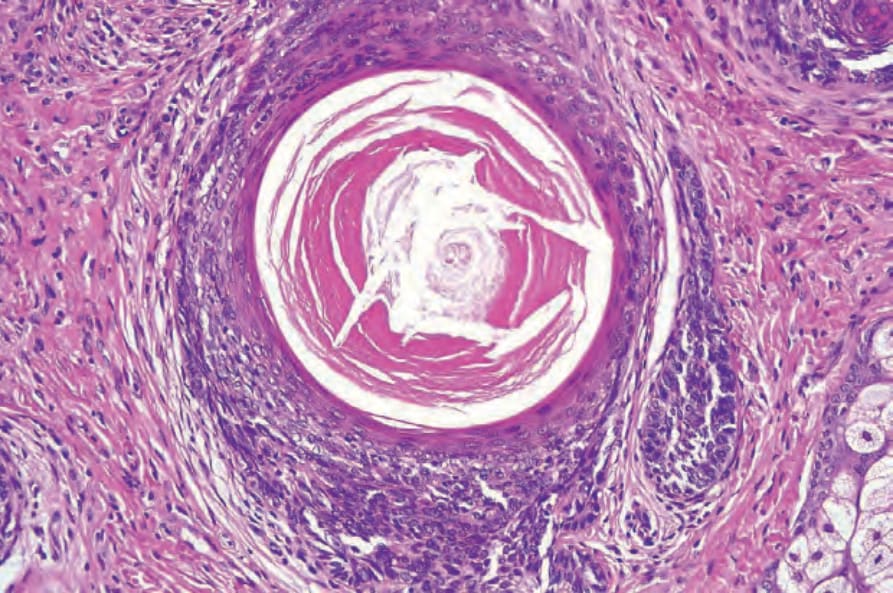
Fig. 31.92 Trichoepithelioma: the keratocysts show infundibular keratinization.
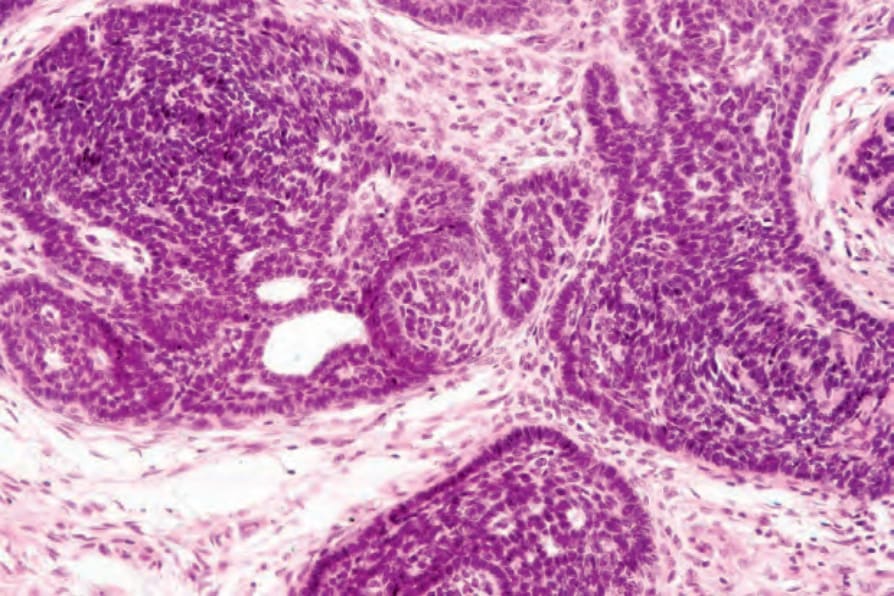
Fig. 31.93 Trichoepithelioma: in this area, the tumor lobules show conspicuous peripheral palisading and are enveloped in a dense connective tissue sheath. A papillary mesenchymal body is evident in the center of the field.
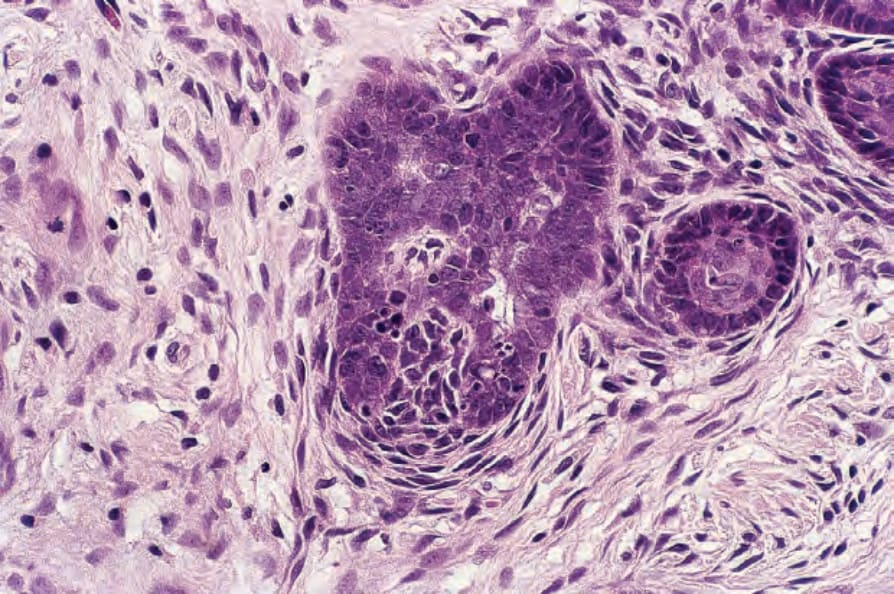
Fig. 31.94 Trichoepithelioma: high-power view of a papillary mesenchymal body.
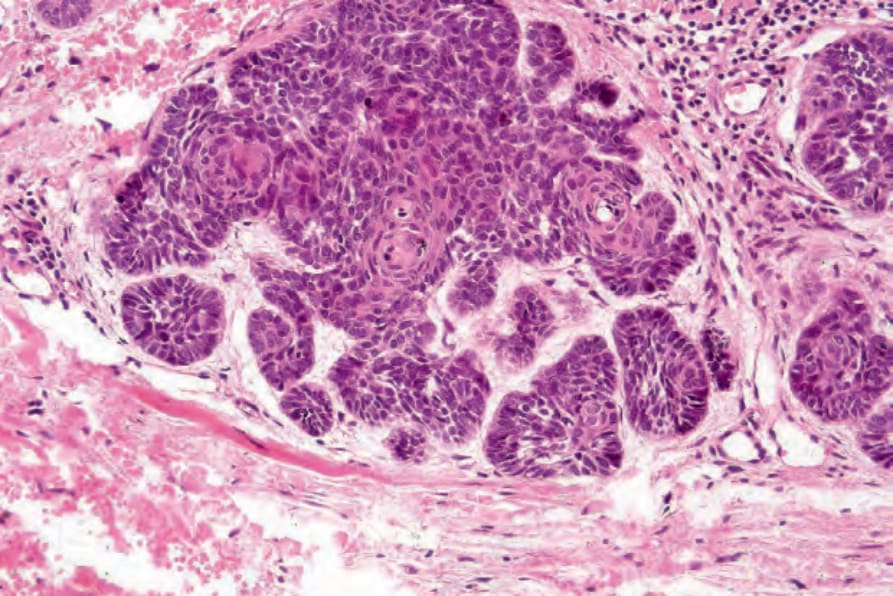
Fig. 31.95 Trichoepithelioma: in this view, the tumor has a delicate frondlike pattern.
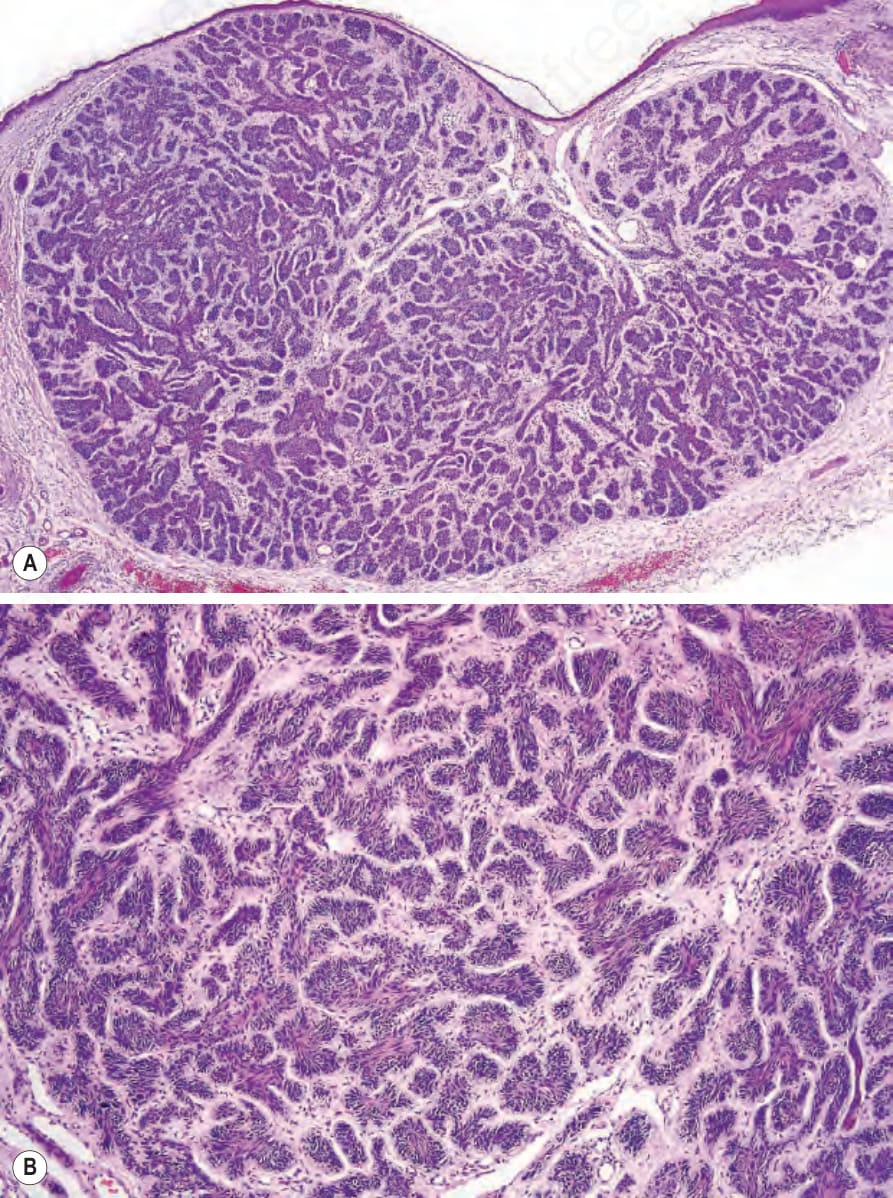
Fig. 31.96 (A, B) Trichoepithelioma: in this example, the tumor is composed of small basophilic lobules surrounded by a dense fibrous stroma. Keratocysts are not present.
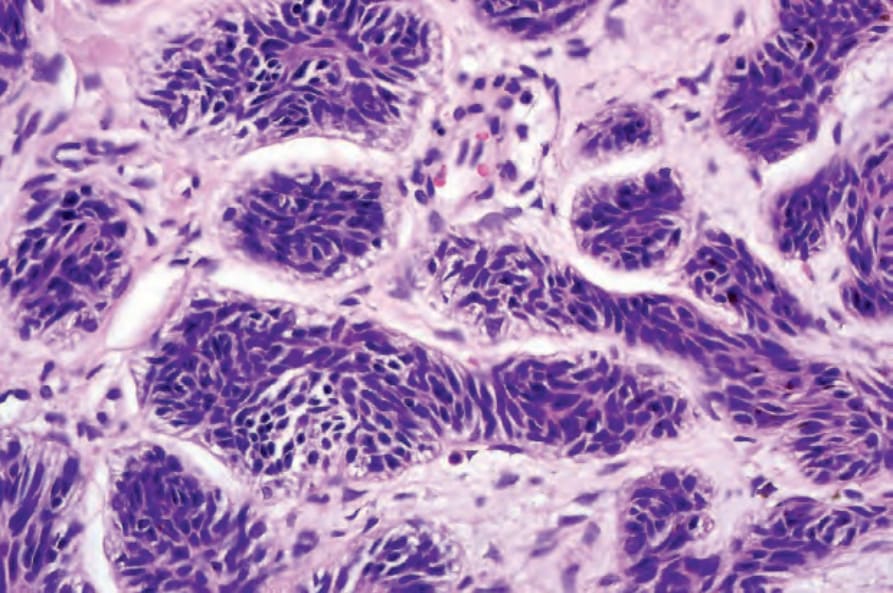
Fig. 31.97 Trichoepithelioma: the tumor is composed of small cells with uniform darkly staining nuclei.

Fig. 31.99 Desmoplastic trichoepithelioma: this example on the nose presented as a depressed area of scarring. By courtesy of the Institute of Dermatology, London, UK.
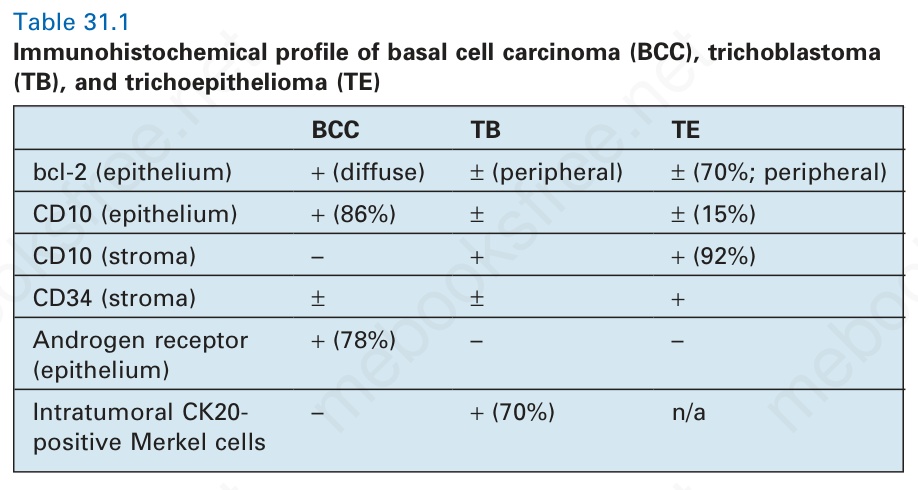
Table 31.1 Immunohistochemical profile of basal cell carcinoma (BCC), trichoblastoma (TB), and trichoepithelioma (TE)
B
1574 Tumors of the hair follicle
Trichoepithelioma shows considerable histologic overlap with trichoblastoma, and indeed some authors might classify it as such.
Desmoplastic trichoepithelioma (sclerosing epithelial hamartoma)
Desmoplastic trichoepithelioma was originally thought to represent a syringoid variant of trichoepithelioma. It was subsequently described simultaneously as desmoplastic trichoepithelioma and sclerosing epithelial hamartoma.
are also present. Desmoplastic trichoepithelioma is not seen in patients with the multiple trichoepithelioma syndromes, and familial occurrence is exceptional.18,19
Histologic features Desmoplastic trichoepithelioma is quite different from conventional trichoepithelioma. It consists of a triad of narrow epithelial strands, keratinous cysts, and a desmoplastic stroma (Figs 31.100 and 31.101).1,3,4
The epidermis may be normal, atrophic, or mildly acanthotic. Marked pseudoepitheliomatous hyperplasia is a rare finding.20,21 Occasionally, a central depression is evident. Situated within the upper and mid-dermis is a variable admixture of linear and branched epithelial strands and keratinizing cysts embedded in a dense fibrous and often collagenous stroma (Figs 31.102 and 31.103). The cysts consist of a peripheral border of small cuboidal basal cells with prominent nuclei and scanty cytoplasm. These mature to form squamous epithelium, which in turn undergoes epidermoid keratinization. Epithelial strands sometimes bud from the cyst walls.1 A foreign body giant cell reaction due to released keratin is very common. Calcification is also frequently seen, and occasionally bone formation occurs (Fig. 31.104).22
Clinical features Desmoplastic trichoepithelioma is an asymptomatic, slowly growing lesion that usually presents on the face or neck of young adults, with favored sites being the cheek, chin, and forehead (Figs 31.98 and 31.99).1–13 Congenital presentation is rare.14 Lesions are usually solitary, although patients with multiple tumors have occasionally been documented.15,16 It shows a predilection for females (4:1).2,13 The tumor is 3–8 mm in diameter, hard and annular, white or yellow, with a depressed or atrophic center and an elevated border.2,17 Typically, the lesion does not ulcerate. Occasionally, milia
The epithelial strands (which sometimes unite with the epidermis) are composed of small cuboidal basaloid cells in a layer 1–3 cells thick. Mitotic activity is very rare and pleomorphism is never a feature. Peripheral
1575 Desmoplastic trichoepithelioma (sclerosing epithelial hamartoma)
palisading is absent. Occasionally, aggregates of ghost cells are evident.23 The tumor cells are PAS-negative. The tumor stroma is dense and often appears hyalinized. Merkel cells are seen and represent an integral component of the tumor.24,25
Perineural infiltration is rarely seen in desmoplastic trichoepithelioma.26
P53 and bcl-2 are not expressed, and the MIB-1 proliferation index is extremely low.27 In contrast to morpheaform basal cell carcinoma, there is no expression of the matrix metalloproteinase stromelysin-3 in perilesional fibroblasts and the surrounding stroma contains CD34+ cells.28–30
Occasionally, desmoplastic trichoepithelioma coexists with an intradermal nevus including blue nevus (Figs 31.105 and 31.106).22,31–35 Whether this is fortuitous or represents melanocyte-induced epithelial hyperplasia, as has been suggested, is uncertain.32,36 It does, however, occur sufficiently frequently to suggest that the association is not random. Desmoplastic trichoepithelioma has also been described in a varicella scar.37
Differential diagnosis Desmoplastic trichoepithelioma is most likely to be confused with morpheaform basal cell carcinoma.3,4,23 It differs by its symmetry, and absence of peripheral palisading, necrosis, retraction artifact, and mitotic activity. Desmoplastic trichoepithelioma rarely ulcerates. Morpheic basal cell carcinoma is not usually associated with horn cyst formation. By immunohistochemistry, CK20-positive Merkel cells are identified in most desmoplastic trichoepitheliomas but only in a small subset of basal cell carcinomas.38 P75 neurotrophin receptor and PHLDA1 are expressed in desmoplastic trichoepithelioma but less frequently in infiltrative or morpheic basal cell carcinoma.39–42 In contrast, fibroblast activation protein is expressed by
1576 Tumors of the hair follicle
the peritumoral stromal cells of infiltrative and morpheic basal cell carcinoma but not desmoplastic trichoepithelioma.43 Most cases of desmoplastic trichoepithelioma are negative for androgen receptor.38,44 Similar to basal cell carcinoma, desmoplastic trichoepithelioma stains positively for Ber-EP4 and this marker is not useful in the distinction from basal cell carcinoma.45
Occasionally, particularly when only small biopsies are available for study, desmoplastic trichoepithelioma may be mistaken for syringoma, microcystic adnexal carcinoma, or eccrine epithelioma (eccrine syringoid carcinoma). The presence of duct formation or intracytoplasmic lumina, as determined with the use of diastase–PAS staining or by assessing EMA and CEA immunohistochemistry, excludes a tumor of follicular differentiation (Fig. 31.107).46,47 Furthermore, mitoses are more common and CK19 expression is more common in microcystic adnexal carcinoma, and CD23 expression is not identified in desmoplastic trichoepithelioma.48,49
adamantinoid features. Due to its distinctive morphological features, it is discussed separately.
Clinical features Trichoblastoma presents clinically as a slowly growing, solitary, well-circumscribed nodule located predominantly in the head and neck area with predilection for the scalp, but other anatomic sites including trunk, proximal extremities, perianal, and genital region may also be affected (Fig. 31.108).1,4–38 Lesions rarely present as infiltrative plaques and these are almost invariably located on the face, especially the cheeks, where they have been referred to as ‘plaque-variant’ of trichoblastic fibroma.5,6 Trichoblastomas are frequently present for multiple years before initial biopsy, and they usually grow to a large size – 3 cm or more in diameter; some examples have reached 8–10 cm across.7–10 Any age group (except young children) may be affected, but most commonly patients are in their fifth to seventh decades.1,4–38 The tumor occurs equally in men and women except for the plaquelike facial lesion where there is a striking female predominance of 9:1.5. There is no relationship with familial multiple trichoepitheliomas, but trichoblastoma has been described in a patient with Birt-Hogg-Dubé syndrome and in one patient with Curry-Jones syndrome, characterized by multiple malformations involving brain and skull abnormalities, polysyndactyly, as well as defects of eyes, skin, and gastrointestinal tract.39,40 Lesions are typically skin colored, although a pigmented variant has also been documented.11,12 They are rarely related to a dilated pore.41 Development of trichoblastoma as well as basal cell carcinoma has been reported as a complication of radiation treatment for ringworm infection of the scalp.42
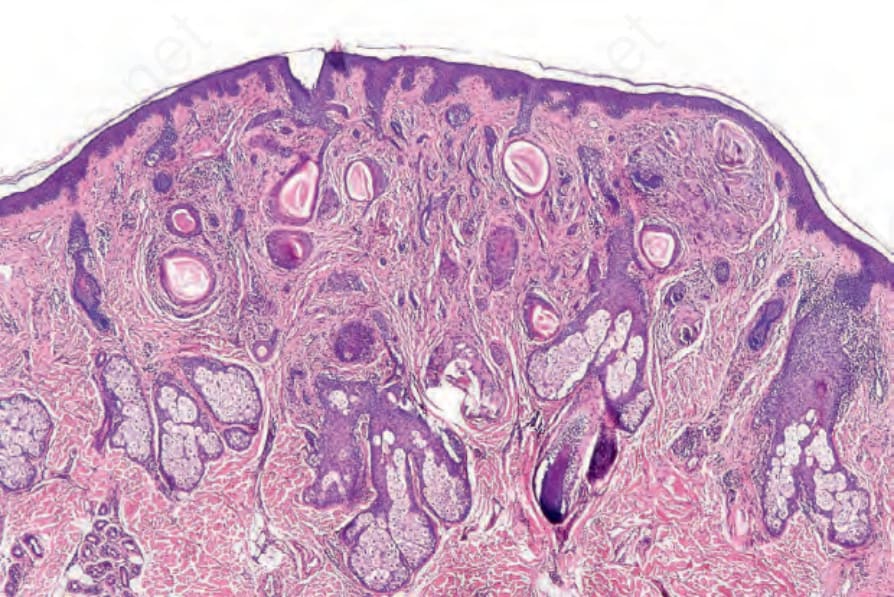
Fig. 31.100 Desmoplastic trichoepithelioma: low-power view showing the typical features. Note the keratocysts and epithelial strands embedded in a dense fibrous stroma.
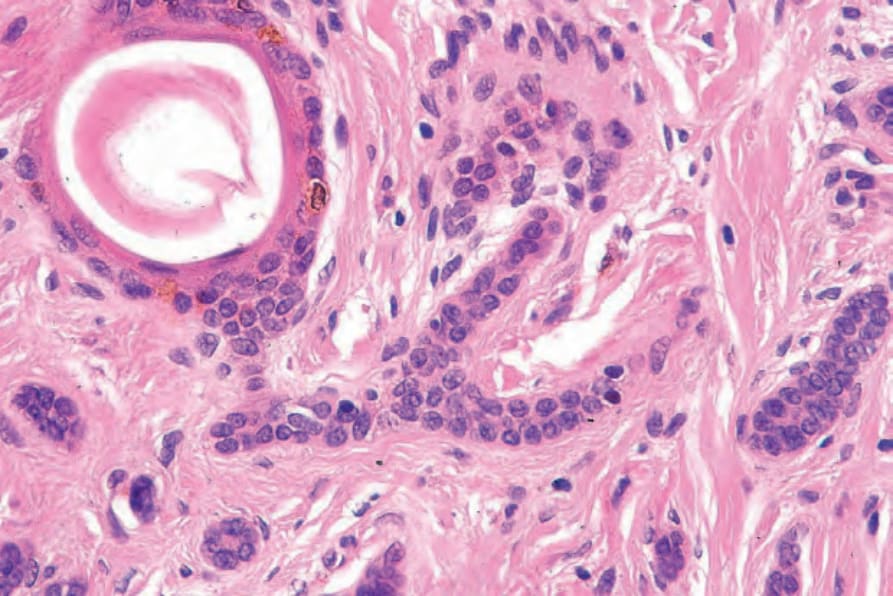
Fig. 31.102 Desmoplastic trichoepithelioma: note the narrow strands of small basophilic cells embedded in a dense collagenous stroma.
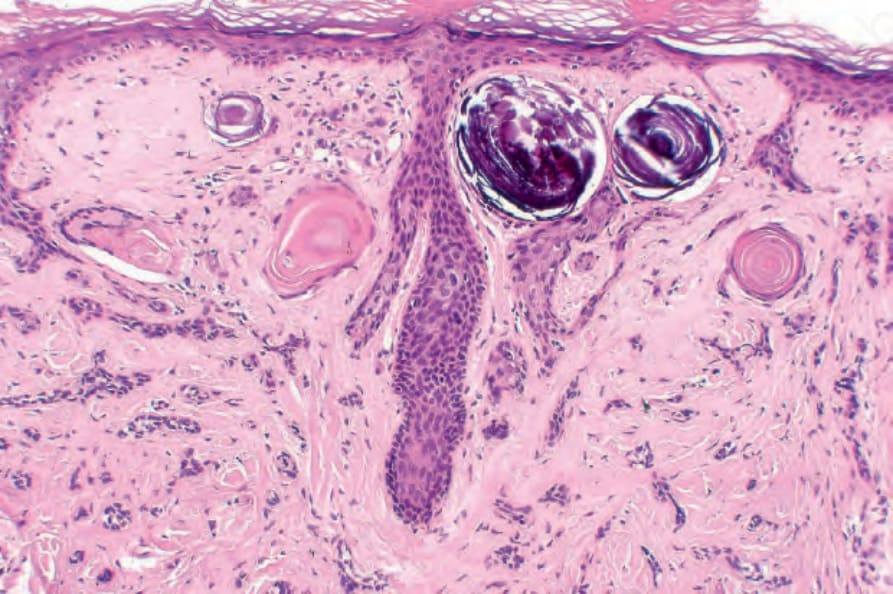
Fig. 31.104 Desmoplastic trichoepithelioma: focal calcification as shown in this field is a very common feature.
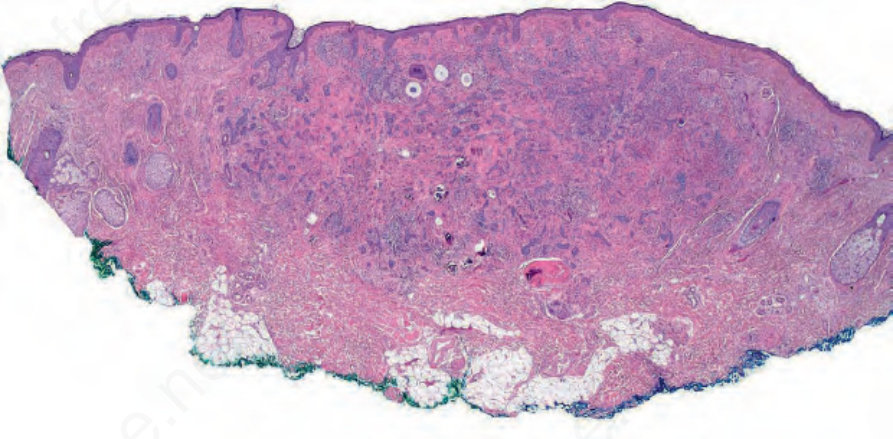
Fig. 31.105 Desmoplastic epithelioma: this example shows a coexistent dermal nevus.
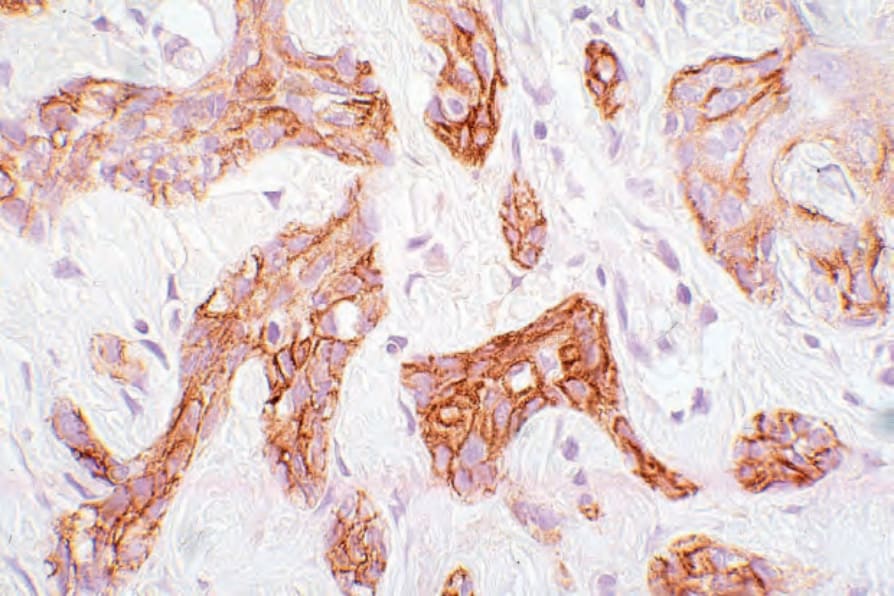
Fig. 31.107 Desmoplastic trichoepithelioma: the tumor cells express EMA, but there is no evidence of ductal differentiation.

Fig. 31.108 Trichoblastoma: this ulcerated, polypoid lesion is present between the buttocks, one of the characteristic sites. By courtesy of E. Wilson Jones, MD, Institute of Dermatology, London, UK.
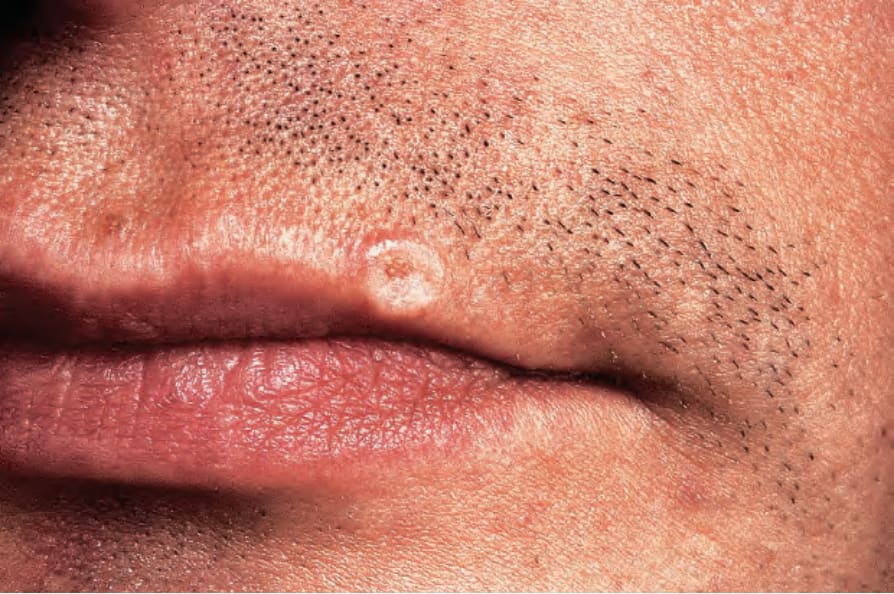
Fig. 31.98 Desmoplastic trichoepithelioma: there is a white annular lesion with a rolled upper border reminiscent of basal cell carcinoma. By courtesy of the Institute of Dermatology, London, UK.