腺癌 (Adenocarcinoma)
(食道癌不到 2% 會播散至皮膚)、口腔、喉與子宮頸。它較少見地可源自身體被覆部位他處、肛門、外陰、陰莖、陰道與扁桃腺的鱗狀細胞癌 (squamous carcinoma)。分化差的轉移病灶常造成困擾,可能需仔細檢視多張切片,才能偵測到鱗狀分化的病灶(角化 [keratinization] 或細胞間橋 [intercellular bridges])。一個重點是,在缺乏角化的情況下,無法區分轉移性分化差的鱗狀細胞癌與移行細胞腫瘤 (transitional cell tumors)。此外,鱗狀細胞癌的原發部位一般無法藉由形態學或免疫組化標記來鑑別。
腺癌沉積 (adenocarcinomatous deposits) 是目前為止最常見的皮膚轉移,乳房 (breast) 為最常見來源(可達皮膚轉移的 23%,其中絕大多數發生於女性)。肺 (lung) 與大腸 (large intestine) 也是轉移性腺癌的重要來源。其他原發部位包括胃、攝護腺、胰臟、子宮內膜、甲狀腺、卵巢與子宮頸內膜 (endocervix)。針對譜系限制性轉錄因子 (lineage restricted transcription factors) 的抗體已可用於許多癌症類型,後文將進一步討論。
源自乳房癌的轉移有多種外觀,某種程度上取決於原發腫瘤的性質 (Figs 30.27–30.31)。結節性沉積與鎧甲狀癌 (carcinoma en cuirasse) 由未分化細胞的瀰漫性浸潤組成,這些細胞具有深染的細胞核與極少的細胞質。轉移性乳房癌至眼瞼有一定的發生頻率,且在該部位腫瘤細胞有時呈現明顯的類組織球樣 (histiocytoid) 外觀。罕見情況下,乳房、攝護腺與大腸的轉移性腺癌可表現出親表皮性 (epidermotropism),可能與原發性皮膚癌或表淺擴散型黑色素瘤 (superficial spreading melanoma) 混淆。極例外地,轉移性乳房癌會模擬顆粒細胞瘤 (granular cell tumor),或含有類似黑色素瘤的黑色素 (melanin pigment)。
通常轉移腫瘤不與其上方的表皮相連。然而極例外地,轉移性鱗狀細胞癌可表現為親表皮性 (epidermotropic) 與/或親毛囊性 (folliculotropic) 的轉移,使其與原發腫瘤的區別變得非常困難。此現象曾被描述於轉移性喉癌、源自唇部的癌,以及源自原發性皮膚鱗狀細胞癌的轉移。高分子量角蛋白 (high molecular weight keratins) 如 CK 5/6 亦可用於鱗狀細胞癌的診斷,尤其是分化差的腫瘤,但這無法區分原發與轉移腫瘤。在缺乏特徵性形態特徵時,p63 與 p40 亦可作為提示鱗狀來源的標記。
CK14 的使用已被提倡為有助於區分鱗狀細胞癌與腺癌。鱗狀細胞
乳房轉移(尤其是小葉型 [lobular type])的典型特徵,是腫瘤細胞於相鄰膠原束之間呈線狀剝離 (linear dissection)(疊銅板 [stacked-penny] 或「單列排列」[single-file] 外觀)(Fig. 30.32)。類似外觀亦可見於若干其他腫瘤,包括攝護腺、胃與胰臟者,以及小細胞癌 (small cell carcinoma)。淋巴瘤、硬化性類上皮纖維肉瘤 (sclerosing epithelioid fibrosarcoma) 與原發性皮膚神經內分泌腫瘤 (primary cutaneous neuroendocrine tumor) 偶爾也可採取相同的型態。可能有明顯的腺體分化,但此型態占主導者並不常見 (Fig. 30.33)。發炎性癌 (inflammatory carcinoma) 的特徵是表皮下與更深層淋巴管道的廣泛浸潤,而在毛細血管擴張型 (telangiectatic variant) 中,血管侵犯亦可能明顯 (Figs 30.34
1531 個別腫瘤
A
B
1532 皮膚轉移與皮膚 Paget 病
與 30.35)。具有局灶性壞死的分化良好腺體結構,較典型地代表大腸或直腸的原發腫瘤 (Figs 30.36–30.39)。在退行發育 (anaplastic) 變異型中,腫瘤細胞的特徵可能與高惡性度淋巴瘤無法區分。免疫組化技術常為建立正確診斷所必需。某些 CD30 陽性的退行發育大細胞淋巴瘤 (anaplastic large cell lymphomas) 不表現白血球共同抗原 (leukocyte common antigen, CD45)。在排除播散性淋巴瘤的診斷之前,務必納入一系列針對 B 細胞與 T 細胞抗原的抗體。亦須記住,淋巴結的 CD30 陽性退行發育大細胞淋巴瘤並不少見地表現上皮膜抗原 (epithelial membrane antigen, EMA),這對不謹慎者可能是一個診斷陷阱。
具有乳頭狀生長型態 (papillary growth pattern) 的轉移腫瘤可能反映若干不同部位,包括大腸、卵巢、甲狀腺、胃,甚至是肺 (Figs 30.40 and 30.41)。某些鑑別特徵有時能讓各種乳頭狀轉移之間得以區分。同心層狀鈣化的砂粒體 (psammomatous bodies) 在漿液性(卵巢)癌與甲狀腺乳頭狀癌中均可能明顯。然而後者可進一步藉由膠質生成 (colloid production)、核溝 (nuclear grooving) 與特徵性的「孤兒安妮眼」核 (‘Orphan Annie’ nuclei) 來辨識。核內細胞質假包涵體 (intranuclear cytoplasmic pseudoinclusions) 有時也是一項特徵。免疫組化呈現甲狀腺球蛋白 (thyroglobulin) 生成可作為確認。具有明顯透明細胞變化的甲狀腺乳頭狀癌之皮膚轉移
可能模擬原發性附屬器腫瘤,如透明細胞汗腺癌 (clear cell hidradenocarcinoma)。一部分轉移性甲狀腺乳頭狀癌的病例顯示 BRAF (V600E) 突變,可藉由使用 VE1 抗體的免疫組化或其他分子方法偵測,此特徵在甲狀腺的濾泡癌 (follicular carcinoma) 與 hidradenocarcinoma 中不存在,使困難病例得以區分。
或許其中一項最具挑戰性的鑑別診斷,在於轉移性腺癌與顯示發育良好導管分化 (ductal differentiation) 的原發性皮膚附屬器癌 (primary cutaneous adnexal carcinoma) 之間。汗腺癌 (eccrine carcinomas),尤其包括微囊性附屬器癌 (microcystic adnexal carcinoma) 與 hidradenocarcinoma,常可模擬自各種原發部位(最常見為乳房、肺、胃腸道或卵巢)轉移至皮膚的腺癌。汗腺腺瘤 (eccrine adenoma) 因其導管形成,在此類病例中亦可能進入鑑別診斷,但缺乏浸潤性生長
1533 個別腫瘤
A
B
1534 皮膚轉移與皮膚 Paget 病
型態與細胞學異型性,一般可將此實體與皮膚的腺癌性內臟轉移區分開來。這些實體之間的區別,尤其是汗腺導管癌 (eccrine ductal carcinoma),僅憑組織學可能非常困難;免疫組化有時非常有用。
有人建議 p63 可作為標記,用以區分原發性附屬器腫瘤與皮膚的轉移性腺癌:p63 一般表現於皮膚附屬器腫瘤,而在轉移性腺癌(乳房、胃腸道、肺)中缺乏。然而須注意,p63 免疫組化染色無法用於區分原發與轉移性鱗狀細胞癌(無論是肺或頭頸部來源)或轉移性尿路上皮癌 (urothelial carcinomas),因為它可在皮膚與其他複層上皮的正常基底細胞中常規地被偵測到,亦見於攝護腺與呼吸道上皮。p63 亦為乳房肌上皮細胞 (myoepithelial cells) 的標記。近期有人建議 p40 在區分原發性皮膚附屬器腫瘤與皮膚轉移上具有較佳的特異性,但其有與前述 p63 相似的警語與缺點。
這些觀察也獲得其他研究的支持。Qureshi 及其同事研究了 15 例轉移至皮膚的癌,包括 14 例腺癌與 1 例尿路上皮癌。只有一例腺癌顯示部分 p63 表現,而此為一分化差的食道癌。Sariya 及其同事發現,當作為單一標記使用時,p63 染色陽性對原發性附屬器腫瘤具有最高敏感度 (96%),而 p63 染色陰性對轉移則具有最高的陽性預測值。Kanitakis 及其同事也報告,絕大多數 (88.5%) 原發性皮膚腫瘤表現 p63,而 89% 轉移至皮膚的腫瘤為 p63 陰性。Ivan 及其同事也證明,在那些罕見的轉移性汗腺癌轉移至其他皮膚部位與淋巴結的病例中,強 p63 表現得以保留。因此,將 p63 用於一組免疫組化研究中,可能對轉移性腺癌與顯示導管分化的原發性皮膚腫瘤之鑑別診斷有價值。雖然仍需更多研究,p40 在區分原發與轉移腫瘤上可能顯示優於 p63 的特異性。
另一項曾被報導對皮膚轉移與原發性皮膚附屬器腫瘤鑑別診斷有用的免疫組化標記為 CK5/6,它表現於大多數原發性皮膚附屬器腫瘤,但僅罕見於內臟腺癌的皮膚轉移。另一項標記 podoplanin (D2-40) 也被報導在原發性附屬器腫瘤中呈陽性,而在各種來源(肺、乳房、胃腸道或泌尿生殖道)的轉移腫瘤中呈陰性。後續一項研究建議將 p63 與 D2-40 (podoplanin) 配對使用,以提高此情境下的特異性。Calretinin 是一種表現於間皮、上皮與基質細胞的鈣結合蛋白 (calcium-binding protein),已發現它在轉移腫瘤中呈陽性,但在某些原發性皮膚腫瘤病例中也呈陽性。
A
對組織學特徵進行適當評估,並結合完整的臨床病史與審慎選用的免疫組化抗體組合,應能解決大多數的診斷問題。然而,必須強調,診斷絕不應僅基於免疫組化結果。
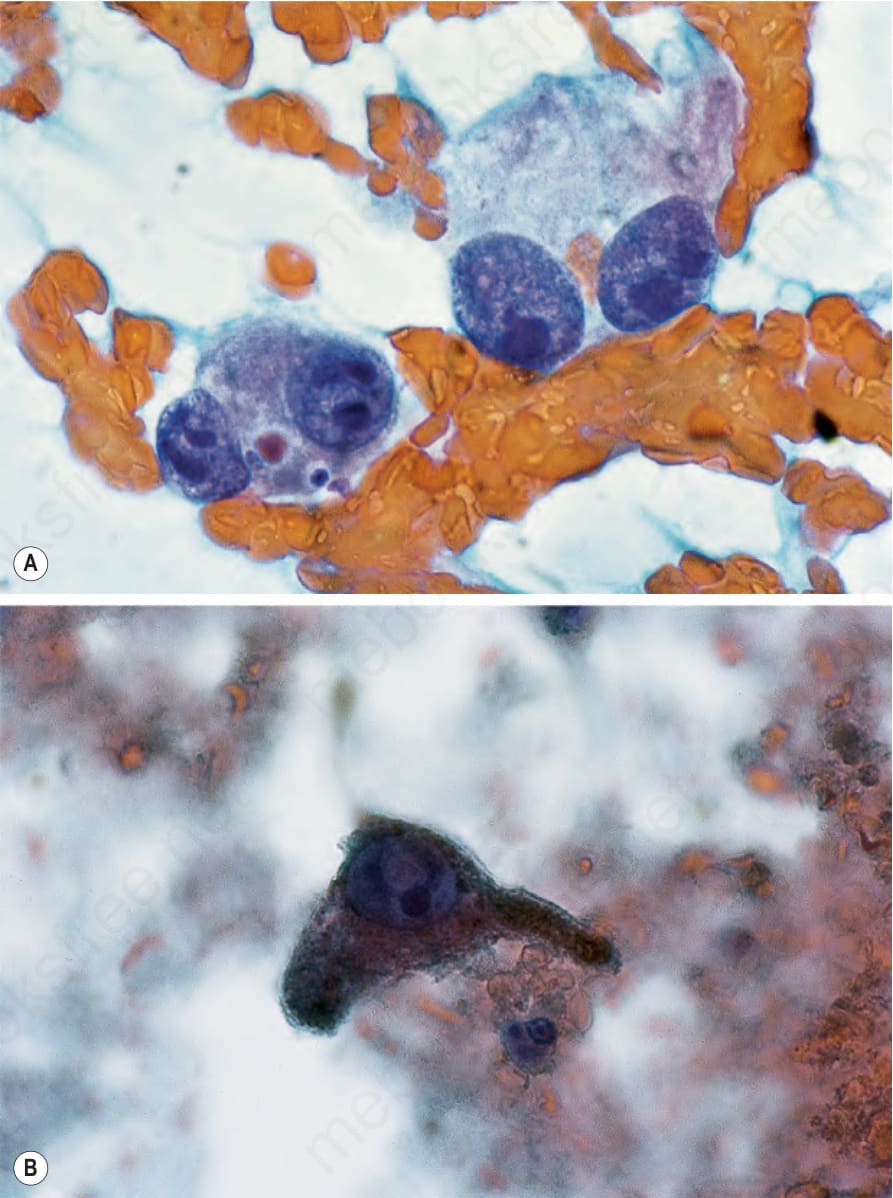
圖 30-26:細針抽吸 (fine needle aspirate):此為轉移性惡性黑色素瘤 (metastatic malignant melanoma) 之範例。注意 (A) 大核仁 (large nucleoli) 與 (B) 細胞質內色素 (intracytoplasmic pigment)。承蒙 G.T. McKee, MD, Massachusetts General Hospital, Boston, USA 惠予提供。
Fig. 30.26 Fine needle aspirate: this is an example of metastatic malignant melanoma. Note (A) the large nucleoli and (B) the intracytoplasmic pigment. By courtesy of G.T. McKee, MD, Massachusetts General Hospital, Boston, USA.
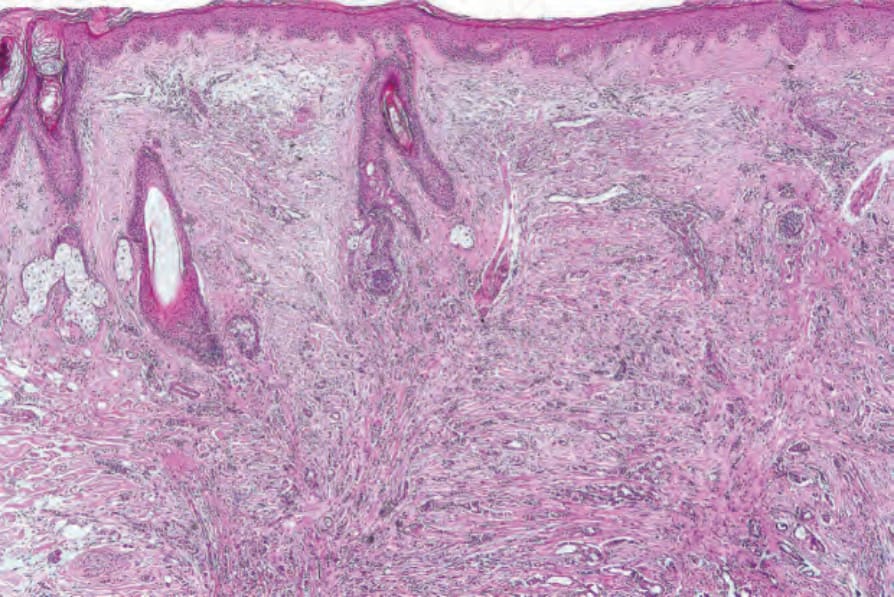
圖 30-27:轉移性乳房癌(腫瘤性禿髮 [alopecia neoplastica]):一名中年女性的頭皮切片顯示真皮被腫瘤廣泛浸潤,導致毛皮脂腺結構 (pilosebaceous structures) 喪失。
Fig. 30.27 Metastatic carcinoma of breast (alopecia neoplastica): scalp biopsy from a middleaged female shows extensive infiltration of the dermis by tumor, resulting in loss of pilosebaceous structures.
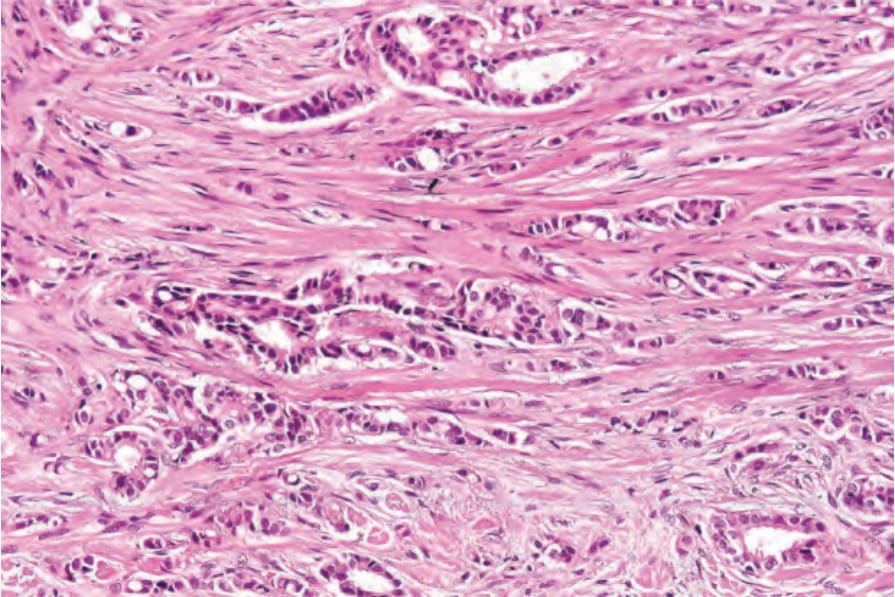
圖 30-28:轉移性乳房癌(腫瘤性禿髮 [alopecia neoplastica]):腫瘤浸潤由分散於緻密纖維基質 (dense fibrous stroma) 中的腫瘤細胞索 (cords) 組成。注意腺體分化 (glandular differentiation)。
Fig. 30.28 Metastatic carcinoma of breast (alopecia neoplastica): the tumor infiltrate is composed of cords of tumor cells dispersed in a dense fibrous stroma. Note the glandular differentiation.
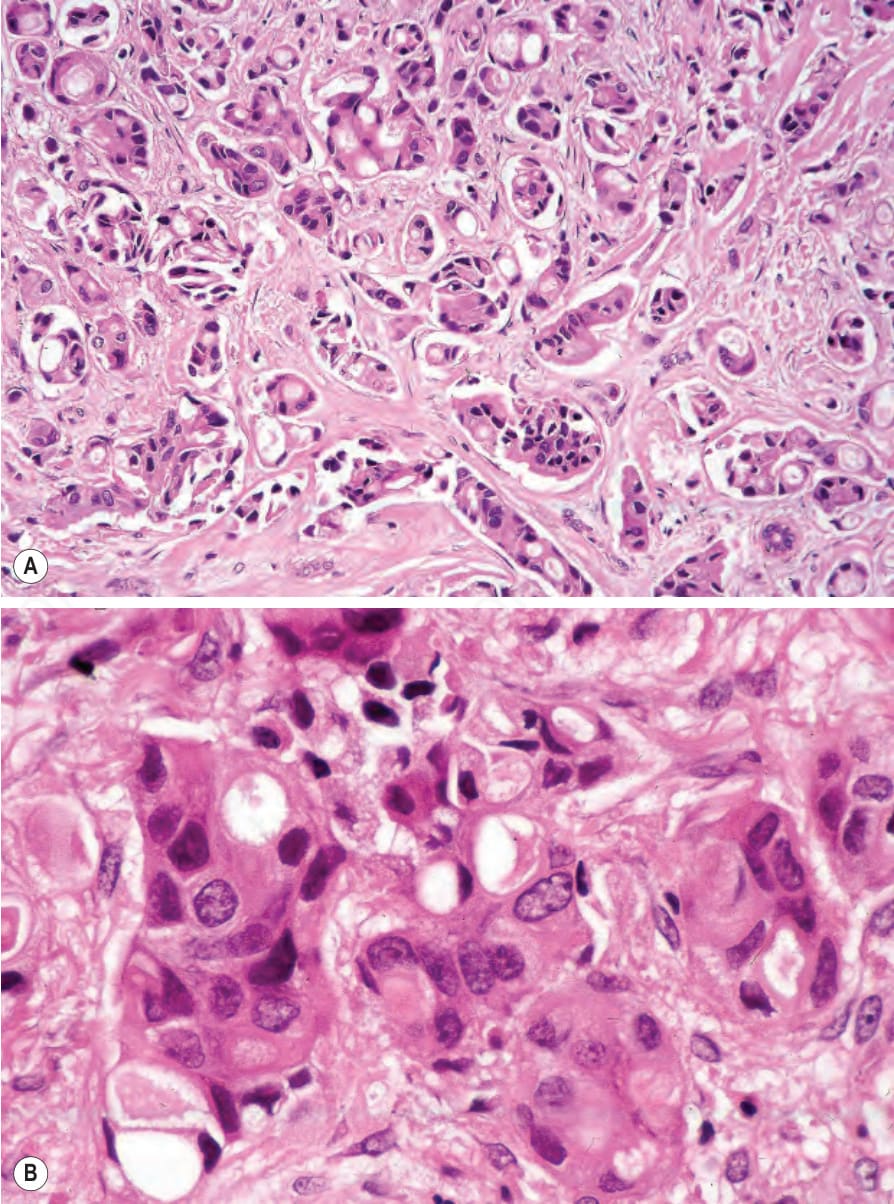
圖 30-29:轉移性乳房癌(腫瘤性禿髮 [alopecia neoplastica]):(A) 此例惡性度高得多。注意多形性 (pleomorphism);(B) 可見細胞質內腔隙 (intracytoplasmic lumina)。
Fig. 30.29 Metastatic carcinoma of the breast (alopecia neoplastica): (A) this example is much more high grade. Note the pleomorphism; (B) intracytoplasmic lumina are present.
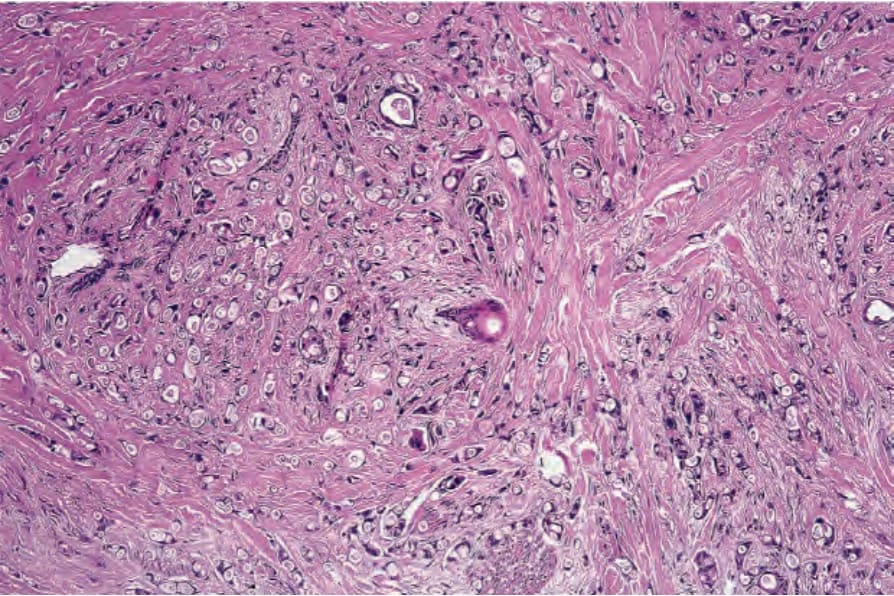
圖 30-30:硬皮病樣轉移性乳房癌 (sclerodermatous metastatic carcinoma of breast):細胞分散於極為緻密的纖維基質 (dense fibrous stroma) 中。
Fig. 30.30 Sclerodermatous metastatic carcinoma of breast: the cells are dispersed in a very dense fibrous stroma.
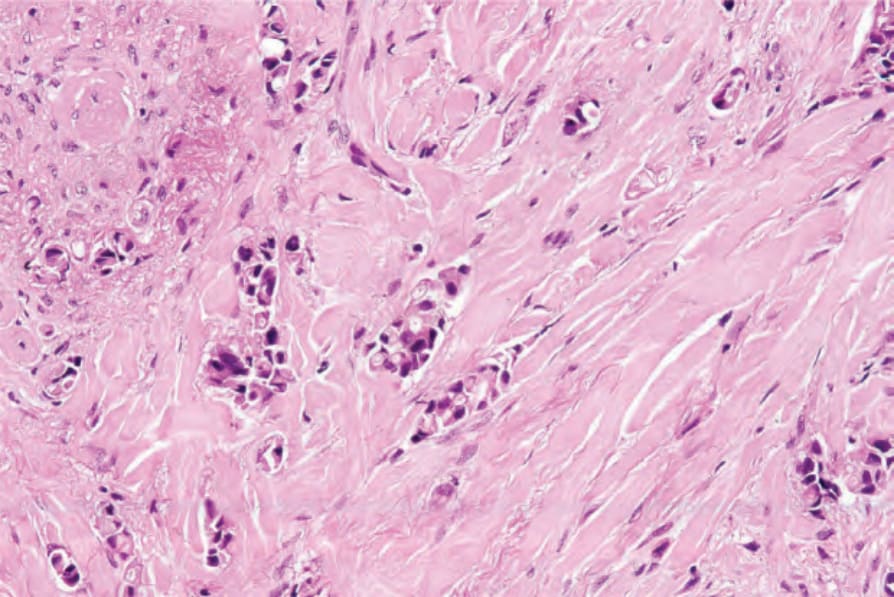
圖 30-31:硬皮病樣轉移性乳房癌 (sclerodermatous metastatic carcinoma of the breast):較高倍視野。
Fig. 30.31 Sclerodermatous metastatic carcinoma of the breast: higher-power view.
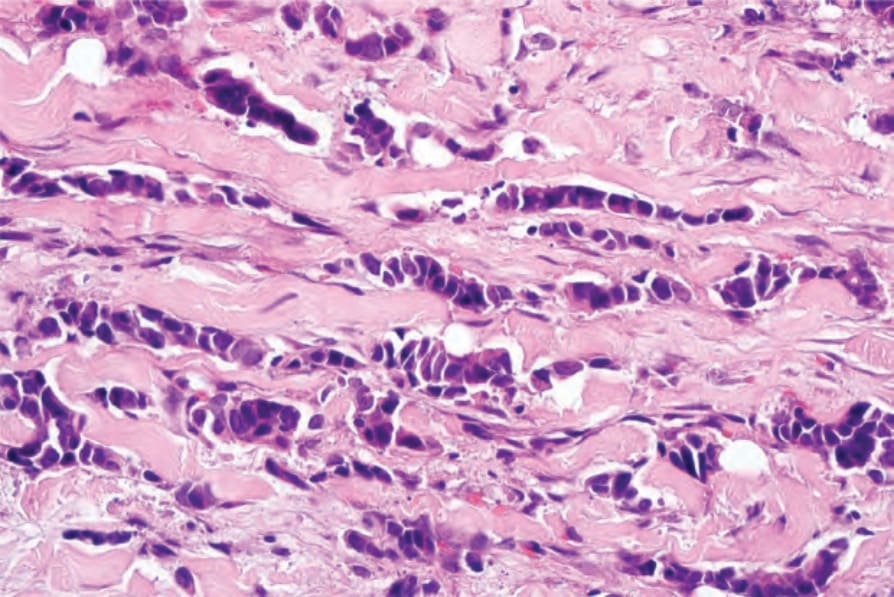
圖 30-32:轉移性乳房癌:此視野中清楚呈現特徵性的疊銅板外觀 (stacked-penny appearance)。承蒙 J. Cohen, MD, Dermatopathology Laboratory, Tucson, USA 惠予提供。
Fig. 30.32 Metastatic carcinoma of breast: the characteristic stacked-penny appearance is well demonstrated in this field. By courtesy of J. Cohen, MD, Dermatopathology Laboratory, Tucson, USA.
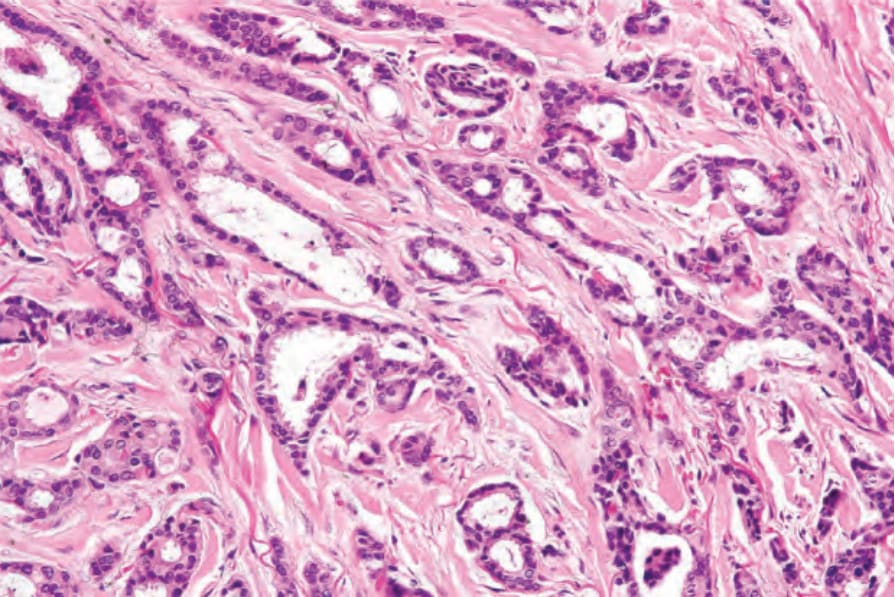
圖 30-33:轉移性乳房癌:此例中有發育良好的導管 (well-developed ducts)。
Fig. 30.33 Metastatic carcinoma of breast: in this example, there are well-developed ducts.
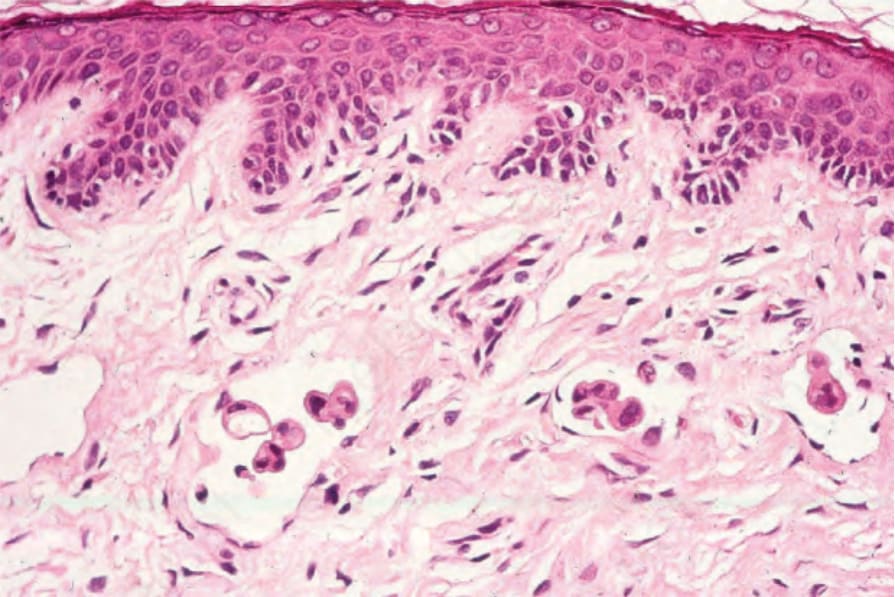
圖 30-34:發炎性癌 (inflammatory carcinoma):有表淺真皮淋巴管 (superficial dermal lymphatics) 受侵犯。
Fig. 30.34 Inflammatory carcinoma: there is involvement of the superficial dermal lymphatics.
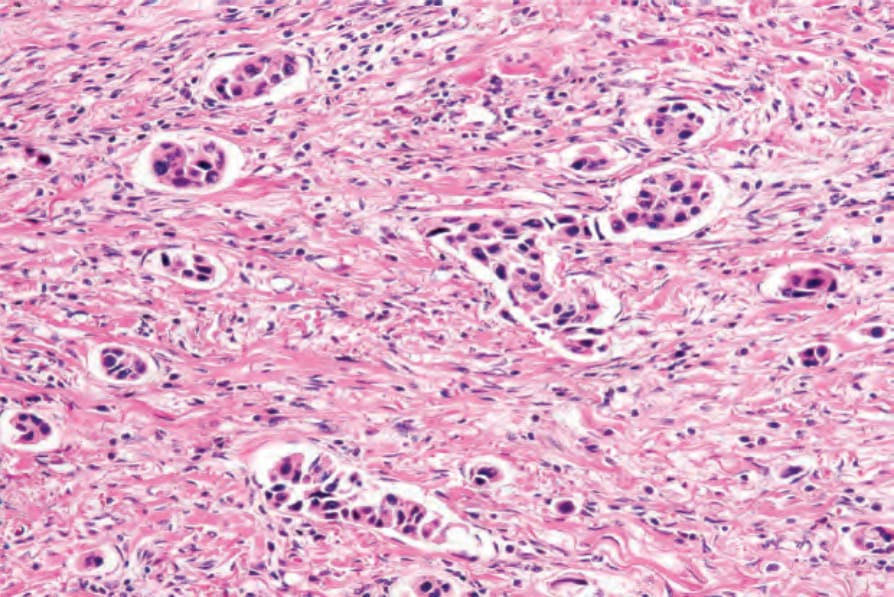
圖 30-35:發炎性癌 (inflammatory carcinoma):此例中有無數血管受波及。
Fig. 30.35 Inflammatory carcinoma: in this example, innumerable vessels were affected.
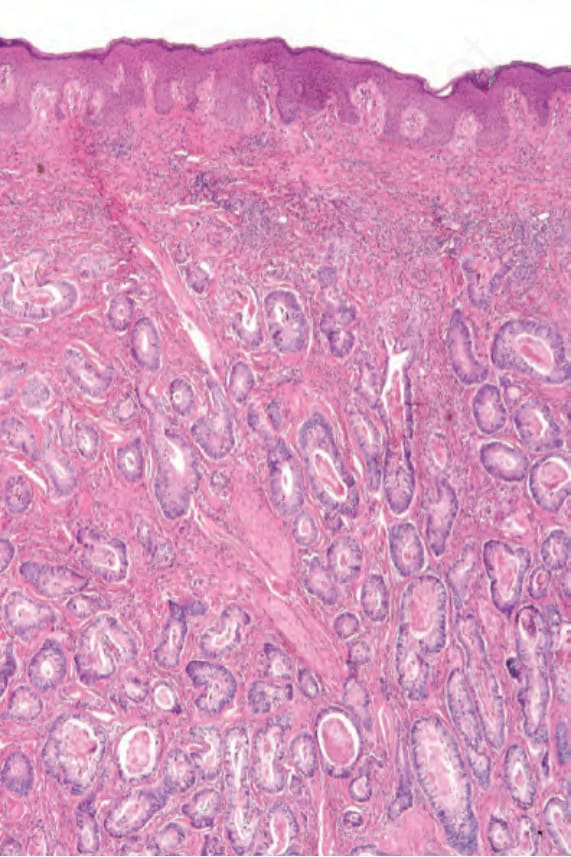
圖 30-36:轉移性大腸腺癌 (metastatic colonic adenocarcinoma):真皮有廣泛浸潤。注意形成良好的導管結構 (well-formed ductal structures)。
Fig. 30.36 Metastatic colonic adenocarcinoma: there is widespread infiltration of the dermis. Note the well-formed ductal structures.
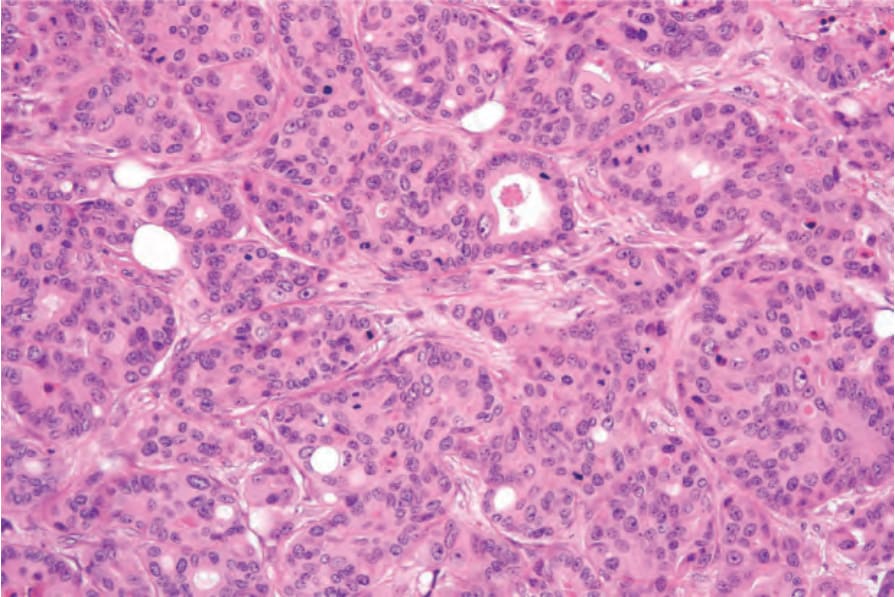
圖 30-37:轉移性大腸腺癌 (metastatic colonic adenocarcinoma):高倍視野。
Fig. 30.37 Metastatic colonic adenocarcinoma: high-power view.
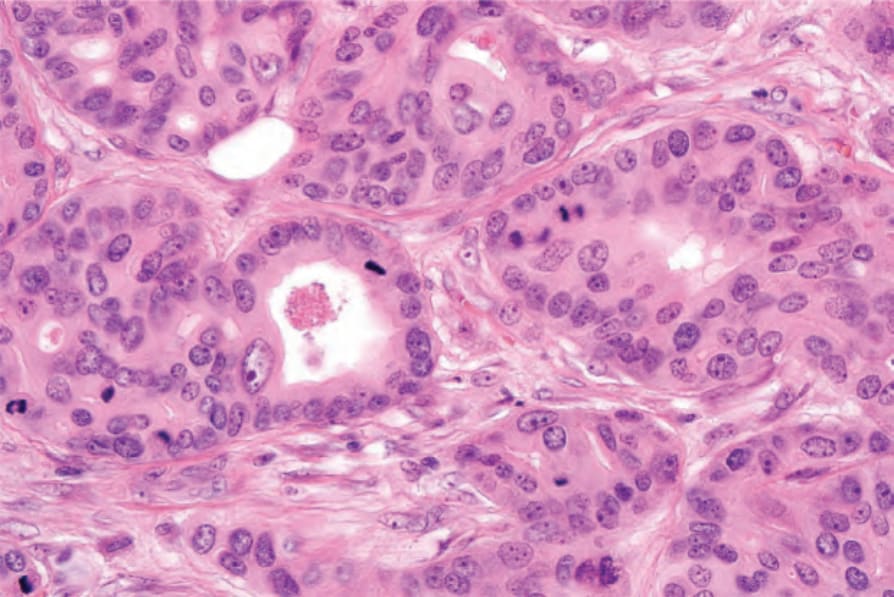
圖 30-38:轉移性大腸腺癌 (metastatic colonic adenocarcinoma):有明顯的有絲分裂活性 (mitotic activity)。
Fig. 30.38 Metastatic colonic adenocarcinoma: there is conspicuous mitotic activity.
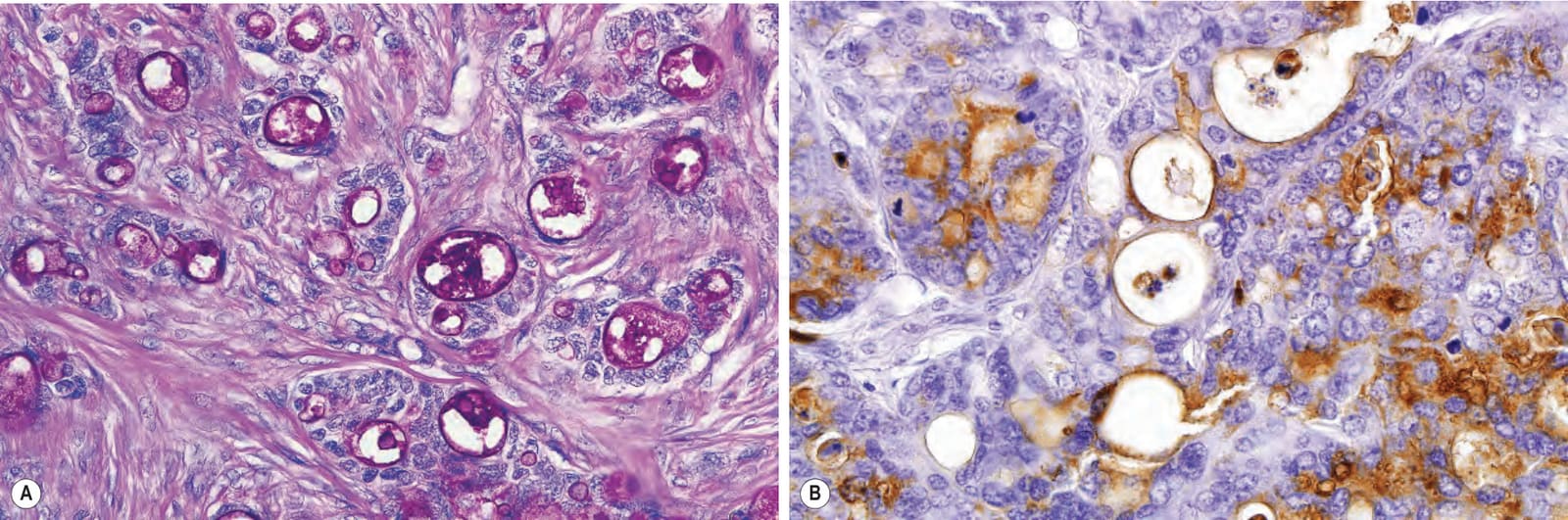
圖 30-39:轉移性大腸腺癌 (metastatic colonic adenocarcinoma):(A) 腫瘤呈強 PAS 陽性、抗澱粉酶 (diastase resistant);(B) 上皮襯裡被癌胚抗原 (carcinoembryonic antigen) 勾勒出輪廓。
Fig. 30.39 Metastatic colonic adenocarcinoma: (A) the tumor is strongly PAS positive, diastase resistant; (B) the epithelial lining is outlined by carcinoembryonic antigen.
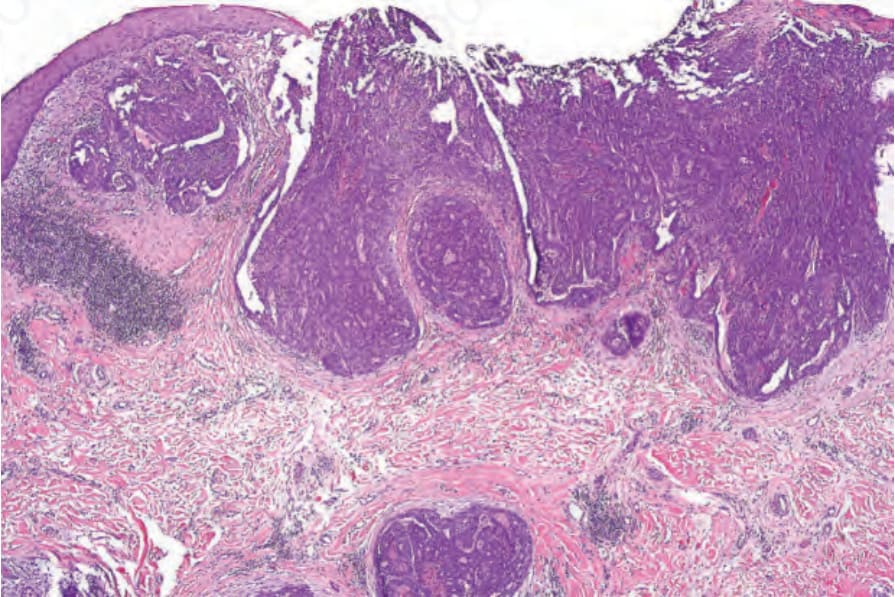
圖 30-40:轉移性甲狀腺乳頭狀癌 (metastatic thyroid papillary carcinoma):表淺與深層真皮中可見一處潰瘍、多灶性、具乳頭狀構造 (papillary configuration) 的癌。
Fig. 30.40 Metastatic thyroid papillary carcinoma: an ulcerated, multifocal carcinoma with a papillary configuration is present in the superficial and deep dermis.
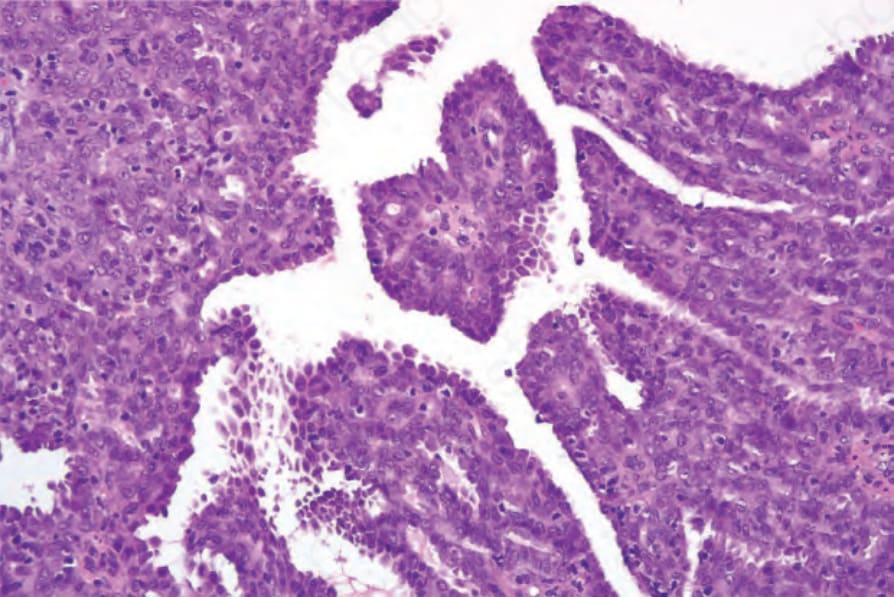
圖 30-41:轉移性甲狀腺乳頭狀癌 (metastatic thyroid papillary carcinoma):乳頭被覆高柱狀上皮細胞 (tall columnar epithelial cells)。
Fig. 30.41 Metastatic thyroid papillary carcinoma: the papillae are covered with tall columnar epithelial cells.
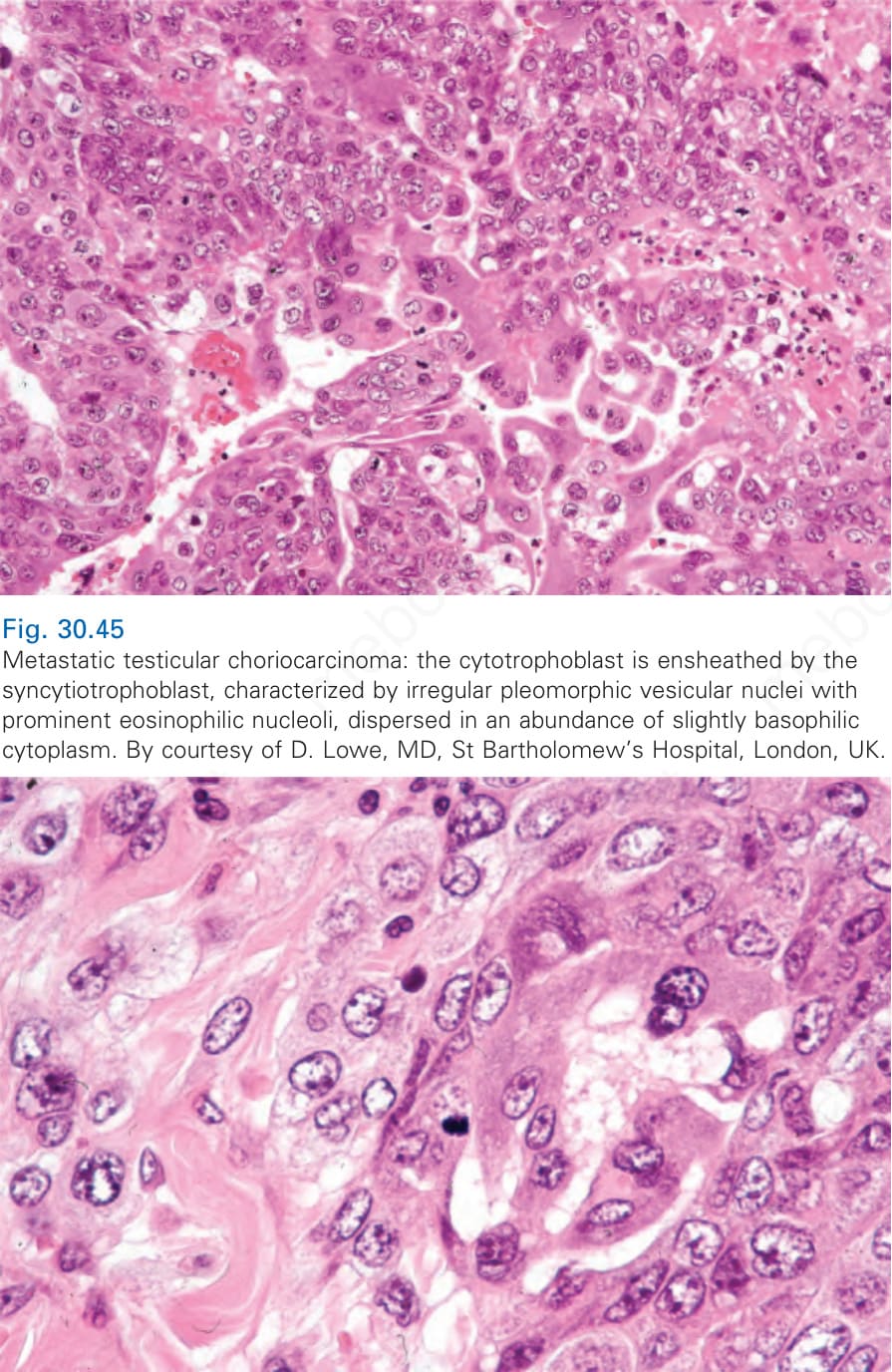
圖 30-45:轉移性睪丸絨毛膜癌 (metastatic testicular choriocarcinoma):細胞滋養層 (cytotrophoblast) 被合體滋養層 (syncytiotrophoblast) 包鞘,後者的特徵為不規則多形性囊泡狀核 (irregular pleomorphic vesicular nuclei),具有明顯的嗜伊紅核仁 (eosinophilic nucleoli),分散於大量略呈嗜鹼性 (basophilic) 的細胞質中。承蒙 D. Lowe, MD, St Bartholomew’s Hospital, London, UK 惠予提供。
Fig. 30.45 Metastatic testicular choriocarcinoma: the cytotrophoblast is ensheathed by the syncytiotrophoblast, characterized by irregular pleomorphic vesicular nuclei with prominent eosinophilic nucleoli, dispersed in an abundance of slightly basophilic cytoplasm. By courtesy of D. Lowe, MD, St Bartholomew’s Hospital, London, UK.
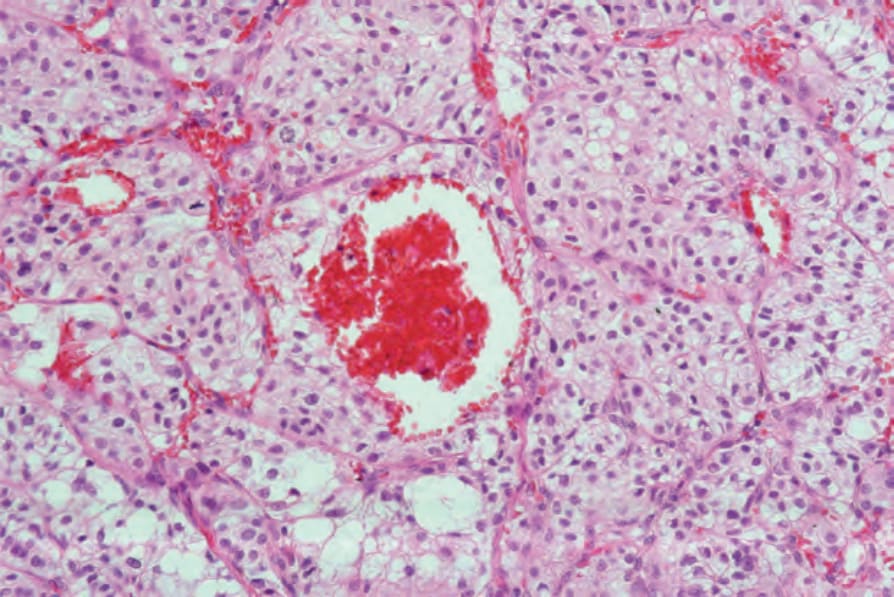
圖 30-49:轉移性腎(透明細胞)癌 (metastatic renal [clear cell] carcinoma):注意透明細胞 (clear cells) 與特徵性出血 (hemorrhage)。
Fig. 30.49 Metastatic renal (clear cell) carcinoma: note the clear cells and characteristic hemorrhage.
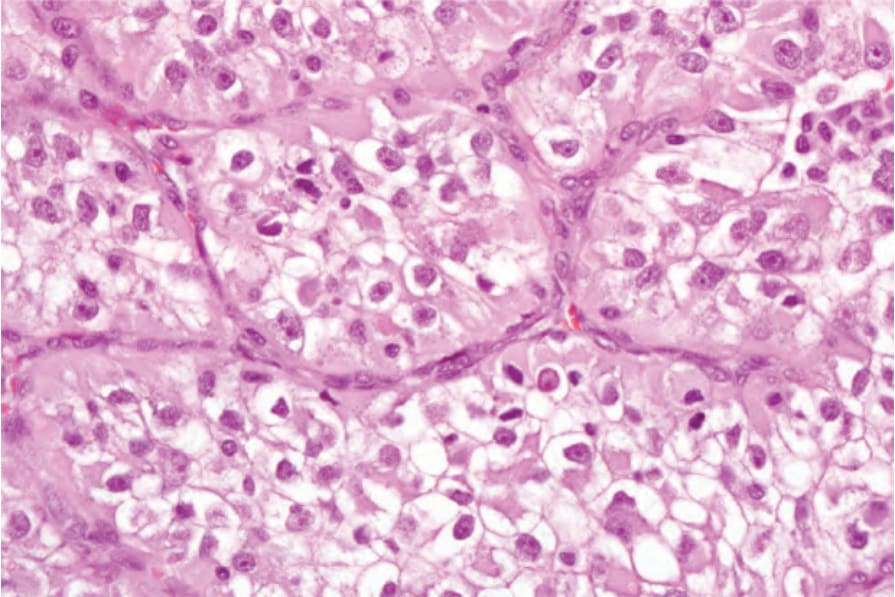
圖 30-50:轉移性腎(透明細胞)癌 (metastatic renal [clear cell] carcinoma):透明細胞外觀係因肝醣 (glycogen) 與脂質 (lipid) 的堆積所致。
Fig. 30.50 Metastatic renal (clear cell) carcinoma: the clear cell appearance is due to the accumulation of glycogen and lipid.
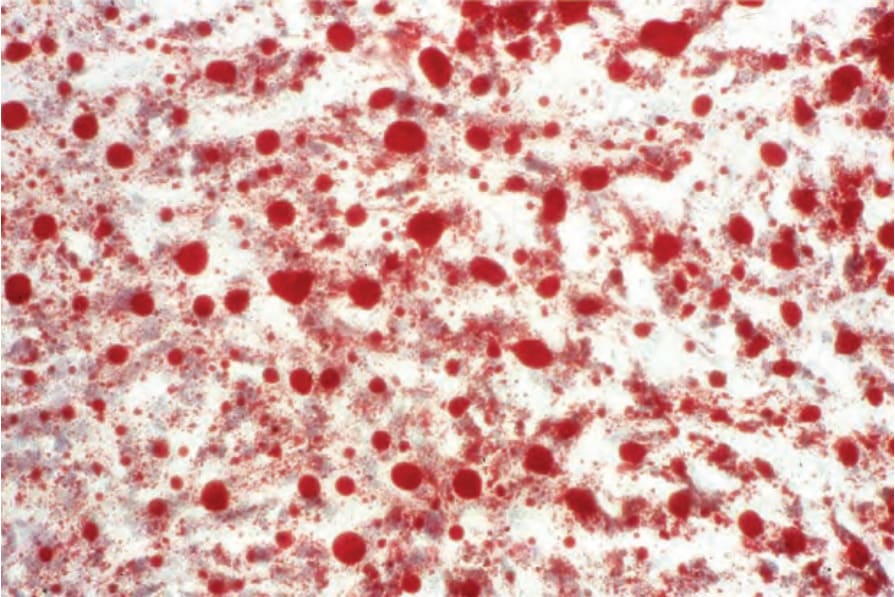
圖 30-51:轉移性腎(透明細胞)癌 (metastatic renal [clear cell] carcinoma):針對脂質的油紅 O 染色 (oil red O staining) 呈強陽性。
Fig. 30.51 Metastatic renal (clear cell) carcinoma: oil red O staining for lipid is strongly positive.
B
黏液性癌 (Mucinous carcinoma)
黏液性癌 (mucinous carcinoma) 的特徵是由纖維索 (fibrous strands) 所形成的隔間,其內含有黏液池 (pools of mucin) 與漂浮的腫瘤細胞巢 (floating nests of tumor cells)。這些細胞通常具有充足的細胞質、位於中央的囊泡狀核,以及僅輕度的細胞學異型性。雖然黏液性癌有時可作為皮膚的原發腫瘤出現(最常見為年長男性頭頸部一個緩慢生長的結節),但有時它代表自乳房、胃、結腸、直腸與胰臟等部位轉移而來的播散 (Fig. 30.42)。
原發與轉移腫瘤之間的區別,通常僅憑組織學依據無法達成;不過在一個大型病例系列中,Kazakov 及其同事報告,存在原位成分 (in situ component) 對原發性皮膚腫瘤的診斷特別有幫助。然而,缺乏此成分並不能排除診斷。骯髒壞死 (dirty necrosis) 已被報導為腸道來源轉移性腺癌的一項恆定組織學發現。發現於軀幹皮膚的黏液性癌通常代表來自內臟原發腫瘤的轉移性疾病。
「印戒細胞」(signet ring) 轉移,其中細胞內黏液堆積導致細胞核被壓擠至細胞周邊,可見於胃、大腸與胰臟的原發腫瘤 (Fig. 30.43)。罕見情況下,它們也可發生於子宮頸內膜與膽囊。印戒細胞變化可見於若干皮膚腫瘤,包括汗腺癌、黑色素瘤、鱗狀細胞癌與基底細胞癌。
具有歷史意義的是,黏液的類型有助於區分原發性皮膚黏液性癌與胃腸道原發的皮膚轉移。在原發性皮膚黏液性癌中,黏液含有豐富的唾液黏蛋白 (sialomucin),因此在 pH 2.5 時 Alcian blue 陽性,但在 pH 1.0 或 0.4 時則否。轉移至皮膚的胃腸道黏液性癌所見的黏液含有硫黏蛋白 (sulfamucins),其
1535 個別腫瘤
A
B
可見於 t(6;9)(q2223;p2324),導致唾液腺腺樣囊性癌 (salivary adenoid cystic carcinomas) 中所見的 MYB-NFIB 融合 (MYB-NFIB fusions)。
絨毛膜癌 (Choriocarcinoma)
絨毛膜癌 (choriocarcinoma) 雖然通常為妊娠性腫瘤,但也可源自睪丸,以及較罕見地源自縱膈、卵巢,而極例外地源自胎盤部位滋養層腫瘤 (placental site trophoblastic tumor)。伴隨顯著的血管侵犯傾向,皮膚轉移並不少見。此腫瘤特徵性地呈出血性與壞死性;存活組織常僅能在周邊辨識。
在 pH 1.0 與 0.4 時 Alcian blue 陽性。然而,這些染色在大多數實驗室中並不常於可變 pH 值下進行。
轉移至皮膚的胃腸道黏液性腫瘤一般保留 CK20 表現,此在原發性皮膚黏液性汗腺癌中則不可見。強 CDX2 表現已在轉移至其他內臟器官的胃腸道轉移中被充分記載,並曾於腸道來源黏液性皮膚轉移的個別病例中觀察到。SATB2 對胃腸道來源轉移腫瘤具有相似的敏感度 (80–90%),並可能具有相較於 CDX2 增加或互補的特異性。GATA3 已被報導於原發性皮膚黏液性癌,因此不能用以支持乳房來源。若辨識出皮膚黏液性腺癌的原位成分,周圍的肌上皮細胞 (myoepithelial cells) 可標記 p63、CK5/6、calponin 或平滑肌肌動蛋白 (smooth muscle actin, SMA)。轉移性黏液性癌通常為 p63 陰性。
絨毛膜癌是一種滋養層組織 (trophoblastic tissue) 的腫瘤:細胞滋養層 (cytotrophoblast) 為增殖成分,合體滋養層 (syncytiotrophoblast) 為具荷爾蒙活性的成分。病灶由這兩種細胞類型不等量的混合所組成,且找不到絨毛膜絨毛 (chorionic villi) (Figs 30.44 and 30.45)。細胞滋養層由規則的多面體細胞 (polyhedral cells) 組成,排列成片狀與索狀,各細胞具有淡染的細胞質與相當大的囊泡狀核,常有明顯的核仁。有絲分裂象 (mitotic figures) 可能明顯,且常為異常。相反地,合體滋養層由極大的多形性細胞 (pleomorphic cells) 組成,具有大量、略呈嗜鹼性的細胞質。它們常為多核 (multinucleate),且常與相鄰的細胞滋養層緊密相伴 (Fig. 30.46)。免疫組化呈現促性腺激素 (gonadotrophin) 是有用的診斷輔助 (Fig. 30.47)。源自睪丸混合性腫瘤的絨毛膜癌成分以及產後病例皆可轉移至皮膚。
腺樣囊性癌 (Adenoid cystic carcinoma)
原發性皮膚腺樣囊性癌 (primary cutaneous adenoid cystic carcinoma) 罕見,因此必須與轉移性疾病區別。全身性原發腫瘤的來源包括唾液腺、淚腺、子宮頸、支氣管或乳房。然而在臨床實務中,這些內臟腫瘤通常為緩慢生長的病灶,其皮膚表現極不可能發生,雖然曾有此類個別病例被描述。因此皮膚中大多數的腺樣囊性癌代表原發腫瘤。轉移病灶最常源自唾液腺。一部分原發性皮膚腺樣囊性癌可帶有 MYB 重排 (MYB rearrangements),如同
透明細胞癌 (Clear cell carcinoma)
轉移性透明細胞癌 (metastatic clear cell carcinoma) 典型上源自腎臟,但其他來源包括肺、肝,以及卵巢、子宮內膜、子宮頸與陰道的中腎透明細胞癌 (mesonephric clear cell carcinomas)。此腫瘤由索狀、肺泡狀,以及偶爾的管狀結構組成,由含有脂質與肝醣的均勻透明細胞所構成 (Figs 30.48–30.51)。基質通常纖細且高度血管化,常導致明顯的出血區,因而說明了此類轉移特徵性的臨床外觀。它必須在組織學上與透明細胞鱗狀細胞癌 (clear cell squamous carcinoma)、透明細胞汗腺癌 (clear cell hidradenocarcinoma)、透明
1536 皮膚轉移與皮膚 Paget 病
細胞汗孔癌 (clear cell porocarcinoma)、毛根鞘癌 (trichilemmal carcinoma)、皮脂腺癌 (sebaceous carcinoma)、無色素性透明細胞黑色素瘤 (amelanotic clear cell melanoma)、PEComa,以及透明細胞肉瘤(軟組織黑色素瘤 [melanoma of soft parts])區別。
免疫組化研究可作為鑑別診斷的輔助,但它們不太具特異性。原發性腎細胞癌 (renal cell carcinoma) 已顯示表現 CD10(常見急性淋巴母細胞白血病抗原 [common acute lymphoblastic leukemia antigen, CALLA]),在皮膚轉移性疾病中亦然。腎細胞癌標記 (renal cell carcinoma marker, RCC-Ma) 對腎細胞癌的皮膚轉移具有高特異性與中等敏感度。因此,RCC-Ma 陽性結果高度提示轉移性腎細胞癌的診斷;然而陰性結果並不能排除診斷。PAX8 是一種譜系特異性轉錄因子 (lineage-specific transcription factor),在腎臟腫瘤中呈陽性,但在卵巢與甲狀腺中亦然,故需在審慎考量鑑別診斷的情況下用於抗體組合。
1537 個別腫瘤
A
神經內分泌癌(小細胞癌)(Neuroendocrine carcinoma [small cell carcinoma])
轉移性神經內分泌癌 (metastatic neuroendocrine carcinoma) 可藉其獨特特徵辨識:小型、深染、圓形至卵圓形的核,伴隨幾乎難以察覺的細胞質 (Fig. 30.52)。此腫瘤的典型特徵是其血管周圍存在大量嗜鹼性核碎屑 (basophilic nuclear debris)。
B
支氣管神經內分泌癌 (bronchial neuroendocrine carcinoma) 必須與之區別的腫瘤包括他處發生的神經內分泌腫瘤(例如源自皮膚、胃腸道與子宮者)、甲狀腺髓質癌 (medullary carcinoma of the thyroid)、小細胞黑色素瘤 (small cell melanoma),以及固定不良的淋巴瘤檢體。免疫組化上,這些腫瘤表現一系列抗原,包括低分子量角蛋白 (low molecular weight keratin, CAM 5.2)、EMA、神經元特異性烯醇化酶 (neuron-specific enolase)、chromogranin、synaptophysin、CD56、PGP 9.5 與 bombesin。甲狀腺髓質癌表現降鈣素 (calcitonin)。唾液腺神經內分泌癌與皮膚腫瘤一貫顯示 CK20 的核周點狀陽性 (perinuclear dotlike positivity),這在它們與其他轉移性神經內分泌癌的鑑別診斷中很有用。Merkel 細胞癌 (Merkel cell carcinoma) 與非 Merkel 細胞原發性皮膚神經內分泌癌兩者皆應納入診斷考量。一些近期資料顯示,判定神經內分泌癌的原發部位可能極為重要。雖然對許多轉移而言,臨床相關性常能提供答案,免疫組化在達成診斷上常為重要輔助。近期隨著分子診斷的進展,有人建議使用 92 基因癌症分類器 (92-gene cancer classifier) 也是預測神經內分泌腫瘤原發部位的一種非常有用的方式。
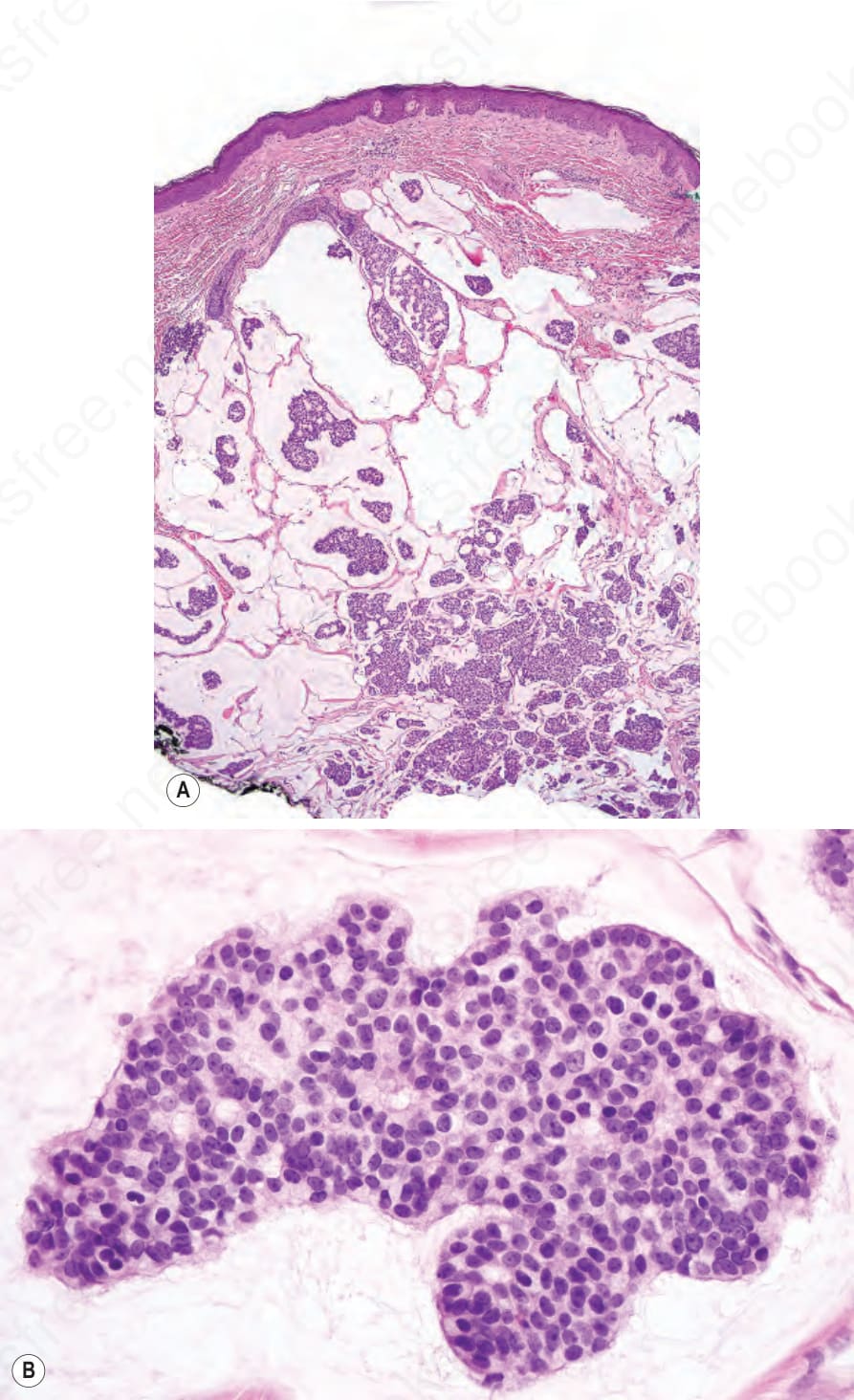
圖 30-42:轉移性黏液性癌 (metastatic mucinous carcinoma):(A) 一處轉移性黏液性癌沉積的低倍視野;(B) 高倍視野。原發與轉移疾病在組織學上無法區分,除非在前者中辨識出原位成分 (in situ component)。
Fig. 30.42 Metastatic mucinous carcinoma: (A) low-power view of a deposit of metastatic mucinous carcinoma; (B) high-power view. Primary and metastatic diseases are histologically indistinguishable unless an in situ component is identified in the former.
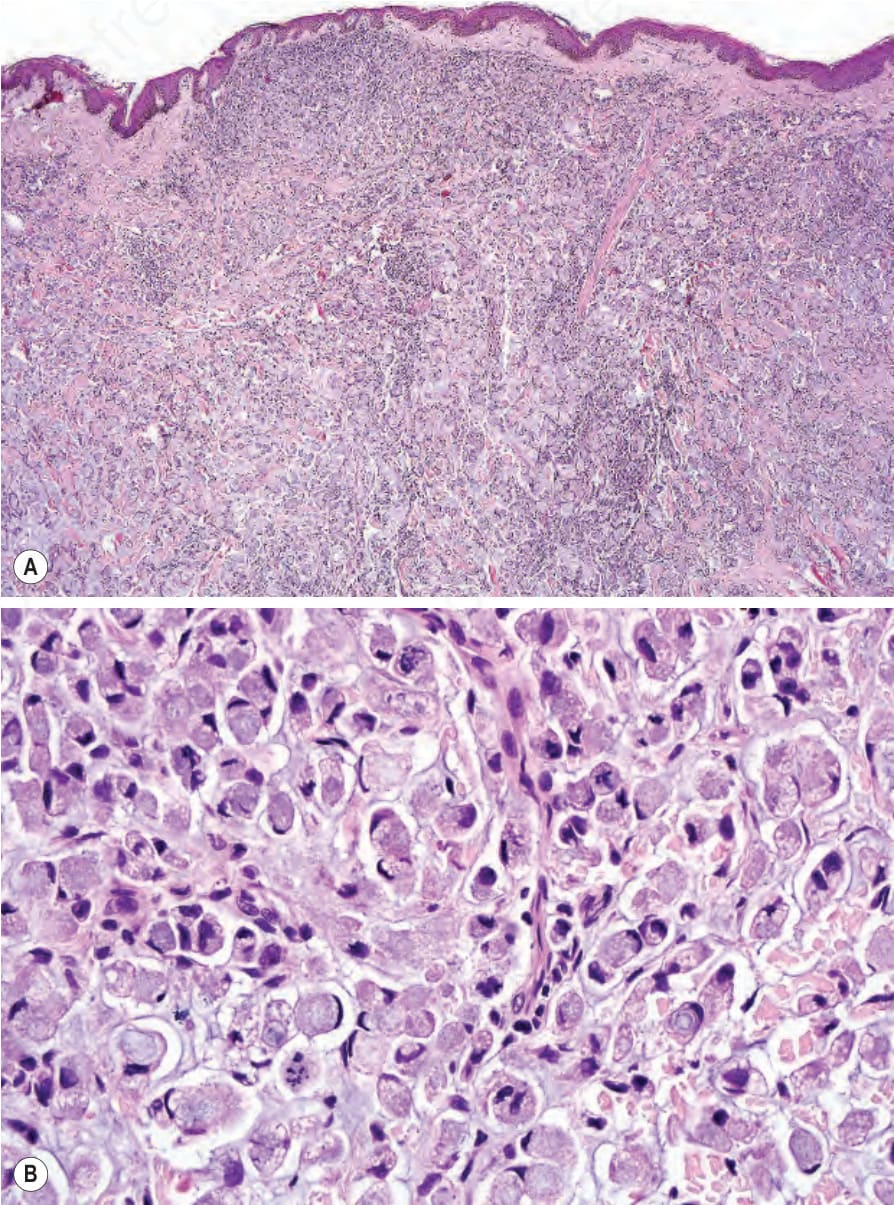
圖 30-43:轉移性印戒細胞癌 (metastatic signet-ring cell carcinoma):(A, B) 真皮被一群純印戒細胞 (signet ring cells) 完全取代。
Fig. 30.43 Metastatic signet-ring cell carcinoma: (A, B) the dermis is completely replaced by a pure population of signet ring cells.
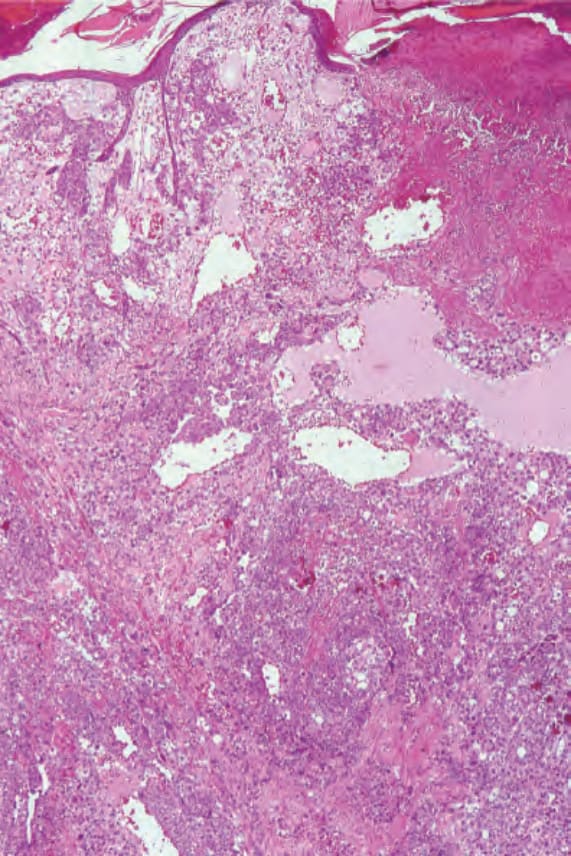
圖 30-44:轉移性睪丸絨毛膜癌 (metastatic testicular choriocarcinoma):低倍視野顯示一充滿真皮的出血性腫瘤。承蒙 D. Lowe, MD, St Bartholomew’s Hospital, London, UK 惠予提供。
Fig. 30.44 Metastatic testicular choriocarcinoma: low-power view showing a hemorrhagic tumor filling the dermis. By courtesy of D. Lowe, MD, St Bartholomew’s Hospital, London, UK.
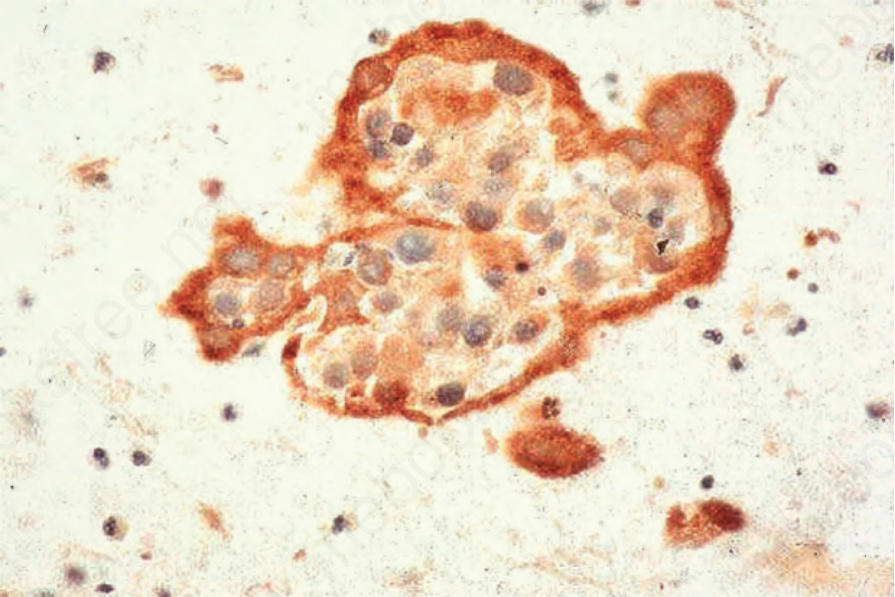
圖 30-46:轉移性睪丸絨毛膜癌 (metastatic testicular choriocarcinoma):高倍視野。承蒙 D. Lowe, MD, St Bartholomew’s Hospital, London, UK 惠予提供。
Fig. 30.46 Metastatic testicular choriocarcinoma: high-power view. By courtesy of D. Lowe, MD, St Bartholomew’s Hospital, London, UK.
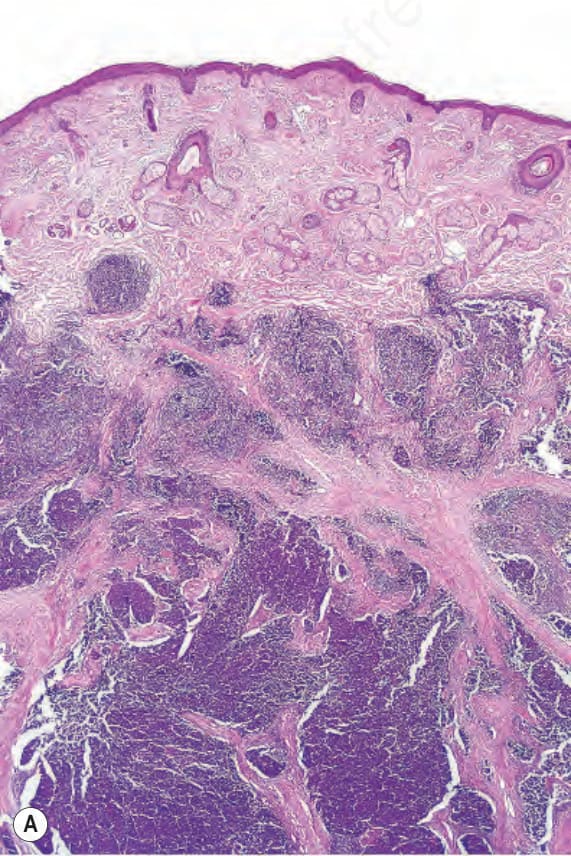
圖 30-47:轉移性睪丸絨毛膜癌 (metastatic testicular choriocarcinoma):有針對人類絨毛膜促性腺激素 (human chorionic gonadotrophin) 的強標記(細針抽吸 [fine needle aspiration])。
Fig. 30.47 Metastatic testicular choriocarcinoma: there is strong labeling for human chorionic gonadotrophin (fine needle aspiration).
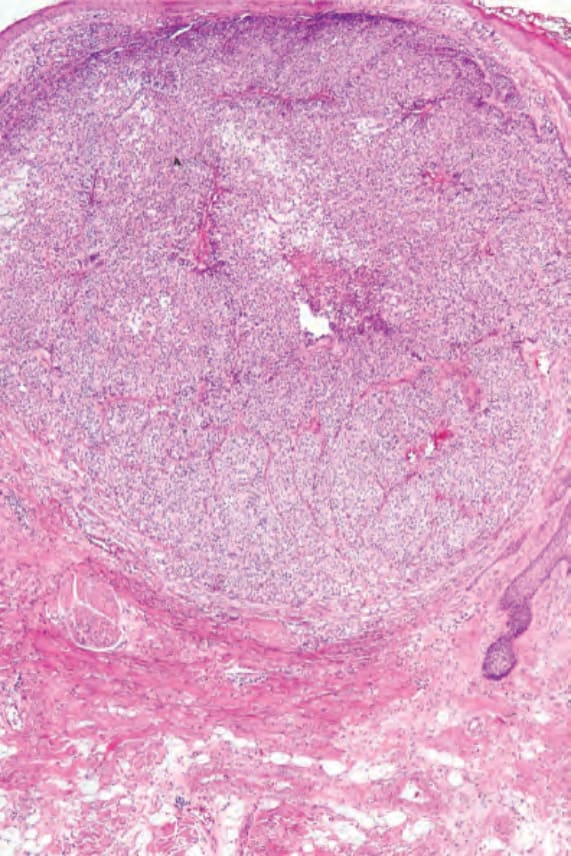
圖 30-48:轉移性腎(透明細胞)癌 (metastatic renal [clear cell] carcinoma):真皮中有一界限分明的腫瘤結節。
Fig. 30.48 Metastatic renal (clear cell) carcinoma: there is a well-circumscribed tumor nodule in the dermis.
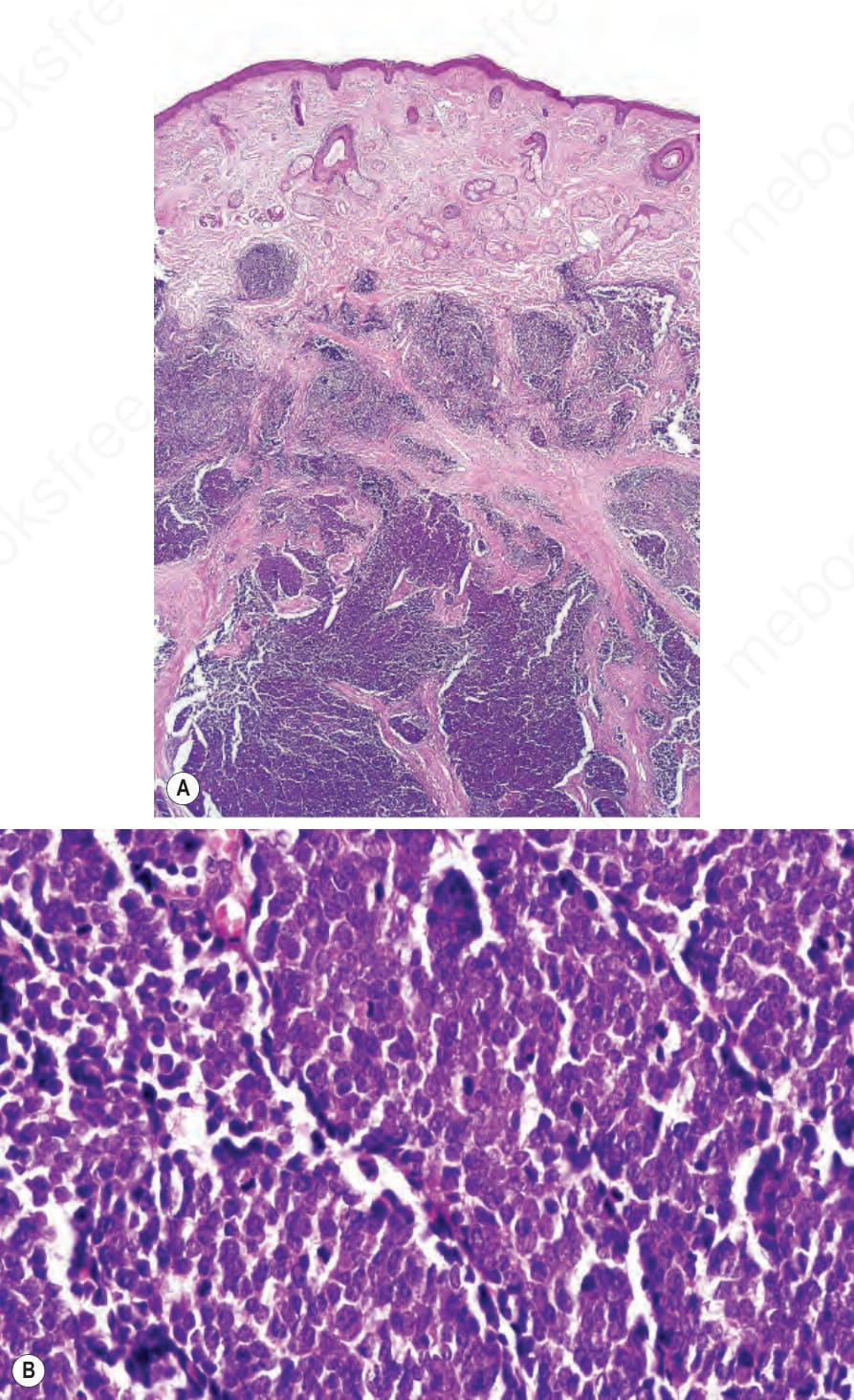
圖 30-52:轉移性小細胞癌 (metastatic small cell carcinoma):(A, B) 在缺乏臨床病史或免疫組化的情況下,無法將此轉移與原發性皮膚神經內分泌癌 (primary cutaneous neuroendocrine carcinoma) 區分開來。
Fig. 30.52 Metastatic small cell carcinoma: (A, B) in the absence of clinical history or immunohistochemistry, it would not be possible to distinguish this metastasis from a primary cutaneous neuroendocrine carcinoma.