Adenocarcinoma
Adenocarcinoma
than 2% of esophageal cancers disseminate to the skin), oral cavity, larynx, and cervix.35–41 It may less frequently arise from a squamous carcinoma elsewhere on the integument, anus, vulva, penis, vagina, and tonsil.42 Poorly differentiated metastases often cause difficulties, and multiple sections may have to be scrutinized carefully before foci of squamous differentiation (keratinization or intercellular bridges) are detected. An important point is that it is not possible to distinguish metastatic poorly differentiated squamous cell from transitional cell tumors in the absence of keratinization. In addition, the site of origin of squamous cell carcinomas is generally not distinguished by morphological or immunohistochemical markers.
Adenocarcinomatous deposits are by far the most common cutaneous metastasis, with the breast being the most frequent source (up to 23% of cutaneous metastases, the vast majority of which occur in women).35,38,51 Lung and large intestine are also important sources of metastatic adenocarcinoma.52,53 Other primary sites include the stomach, prostate, pancreas, endometrium, thyroid gland, ovaries, and endocervix.4,35,38,54–61 Antibodies against lineage restricted transcription factors are available for many cancer types and will be discussed further below.
Metastases from carcinoma of the breast have a variety of appearances, depending to some extent on the nature of the primary tumor (Figs 30.27–30.31).62 Nodular deposits and carcinoma en cuirasse consist of a diffuse infiltrate of undifferentiated cells with hyperchromatic nuclei and minimal cytoplasm. Metastatic breast carcinoma to the eyelid is seen with some frequency, and at that site the tumor cells sometimes have a prominent histiocytoid appearance.63 Rarely, metastatic adenocarcinoma of the breast, prostate, and colon can present with epidermotropism, and confusion with primary cutaneous carcinoma or superficial spreading melanoma may ensue.43,64 Exceptionally, metastatic breast carcinoma mimics a granular cell tumor or contains melanin pigment resembling a melanoma.65–67
Usually, the metastatic tumor does not connect with the overlying epidermis. Exceptionally, however, a metastatic squamous cell carcinoma can present as an epidermotropic and/or folliculotropic metastasis, making distinction from a primary tumor very difficult. This phenomenon has been described in a metastatic laryngeal carcinoma, in a carcinoma from the lip, and in metastases from a primary cutaneous squamous cell carcinoma.43,44 High molecular weight keratins such as CK 5/6 can also be used for the diagnosis of squamous cell carcinoma, particularly in poorly differentiated tumors, but this does not allow a distinction between primary and metastatic neoplasms.28,45,46 Both p63 and p40 can also be used as markers that suggest squamous origin if characteristic morphological features are lacking.47–49
The use of CK14 has been advocated as being helpful in distinguishing between a squamous cell carcinoma and an adenocarcinoma. Squamous cell
Typical of a breast metastasis, especially the lobular type, is the presence of linear dissection of tumor cells between adjacent collagen bundles (stacked-penny or ‘single-file’ appearance) (Fig. 30.32). Similar appearances may be seen with a number of other tumors including those of the prostate, stomach, and pancreas, and small cell carcinoma. Lymphoma, sclerosing epithelioid fibrosarcoma, and primary cutaneous neuroendocrine tumor may occasionally adopt an identical pattern. There may be obvious glandular differentiation, but it is unusual for this to predominate (Fig. 30.33). Inflammatory carcinoma is characterized by a widespread infiltration of the subepidermal and deeper lymphatic channels, and, in the telangiectatic variant, vascular involvement may also be apparent68 (Figs 30.34
1531 Individual tumors
A
B
1532 Cutaneous metastases and Paget disease of the skin
and 30.35). A well-differentiated glandular architecture, with focal necrosis, is more typical of a primary tumor in the large intestine or rectum (Figs 30.36–30.39). In anaplastic variants, the features of the tumor cells may be indistinguishable from those of a high-grade lymphoma. Immunohistochemical techniques are often necessary to establish the correct diagnosis. Some CD30-positive anaplastic large cell lymphomas fail to express leukocyte common antigen (CD45). It is important to include a range of antibodies to both B- and T-cell antigens before excluding the diagnosis of disseminated lymphoma. It must also be remembered that nodal CD30-positive anaplastic large cell lymphoma not uncommonly expresses epithelial membrane antigen (EMA), which may therefore be a diagnostic pitfall for the unwary.
Metastatic tumors with a papillary growth pattern may reflect a number of different sites, including the colon, ovary, thyroid gland, stomach, and even the lung (Figs 30.40 and 30.41).58–60 Certain distinguishing features sometimes permit differentiation between various papillary metastases. Concentrically laminated calcified psammomatous bodies may be conspicuous in both serous (ovarian) carcinoma and thyroid papillary carcinoma. The latter, however, may be further identified by colloid production, nuclear grooving, and characteristic ‘Orphan Annie’ nuclei.35 Intranuclear cytoplasmic pseudoinclusions are also sometimes a feature. The immunohistochemical demonstration of thyroglobulin production is confirmatory. Cutaneous metastasis of papillary thyroid carcinoma with prominent clear cell change
may mimic a primary adnexal tumor such as a clear cell hidradenocarcinoma. A percentage of cases of metastatic papillary thyroid carcinoma show BRAF (V600E) mutations detectable by immunohistochemistry using the VE1 antibody or other molecular methods, a feature that is absent in follicular carcinoma of the thyroid and in hidradenocarcinoma, allowing distinction in difficult cases.69,70
Perhaps one of the most challenging differential diagnoses lies between metastatic adenocarcinoma and a primary cutaneous adnexal carcinoma showing well-developed ductal differentiation. Eccrine carcinomas, including microcystic adnexal carcinoma and hidradenocarcinoma in particular, can commonly mimic adenocarcinoma metastatic to the skin from a variety of primary sites, most commonly breast, lung, gastrointestinal tract, or ovary. Eccrine adenoma can also enter the differential diagnosis in such cases because of the duct formation, but the absence of an infiltrative growth
1533 Individual tumors
A
B
1534 Cutaneous metastases and Paget disease of the skin
pattern and cytological atypia will generally distinguish this entity from a cutaneous adenocarcinomatous visceral metastasis. Distinction between these entities, particularly eccrine ductal carcinoma, can be very difficult based on histology alone; immunohistochemistry is sometimes very useful.
It has been suggested that p63 can be used as a marker to distinguish primary adnexal tumors from metastatic adenocarcinoma in the skin: p63 is generally expressed in cutaneous adnexal tumors and is lacking in metastatic adenocarcinomas (breast, gastrointestinal tract, lung).21,71 It is important to note, however, that p63 immunohistochemical staining cannot be used to distinguish between primary and metastatic squamous cell carcinomas (whether of lung or head and neck origin) or metastatic urothelial carcinomas since it can be routinely identified in the normal basal cells of skin and other stratified epithelia, as well as in prostatic and respiratory epithelium.72,73 p63 is also a marker for myoepithelial cells of the breast.67 Recently, p40 has been suggested as having better specificity for distinguishing primary skin adnexal tumors from cutaneous metastases, but has similar caveats and drawbacks to those discussed above for p63.74
These observations have also been supported by other studies. Qureshi and coworkers studied 15 metastatic carcinomas to the skin including 14 adenocarcinomas and 1 urothelial carcinoma.21 Only one of the adenocarcinomas displayed partial p63 expression, and this was a poorly differentiated esophageal carcinoma. Sariya and coworkers found that when used as a single marker, a positive p63 stain had the highest sensitivity (96%) for primary adnexal tumors and a negative p63 stain had the highest positive predictive value for a metastasis.75 Kanitakis and coworkers also reported that the large majority (88.5%) of primary skin tumors express p63 while 89% of the metastatic tumors to skin are p63-negative.76 Ivan and coworkers have also demonstrated that strong p63 expression is retained in those rare cases of metastatic sweat gland carcinoma to other skin sites and lymph nodes.77 The use of p63 in a panel of immunohistochemical studies may therefore be of value in the differential diagnosis of metastatic adenocarcinoma to skin from primary cutaneous tumors showing ductal differentiation. Although additional studies are needed, p40 may show superior specificity over p63 in distinguishing primary and metastatic tumors.74
Another immunohistochemical marker that has been reported as useful in the differential diagnosis of cutaneous metastases from primary cutaneous adnexal neoplasms is CK5/6, which is expressed in the majority of primary cutaneous adnexal neoplasms, but only rarely in cutaneous metastases of internal adenocarcinoma.46 A further marker, podoplanin (D2-40), has also been reported as positive in primary adnexal tumors and not in metastatic tumors of various origin (lung, breast, gastrointestinal, or genitourinary tracts).78 A subsequent study suggests pairing p63 with D2-40 (podoplanin) to increase the specificity in this setting.79 Calretinin, a calcium-binding protein expressed in mesothelial, epithelial, and stromal cells, has been found to be positive in metastatic tumors but also in some cases of primary cutaneous neoplasms.75
A
Appropriate assessment of the histologic features in combination with a complete clinical history and utilization of a carefully selected immunohistochemical panel should help resolve the majority of diagnostic problems. However, it must be emphasized that a diagnosis should never be based solely on immunohistochemical findings.
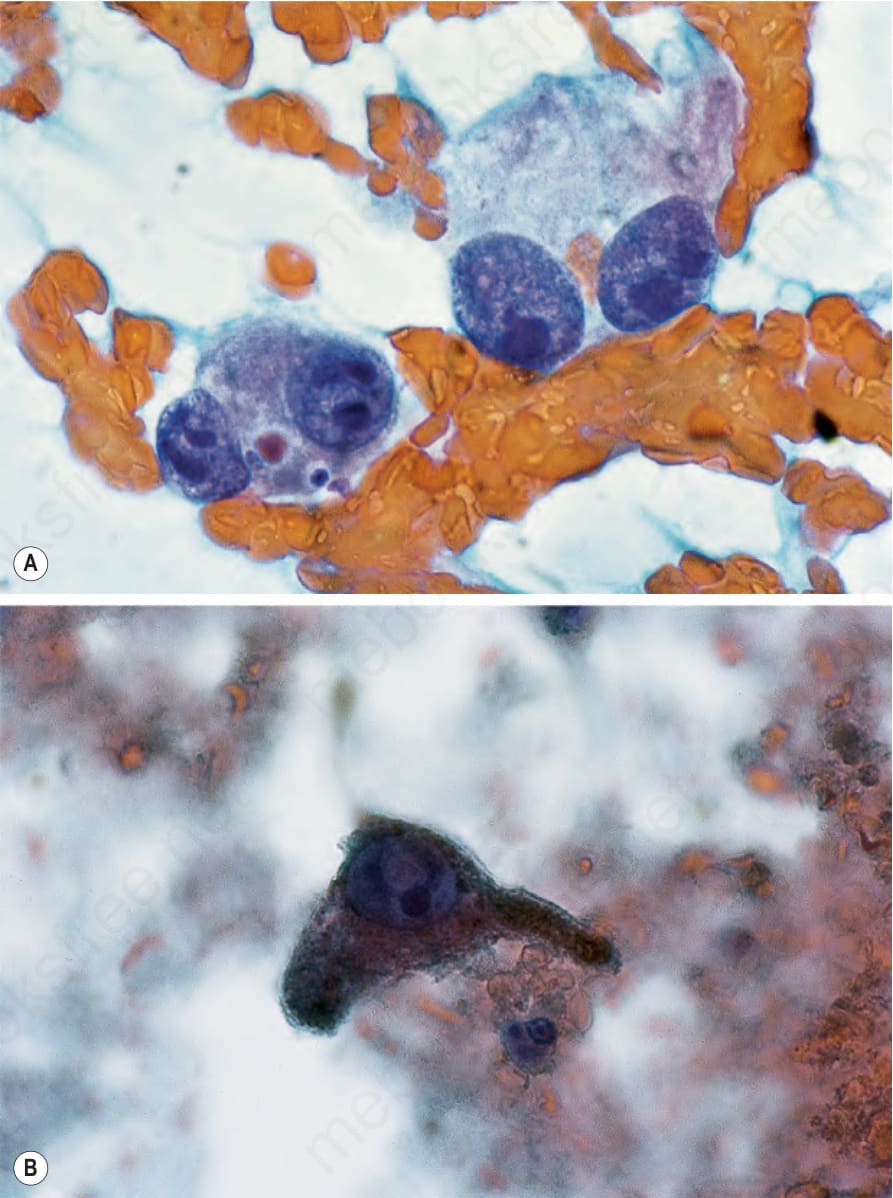
Fig. 30.26 Fine needle aspirate: this is an example of metastatic malignant melanoma. Note (A) the large nucleoli and (B) the intracytoplasmic pigment. By courtesy of G.T. McKee, MD, Massachusetts General Hospital, Boston, USA.
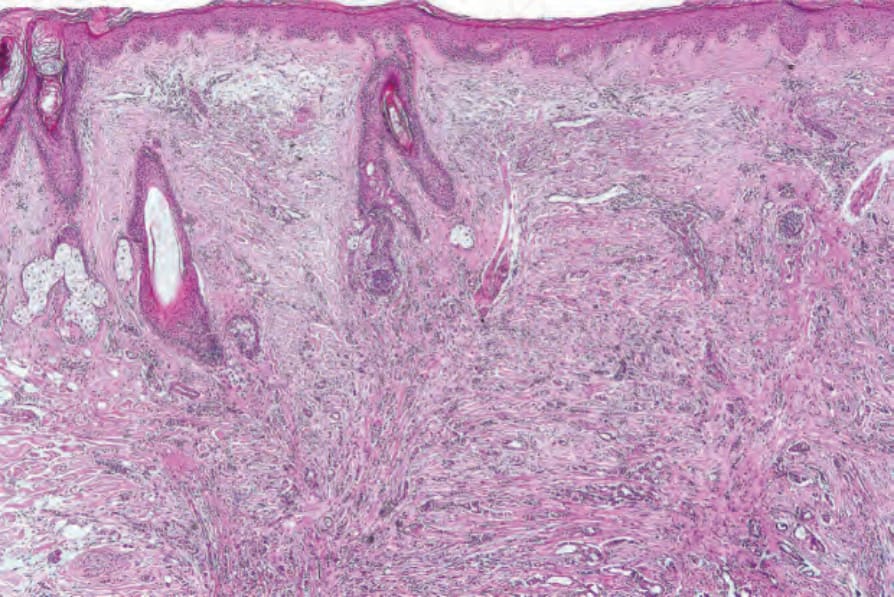
Fig. 30.27 Metastatic carcinoma of breast (alopecia neoplastica): scalp biopsy from a middleaged female shows extensive infiltration of the dermis by tumor, resulting in loss of pilosebaceous structures.
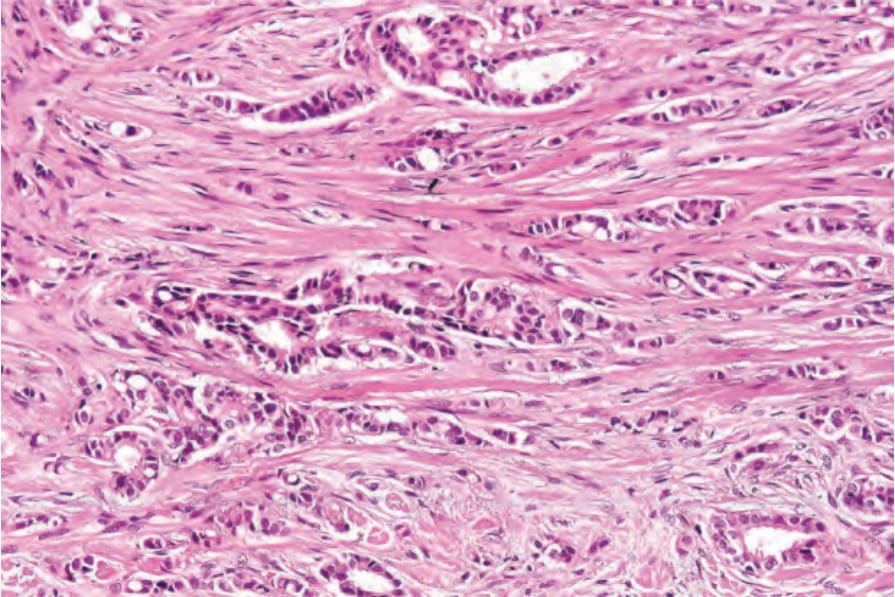
Fig. 30.28 Metastatic carcinoma of breast (alopecia neoplastica): the tumor infiltrate is composed of cords of tumor cells dispersed in a dense fibrous stroma. Note the glandular differentiation.
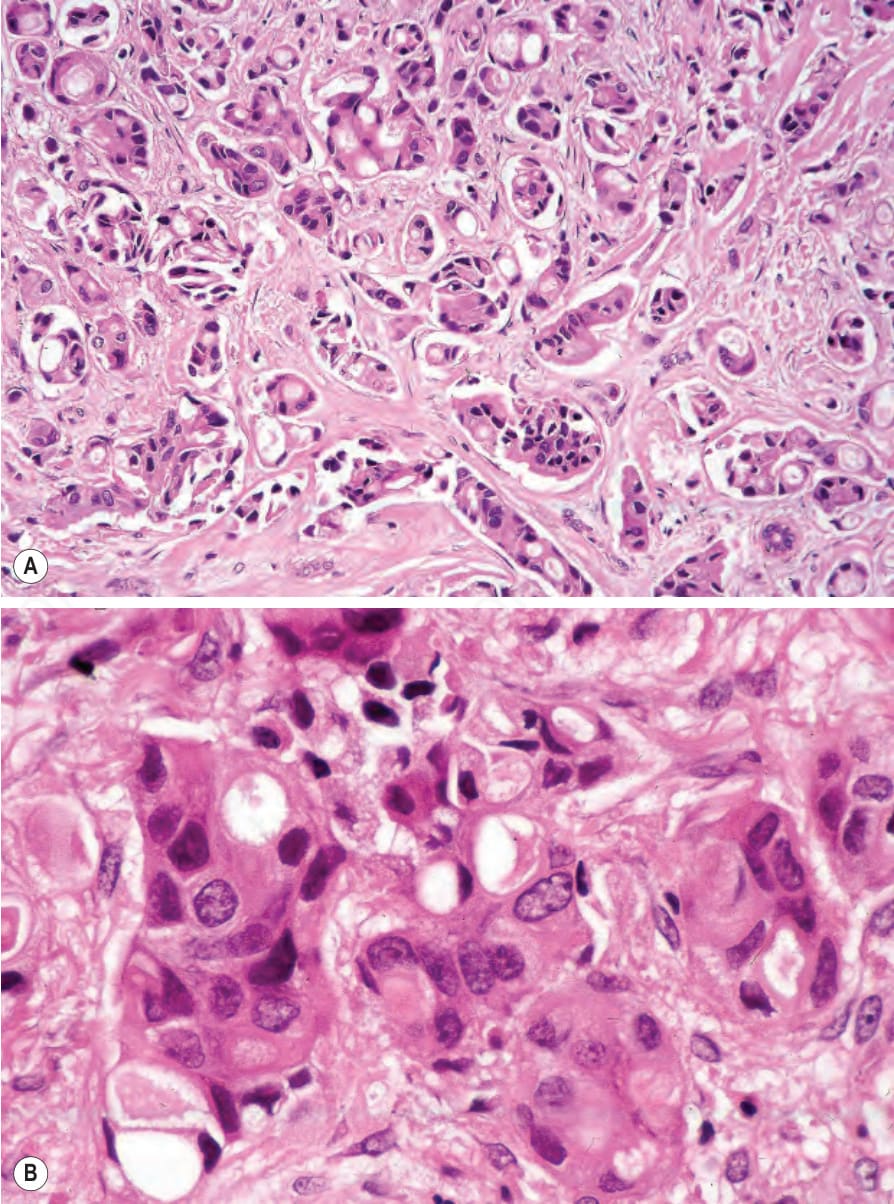
Fig. 30.29 Metastatic carcinoma of the breast (alopecia neoplastica): (A) this example is much more high grade. Note the pleomorphism; (B) intracytoplasmic lumina are present.
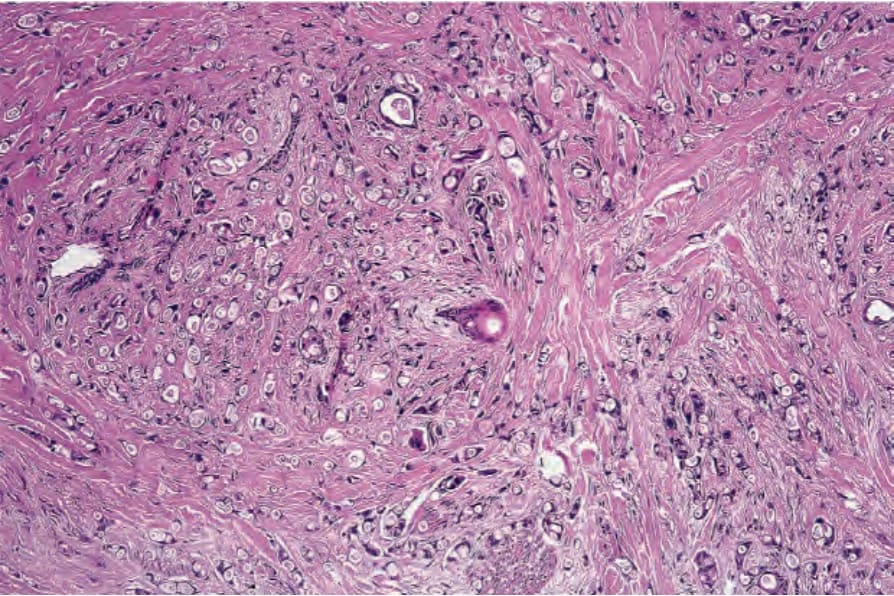
Fig. 30.30 Sclerodermatous metastatic carcinoma of breast: the cells are dispersed in a very dense fibrous stroma.
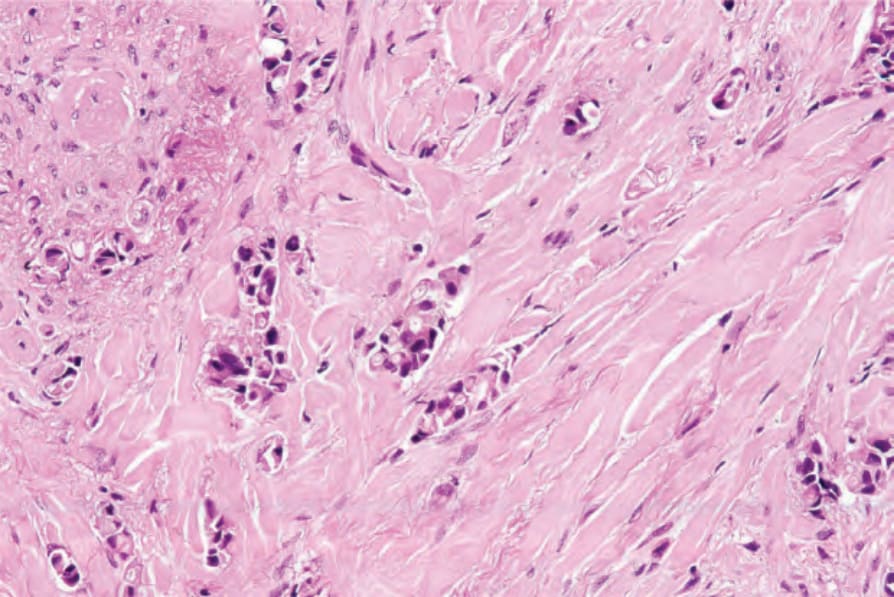
Fig. 30.31 Sclerodermatous metastatic carcinoma of the breast: higher-power view.
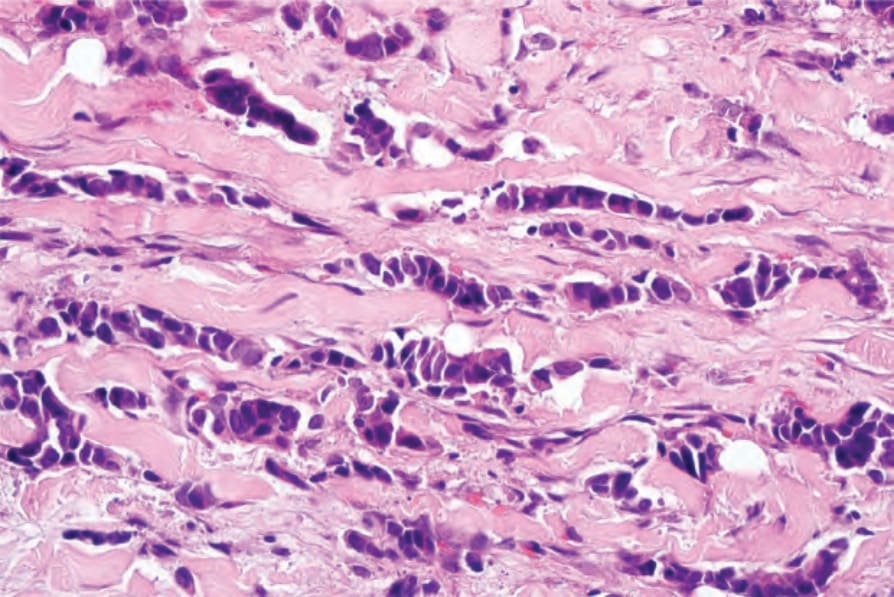
Fig. 30.32 Metastatic carcinoma of breast: the characteristic stacked-penny appearance is well demonstrated in this field. By courtesy of J. Cohen, MD, Dermatopathology Laboratory, Tucson, USA.
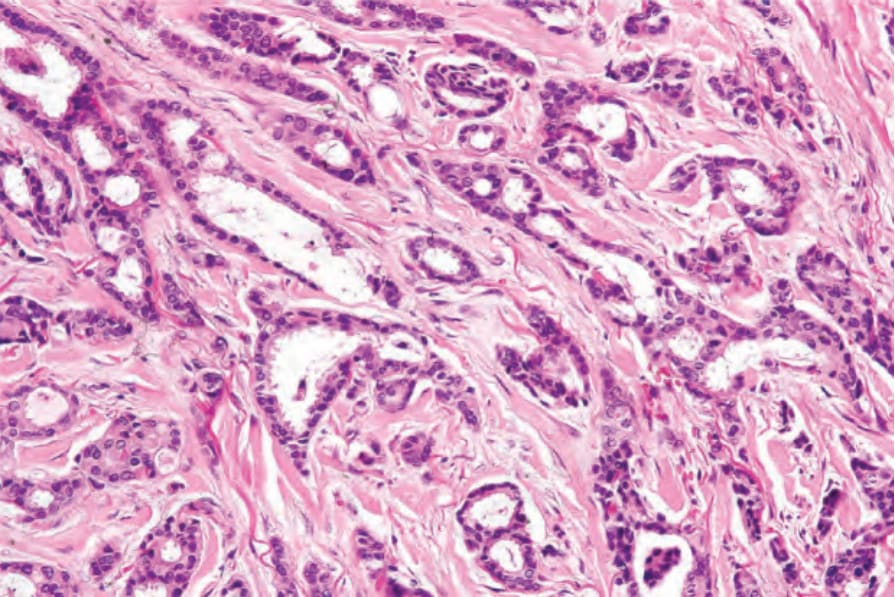
Fig. 30.33 Metastatic carcinoma of breast: in this example, there are well-developed ducts.
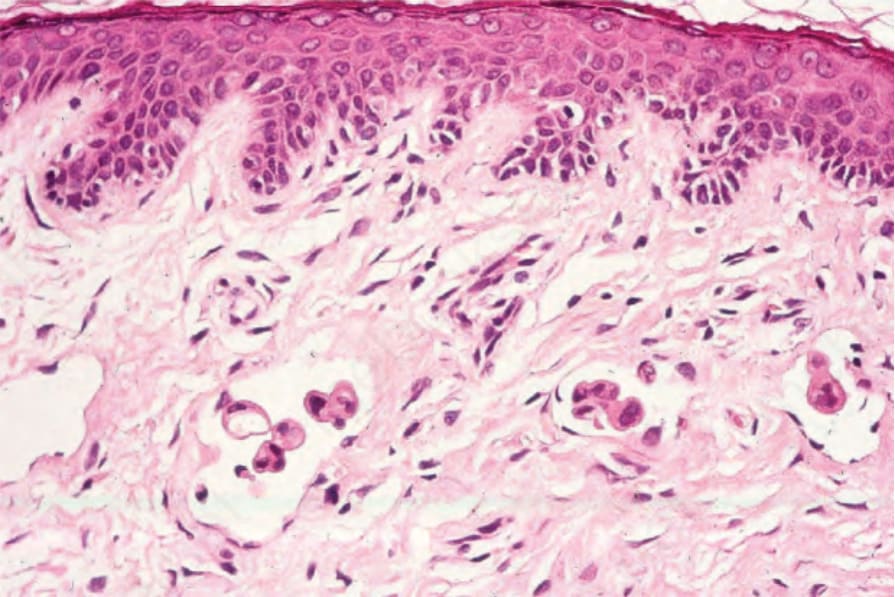
Fig. 30.34 Inflammatory carcinoma: there is involvement of the superficial dermal lymphatics.
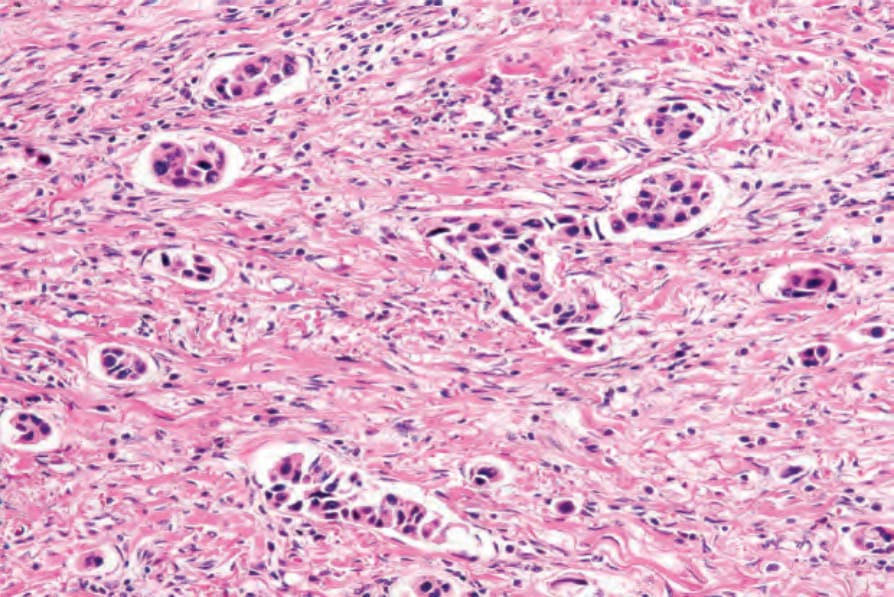
Fig. 30.35 Inflammatory carcinoma: in this example, innumerable vessels were affected.
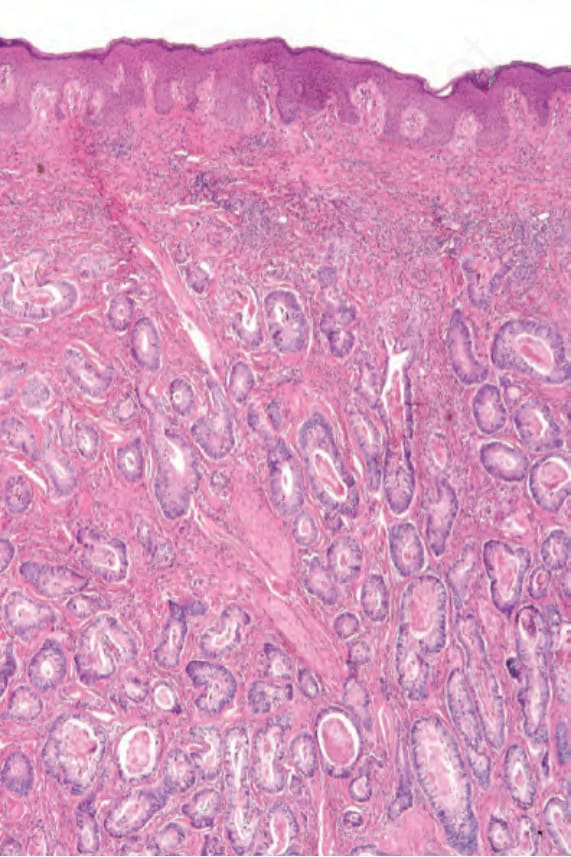
Fig. 30.36 Metastatic colonic adenocarcinoma: there is widespread infiltration of the dermis. Note the well-formed ductal structures.
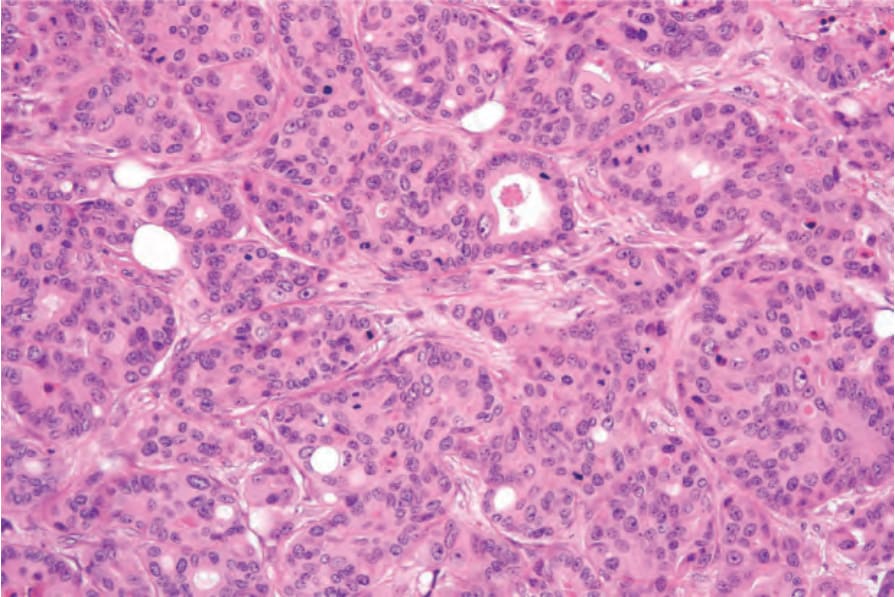
Fig. 30.37 Metastatic colonic adenocarcinoma: high-power view.
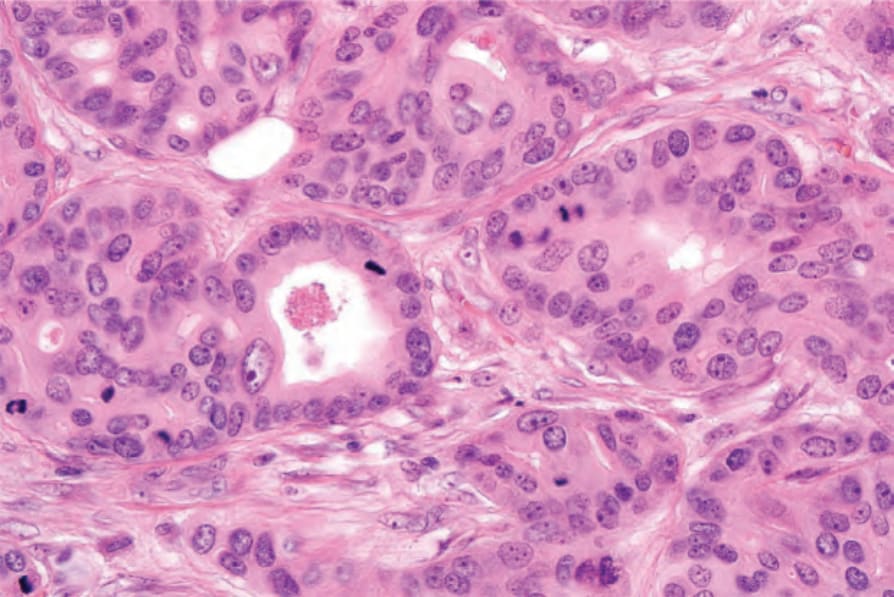
Fig. 30.38 Metastatic colonic adenocarcinoma: there is conspicuous mitotic activity.
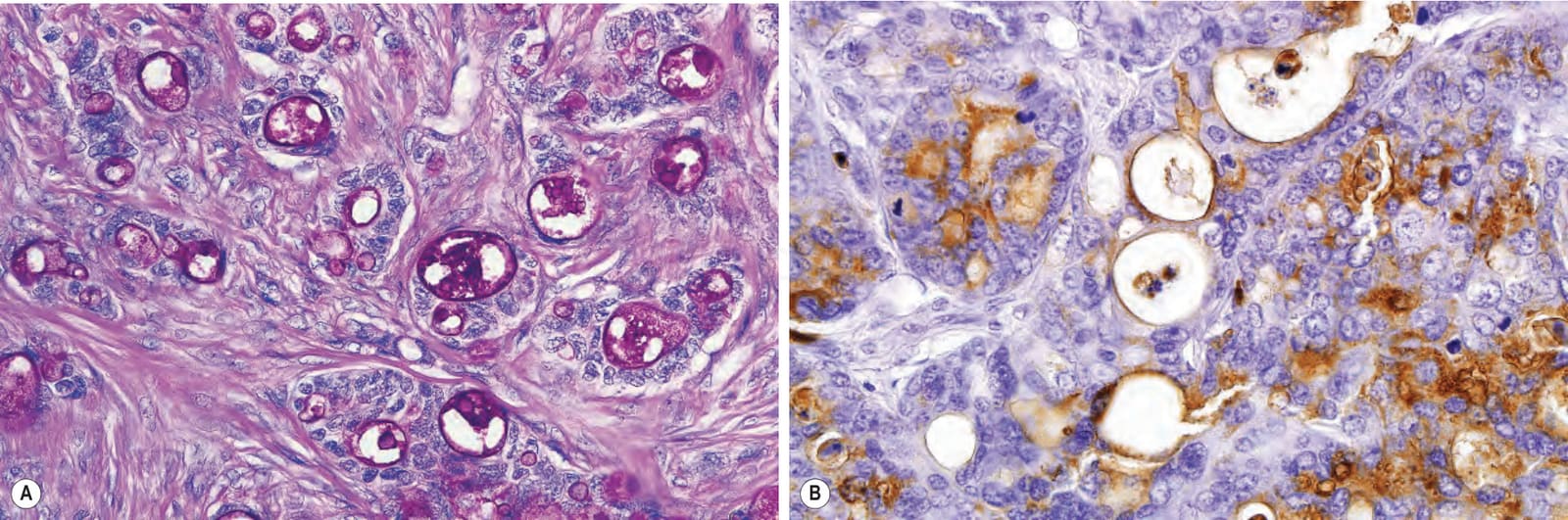
Fig. 30.39 Metastatic colonic adenocarcinoma: (A) the tumor is strongly PAS positive, diastase resistant; (B) the epithelial lining is outlined by carcinoembryonic antigen.
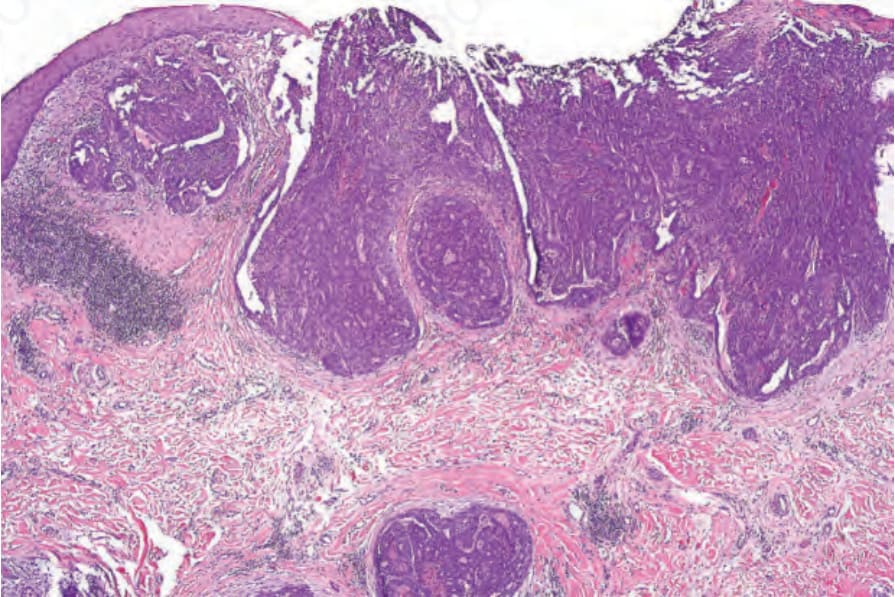
Fig. 30.40 Metastatic thyroid papillary carcinoma: an ulcerated, multifocal carcinoma with a papillary configuration is present in the superficial and deep dermis.
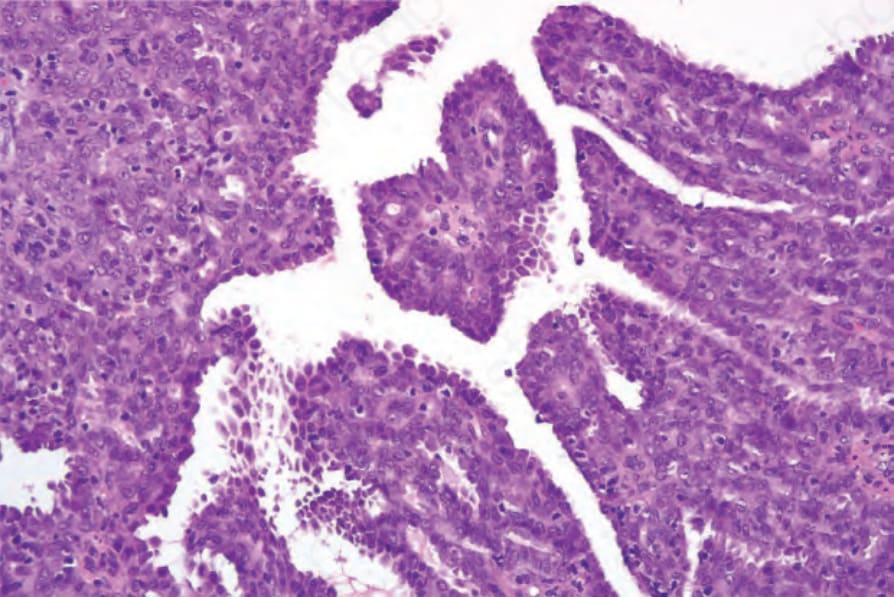
Fig. 30.41 Metastatic thyroid papillary carcinoma: the papillae are covered with tall columnar epithelial cells.
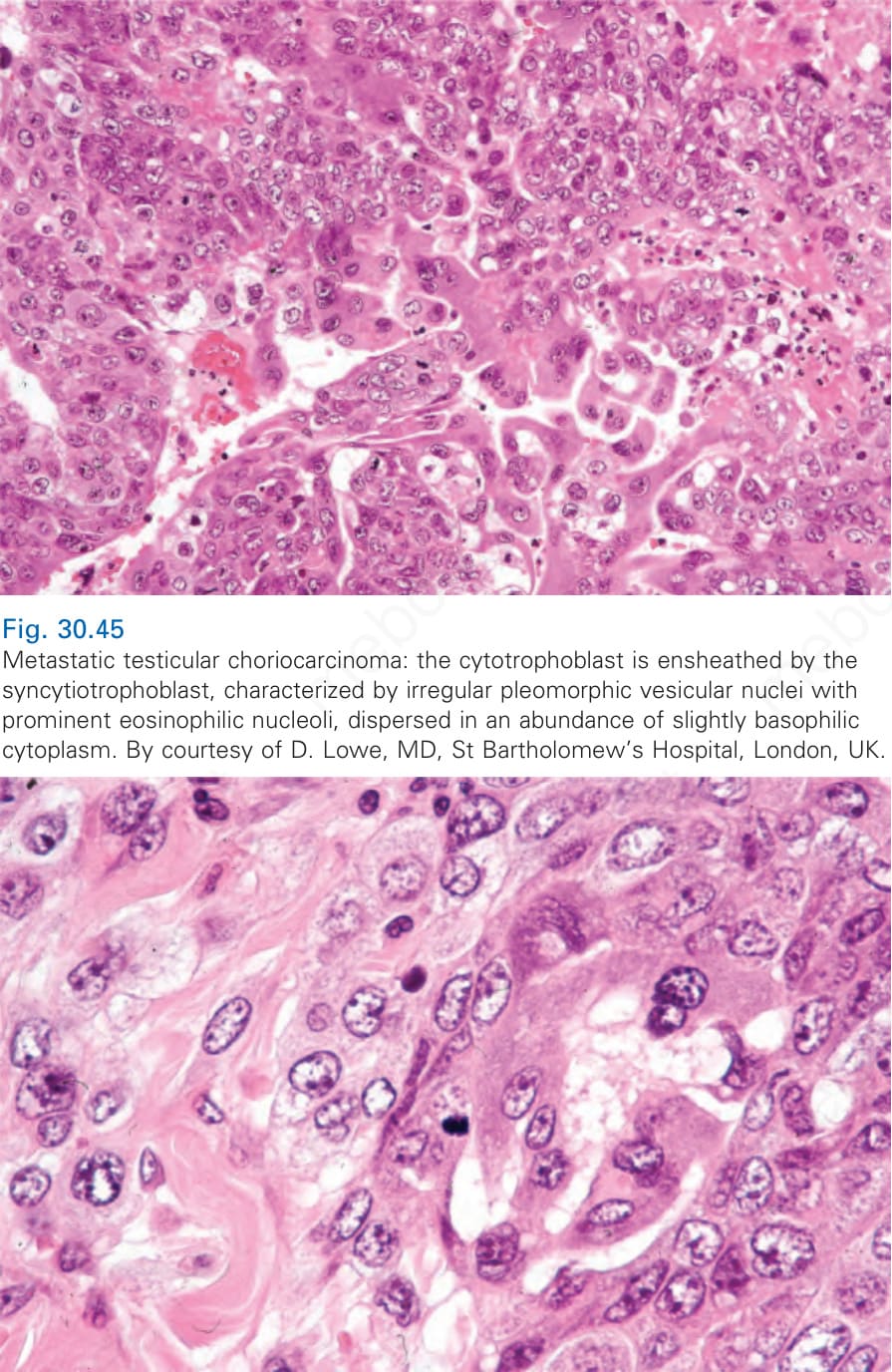
Fig. 30.45 Metastatic testicular choriocarcinoma: the cytotrophoblast is ensheathed by the syncytiotrophoblast, characterized by irregular pleomorphic vesicular nuclei with prominent eosinophilic nucleoli, dispersed in an abundance of slightly basophilic cytoplasm. By courtesy of D. Lowe, MD, St Bartholomew’s Hospital, London, UK.
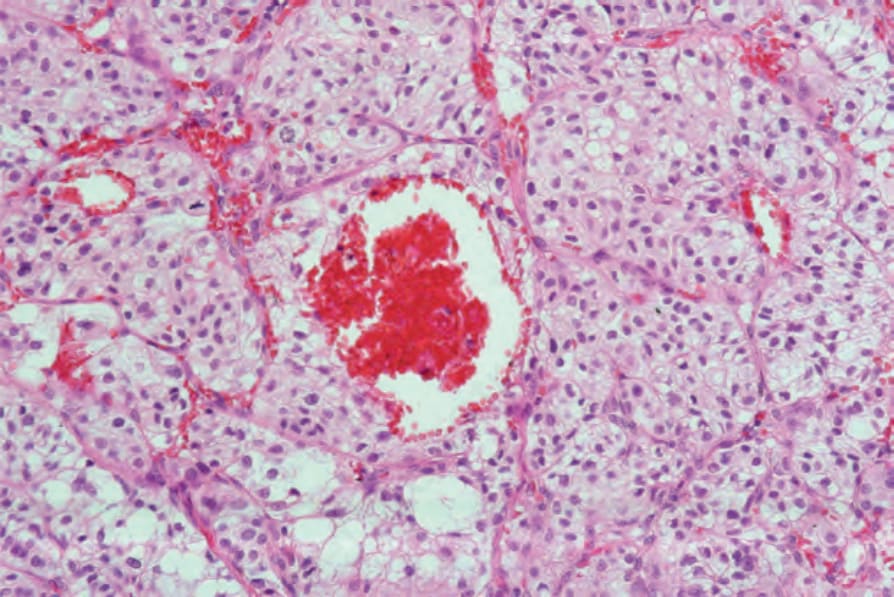
Fig. 30.49 Metastatic renal (clear cell) carcinoma: note the clear cells and characteristic hemorrhage.
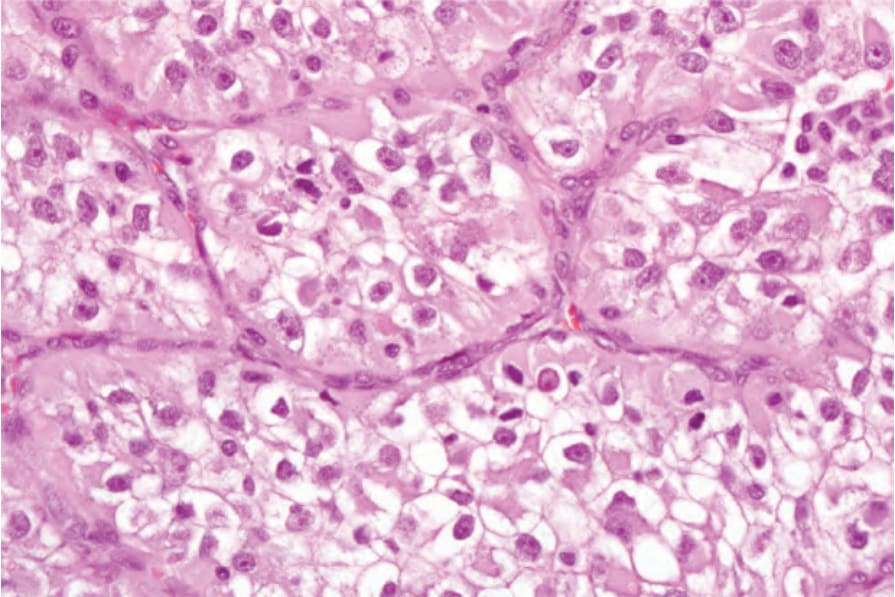
Fig. 30.50 Metastatic renal (clear cell) carcinoma: the clear cell appearance is due to the accumulation of glycogen and lipid.
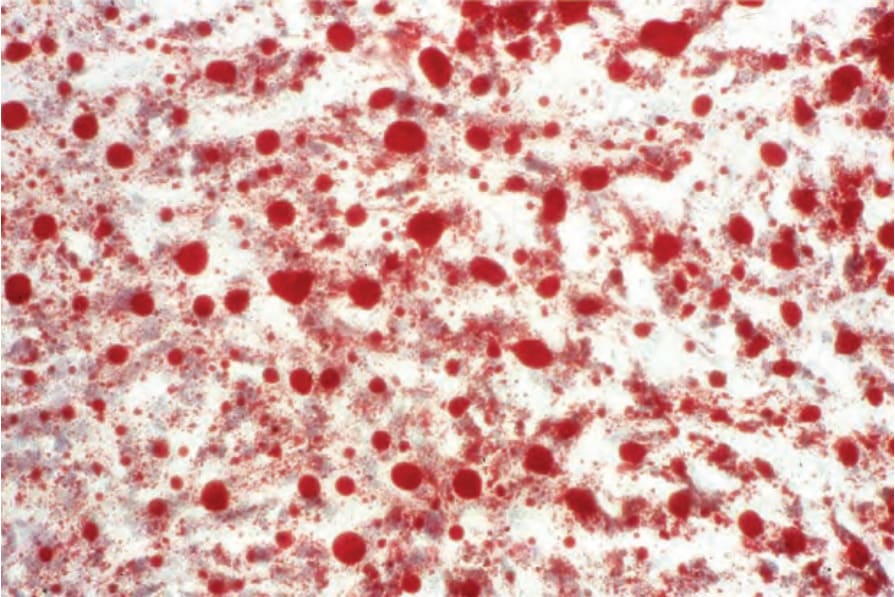
Fig. 30.51 Metastatic renal (clear cell) carcinoma: oil red O staining for lipid is strongly positive.
B
Mucinous carcinoma Mucinous carcinoma is characterized by compartments created by fibrous strands, which contain pools of mucin and floating nests of tumor cells. These usually have ample cytoplasm, centrally placed vesicular nuclei, and only mild cytological atypia. Although mucinous carcinoma may sometimes arise as a primary tumor in the skin (most commonly as a slow-growing nodule on the head or neck of older men), on occasions it represents metastatic spread from sites such as the breast, stomach, colon, rectum, and pancreas (Fig. 30.42).80–82
Distinction between a primary and a metastatic tumor is usually not possible on histologic grounds alone, although in a large case series, Kazakov and coworkers reported that the presence of an in situ component is particularly helpful in the diagnosis of primary cutaneous neoplasms. However, the absence of such a component does not exclude the diagnosis.81,83 Dirty necrosis has been reported as a constant histologic finding in metastatic
adenocarcinoma of intestinal origin.81 Mucinous carcinoma found in the skin of the trunk usually represents metastatic disease from internal primary tumors.81
‘Signet ring’ metastases, in which intracellular mucin accumulation results in compression of the nucleus to the cell periphery, may be seen with gastric, large intestinal, and pancreatic primary tumors (Fig. 30.43). Rarely, they may also arise in the endocervix and gallbladder. Signet ring cell change may be seen in a number of cutaneous tumors including sweat gland carcinoma, melanoma, squamous cell carcinoma, and basal cell carcinoma.
Of historical interest, the type of mucin can help distinguish between primary cutaneous mucinous carcinoma and cutaneous metastases of a gastrointestinal primary. In primary cutaneous mucinous carcinoma, the mucin contains abundant sialomucin, and is therefore Alcian blue positive at pH 2.5, but not at pH 1.0 or 0.4.84 The mucin seen in gastrointestinal mucinous carcinomas that metastasize to the skin contains sulfamucins, which
1535 Individual tumors
A
B
seen with the t(6;9)(q2223;p2324) resulting in MYB-NFIB fusions present in salivary adenoid cystic carcinomas.99
Choriocarcinoma Choriocarcinoma, although usually a gestational tumor, may also be derived from the testis and, more rarely, the mediastinum, ovary, and, exceptionally, a placental site trophoblastic tumor.100 Associated with a marked propensity for vascular invasion, cutaneous metastases are not uncommon.100–105 The tumor is characteristically hemorrhagic and necrotic; frequently, viable tissue is only recognizable at the periphery.
are Alcian blue positive at a pH of 1.0 and 0.4.85 However, these stains are not commonly performed at variable pH levels in most laboratories.
Gastrointestinal mucinous tumors metastatic to the skin generally retain CK20 expression, which is not seen in primary cutaneous mucinous sweat gland carcinoma.81,86,87 Strong CDX2 expression has been well documented in gastrointestinal metastases to other visceral organs, and has been observed in isolated cases of mucinous cutaneous metastases of intestinal origin.88,89 SATB2 has similar sensitivity (80–90%) for metastatic tumors of gastrointestinal origin and may have increased or complementary specificity with CDX2.90,91 GATA3 has been reported in primary cutaneous mucinous carcinoma and thus cannot be used to favor breast origin.92 If an in situ component of cutaneous mucinous adenocarcinoma is identified, the surrounding myoepithelial cells may label for p63, CK5/6, calponin, or smooth muscle actine (SMA).76,77,81,83 Metastatic mucinous carcinomas are usually negative for p63.77
Choriocarcinoma is a tumor of trophoblastic tissue: the cytotrophoblast, the proliferative component, and the syncytiotrophoblast, the hormonally active element. The lesion is composed of a variable admixture of these two cell types, and no chorionic villi are found (Figs 30.44 and 30.45). The cytotrophoblast consists of regular polyhedral cells, arranged in sheets and cords, each with pale cytoplasm and a fairly large vesicular nucleus, often with a prominent nucleolus. Mitotic figures may be conspicuous and are frequently abnormal. In contrast, the syncytiotrophoblast is composed of very large pleomorphic cells with abundant, somewhat basophilic, cytoplasm. They are frequently multinucleate and are often seen in intimate association with the neighboring cytotrophoblast (Fig. 30.46). Immunohistochemical demonstration of gonadotrophin is a useful diagnostic aid (Fig. 30.47). Choriocarcinoma components from testicular mixed tumors as well as postpartum cases can metastasize to skin.106–109
Adenoid cystic carcinoma Primary cutaneous adenoid cystic carcinoma is rare and therefore must be distinguished from metastatic disease. Sources of a systemic primary tumor include salivary gland, lacrimal gland, cervix, bronchus, or breast.93,94 In clinical practice, however, these visceral tumors are usually slowly-growing lesions in which cutaneous presentation would be most unlikely, although isolated cases of such have been described.95,96 The majority of adenoid cystic carcinomas in the skin therefore represent primary neoplasms. Metastatic lesions most often arise from the salivary gland.97,98 A subset of primary cutaneous adenoid cystic carcinomas can harbor MYB rearrangements as
Clear cell carcinoma Metastatic clear cell carcinoma is typically derived from the kidney, but other sources include the lungs, liver, and the mesonephric clear cell carcinomas of the ovaries, endometrium, cervix, and vagina.110–112 The tumor is composed of cords, alveoli, and, occasionally, tubular structures consisting of uniform clear cells containing both lipid and glycogen (Figs 30.48–30.51). The stroma is usually delicate and highly vascular, often resulting in conspicuous areas of hemorrhage and therefore accounting for the characteristic clinical appearance of such a metastasis. It must be histologically differentiated from clear cell squamous carcinoma, clear cell hidradenocarcinoma, clear
1536 Cutaneous metastases and Paget disease of the skin
cell porocarcinoma, trichilemmal carcinoma, sebaceous carcinoma, amelanotic clear cell melanoma, PEComa, and clear cell sarcoma (melanoma of soft parts).
Immunohistochemical studies can be used as an adjuvant in the differential diagnosis, but they are not very specific. Primary renal cell carcinoma has been shown to express CD10 (common acute lymphoblastic leukemia antigen [CALLA]) and also in cutaneous metastatic disease.113–116 The renal cell carcinoma marker (RCC-Ma) has a high specificity and moderate sensitivity for cutaneous metastases of renal cell carcinoma.117 As such, a positive result with RCC-Ma is highly suggestive of a diagnosis of metastatic renal cell carcinoma; however, a negative result does not exclude the diagnosis.118 PAX8 is a lineage-specific transcription factor that is positive in kidney tumors, but also in ovary and thyroid, so use in panels with careful consideration of the differential diagnosis is needed.28,119,120
1537 Individual tumors
A
Neuroendocrine carcinoma (small cell carcinoma) Metastatic neuroendocrine carcinoma is recognized by its distinctive features of small, hyperchromatic, and round to oval nuclei with barely perceptible cytoplasm (Fig. 30.52). Typical of the tumor is the presence of abundant basophilic nuclear debris around its vasculature.
B
Tumors from which bronchial neuroendocrine carcinoma must be differentiated include neuroendocrine tumors arising elsewhere (e.g., from skin, gastrointestinal tract, and uterus), medullary carcinoma of the thyroid, small cell melanoma, and poorly fixed specimens of lymphoma.121,122 Immunohistochemically, these tumors express a range of antigens including low molecular weight keratin (CAM 5.2), EMA, neuron-specific enolase, chromogranin, synaptophysin, CD56, PGP 9.5, and bombesin. Medullary carcinoma of the thyroid expresses calcitonin. Neuroendocrine carcinoma of the salivary gland and cutaneous tumors consistently show perinuclear dotlike positivity for CK20, and this is useful in their differential diagnosis from other metastatic neuroendocrine carcinomas.5,6 Both Merkel cell carcinoma and non-Merkel cell primary cutaneous neuroendocrine carcinomas should also receive diagnostic consideration.123–127 Some recent data suggest that determining the site of origin of neuroendocrine carcinomas could be of utmost importance.128 Although for many metastases clinical correlation
often provides the answer, immunohistochemistry is often an important aid in reaching a diagnosis. More recently with advances in molecular diagnostics, it has been suggested that the use of a 92-gene cancer classifier is also a very useful way to predict the site of origin of neuroendocrine tumors.129
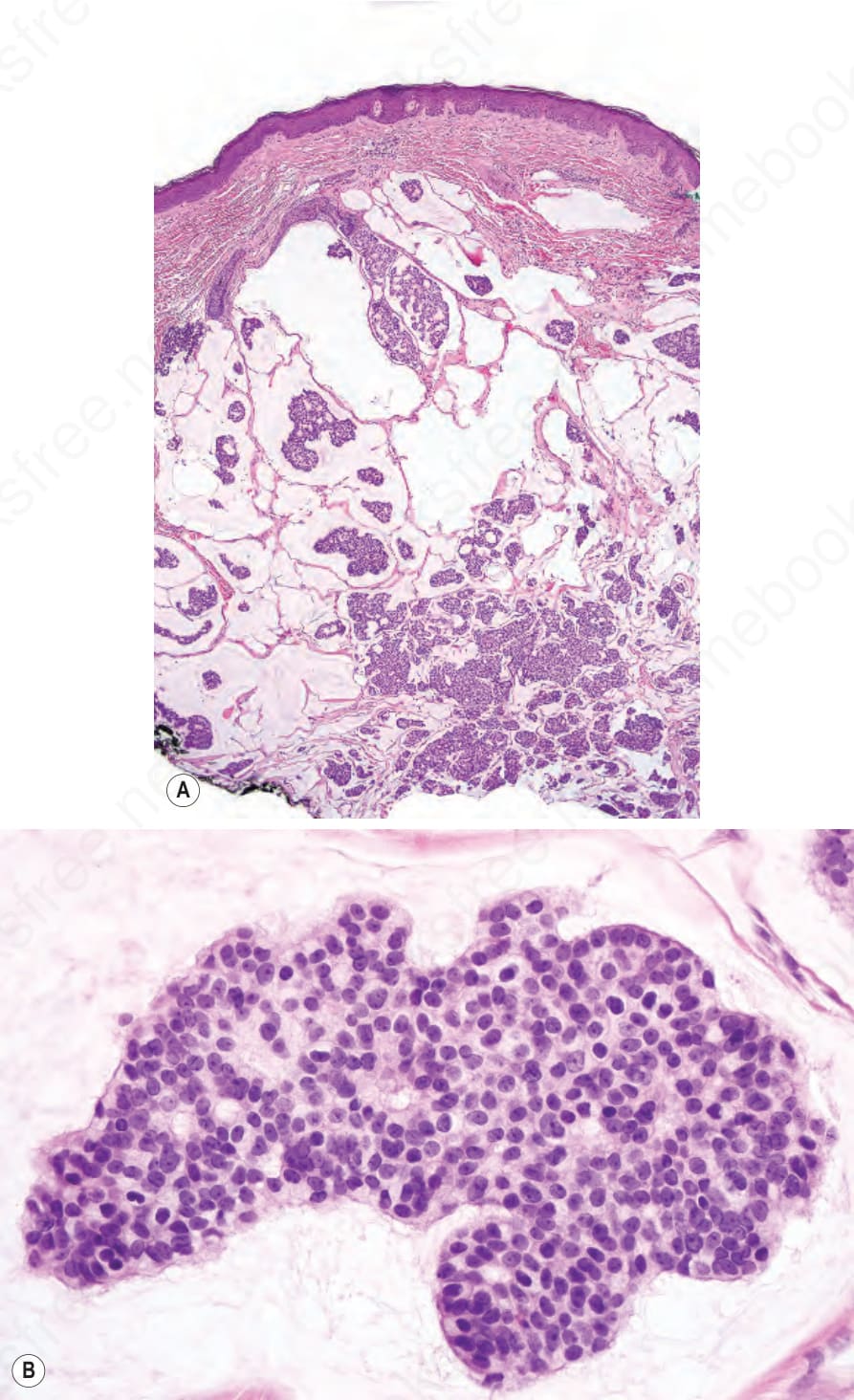
Fig. 30.42 Metastatic mucinous carcinoma: (A) low-power view of a deposit of metastatic mucinous carcinoma; (B) high-power view. Primary and metastatic diseases are histologically indistinguishable unless an in situ component is identified in the former.
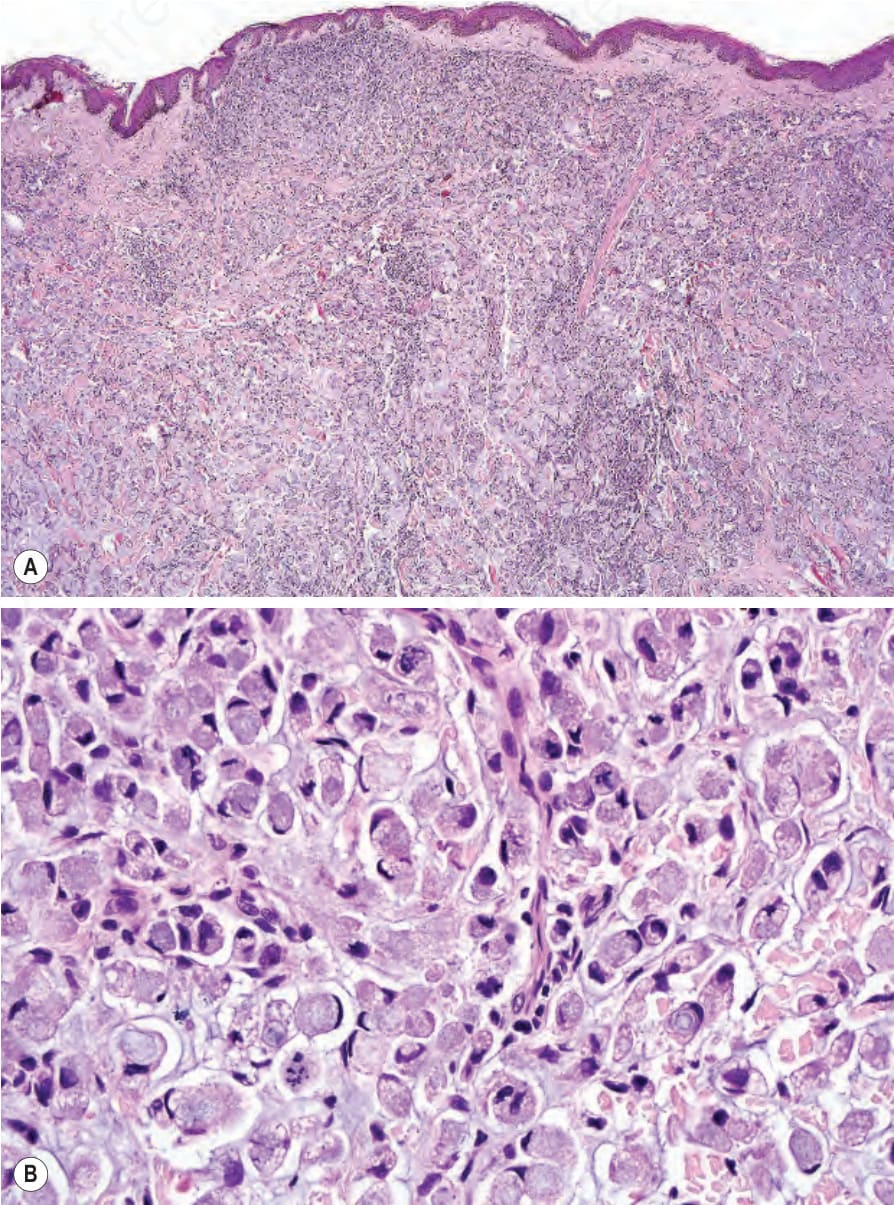
Fig. 30.43 Metastatic signet-ring cell carcinoma: (A, B) the dermis is completely replaced by a pure population of signet ring cells.
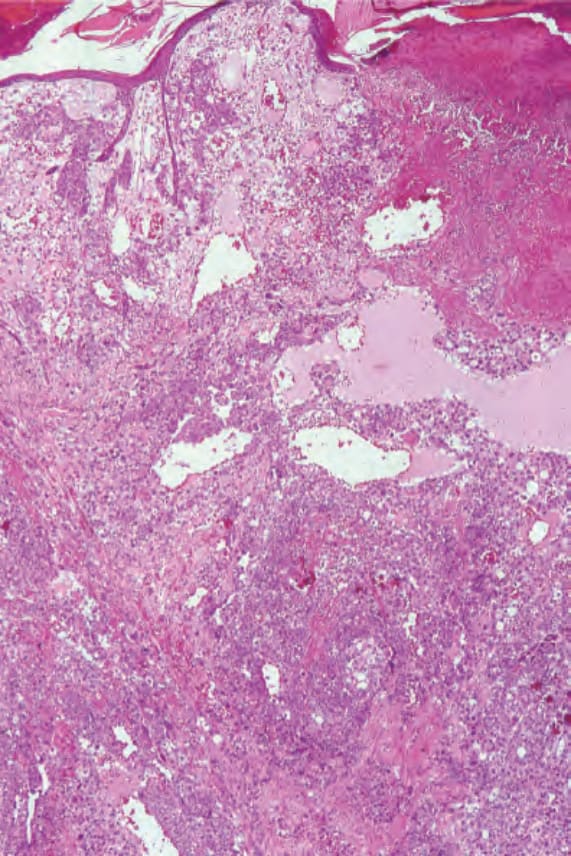
Fig. 30.44 Metastatic testicular choriocarcinoma: low-power view showing a hemorrhagic tumor filling the dermis. By courtesy of D. Lowe, MD, St Bartholomew’s Hospital, London, UK.
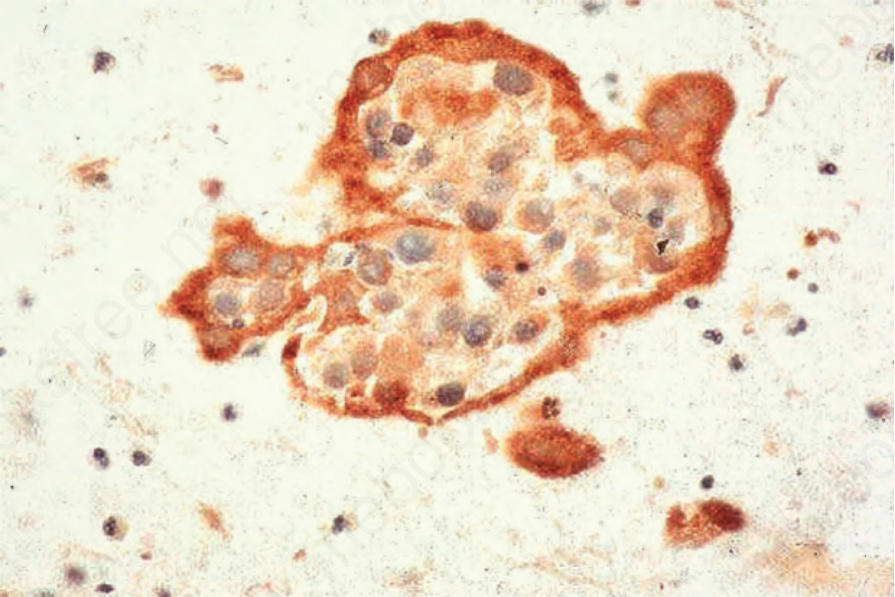
Fig. 30.46 Metastatic testicular choriocarcinoma: high-power view. By courtesy of D. Lowe, MD, St Bartholomew’s Hospital, London, UK.
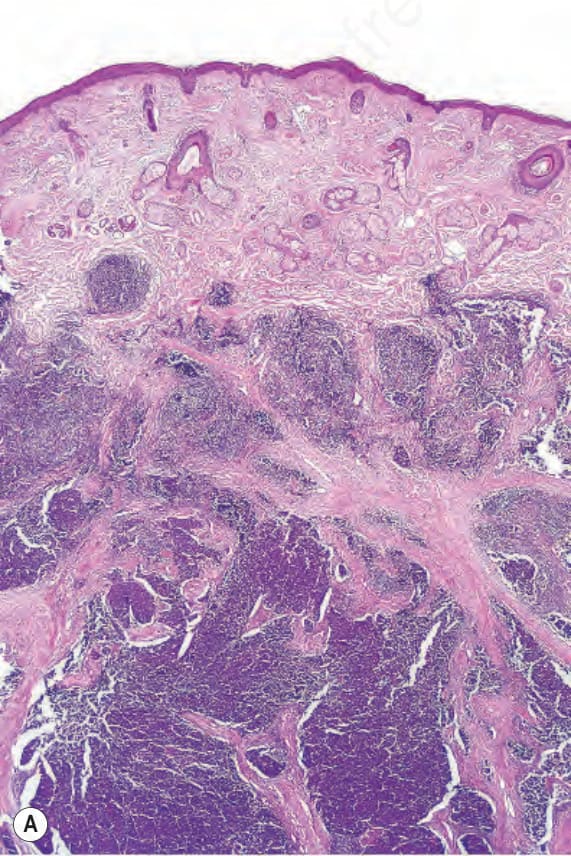
Fig. 30.47 Metastatic testicular choriocarcinoma: there is strong labeling for human chorionic gonadotrophin (fine needle aspiration).
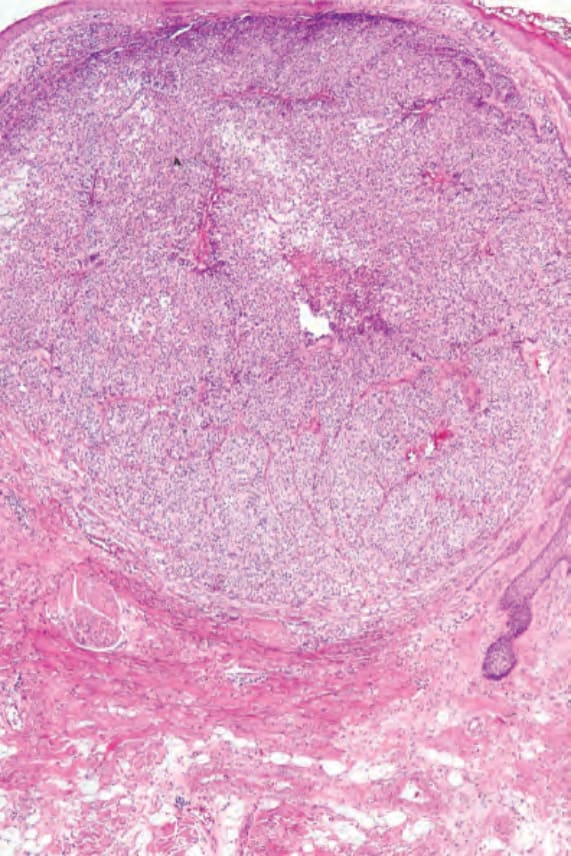
Fig. 30.48 Metastatic renal (clear cell) carcinoma: there is a well-circumscribed tumor nodule in the dermis.
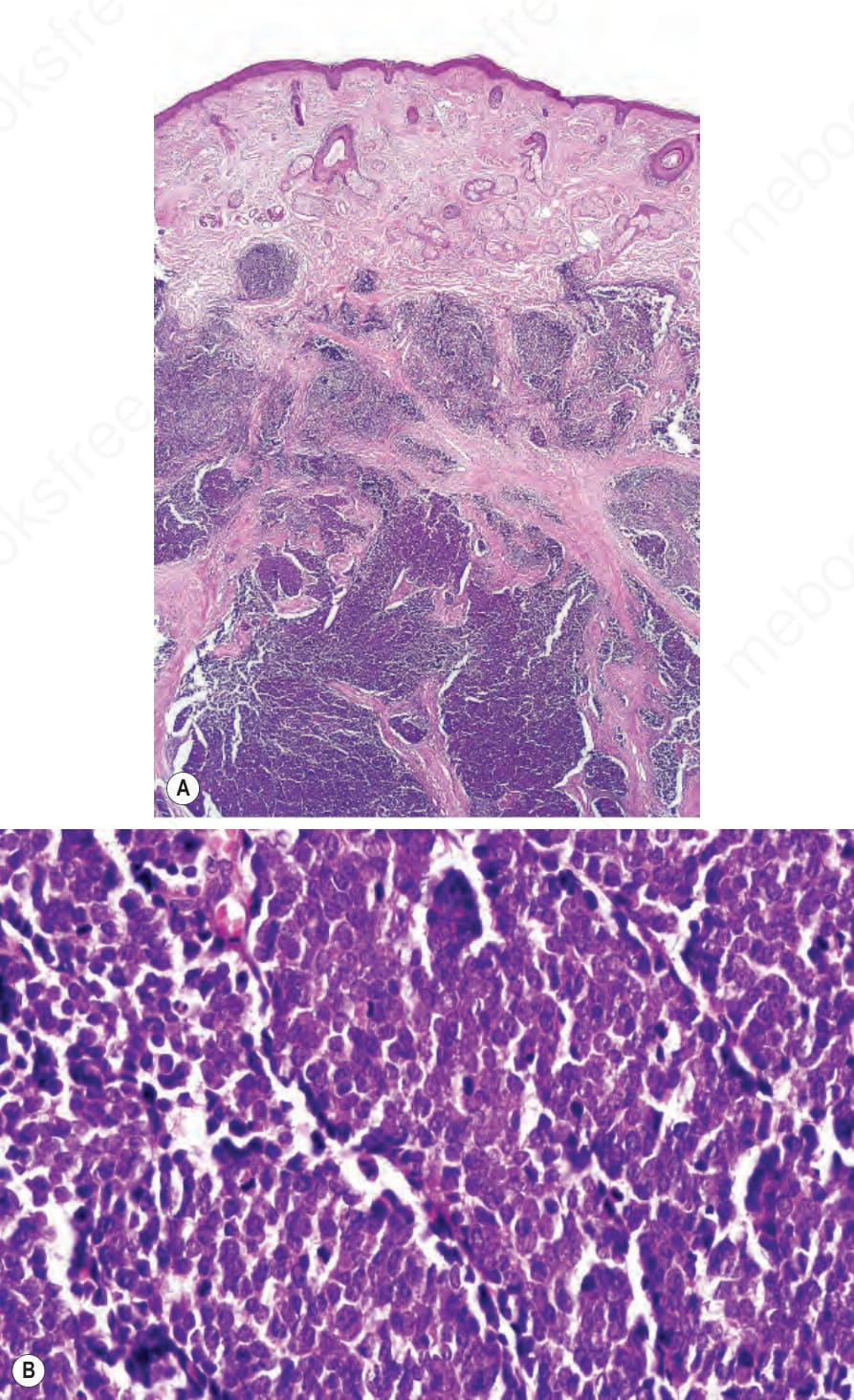
Fig. 30.52 Metastatic small cell carcinoma: (A, B) in the absence of clinical history or immunohistochemistry, it would not be possible to distinguish this metastasis from a primary cutaneous neuroendocrine carcinoma.