疾病定義與分類
- 肥大細胞肉瘤 (mast cell sarcoma) 極為罕見,雖然其最初表現為單一病灶 (solitary lesion),但無一例外地會迅速播散 (dissemination),並出現類似肥大細胞白血病 (mast cell leukemia) 的終末期 (terminal phase)。
- 此病已見於喉部 (larynx)、大腸 (large bowel)、腦膜 (meninges)、骨骼 (bone) 與皮膚的紀錄。
致病機轉與組織學特徵 (Pathogenesis and histologic features)
- 在 mastocytosis 中,位於第 4q12 號染色體 KIT 基因內的體細胞活化性點突變 (somatic activating point mutations) 相當常見。
- 這些突變大多數影響 tyrosine kinase domain 中的密碼子 816 (codon 816),涉及 Val 取代 Asp 的替換 (D816V)。此突變見於 ≥95% 的成人系統性 mastocytosis (systemic mastocytosis) 患者,但只見於約三分之一的皮膚型 mastocytosis (cutaneous mastocytosis) 患者。D816V 以外之點突變的發生頻率,在皮膚型較系統性 mastocytosis 顯著為高。
- 這些突變導致 KIT 的組成性活化 (constitutive activation),進而對下游路徑 (downstream pathways) 產生致癌效應 (oncogenic effects),影響細胞存活與功能;其中部分突變會使腫瘤對 tyrosine kinase inhibitors(如 imatinib)的治療產生抗性。在 mastocytosis 患者皮膚與骨髓的肥大細胞中,亦曾紀錄到抗凋亡蛋白 (antiapoptotic proteins) 表現增加。
- 一般而言,成人皮膚型 mastocytosis 的肥大細胞數量通常少於兒童型。其變化可能相當微妙,僅由乳頭層真皮 (papillary dermis) 內血管周圍肥大細胞輕度增加所構成,尤其見於臨床表現為持久發疹性斑狀毛細血管擴張症 (telangiectasia macularis eruptiva perstans) 的患者切片 (Figs 29.354 與 29.355)。
- 正常肥大細胞通常為卵圓形至多角形 (oval to polygonally shaped) 的細胞,具有中等量豐富的嗜伊紅性 (eosinophilic) 或雙嗜性 (amphophilic) 細胞質,內含許多細小、隱約可見的顆粒。肥大細胞以 Giemsa 或 toluidine blue 染色時呈異染性 (metachromatic),且細胞質內含 tryptase (Fig. 29.351)。細胞核呈圓形至卵圓形,染色質凝聚 (clumped chromatin),核仁不明顯 (indistinct nucleoli)。偶見雙核或多核細胞。當細胞核位於中央時,即呈現「煎蛋 (fried egg)」外觀。常見梭形 (spindled) 型態。在正常皮膚中,肥大細胞見於血管周圍並散布於整個真皮,但不形成聚集 (clusters)。
- 在較大的結節性病灶與單發性肥大細胞瘤 (solitary mastocytomas) 中,腫瘤樣沉積 (tumorlike deposits) 充滿整個真皮,並常延伸至皮下組織 (subcutis) (Figs 29.356 與 29.357)。
- 覆蓋表皮的基底層色素增加 (basal cell hyperpigmentation) 是色素性蕁麻疹 (urticaria pigmentosa) 的常見特徵,尤其見於斑丘疹性病灶 (maculopapular lesions) 中較陳舊的病灶,而結節 (nodules) 中較少見。淺層淋巴細胞 (lymphocytes) 與組織球 (histiocytes) 可能明顯,尤其在成人發病型 (adult-onset variant)。常可見嗜酸性球 (eosinophils),特別是在切片前病灶曾被搔抓 (rubbed) 的情況下。
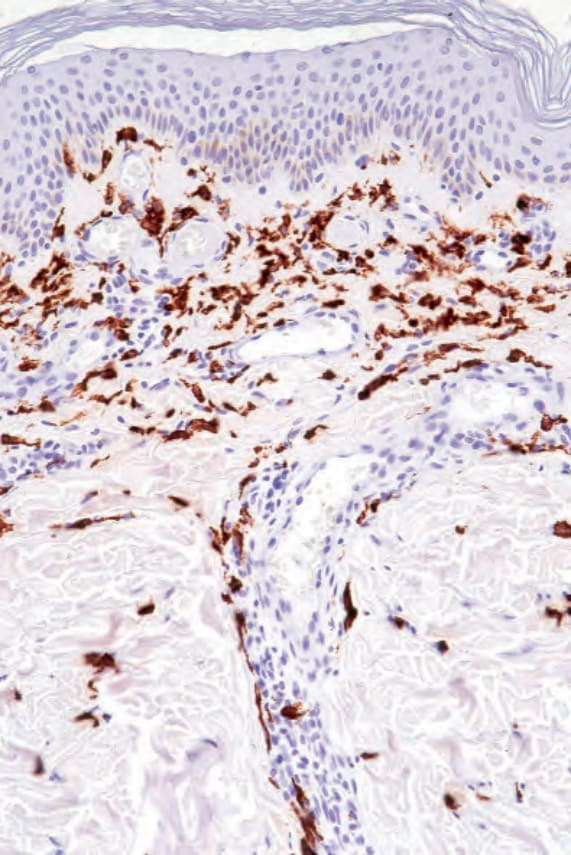
圖 29-351:色素性蕁麻疹 (urticaria pigmentosa):肥大細胞 tryptase 染色呈陽性。
Fig. 29.351 Urticaria pigmentosa: the mast cells are positive for tryptase.
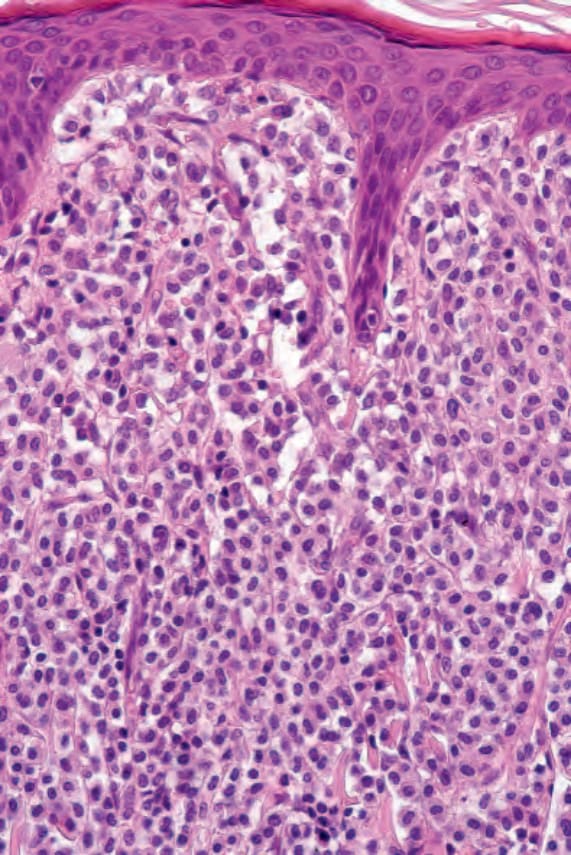
圖 29-352:色素性蕁麻疹 (urticaria pigmentosa):可見緻密的真皮細胞浸潤 (dense dermal cellular infiltrate)。
Fig. 29.352 Urticaria pigmentosa: there is a dense dermal cellular infiltrate.
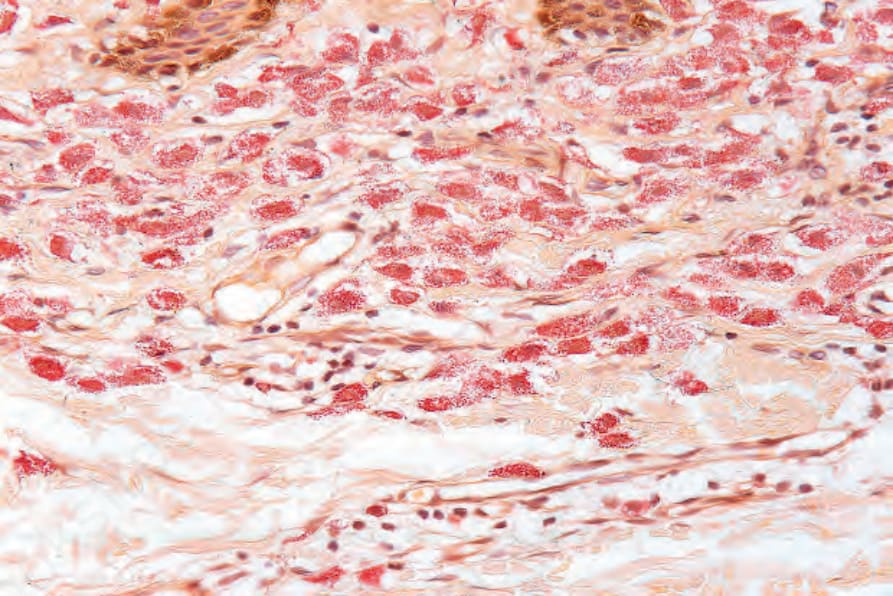
圖 29-353:色素性蕁麻疹 (urticaria pigmentosa):肥大細胞 chloracetate esterase 染色呈陽性。
Fig. 29.353 Urticaria pigmentosa: the mast cells stain for chloracetate esterase.
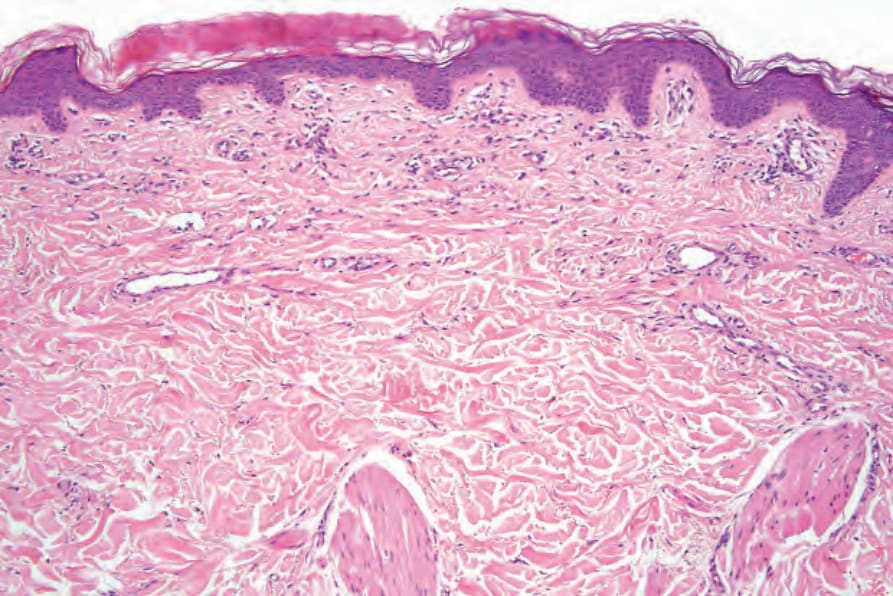
圖 29-354:持久發疹性斑狀毛細血管擴張症 (telangiectasia macularis eruptiva perstans):其特徵常極為微妙且容易被忽略。可見毛細血管擴張 (telangiectasia) 與極輕微的血管周圍浸潤 (perivascular infiltrate)。
Fig. 29.354 Telangiectasia macularis eruptiva perstans: the features are often very subtle and easily missed. There is telangiectasia and a very slight perivascular infiltrate.
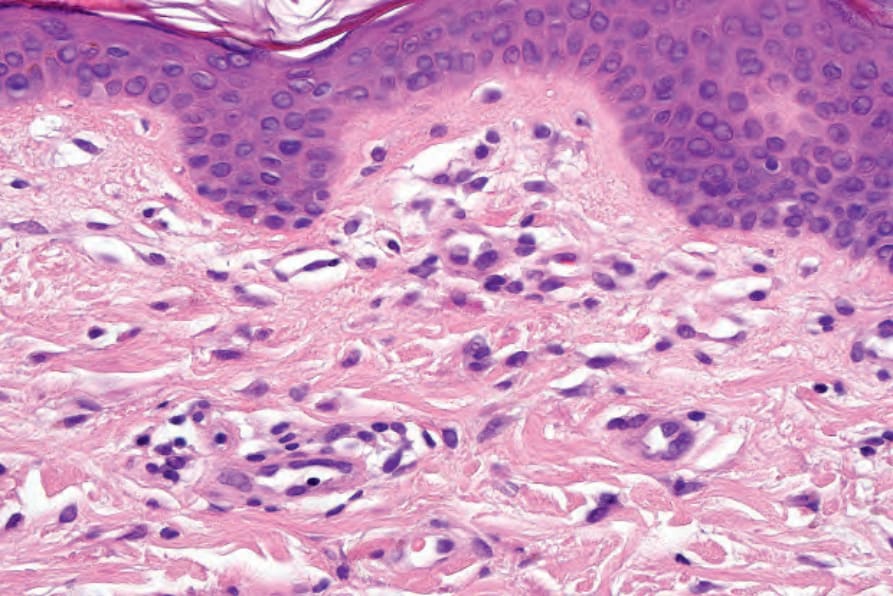
圖 29-355:持久發疹性斑狀毛細血管擴張症 (telangiectasia macularis eruptiva perstans):在此亞型中,肥大細胞常呈梭形型態 (spindled morphology)。
Fig. 29.355 Telangiectasia macularis eruptiva perstans: in this variant, the mast cells often adopt a spindled morphology.
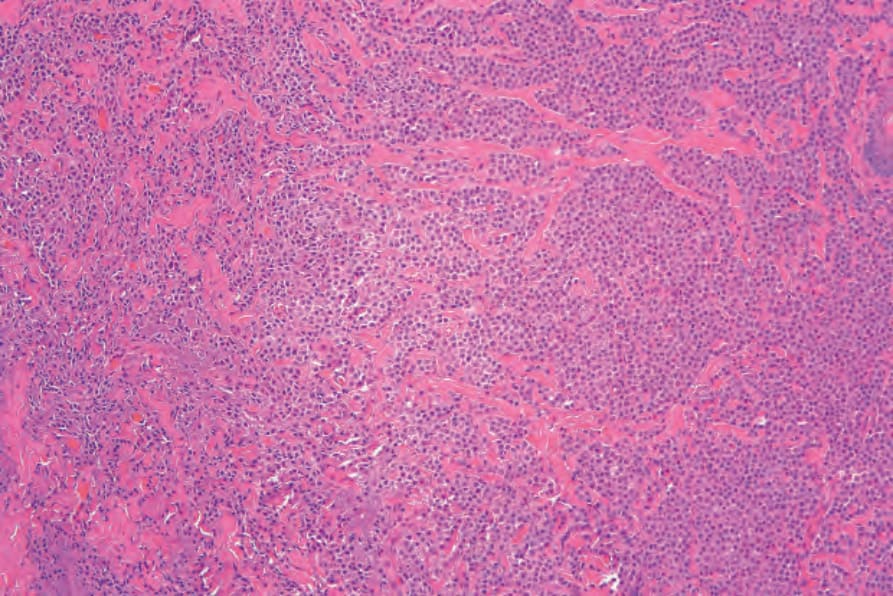
圖 29-356:肥大細胞瘤 (mastocytoma):腫瘤細胞具有豐富的嗜伊紅性細胞質 (eosinophilic cytoplasm) 與一致的深染細胞核 (uniform darkly staining nuclei)。
Fig. 29.356 Mastocytoma: the tumor cells have abundant eosinophilic cytoplasm and uniform darkly staining nuclei.
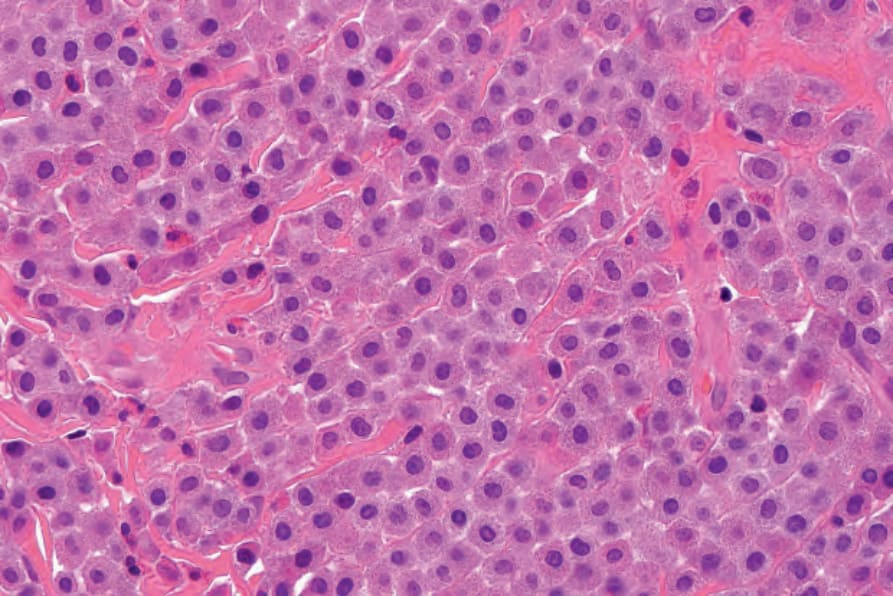
圖 29-357:肥大細胞瘤 (mastocytoma):高倍視野 (high-power view)。
Fig. 29.357 Mastocytoma: high-power view.
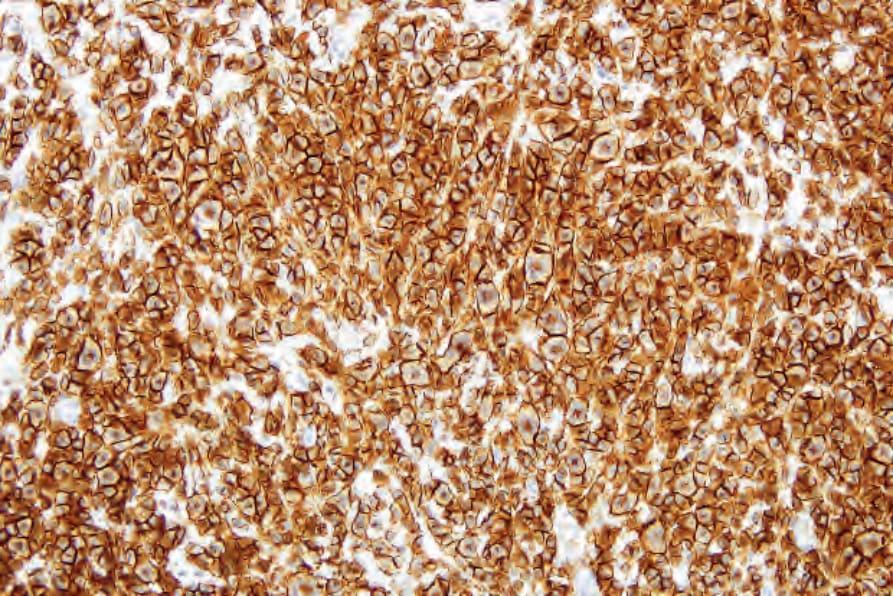
圖 29-358:肥大細胞瘤 (mastocytoma):CD117 染色呈顯著陽性。
Fig. 29.358 Mastocytoma: CD117 is strikingly positive.
免疫組化 (Immunohistochemistry)
- 肥大細胞表現 CD33、CD5、CD68、CD117、tryptase 與 chymase。CD117 也許是肥大細胞最敏感的標記,但並非特異性標記 (Fig. 29.358)。Chymase 具高度特異性,但其偵測敏感度較低。骨髓單核細胞標記 (myelomonocytic markers)(如 CD14、CD15、CD16)缺失,多數 T 細胞與 B 細胞標記亦缺失。
- 腫瘤性肥大細胞 (neoplastic mast cells) 與其正常對應細胞的不同之處,在於它們表現 CD2 與/或 CD25。此外,皮膚病灶中 CD25 的表現,是潛在系統性疾病 (underlying systemic disease) 的預測因子。
- 在 mastocytosis 中,腫瘤性肥大細胞在組織學上與正常者無法區分,診斷取決於評估其數量、分布與免疫表型 (immunoprofile)。尤其,必須存在肥大細胞的聚集 (aggregates) 才能做出明確診斷。在斑與丘疹 (macules and papules) 內,肥大細胞通常主要見於乳頭層真皮 (papillary dermis),且外觀正常 (Figs 29.352 與 29.353)。可能出現乳頭層真皮水腫 (edema of the papillary dermis);若病灶在切片前曾受外傷 (traumatized),有時可見表皮下水皰形成 (subepidermal vesiculation),主要見於單發性肥大細胞瘤 (solitary mastocytoma)。
鑑別診斷 (Differential diagnosis)
- 許多發炎性疾病 (inflammatory disorders) 中可見肥大細胞數量增加。此類反應性肥大細胞浸潤 (reactive mast cell infiltrates) 可能難以與腫瘤性浸潤相對稀疏的皮膚型 mastocytosis 病例區分。臨床資訊可能有所助益,但要確定診斷,應見到肥大細胞的聚集 (clusters);這可能需要不只一次的切片才能呈現出來。此外,免疫組化可能有所助益,CD2 與/或 CD25 的表現有助於將腫瘤性肥大細胞與反應性者區分開來。
請至 ExpertConsult.com 取得完整參考文獻列表。