Mast cell sarcoma
Mast cell sarcoma
Mast cell sarcoma is extremely rare, and although it presents initially as a solitary lesion, there is invariably rapid dissemination and a terminal phase
1518 Cutaneous lymphoproliferative diseases and related disorders
resembling mast cell leukemia. It has been documented in the larynx, large bowel, meninges, bone, and skin.1,52–55
Pathogenesis and histologic features Somatic activating point mutations within the KIT gene on chromosome 4q12 are common in mastocytosis.5,56–58 The majority of these affect codon 816 in the tyrosine kinase domain, and involve substitution of Val for Asp (D816V).56–63 This is seen in ≥95% of adult patients with systemic mastocytosis, but only in about one-third of patients with cutaneous mastocytosis.58,61–63 The frequency of point mutations other than D816V is significantly higher in cutaneous than in systemic mastocytosis.5,38,58,62–64 These mutations result in constitutive activation of KIT with subsequent oncogenic effects on downstream pathways that influence cell survival and function, and some render the tumor resistant to treatment with tyrosine kinase inhibitors such as imatinib.56,65 Increased expression of antiapoptotic proteins has also been documented in mast cells in the skin and bone marrow of patients with mastocytosis.13,66
As a rule, there are generally fewer mast cells in adult than childhood cutaneous mastocytosis. Changes may be quite subtle and consist only of a mild increase in perivascular mast cells in the papillary dermis, particularly in biopsies from patients showing clinical features of telangiectasia macularis eruptive perstans (Figs 29.354 and 29.355).
Normal mast cells are usually oval to polygonally shaped cells with moderately abundant, eosinophilic or amphophilic cytoplasm containing numerous small, faintly visible granules. Mast cells are metachromatic when stained with Giemsa or toluidine blue and contain cytoplasmic tryptase (Fig. 29.351). Nuclei are round to oval in shape with clumped chromatin and indistinct nucleoli. They are occasionally binucleate or multinucleate. When nuclei are centrally placed, a ‘fried egg’ appearance is present. A spindled morphology is frequent.14,18 In normal skin, mast cells are seen perivascularly and scattered throughout the dermis, but do not form clusters.
In the larger nodular lesions and in solitary mastocytomas, tumorlike deposits fill the entire dermis and often extend into the subcutis (Figs 29.356 and 29.357).
Basal cell hyperpigmentation of the overlying epidermis is a common feature in urticaria pigmentosa. It is found particularly in older lesions in the maculopapular lesions and less so in nodules.67 Superficial lymphocytes and histiocytes may be evident, especially in the adult-onset variant.67 Eosinophils are often seen, particularly if the lesion has been rubbed before biopsy.
Immunohistochemistry Mast cells express CD33, CD5, CD68, CD117, tryptase, and chymase. CD117 is perhaps the most sensitive but not a specific marker for mast cells (Fig. 29.358). Chymase is highly specific but its detection is less sensitive. Myelomonocytic markers such as CD14, CD15, and CD16 are absent, as are most T- and B-cell markers.4,68–71 Neoplastic mast cells differ from their normal counterparts in that they express CD2 and/or CD25. Moreover, expression of CD25 in skin lesions is a predictor for underlying systemic disease.72
In mastocytosis, the neoplastic mast cells are histologically indistinguishable from normal, and diagnosis depends on assessing their number, distribution, and immunoprofile. In particular, aggregates of mast cells must be present for an unequivocal diagnosis. Within the macules and papules, the mast cells are usually seen predominantly in the papillary dermis and they have normal appearance (Figs 29.352 and 29.353). There may be edema of the papillary dermis and if the lesion has been traumatized before biopsy, subepidermal vesiculation is sometimes evident mainly in solitary mastocytoma.39
Differential diagnosis Increased numbers of mast cells may be seen in many inflammatory disorders. Such reactive mast cell infiltrates may be difficult to differentiate from cases of cutaneous mastocytosis in which the neoplastic infiltrate is relatively sparse. Clinical information may be helpful, but to be certain of a diagnosis, clusters of mast cells should be seen. This may take more than one biopsy to demonstrate. In addition, immunohistochemistry may be helpful, with expression of CD2 and/or CD25 facilitating differentiation of neoplastic mast cells from reactive ones.1
Access ExpertConsult.com for the complete list of references
1519 Mastocytosis
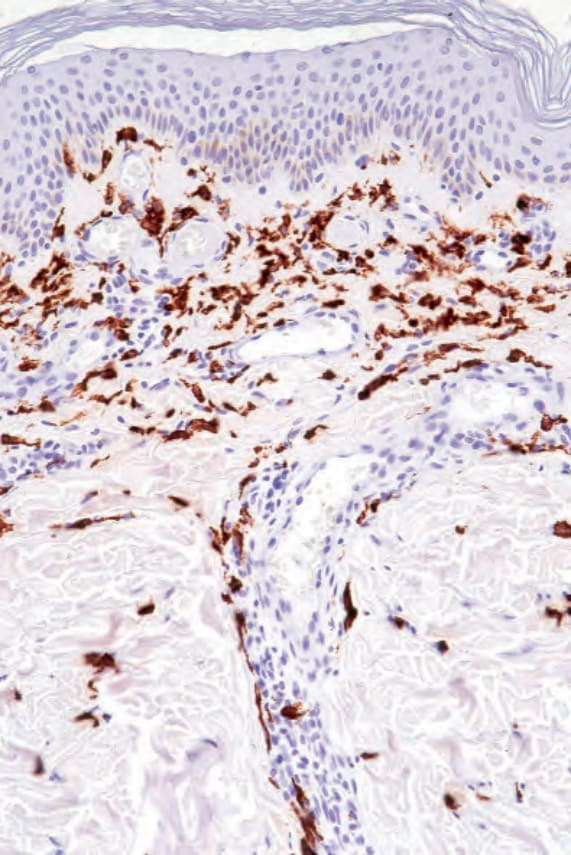
Fig. 29.351 Urticaria pigmentosa: the mast cells are positive for tryptase.
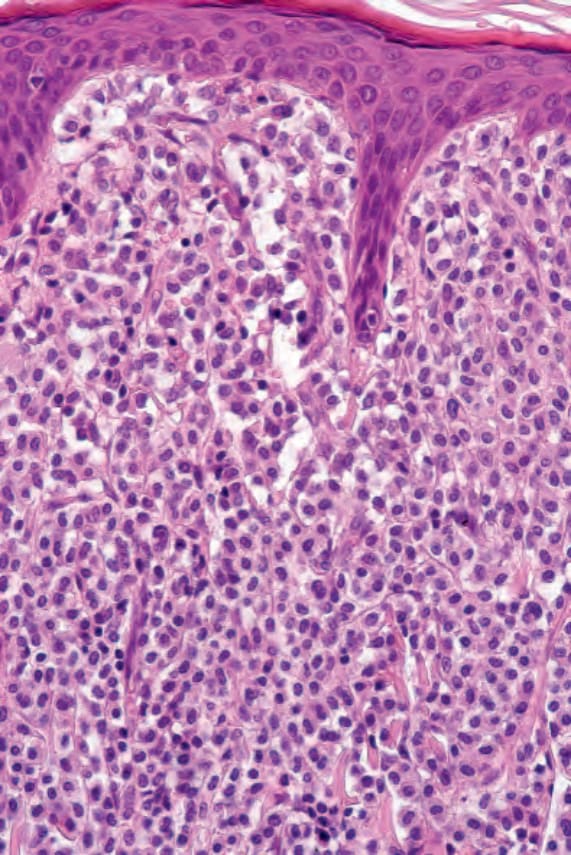
Fig. 29.352 Urticaria pigmentosa: there is a dense dermal cellular infiltrate.
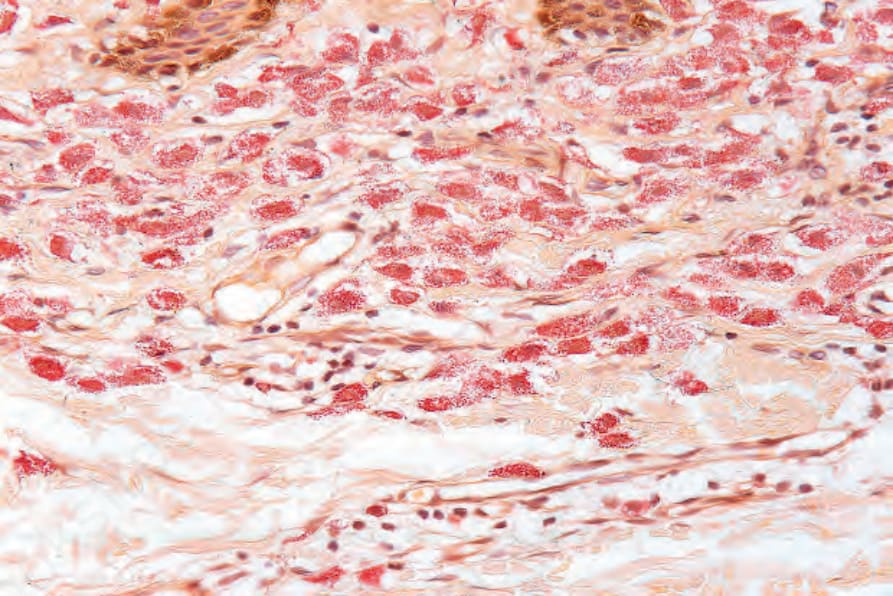
Fig. 29.353 Urticaria pigmentosa: the mast cells stain for chloracetate esterase.
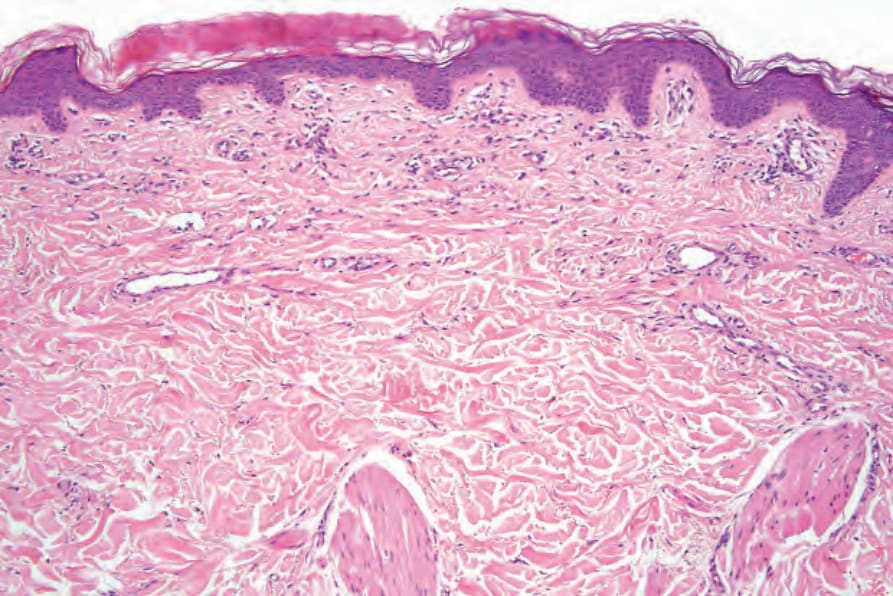
Fig. 29.354 Telangiectasia macularis eruptiva perstans: the features are often very subtle and easily missed. There is telangiectasia and a very slight perivascular infiltrate.
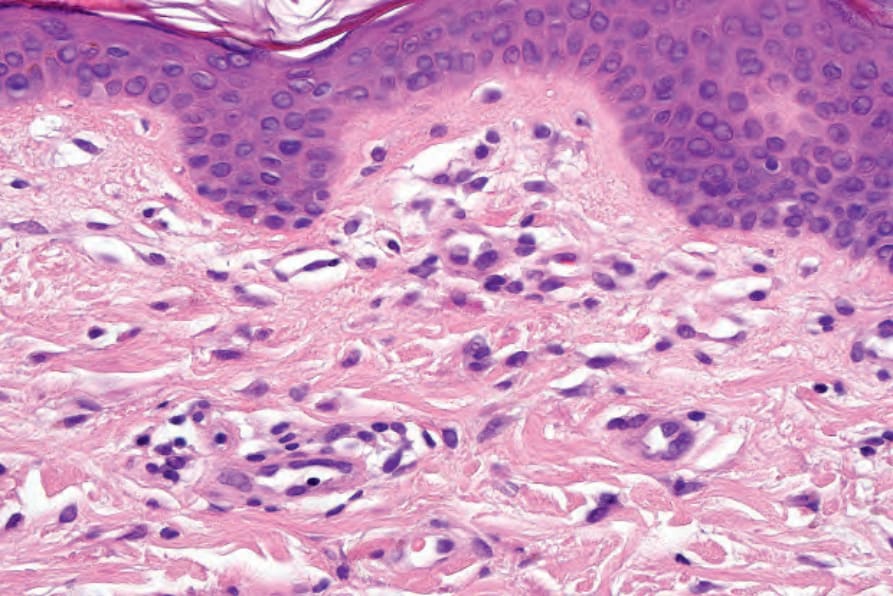
Fig. 29.355 Telangiectasia macularis eruptiva perstans: in this variant, the mast cells often adopt a spindled morphology.
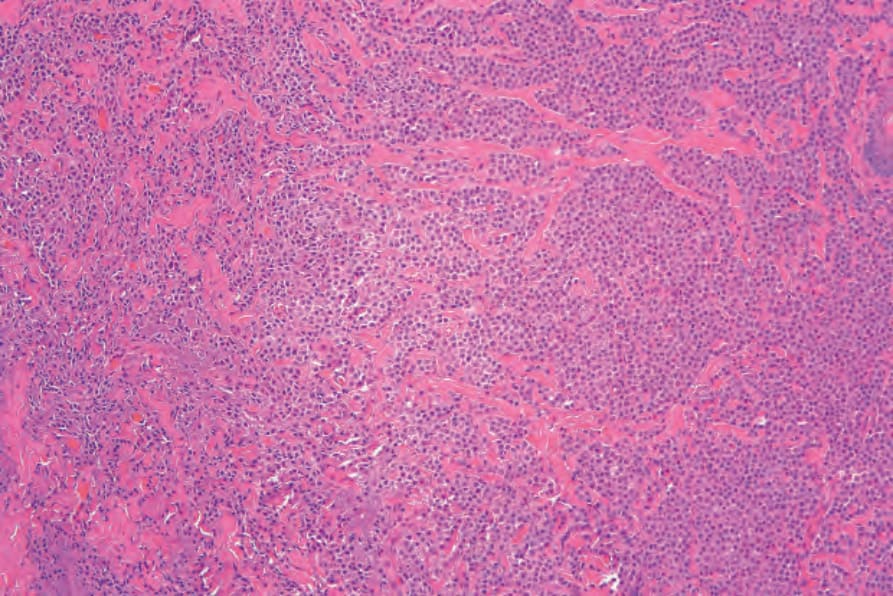
Fig. 29.356 Mastocytoma: the tumor cells have abundant eosinophilic cytoplasm and uniform darkly staining nuclei.
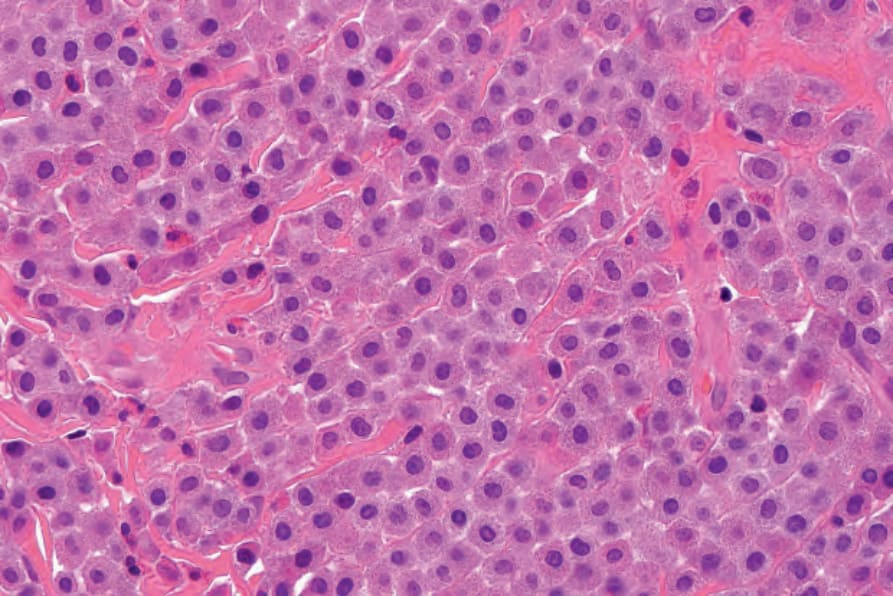
Fig. 29.357 Mastocytoma: high-power view.
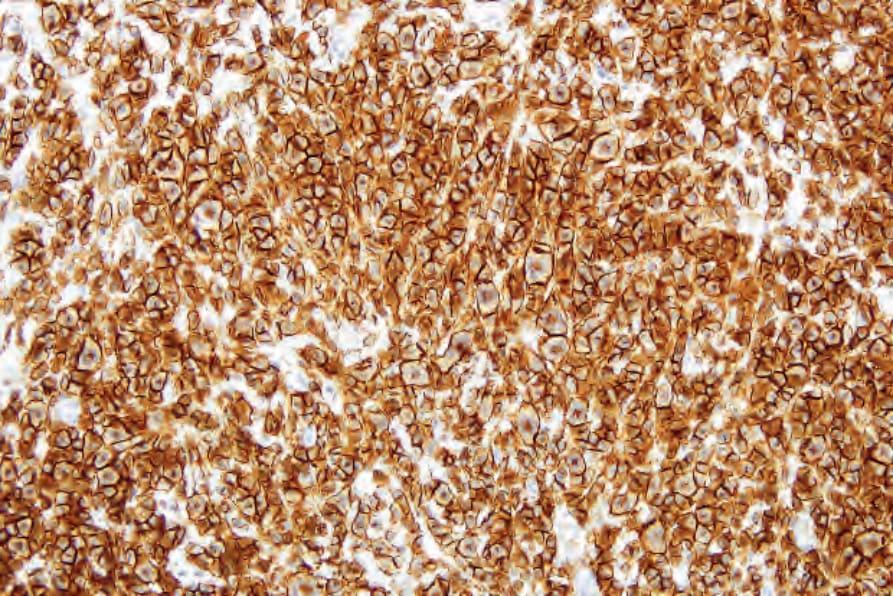
Fig. 29.358 Mastocytoma: CD117 is strikingly positive.