HISTIOCYTIC DISORDERS
引言
組織球增多症 (histiocytoses) 是一群異質性的反應性與腫瘤性疾病,其特徵為樹突細胞 (dendritic) 或單核球—巨噬細胞 (monocyte–macrophage) 系的細胞在包括皮膚在內的各種組織中增生。由於其相對罕見、術語使用不精確,以及對病灶細胞確切系別 (lineage) 缺乏認識,這群疾病一直是相當混淆的來源。
「組織球 (histiocyte)」一詞泛指一群以組織為基礎的免疫細胞,包含巨噬細胞 (macrophages) 與樹突細胞 (dendritic cells) 兩者。巨噬細胞展現強大的吞噬能力 (phagocytic capabilities),主要作為抗原呈現細胞 (antigen presenting cells) 發揮功能;而樹突細胞則主要為具有抗原呈現功能的輔助細胞 (accessory cells)。這兩群之間的區分往往並不清楚,因為兩種細胞類型都展現相當的可塑性 (plasticity),其特性會隨其發育階段及/或所處微環境 (microenvironment) 的影響而改變。這導致了相當程度的功能性、形態學與免疫表型 (immunophenotypic) 重疊。
本版用以定義各種疾病實體的系統,是基於 Histiocyte Society 近期提出、針對組織球增多症與巨噬細胞—樹突細胞系腫瘤的修訂分類。此分類考量了組織學、表型、分子、臨床與影像學特徵。它辨識出五群疾病:
- 皮膚與皮膚黏膜 (非 Langerhans 細胞) 組織球增多症 (cutaneous and mucocutaneous [non-Langerhans cell] histiocytoses),
- Rosai-Dorfman disease (RDD),
- 惡性組織球增多症 (malignant histiocytoses),
- 噬血性淋巴組織球增多症 (hemophagocytic lymphohistiocytosis, HLH) 與巨噬細胞活化症候群 (macrophage activation syndrome)。
歷史上,LCH 一直與非 Langerhans 細胞組織球增多症分開。然而,LCH 與 Erdheim-Chester disease (ECD) 之間共有的遺傳異常與臨床特徵之發現,使得兩者連同未定型細胞組織球增多症 (indeterminate cell histiocytosis) 一同被歸入 Langerhans cell-related 群組。皮膚與皮膚黏膜組織球增多症涵蓋了黃色肉芽腫家族疾病 (xanthogranuloma family of diseases) 以及多中心性網狀組織球增多症 (multicentric reticulohistiocytosis, MRH)。皮膚型 RDD (cutaneous RDD) 亦納入此群組,與典型散發性 RDD (classical sporadic RDD) 以及繼發於易感性遺傳病況的 RDD (RDD secondary to predisposing inherited conditions) 分開。惡性組織球增多症 (malignant histiocytosis) 包含先前被診斷為組織球肉瘤 (histiocytic sarcoma, HS)、交織狀樹突細胞 (interdigitating dendritic cell, IDC) 肉瘤、Langerhans 細胞肉瘤 (Langerhans cell sarcoma, LCS) 與未定型細胞肉瘤 (indeterminate cell sarcoma) 的病例。這些可能為原發 (de novo) 或繼發於其他惡性腫瘤。最後,還有一類為 HLH 與巨噬細胞活化症候群,可能與遺傳性基因疾病相關或繼發於其他病因。這些疾病詳列於 Table 29.5。
大多數組織球源自 CD34+ 骨髓前驅細胞 (CD34+ bone marrow progenitor),不過有些可能衍生自間葉細胞 (mesenchymal cells,如 FDCs) 甚至淋巴球 (lymphocytes)。對後續發育的一種簡化觀點認為,發育遵循兩條路徑之一,成熟為 CD14– 或 CD14+ 細胞。前者衍生出 Langerhans cells,而後者則為真皮樹突細胞 (dermal dendritic cells) 或單核球/巨噬細胞 (monocyte/macrophages) 的來源。
表中未列出的兩個額外疾病實體會先行討論,這兩者為皮膚型 Kikuchi-Fujimoto disease (cutaneous Kikuchi-Fujimoto disease, KFD) 與淋巴管內組織球增多症 (intralymphatic histiocytosis, IH)。
鑑別診斷 (Differential Diagnosis)
鑑別診斷包括 pityriasis lichenoides、紅斑性狼瘡 (lupus erythematosus),以及與 EBV 感染相關之抗生素誘發性不良疹 (antibiotic-induced eruptions)。在 pityriasis lichenoides 中,可見壞死性角質細胞 (necrotic keratinocytes) 與基底細胞的水樣變性 (hydropic degeneration of basal cells)。然而其浸潤 (infiltrate) 以淋巴球為主,且核碎屑 (nuclear debris) 若存在也非常局灶性。與 lupus erythematosus 的區分極為困難,特別是其淋巴結變化可能完全相同。區分需依賴臨床病理對照 (clinicopathological correlation)、免疫螢光 (immunofluorescence),以及 lupus erythematosus 皮膚病灶中組織球稀少與漿細胞 (plasma cells) 存在這一點。與 EBV 感染相關之抗生素誘發性不良疹的組織學特徵,與 KFD 所見者完全相同,其區分需依賴臨床資訊。
Table 29.5 各組織球增多症之分類
Langerhans 細胞家族組織球增多症 (Langerhans cell family of histiocytoses):Langerhans cell histiocytosis、Congenital self-healing histiocytosis、Indeterminate dendritic cell tumor、Erdheim-Chester disease
皮膚與皮膚黏膜組織球增多症 (非 Langerhans 細胞) (Cutaneous and mucocutaneous histiocytoses, non-Langerhans cell)——黃色肉芽腫家族 (Xanthogranuloma family):
- Juvenile xanthogranuloma
- Benign cephalic histiocytosis
- Generalized eruptive histiocytosis
- Xanthoma disseminatum
- (scalloped cell granuloma)
- Papular xanthoma
- Progressive nodular histiocytosis
- (spindle cell xanthogranuloma) (Cutaneous Rosai-Dorfman disease) Multicentric reticulohistiocytosis
淋巴管內組織球增多症 (Intralymphatic histiocytosis)
惡性組織球增多症 (Malignant histiocytoses):Langerhans cell sarcoma、Follicular dendritic cell sarcoma、Interdigitating dendritic cell sarcoma、Histiocytic sarcoma
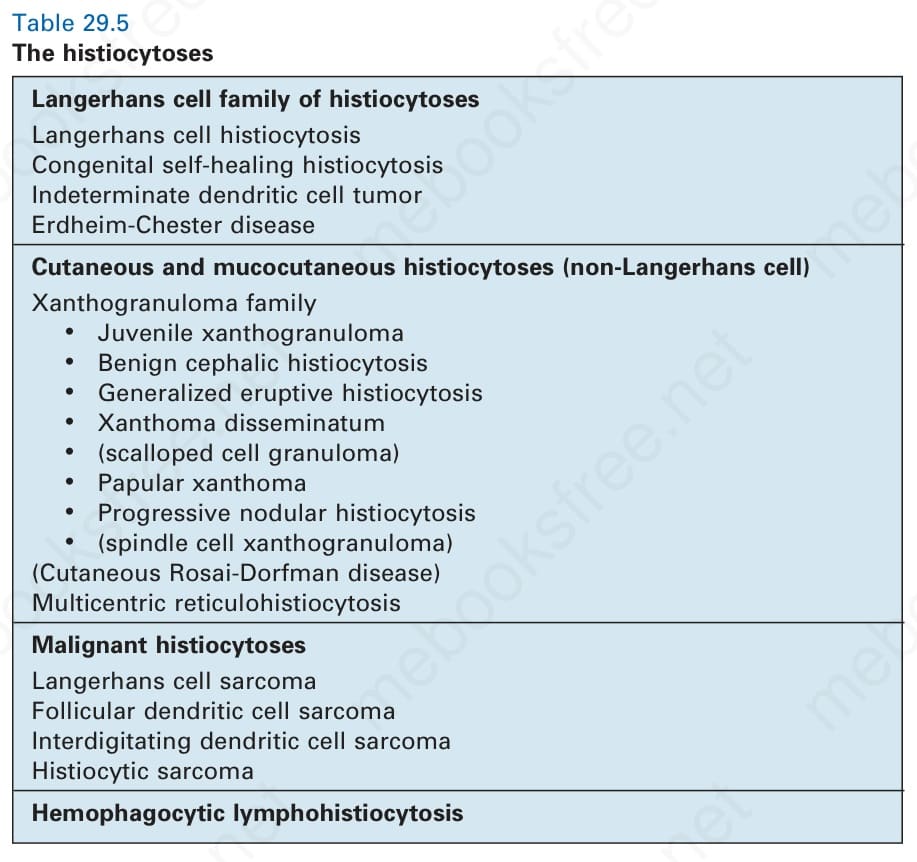
表 29-5:各組織球增多症之分類 (the histiocytoses)。
Table 29.5 The histiocytoses