B 細胞皮膚淋巴樣增生 (B-cutaneous lymphoid hyperplasia)
臨床特徵 (Clinical Features)
- B 細胞皮膚淋巴樣增生 (B-cutaneous lymphoid hyperplasia;cutaneous B-cell pseudolymphoma) 為一通稱,用以指稱含顯著 B 細胞成分、會模擬 B 細胞淋巴瘤 (B-cell lymphoma) 的反應性淋巴樣浸潤。它涵蓋多種不同的臨床病理情境,但具有共同的組織學終點;最適切的描述方式是稱為 B-cutaneous lymphoid hyperplasia (B-CLH)。此類疾病的歷史名稱包括 sarcomatosis cutis、lymphocytoma cutis、lymphadenosis benigna cutis,以及 pseudolymphoma of Spiegler and Fendt。
- 在某些情況下可辨識出誘發病因。例子包括節肢動物叮咬 (arthropod bites)、Borrelia 感染、外傷 (trauma)、疫苗接種 (vaccinations)、注射藥物或減敏用抗原 (injected drugs or antigens for hyposensitization)、針灸 (acupuncture)、金製穿洞耳環 (gold pierced earrings)、刺青 (tattoos),以及水痘-帶狀疱疹感染後留下的疤痕 (varicella-zoster infection scars)。然而,在大多數病例中,病因仍不明。
- 臨床表現在某種程度上取決於 B 細胞假性淋巴瘤 (B-cell pseudolymphoma) 發生的情境。原發性(特發性)cutaneous B-cell pseudolymphoma 可能構成最大的一群,最常見於顏面(臉頰、鼻、耳垂)(70%)、胸部與上肢。對女性有偏好性 (3 : 1),且白人較黑人更常受影響 (9 : 1)。
- 在歐洲流行區,B. burgdorferi 可能是最常見的病因,雖然 cutaneous B-cell pseudolymphoma 是 Lyme 病 (Lyme disease) 的罕見表現,在具有血清學和/或臨床感染證據的患者中盛行率僅 0.6–1.3%。特異性皮膚病灶通常在被蜱叮咬後數週至數月內出現,通常位於乳頭區、生殖器區或耳垂 (Fig. 29.254)。這些病灶可能新發 (de novo),也可能在慢性遊走性紅斑 (erythema chronicum migrans) 的背景上發生。
- 無論病因為何,大多數患者表現為單發、小型、紅色至李子色 (plum-colored) 或藍色的斑塊與結節。潰瘍 (ulceration) 極為罕見,多發性病灶 (multiple lesions) 不常見。多數病例呈良性臨床病程,許多在移除致病刺激後消退,但部分病例呈慢性且對治療頑固。B-CLH 演變為明顯 B-cell lymphoma 的例子亦有充分文獻記載,因此可能存在一個疾病譜系。故建議所有患者均接受追蹤。
致病機轉與組織病理特徵 (Pathogenesis and Histopathological Features)
- 在 cutaneous B-cell pseudolymphoma 中,持續性抗原刺激 (persistent antigenic stimulation) 被推測為 B-CLH 的成因,尤其在可辨識出誘發病因時更是如此。例如,在許多與 Borrelia 相關的 cutaneous B-cell pseudolymphoma 病例中可偵測到 B. burgdorferi 特異性 DNA。在與節肢動物叮咬相關而發生 B-CLH 的皮膚切片中曾辨識出口器 (mouthparts),且在與疫苗接種相關之 cutaneous B-cell pseudolymphoma 的部位曾證實有佐劑(aluminum hydroxide,氫氧化鋁)的存在。刺青誘發之 B-CLH 似乎主要與紅色刺青色素相關,只有罕見情況與綠色或藍色刺青相關。亦有一例 B-CLH 記載於一位 Sjögren syndrome 患者,提示在某些病例中可能有自體抗原刺激 (autoantigenic stimulation)。此外,某些樹突細胞亞型 (dendritic cell subtypes) 在 B-CLH 中的數量多於 cutaneous B-cell lymphoma,更進一步暗示持續性抗原刺激在致病機轉中的角色。
- 在歷史文獻中報導為對 cutaneous B-cell pseudolymphoma 相對具特異性的組織學特徵,包括「上重型 (top heavy)」分布,在現代的審視下並不成立,尤其因為許多早期系列研究在其假性淋巴瘤世代中錯誤地納入了 cutaneous B-cell lymphoma 的例子。事實上,低倍鏡檢查常顯示一片瀰漫、隱約呈結節狀的浸潤,充滿真皮且有時侵犯皮下組織 (subcutis) (Fig. 29.255)。在較不旺盛的例子中,浸潤傾向呈結節狀並呈血管周圍 (perivascular) 及附屬器周圍 (periadnexal) 分布,但仍可能延伸至深層網狀真皮 (deep reticular dermis) 與皮下組織。常見有 grenz zone,但也可見胞吐 (exocytosis) 與海綿水腫 (spongiosis),且其他表皮變化(如萎縮 (atrophy)、增生 (hyperplasia) 及角化不全 (parakeratosis))相對常見。
- 此淋巴樣組織與較常見部位(如淋巴結、扁桃腺)的反應性淋巴樣組織相似。淋巴濾泡 (lymphoid follicles) 幾乎總是存在。這些濾泡本質上可能為原發性 (primary),由緊密排列的小淋巴細胞組成,但在大多數病例中反應性生發中心 (reactive germinal centers) 亦相當顯著。生發中心 (germinal centers) 由大型中心母細胞 (centroblasts)、大小中心細胞 (centrocytes) 以及可染小體巨噬細胞 (tingible body macrophages) 混合組成。雖然在其他部位的生發中心中,受壓的小淋巴細胞外套層 (mantle) 是常態,但在 B-CLH 中卻常缺乏,尤其在與 Borrelia 感染相關的病例。反應性生發中心具有高增殖率,常呈「分區 (zoned)」外觀,深染區域充滿增殖中的 centroblasts,而較淡的區域則以 centrocytes 為主 (Figs 29.256 and 29.257)。濾泡間區域 (interfollicular areas) 則由多形性浸潤填充,以小淋巴細胞為主,散在的母細胞 (blast cells)、組織球 (histiocytes)、漿細胞 (plasma cells),有時還有嗜酸性球 (eosinophils)。
- 淋巴濾泡可藉由標記 FDC 網絡 (FDC networks) 的抗體(CD21、CD23 與 CD35)以免疫組化方式辨識 (Fig. 29.258)。原發性 B 細胞濾泡含有均一的小 B 淋巴細胞群(CD20 陽性),其中許多共同表現 CD23 (Fig. 29.259)。生發中心 B 細胞表現 CD10 與 bcl-6,但不表現 bcl-2。T 細胞在濾泡間區域中佔主導,但亦可見少量 B 細胞 (Fig. 29.260),包括一部分散在的母細胞 (Fig. 29.260)。這些細胞通常不表現 CD10。針對輕鏈 (light chains) 的免疫組化或原位雜交 (in situ hybridization) 顯示 B 淋巴細胞與漿細胞呈多型性 (polytypic) 染色模式 (Figs 29.261 and 29.262)。
- PCR 株系性 (clonality) 分析最常顯示免疫球蛋白基因重排 (immunoglobulin gene rearrangement) 呈多株性 (polyclonal) 模式。然而,在其他方面均符合 B-CLH 典型表現的病灶中亦曾證實有株系性 (clonality)。
鑑別診斷 (Differential Diagnosis)
- B-CLH 的主要鑑別診斷為原發性皮膚邊緣區淋巴瘤 (primary cutaneous marginal zone lymphoma) 與皮膚濾泡中心淋巴瘤 (cutaneous follicle center lymphoma),如先前在這些疾病的相關章節中所討論。簡言之,在 marginal zone lymphoma 中可見成片的邊緣區細胞 (marginal zone cells)、濾泡間 B 淋巴細胞佔主導,以及 B 細胞異常表現 CD43。
- PCFCL 或續發性侵犯皮膚的 follicular lymphoma 中的腫瘤性濾泡,通常呈單調 (monotonous) 外觀,無分區 (zonation),可染小體巨噬細胞與有絲分裂象 (mitotic figures) 相對較少,且增殖比例 (proliferation fraction) 低。在續發性 follicular lymphoma 中,腫瘤性濾泡通常亦呈 bcl-2 陽性,雖然在 PCFCL 中此情況較少見。
- 此發現通常會提示淋巴瘤,但在此情境下,這些聚集物可能代表缺乏外套層之濾泡中心的小型橫切面。傾向良性診斷的依據包括存在大量可染小體巨噬細胞,以及伴隨的小淋巴細胞、組織球、嗜酸性球與漿細胞所組成的混合性反應性浸潤。
- 藉由原位雜交或輕鏈免疫組化證實單株性 (monoclonality) 是淋巴瘤的強烈證據,但鑑於已有充分文獻記載的株系性 B-CLH (clonal B-CLH) 例子,免疫球蛋白基因重排研究較不具決定性。此外,由於在皮膚切片上進行 PCR 時遭遇假株系性 (pseudoclonality) 的發生率相對較高,分子檢測結果的判讀更為受限。

圖 29-254:B 細胞皮膚淋巴樣增生 (B-cutaneous lymphoid hyperplasia):耳垂 (earlobe) 是常受影響的部位。病灶通常為單發。By courtesy of the Institute of Dermatology, London, UK.
Fig. 29.254 B-cutaneous lymphoid hyperplasia: the earlobe is a commonly affected site. Lesions are usually solitary. By courtesy of the Institute of Dermatology, London, UK.
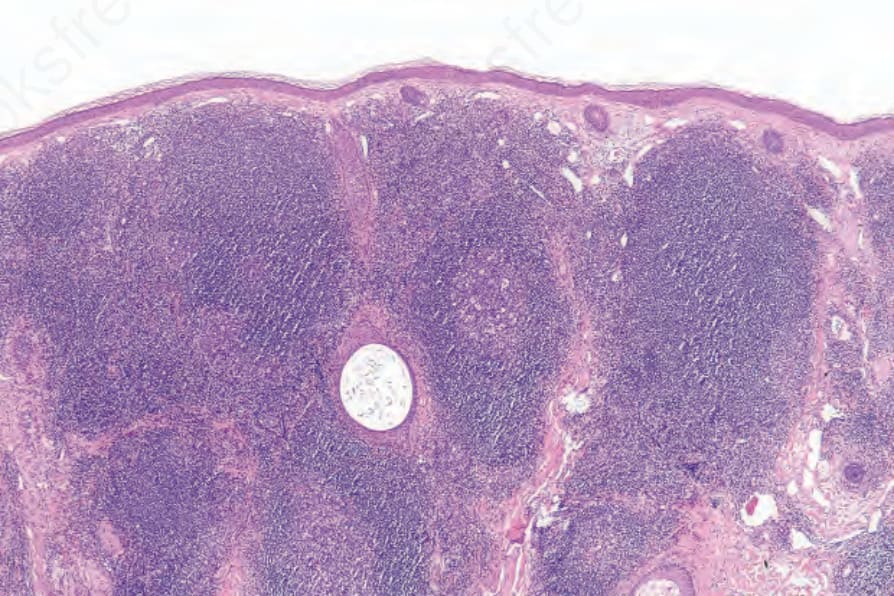
圖 29-255:B 細胞皮膚淋巴樣增生 (B-cutaneous lymphoid hyperplasia):可見緻密的真皮淋巴樣浸潤 (dense dermal lymphoid infiltrate) 伴有明顯的生發中心 (germinal centers)。
Fig. 29.255 B-cutaneous lymphoid hyperplasia: there is a dense dermal lymphoid infiltrate with conspicuous germinal centers.
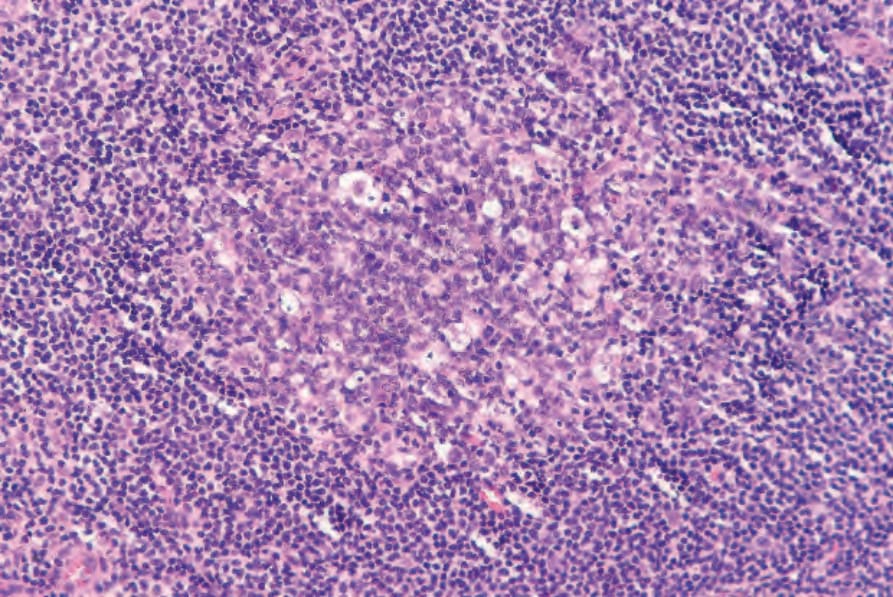
圖 29-256:B 細胞皮膚淋巴樣增生 (B-cutaneous lymphoid hyperplasia):生發中心 (germinal center) 內有明顯的可染小體巨噬細胞 (tingible body macrophages)。
Fig. 29.256 B-cutaneous lymphoid hyperplasia: there are prominent tingible body macrophages within the germinal center.
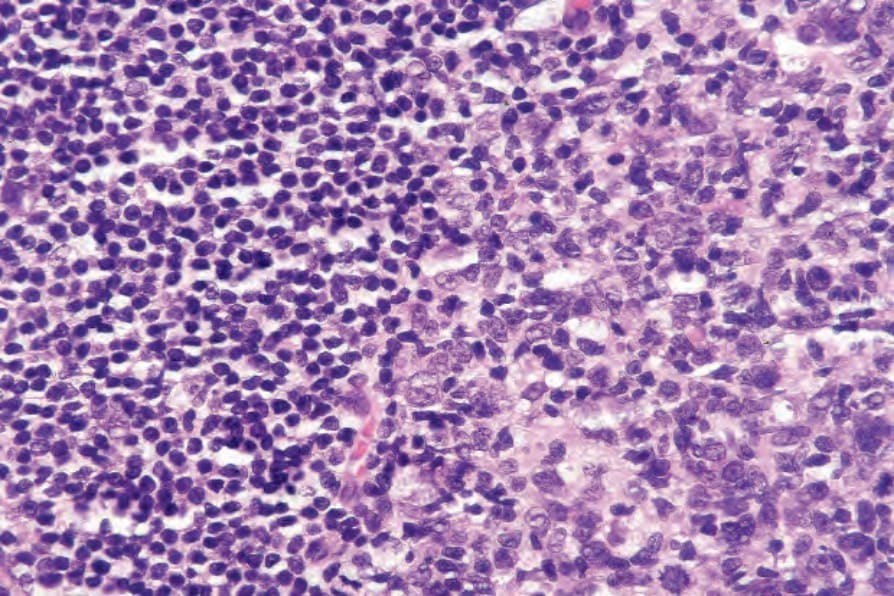
圖 29-257:B 細胞皮膚淋巴樣增生 (B-cutaneous lymphoid hyperplasia):生發中心 (germinal center) 邊緣及鄰近成熟小淋巴細胞 (mature small lymphocytes) 群的高倍視野。
Fig. 29.257 B-cutaneous lymphoid hyperplasia: high-power view of edge of germinal center and adjacent population of mature small lymphocytes.
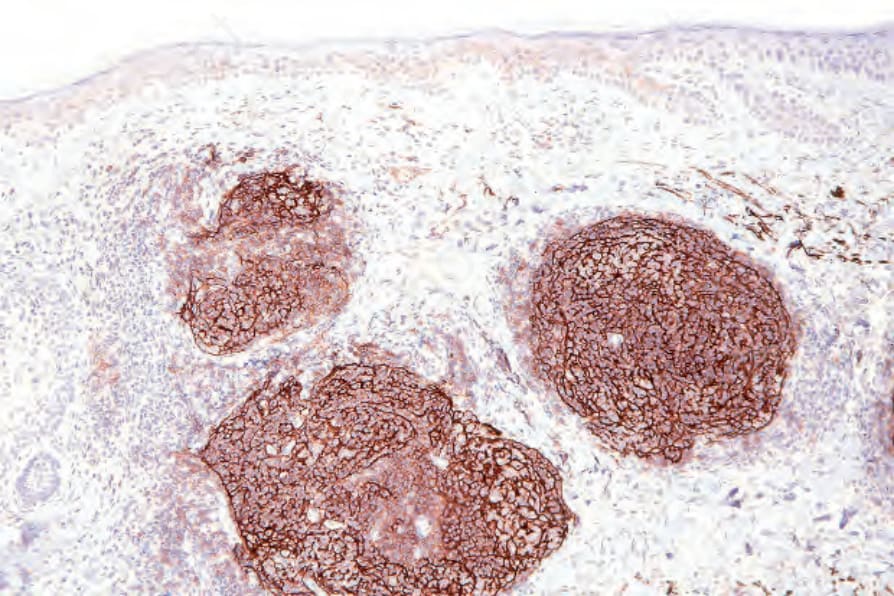
圖 29-258:B 細胞皮膚淋巴樣增生 (B-cutaneous lymphoid hyperplasia):藉由顯示濾泡樹突細胞群 (follicular dendritic cell population)(CD21)勾勒出濾泡結構。
Fig. 29.258 B-cutaneous lymphoid hyperplasia: the follicular architecture is outlined by demonstration of the follicular dendritic cell population (CD21).
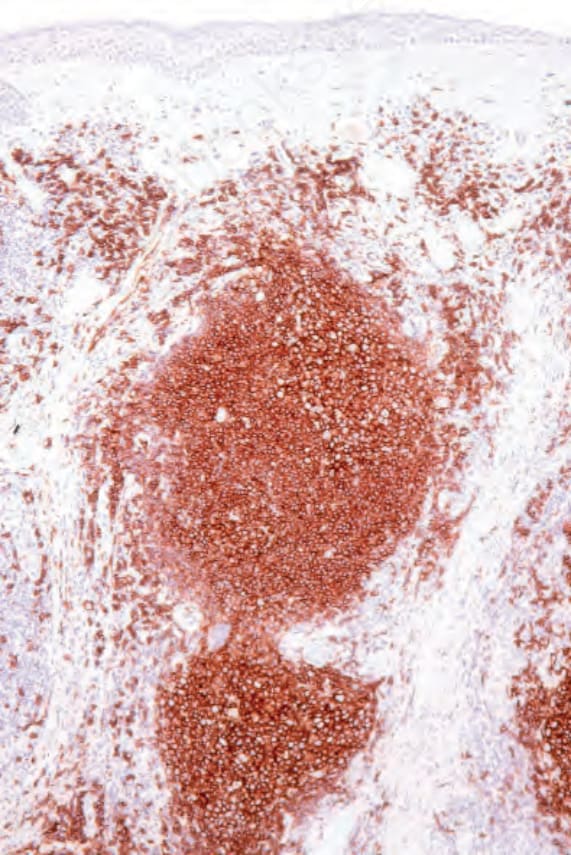
圖 29-259:B 細胞皮膚淋巴樣增生 (B-cutaneous lymphoid hyperplasia):以 CD20 免疫組化勾勒出 B 細胞成分。
Fig. 29.259 B-cutaneous lymphoid hyperplasia: the B-cell component is outlined with CD20 immunohistochemistry.
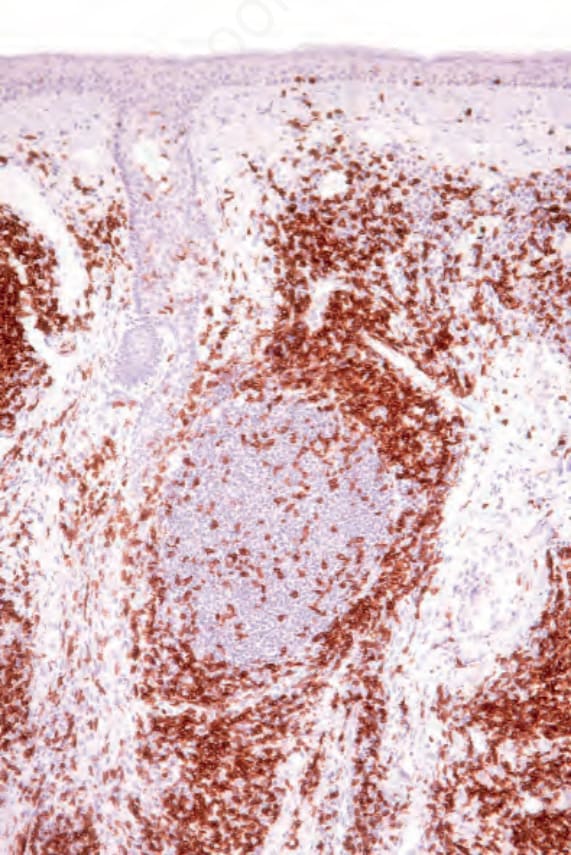
圖 29-260:B 細胞皮膚淋巴樣增生 (B-cutaneous lymphoid hyperplasia):一層 T 細胞 (T cells)(CD3)環繞著 B 細胞結節 (B-cell nodules)。
Fig. 29.260 B-cutaneous lymphoid hyperplasia: a layer of T cells (CD3) surrounds the B-cell nodules.
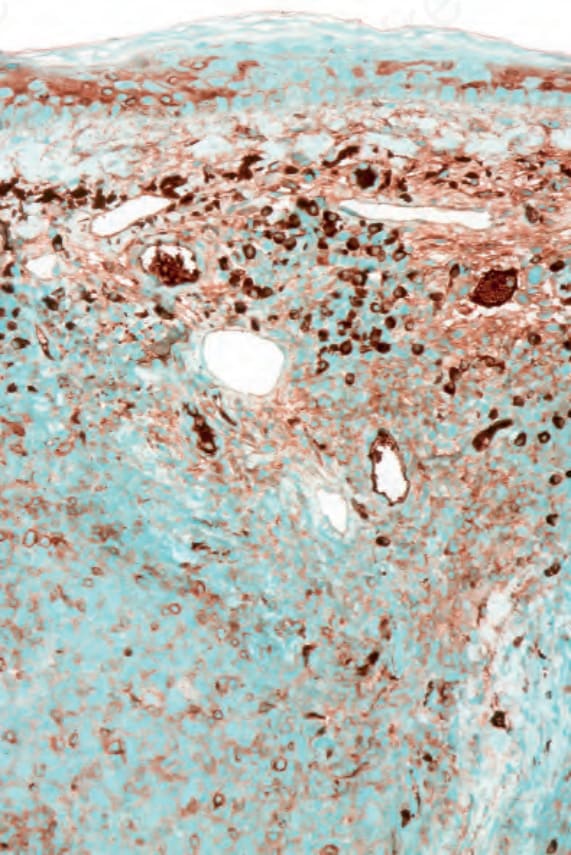
圖 29-261:B 細胞皮膚淋巴樣增生 (B-cutaneous lymphoid hyperplasia):kappa 漿細胞 (kappa plasma cells) 散布於整個浸潤中。
Fig. 29.261 B-cutaneous lymphoid hyperplasia: kappa plasma cells are scattered throughout the infiltrate.