B-cutaneous lymphoid hyperplasia
B-cutaneous lymphoid hyperplasia
Clinical features B-cutaneous lymphoid hyperplasia (cutaneous B-cell pseudolymphoma) is a generic term employed to denote reactive lymphoid infiltrates with a significant B-cell component that simulate B-cell lymphoma. It encompasses a variety of different clinicopathological scenarios with a common histologic endpoint; it is best described as B-cutaneous lymphoid hyperplasia (B-CLH). The historical terminology for this group of disorders includes
sarcomatosis cutis, lymphocytoma cutis, lymphadenosis benigna cutis, and pseudolymphoma of Spiegler and Fendt.1 In some instances, a precipitating cause can be identified. Examples include arthropod bites,2,3 Borrelia infection,4–7 trauma,8 vaccinations,9–11 injected drugs or antigens for hyposensitization,12,13 acupuncture,1 gold pierced earings,14–16 tattoos,17–19 and varicella-zoster infection scars.20–22 However, in most cases, the cause remains unknown.
The clinical features depend to a certain extent on the situation in which the B-cell pseudolymphoma arises. Idiopathic cutaneous B-cell pseudolymphoma probably constitutes the largest group and is most frequent on the face (cheek, nose, earlobe) (70%), chest, and upper extremities. There is predilection for females (3 : 1), and white races are affected more often than black (9 : 1).1 B. burgdorferi is probably the commonest cause in endemic regions in Europe, although cutaneous B-cell pseudolymphoma is a rare
1483 B-cutaneous lymphoid hyperplasia
manifestation of Lyme disease, showing a prevalence of only 0.6–1.3% in patients with serological and/or clinical evidence of infection.5,23,24 Specific skin lesions usually develop within a few weeks to months of a tick bite, usually in the nipple region, genital region, or on the ear lobe (Fig. 29.254).1,7,25 They may develop de novo or arise in a background of erythema chronicum migrans.7
Whatever the cause, most patients present with solitary, small, erythematous to plum-colored or bluish plaques and nodules. Ulceration is very rare and multiple lesions uncommon. Most cases run a benign clinical course, and many resolve following removal of the causative stimulus, although in some the process is chronic and recalcitrant to treatment.1 Examples of B-CLH evolving into overt B-cell lymphoma are also well documented, and it is possible that a spectrum of disease exists.6,26–29 Follow-up of all patients is therefore advisable.
Pathogenesis and histopathological features Persistent antigenic stimulation is the presumed cause of B-CLH in cutaneous B-cell pseudolymphoma, particularly when a precipitating cause can be identified. For example, B. burgdorferi-specific DNA is present in many Borrelia-associated cases of cutaneous B-cell pseudolymphoma. Mouthparts have been identified in skin biopsies showing B-CLH developing in association with arthropod bites, and adjuvant (aluminum hydroxide) has been demonstrated at the site of vaccination-associated cutaneous B-cell pseudolymphoma.2,7,17,30 Tattoo-induced B-CLH appears to occur principally in association with red tattoo pigment and only rarely with green or blue tattoos.1,17–19 A case of B-CLH has also been documented in a patient with Sjögren syndrome, raising the possibility of autoantigenic stimulation in some cases.31 In addition, certain dendritic cell subtypes are present in greater numbers in B-CLH than cutaneous B-cell lymphomas, further implicating persistent antigenic stimulation in the pathogenesis.32–34
often reveals a diffuse, vaguely nodular infiltrate that fills the dermis and sometimes involving the subcutis (Fig. 29.255). In less florid examples, the infiltrate tends to be nodular and perivascular and periadnexal in distribution, but may still extend to the deep reticular dermis and subcutis. A grenz zone is often present, but exocytosis and spongiosis may be seen, and other epidermal changes, such as atrophy, hyperplasia, and parakeratosis, are relatively frequent.7,36,37
Histologic features reported to be relatively specific for cutaneous B-cell pseudolymphoma in the historical literature including a ‘top heavy’ distribution, do not hold up to modern-day scrutiny, especially as many of the early series mistakenly included examples of cutaneous B-cell lymphoma in their cohorts of pseudolymphoma.8,35 In fact, low-power examination
The lymphoid tissue is similar to reactive lymphoid tissue at sites where it is more usually encountered (e.g., lymph nodes, tonsils). Lymphoid follicles are almost always present. These may be primary in nature, and composed of closely packed small lymphocytes, but in most cases reactive germinal centers are also prominent.7,25,36,37 Germinal centers comprise an admixture of large centroblasts, small and large centrocytes, and tingible body macrophages. Whilst a compressed mantle of small lymphocytes is the norm in germinal centers at other sites, it is often lacking in B-CLH, particularly in cases associated with Borrelia infection.7,25,38 Reactive germinal centers have a high proliferation rate and often appear ‘zoned’, with darkly staining areas full of proliferating centroblasts and lighter zones in which centrocytes predominate (Figs 29.256 and 29.257). The interfollicular areas are populated by a polymorphic infiltrate with predominant small lymphocytes, scattered blast cells, histiocytes, plasma cells, and sometimes eosinophils.7,25,36,37
1484 Cutaneous lymphoproliferative diseases and related disorders
Lymphoid follicles can be identified immunohistochemically by antibodies marking the FDC networks (CD21, CD23, and CD35) (Fig. 29.258). Primary B-cell follicles contain a uniform population of small B lymphocytes (CD20 positive), many of which coexpress CD23 (Fig. 29.259). The germinal center B cells express CD10 and bcl-6, but lack bcl-2. T cells predominate in the interfollicular areas, although small numbers of B cells are also seen (Fig. 29.260), including a proportion of the scattered blasts (Fig. 29.260). These typically show no expression of CD10. Immunohistochemistry or in situ hybridization for light chains shows a polytypic pattern of staining for the B lymphocytes and plasma cells (Figs 29.261 and 29.262).7,25,36,37,39
PCR clonality assays most often show a polyclonal pattern of immunoglobulin gene rearrangement. However, clonality has been demonstrated in lesions otherwise typical for B-CLH.40–42
Differential diagnosis The main differential diagnoses of B-CLH are primary cutaneous marginal zone lymphoma and cutaneous follicle center lymphoma, as discussed previously in the relevant sections on these entities. Briefly, in marginal zone lymphoma there are sheets of marginal zone cells, a predominance of interfollicular B lymphocytes, and aberrant B-cell expression of CD43.36,43
Neoplastic follicles in PCFCL, or follicular lymphoma secondarily involving the skin, typically have a monotonous appearance with no zonation, relatively few tingible body macrophages and mitotic figures, and a low proliferation fraction. In secondary follicular lymphoma, the neoplastic follicles are also usually bcl-2 positive, although this is less often the case for PCFCL.37,39
1485 Cutaneous and systemic plasmacytosis
finding would normally be indicative of lymphoma, but in this situation the aggregates probably represent small cross sections of follicle centers that are devoid of mantles. A benign diagnosis is favored by the presence of numerous tingible body macrophages and an associated mixed reactive infiltrate of small lymphocytes, histiocytes, eosinophils, and plasma cells.7,38
Demonstration of monoclonality by in situ hybridization or light chain immunohistochemistry is strong evidence of lymphoma, but immunoglobulin gene rearrangement studies are less conclusive in view of the well-documented examples of clonal B-CLH.28,29,40,41 Moreover, interpretation of molecular results is further hampered by the relatively high incidence of pseudoclonality encountered when performing PCR on skin biopsies.44

Fig. 29.254 B-cutaneous lymphoid hyperplasia: the earlobe is a commonly affected site. Lesions are usually solitary. By courtesy of the Institute of Dermatology, London, UK.
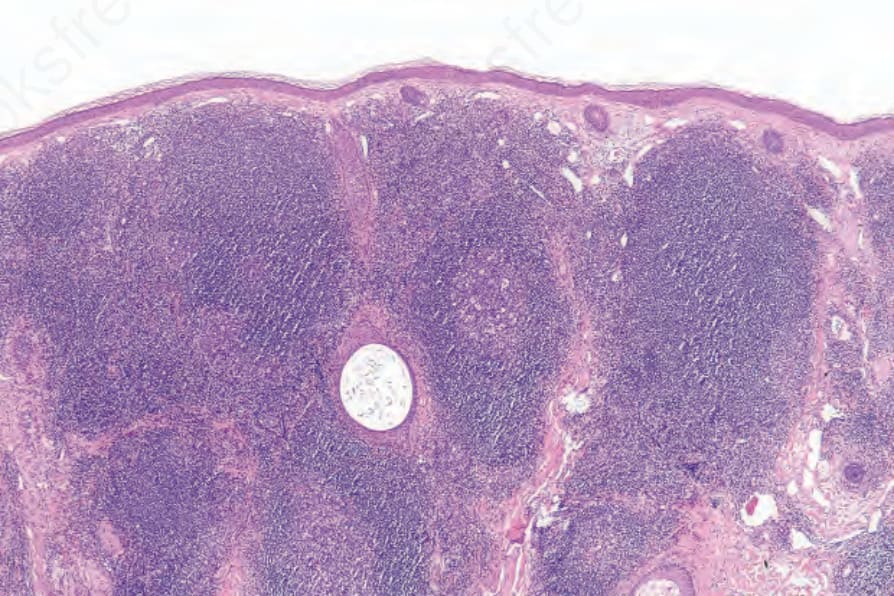
Fig. 29.255 B-cutaneous lymphoid hyperplasia: there is a dense dermal lymphoid infiltrate with conspicuous germinal centers.
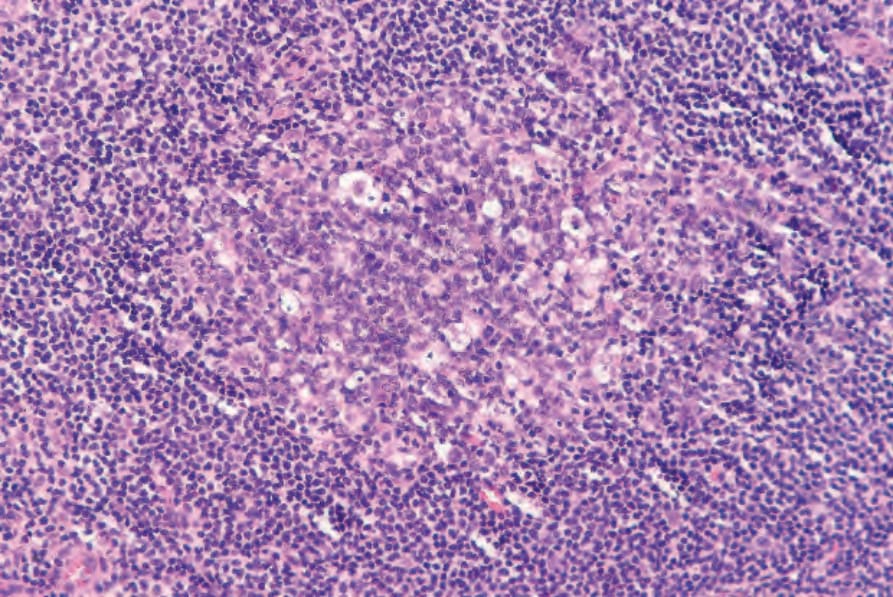
Fig. 29.256 B-cutaneous lymphoid hyperplasia: there are prominent tingible body macrophages within the germinal center.
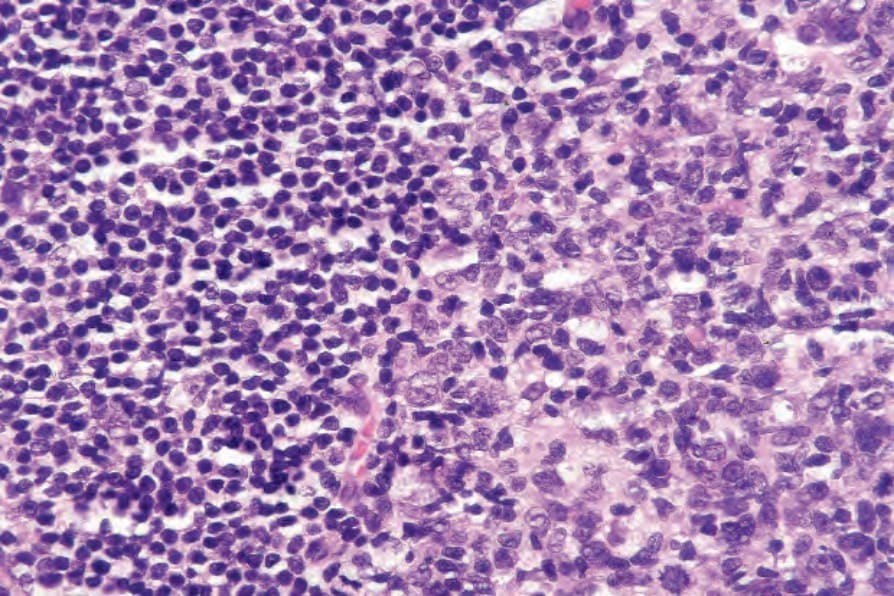
Fig. 29.257 B-cutaneous lymphoid hyperplasia: high-power view of edge of germinal center and adjacent population of mature small lymphocytes.
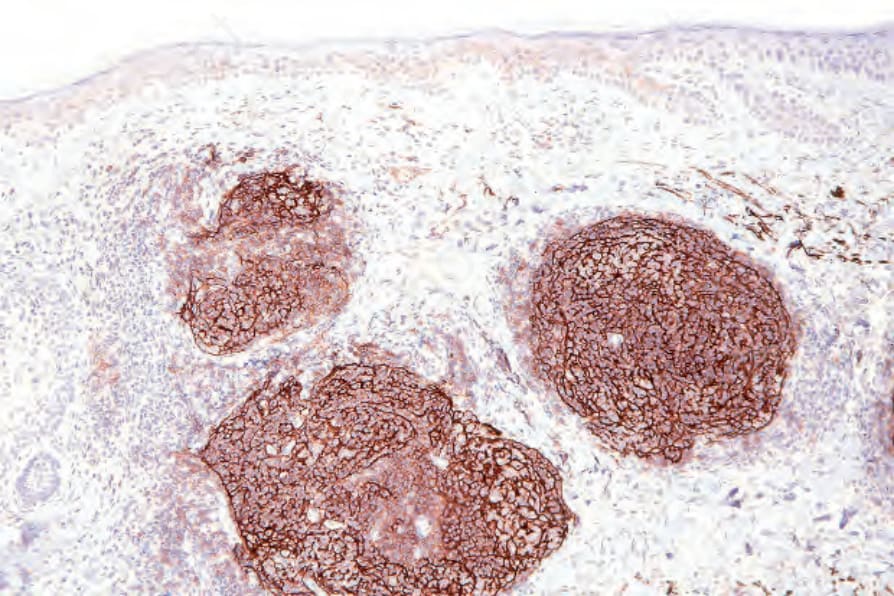
Fig. 29.258 B-cutaneous lymphoid hyperplasia: the follicular architecture is outlined by demonstration of the follicular dendritic cell population (CD21).
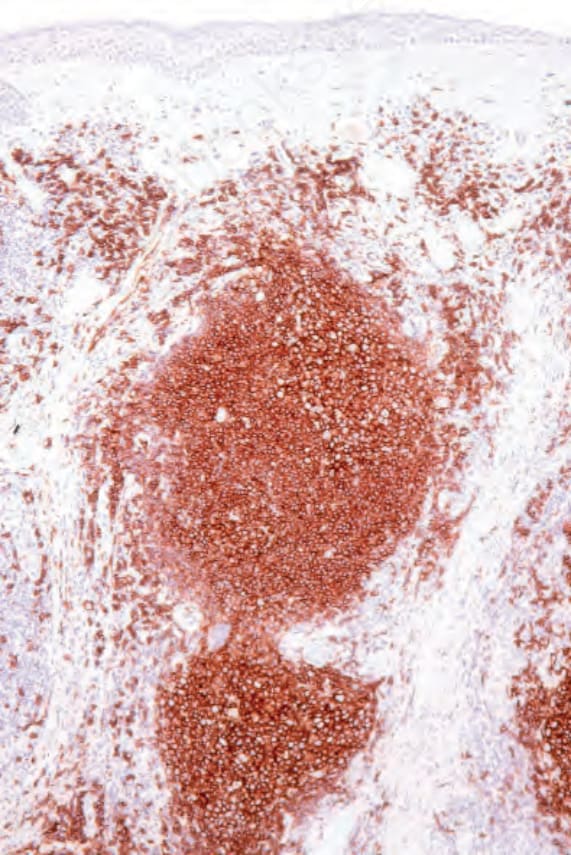
Fig. 29.259 B-cutaneous lymphoid hyperplasia: the B-cell component is outlined with CD20 immunohistochemistry.
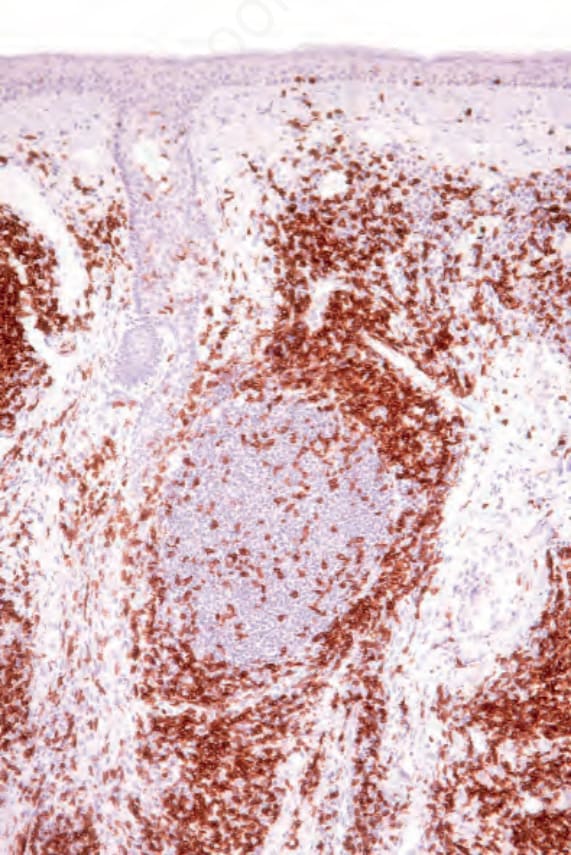
Fig. 29.260 B-cutaneous lymphoid hyperplasia: a layer of T cells (CD3) surrounds the B-cell nodules.
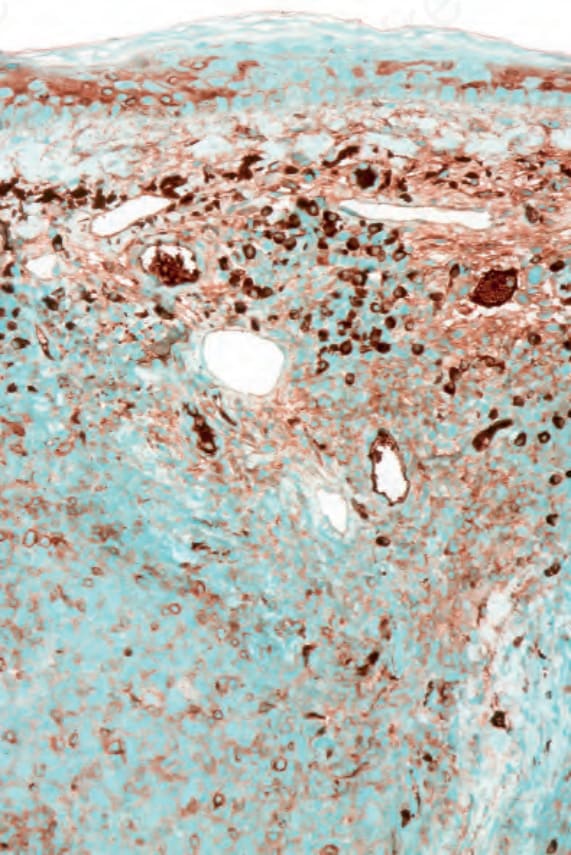
Fig. 29.261 B-cutaneous lymphoid hyperplasia: kappa plasma cells are scattered throughout the infiltrate.