淋巴瘤樣丘疹病 (Lymphomatoid Papulosis)
臨床特徵 (Clinical Features)
- 淋巴瘤樣丘疹病 (lymphomatoid papulosis) 最早於 1968 年被描述,是一種慢性、會自行癒合的皮疹。在 WHO 分類中,目前被歸類為一種惰性 (indolent) 淋巴增生性疾病 (lymphoproliferative disorder)。
- 在日本有特殊的表現型態。兒童與青少年病例占所有病例的百分之六至十。臨床表現可能令人警覺,除了一般常見的丘疹樣皮疹之外,還會快速出現大型潰瘍性病灶。然而,除此之外疾病表現屬於典型。
- Lymphomatoid papulosis 可能呈現短暫、自限性的病程,或更為遷延、持續五至十年甚至更久的病程。不論屬於何種情況,預後一般良好;僅在病灶特別多且/或在外觀上造成困擾時才需要治療。然而,有百分之九至十九的病例會合併另一種淋巴瘤,例如蕈狀肉芽腫 (mycosis fungoides)、原發性皮膚退行發育大細胞淋巴瘤 (primary cutaneous anaplastic large cell lymphoma) 或 HL(霍奇金淋巴瘤)。該淋巴瘤可能先於 lymphomatoid papulosis 出現、與其同時發生,或在其之後出現。當 lymphomatoid papulosis 的病灶侷限於 mycosis fungoides 病灶部位時,這種情況被描述為 lymphomatoid papulosis 的持續性叢集 (persistent agmination)。
- Lymphomatoid papulosis 較常發生於男性(2:1)。患者通常處於第五個十年(約五十多歲),但廣泛的年齡範圍(包括兒童)皆可能受影響。典型表現為成簇的紅斑性丘疹,直徑 0.5–1.0 cm,在三至四週的病程中發展,變得出血與壞死,然後癒合並形成萎縮性瘢痕 (atrophic scars)(圖 29.102–29.104)。臨床特徵常與急性痘瘡樣苔癬樣糠疹 (pityriasis lichenoides acuta) 重疊。其他病灶可能較大且呈結節狀,並以深層痘瘡樣瘢痕 (varioliform scars) 癒合。本病常表現於軀幹與四肢,但偶爾也會侵犯其他部位。病灶數目不一,從數個到數百個不等,並需數週至數月才會消退。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
-
致病機轉仍未確定。多數病例似乎代表 T 淋巴細胞的單株性增生 (clonal proliferations),更可能屬於調節性 T 細胞 (T-regulatory cell) 亞群。某些研究顯示有高比率的細胞凋亡 (apoptosis),可能促成病灶消退。此可能由經由細胞表面 Fas (CD95) 訊息傳遞的死亡受體途徑 (death-receptor pathway) 所媒介,及/或因促凋亡蛋白 (proapoptotic protein) bax 濃度增加所致。曾有人提出一種由 TGF-β 分泌與訊息傳遞所媒介的自分泌 (autocrine) 或旁分泌 (paracrine) 生長控制機制。TGF-β 訊息傳遞受體基因 (signaling receptor genes) 的突變會導致疾病進展。較近期,曾有人描述一種特殊的 lymphomatoid papulosis 亞群,其特徵為主要呈侷限性病灶、表現於年長患者,並與涉及 6p25.3 的染色體重排 (chromosomal rearrangements) 相關。
-
已有罕見的臨床變異型被描述。在區域型 lymphomatoid papulosis (regional lymphomatoid papulosis) 中,病灶數年間侷限於單一身體區域,且似乎在兒童較為常見。黏膜侵犯極為罕見。口腔病灶表現為反覆發作並自發消退的疼痛性潰瘍、結節,或紅斑性硬化斑塊 (erythematous indurated plaques)。已有人描述毛囊型 (follicular) 與膿疱型 (pustular) 變異型,以及一種類水皰性痘瘡樣皮膚病 (hydroa vacciniforme, HV)-like 的表現型態。
-
在合併另一種淋巴瘤的 lymphomatoid papulosis 病例中,常可證明兩者具有共同的單株身份 (common clonal identity),提示有一共同的幹細胞 (stem cell) 同時衍生出兩者。此理論受到細胞遺傳學 (cytogenetic) 發現的支持,認為具有不同組織病理與行為的不同腫瘤細胞表現型 (tumor cell phenotypes),係由一共同、隱匿性 (occult) 幹細胞的亞株 (subclones) 中累積的基因改變所衍生。
-
Lymphomatoid papulosis 患者呈現多種病理表現。認識此一譜系十分重要,因為許多所遇到的型態可能被誤認為更具侵襲性的淋巴瘤。所描述的不同類型彼此重疊,且可能在同一患者的不同切片中見到。傳統上,lymphomatoid papulosis 的不同型態被指定為亞型,並附加一個英文字母作為辨識。此種劃分相當任意,但本文仍加以遵循,以凸顯可能遇到的特定特徵範圍。
-
A 型型態 (Type A pattern)(占病例的百分之七十五至八十)由混合性、楔形 (wedge-shaped) 的真皮,極少數可局部侵犯皮下的浸潤所構成,其中含有大型退行發育細胞 (large anaplastic cells)(直徑 15–30 µm),具有多形性 (pleomorphic) 的泡狀核 (vesicular nuclei),內含明顯的核仁 (nucleoli) 與豐富的細胞質(圖 29.105–29.109)。這些細胞可能為多核,並可類似 Reed-Sternberg 細胞。有絲分裂象 (mitotic figures) 頻繁可見(圖 29.110)。在成熟病灶中,這些細胞散在分布或排列成小群集,並與嗜中性球 (neutrophils)、嗜酸性球 (eosinophils)、漿細胞 (plasma cells)、淋巴細胞與組織球 (histiocytes) 混雜。大型非典型細胞的表皮趨向性 (epidermotropism) 罕見。
-
B 型型態 (Type B pattern)(占病例的百分之五至十)以小至中型淋巴細胞為主,具有多形性、不規則且增大的核(圖 29.111 與 29.112)。浸潤在上部真皮呈帶狀 (bandlike) 分布。表皮趨向性明顯,並模擬斑塊期蕈狀肉芽腫 (plaque stage mycosis fungoides),但通常缺乏 Pautrier 微膿瘍 (Pautrier microabscesses)、暈圈 (halos) 與基底淋巴細胞柵欄 (basal lymphocytic palisades)。
-
在 C 型型態 (type C pattern)(占病例的百分之七至十)中,浸潤呈結節狀,由 A 型細胞構成的大型群集或凝聚成片 (cohesive sheets),伴隨相對少量的發炎細胞。其特徵可能與原發性皮膚退行發育大細胞淋巴瘤 (primary cutaneous anaplastic large cell lymphoma) 所見者完全相同,此二者僅能根據臨床特徵加以區分。
-
D 型 lymphomatoid papulosis (Type D) 伴隨明顯的表皮增生 (epidermal hyperplasia) 與顯著的表皮趨向性。表皮內淋巴細胞 (intraepidermal lymphocytes) 通常較 B 型病灶所見者為大,並表現 CD8 而非 CD4。然而,如 A 型與 C 型 lymphomatoid papulosis 所見的大型退行發育細胞通常不存在。
-
所謂的 E 型 lymphomatoid papulosis (Type E) 的特徵為一種血管侵襲性 (angioinvasive) 生長型態,伴隨血管壁的破壞。浸潤的淋巴細胞可能為小、中或大型,並與嗜酸性球及嗜中性球混雜。常伴有壞死。在臨床上,這些患者與典型 lymphomatoid papulosis 患者略有不同,表現為相對少數的丘疹結節 (papulonodules),進展成大型扁平潰瘍(焦痂樣,eschar-like),直徑可達 4 cm。
-
也有人提出 F 型 lymphomatoid papulosis (Type F),用於表現出明顯毛囊趨向性 (folliculotropism) 的病例,雖然此特徵在合併其他浸潤型態時並不少見。常隨之出現繼發性變化,包括毛囊黏液變性 (follicular mucinosis)、毛囊上皮增生 (hyperplasia of hair follicle epithelium)、毛囊炎 (folliculitis) 與肉芽腫性發炎 (granulomatous inflammation)。
-
近期,在少數患者中描述了一種與特定基因異常相關的 lymphomatoid papulosis 特定亞型。所有病例皆具有涉及 6p25.3 上 DUSP22-IRF4 基因座 (DUSP22-IRF4 locus) 的易位 (translocations)。這些患者表現為一至數個爆發性丘疹結節病灶,侷限於單一身體區域。切片顯示由中至大型胚母細胞 (blast cells) 構成的凝聚性結節狀真皮浸潤。其上覆的表皮顯示被小至中型淋巴細胞廣泛地定植 (colonization),常具有腦回狀 (cerebriform) 的核輪廓。可能見到類 Pautrier 微膿瘍 (Pautrier microabscess-like) 的聚集,且表皮變化常類似佩吉特樣網狀組織增生症 (pagetoid reticulosis) 所見者。
-
應注意的是,並非所有 lymphomatoid papulosis 病例都能整齊地次分類至上述變異型。在高達百分之十的病例中,單一病灶內存在兩種或更多亞型的重疊特徵;且呈現不同型態的病灶可能在同一患者的不同部位及/或不同時間出現。
-
其他特徵則為所有亞型所共有。真皮水腫 (dermal edema) 與出血 (hemorrhage) 常很明顯。某些血管可能顯示纖維蛋白 (fibrin) 沉積與阻塞。反應性表皮變化不一,取決於丘疹演變的階段。早期病灶顯示細胞間水腫 (intercellular edema) 與偶見的表皮內淋巴細胞。中期病灶的特徵為角質形成細胞 (keratinocytes) 不等程度的壞死、細胞間水腫,以及表皮內細胞(其中許多為非典型)。常可見表皮內多形核細胞 (intraepidermal polymorphs) 與紅血球 (erythrocytes)。晚期病灶的特徵為廣泛的表皮壞死、潰瘍,以及形成鱗屑狀、角化不全 (parakeratotic) 的痂皮。偶爾會出現顯著的假性上皮瘤樣增生 (pseudoepitheliomatous hyperplasia),以致可能誤診為鱗狀細胞癌 (squamous cell carcinoma) 或角化棘皮瘤 (keratoacanthoma)。
-
已描述的罕見組織學型態包括一種具有肉瘤樣 (sarcoma-like) 外觀的黏液樣變異型 (myxoid variant),以及一種汗管趨向性 (syringotropic) 的例子。
免疫組化與分子特徵 (Immunohistochemistry & Molecular Features)
- 在所有組織學型態中,非典型淋巴樣細胞表現 CLA,且通常為 CD4+ 與 CD8–,雖然偶爾會遇到 CD4–/CD8+(特別是 D 型與 E 型)、CD4–/CD8– 與 CD4+/CD8+ 的變異型。細胞毒性分子 (cytotoxic molecules),如 TIA-1、perforin 與 granzyme B,通常可被辨識,不論其 CD4/CD8 狀態如何。泛 T 細胞抗原 (pan-T-cell antigens) CD2、CD3、CD5 與 CD7 的表現不一。A 型與 C 型變異型中的退行發育細胞表現 CD45 與 CD30,但不表現 CD15 或 p80/ALK1;也可能見到 CD25 的反應性(圖 29.113)。雖然上皮膜抗原 (epithelial membrane antigen, EMA) 通常為陰性,但在某些病例中可能呈局部陽性。相反地,在 B 型病灶中,CD30 常為陰性,雖然並非總是如此。雖然較早的研究提示缺乏 CD56,但較近期則常見此分子的表現。一般而言,自然殺手 (natural killer, NK)/T 細胞來源的腫瘤通常與非常差的預後相關,但在 lymphomatoid papulosis 似乎並非如此。多數 (75–80%) lymphomatoid papulosis 病例亦對 IRF4 (MUM1) 呈陽性,但此蛋白也表現於多數原發性皮膚退行發育大細胞淋巴瘤 (primary cutaneous anaplastic large cell lymphomas),並非用於區分此一譜系兩端的有用標記。某些 lymphomatoid papulosis type D 病例表現 TCR-γ。
- 約百分之六十的病例可偵測到 TCR 基因重排 (TCR gene rearrangements)。
鑑別診斷 (Differential Diagnosis)
- CD30 的表現並非可靠的區別指標,無法用於區分皮膚 CD30+ T 細胞淋巴增生性疾病 (cutaneous CD30+ T-cell lymphoproliferative disorders) 與反應性發炎性皮膚病或其他類型的淋巴瘤。越來越多的感染性皮膚病已被證明含有大量 CD30+ 細胞,並模擬 lymphomatoid papulosis。這些包括各種病毒感染的皮膚病灶,包括 herpes virus、傳染性軟疣 (molluscum contagiosum)、parapox virus(擠奶者結節,milker’s nodule)、EBV、HTLV-1 與 HIV。疥瘡 (scabies)、梅毒 (syphilis) 與淺表性黴菌感染 (superficial fungal infections) 的病灶也可能含有 CD30+ 細胞。非感染性皮膚發炎性病程,例如急性痘瘡樣苔癬樣糠疹 (pityriasis lichenoides et varioliformis acuta)、異位性皮膚炎 (atopic dermatitis) 與藥物反應(特別是對抗痙攣藥 anticonvulsants 的反應),也可能含有少量 CD30+ 細胞。淋巴細胞恢復性皮膚疹 (cutaneous eruption of lymphocyte recovery) 也可能含有 CD30+ 細胞。
- 在這些疾病中的多數,CD30+ 細胞缺乏退行發育特徵,且數量較 lymphomatoid papulosis 為少。它們也傾向於散在分布,而非呈小群集,但這並非總是如此。然而,密切的臨床病理對照 (clinicopathological correlation) 仍屬必要。
- 表現出表皮趨向性的 B 型與 D 型 lymphomatoid papulosis,可能無法根據病理特徵與其他表皮趨向性淋巴瘤(如 mycosis fungoides,包括 pagetoid reticulosis)及原發性皮膚 CD8 陽性侵襲性表皮趨向性 T 細胞淋巴瘤 (primary cutaneous CD8-positive aggressive epidermotropic T-cell lymphoma) 加以區分。在此種情況下,診斷有賴於臨床特徵。
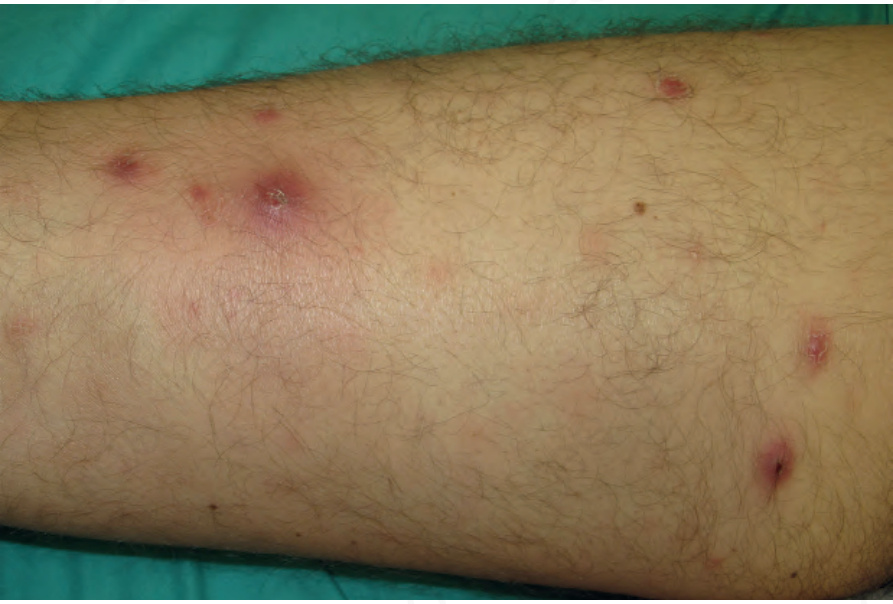
圖 29.102:淋巴瘤樣丘疹病 (lymphomatoid papulosis):四肢上多個大小不一的丘疹。Courtesy of Dr Teresa Estrach Panella, Barcelona, Spain。
Fig. 29.102 Lymphomatoid papulosis: multiple variably sized papules on a limb. Courtesy of Dr Teresa Estrach Panella, Barcelona, Spain.

圖 29.103:淋巴瘤樣丘疹病 (lymphomatoid papulosis):紅斑性丘疹的近觀。By courtesy of R.A. Johnson, MD, Massachusetts General Hospital, Harvard Medical School, Boston, USA。
Fig. 29.103 Lymphomatoid papulosis: close-up view of erythematous papules. By courtesy of R.A. Johnson, MD, Massachusetts General Hospital, Harvard Medical School, Boston, USA.

圖 29.104:淋巴瘤樣丘疹病 (lymphomatoid papulosis):在此例中,病灶位於頸部。By courtesy of the Institute of Dermatology, London, UK。
Fig. 29.104 Lymphomatoid papulosis: in this example, lesions are present on the neck. By courtesy of the Institute of Dermatology, London, UK.
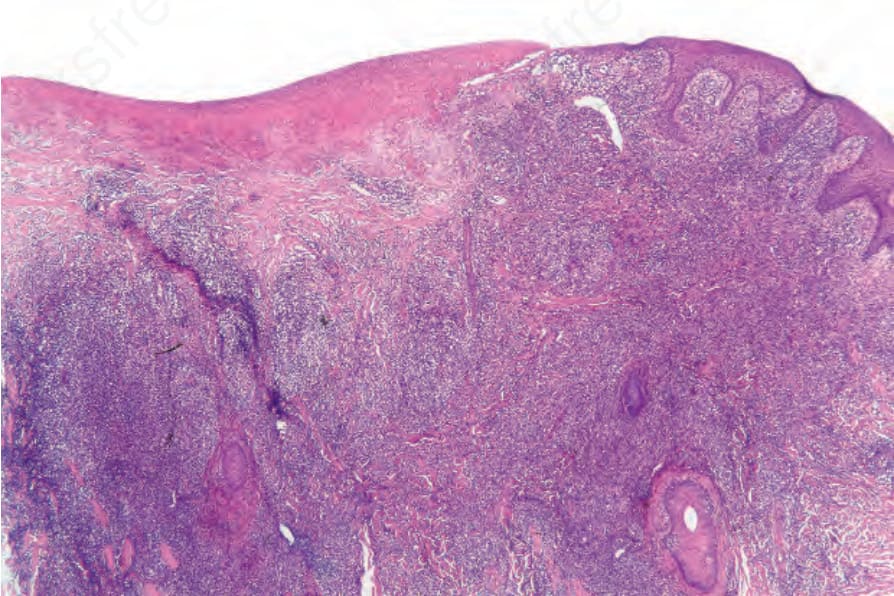
圖 29.105:淋巴瘤樣丘疹病 (lymphomatoid papulosis):低倍視野顯示潰瘍與緻密的真皮浸潤 (dense dermal infiltrate)。
Fig. 29.105 Lymphomatoid papulosis: low-power view showing ulceration and a dense dermal infiltrate.
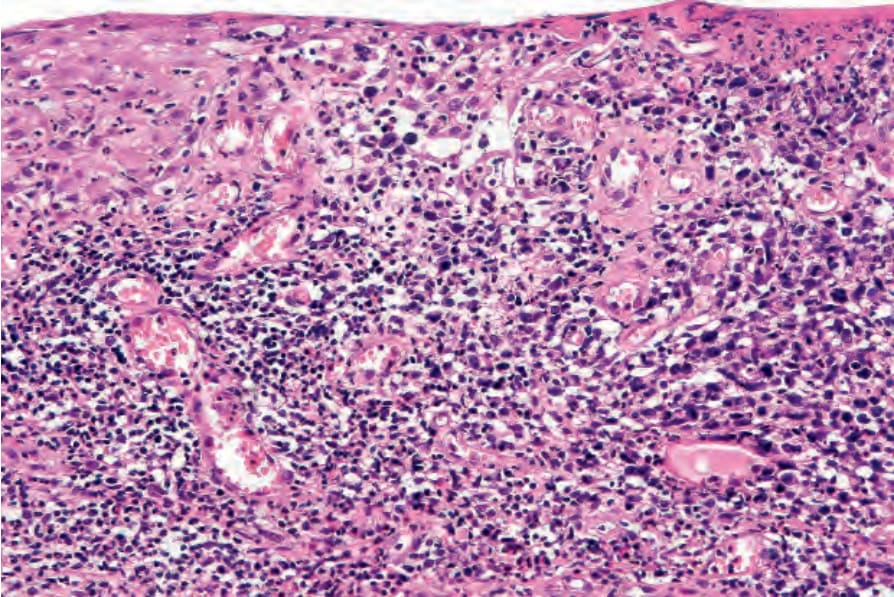
圖 29.106:淋巴瘤樣丘疹病 (lymphomatoid papulosis):表皮被非典型多形性淋巴細胞 (atypical pleomorphic lymphocytes) 浸潤。
Fig. 29.106 Lymphomatoid papulosis: the epidermis is infiltrated by atypical pleomorphic lymphocytes.
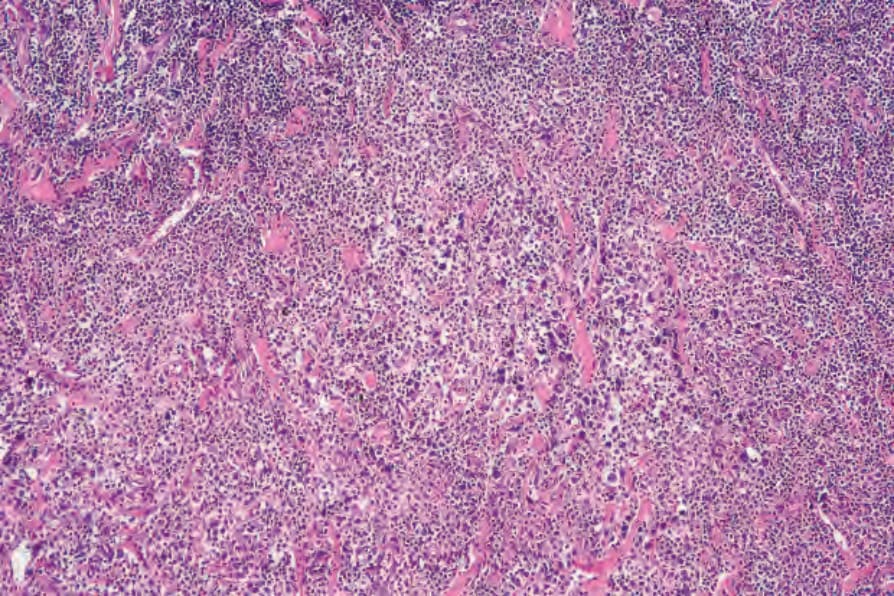
圖 29.107:淋巴瘤樣丘疹病 (lymphomatoid papulosis):緻密的真皮浸潤。即使在此倍率下,細胞學上的非典型性 (cytological atypia) 也很明顯。
Fig. 29.107 Lymphomatoid papulosis: dense dermal infiltrate. Even at this magnification, the cytological atypia is obvious.
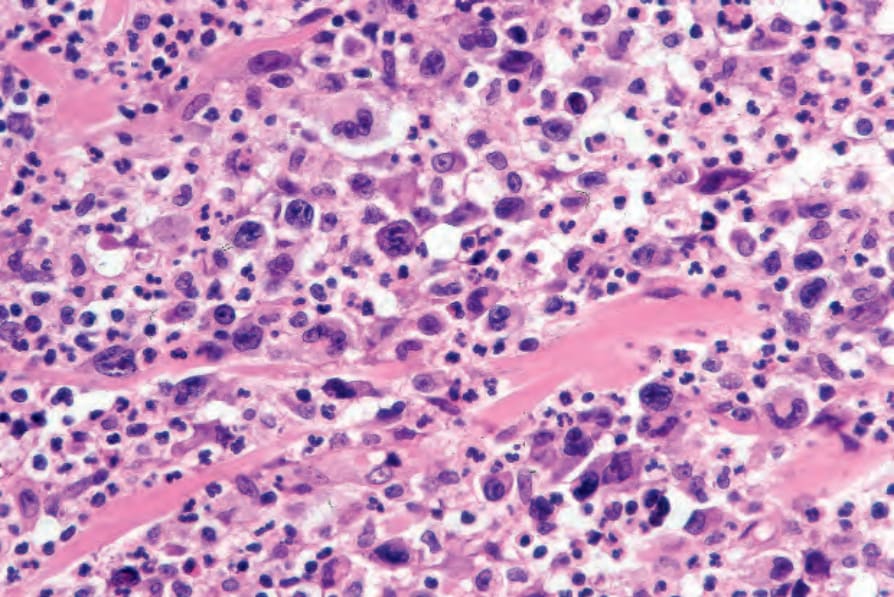
圖 29.108:淋巴瘤樣丘疹病 (lymphomatoid papulosis):淋巴細胞具有高度不規則、深染 (hyperchromatic) 或泡狀的核。注意背景中的嗜中性球 (neutrophils) 群。
Fig. 29.108 Lymphomatoid papulosis: the lymphocytes have highly irregular hyperchromatic or vesicular nuclei. Note the background population of neutrophils.
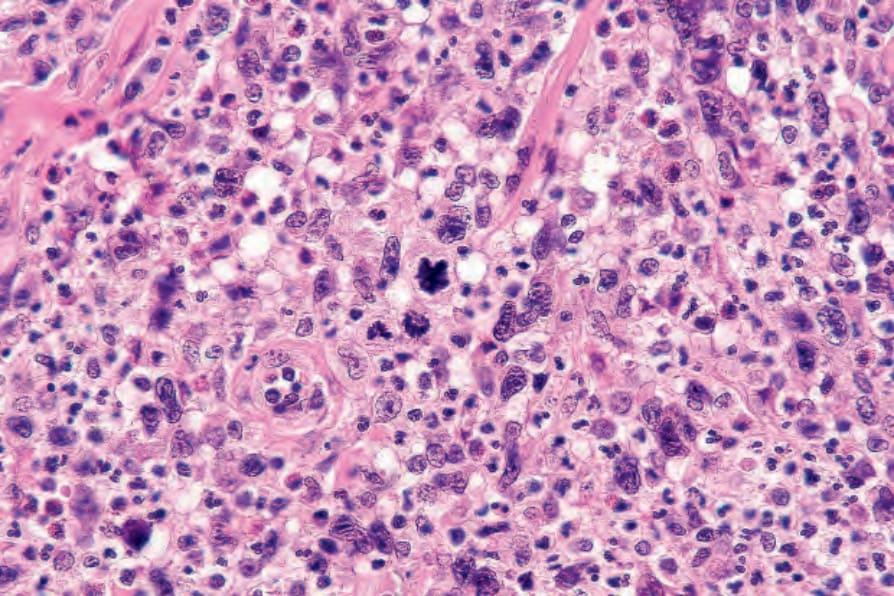
圖 29.109:淋巴瘤樣丘疹病 (lymphomatoid papulosis):可見多個有絲分裂象 (mitotic figures)。
Fig. 29.109 Lymphomatoid papulosis: multiple mitotic figures are present.
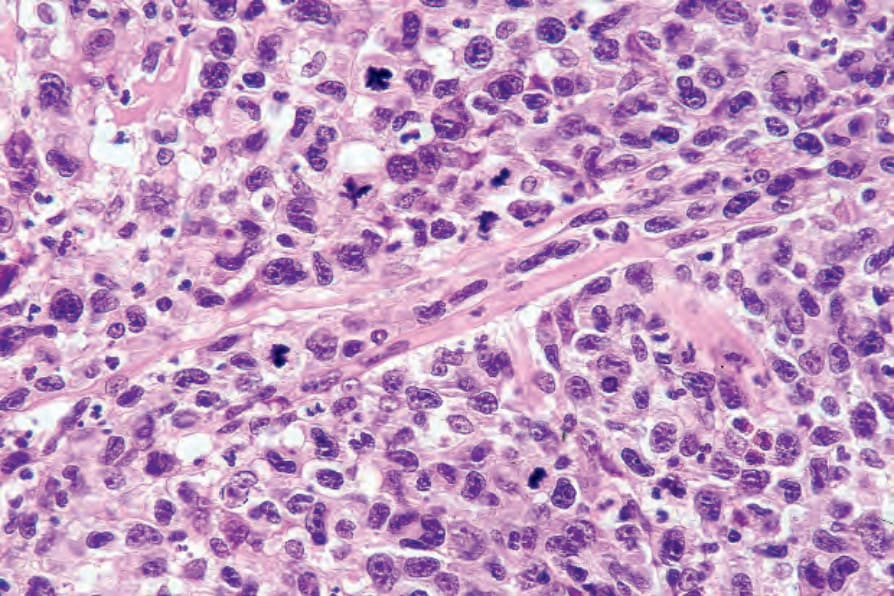
圖 29.110:淋巴瘤樣丘疹病 (lymphomatoid papulosis):在視野中央上方可見一個非典型有絲分裂象 (atypical mitosis)。
Fig. 29.110 Lymphomatoid papulosis: an atypical mitosis is seen just above the center of the field.
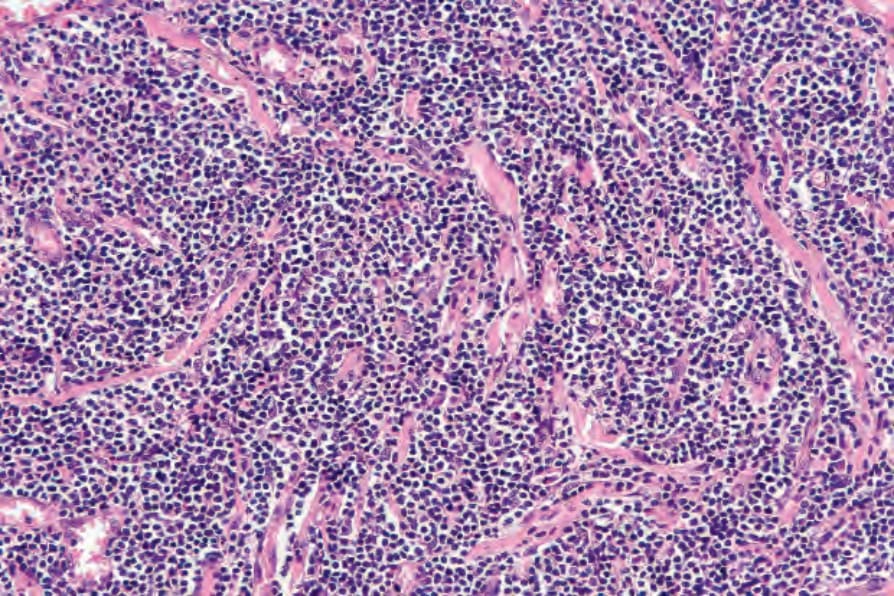
圖 29.111:淋巴瘤樣丘疹病 (lymphomatoid papulosis):可見緻密的 B 型細胞 (type B cells) 浸潤。
Fig. 29.111 Lymphomatoid papulosis: there is a dense infiltrate of type B cells.
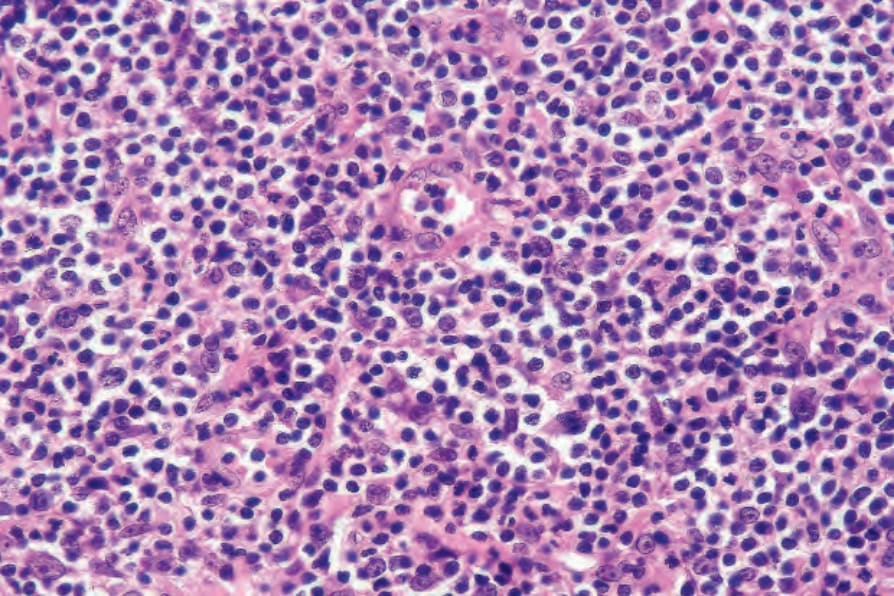
圖 29.112:淋巴瘤樣丘疹病 (lymphomatoid papulosis):B 型細胞 (type B cells) 具有增大、不規則的深染核 (hyperchromatic nuclei) 與稀少的細胞質,令人聯想到 mycosis 細胞。
Fig. 29.112 Lymphomatoid papulosis: the type B cells have enlarged, irregular hyperchromatic nuclei and scanty cytoplasm reminiscent of mycosis cells.
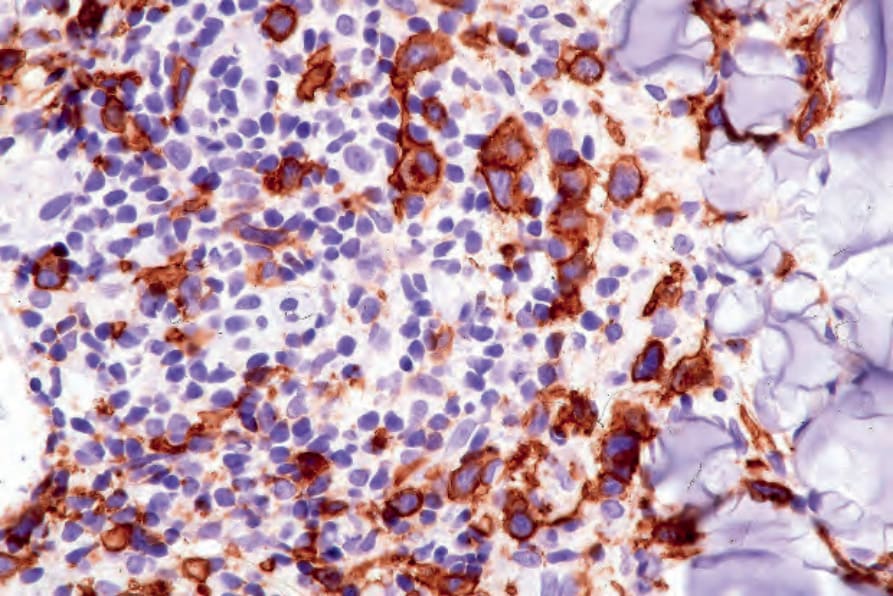
圖 29.113:淋巴瘤樣丘疹病 (lymphomatoid papulosis):可見眾多 CD30+ 細胞。
Fig. 29.113 Lymphomatoid papulosis: numerous CD30+ cells are present.

圖 29.114:原發性皮膚退行發育大細胞淋巴瘤 (primary cutaneous anaplastic large cell lymphoma):前額上紅斑性、潰瘍性的腫瘤結節。By courtesy of the Institute of Dermatology, London, UK。
Fig. 29.114 Primary cutaneous anaplastic large cell lymphoma: erythematous, ulcerated tumor nodule on the forehead. By courtesy of the Institute of Dermatology, London, UK.

圖 29.115:原發性皮膚退行發育大細胞淋巴瘤 (primary cutaneous anaplastic large cell lymphoma):前臂上大型潰瘍性結節。Courtesy of Dr Teresa Estrach Panella, Barcelona, Spain。
Fig. 29.115 Primary cutaneous anaplastic large cell lymphoma; large ulcerated nodule on the forearm. Courtesy of Dr Teresa Estrach Panella, Barcelona, Spain.