佩吉特樣網狀細胞增生症 (Pagetoid Reticulosis)
臨床特徵 (Clinical Features)
- 佩吉特樣網狀細胞增生症 (pagetoid reticulosis, PR) 罕見,特徵為局部性病灶,以及顯著的腫瘤性淋巴球於表皮內增生 (intraepidermal proliferation of neoplastic lymphocytes)。
- 在歷史上,局部型 (localized) 與瀰漫型 (disseminated) 的 pagetoid reticulosis 曾分別以 Woringer-Kolopp disease 及 Ketron-Goodman disease 之名描述。然而,多數瀰漫型 pagetoid reticulosis 案例很可能代表的是侵襲性 CD8 陽性嗜表皮性皮膚 T 細胞淋巴瘤 (aggressive epidermotropic CD8-positive cutaneous T-cell lymphoma)、皮膚 γ/δ T 細胞淋巴瘤 (cutaneous γ/δ T-cell lymphoma),或腫瘤期蕈狀肉芽腫 (tumor stage mycosis fungoides) 的例子;因此 pagetoid reticulosis 一詞應僅保留給此病的局部型。
- 多數案例表現為單一的紅斑性病灶,典型上會緩慢擴大,形成厚斑塊或局部成群的斑塊,其演變過程往往歷時多年。本病明顯好發於肢端 (extremities)。斑塊傾向有鱗屑,且邊界清楚分明 (Fig. 29.86)。病灶直徑可達 30 cm。潰瘍 (ulceration)、疣狀變化 (verrucosity) 與腫瘤形成 (tumor formation) 為常見的併發症。
- 這些病灶在臨床上很容易被誤診為 Bowen disease 的斑塊、表淺型基底細胞癌 (superficial basal cell carcinoma)、錢幣狀濕疹 (discoid eczema)、psoriasis,甚至乳房外佩吉特病 (extramammary Paget disease)。局部淋巴結 (regional lymph nodes) 可能腫大,但組織學上僅顯示反應性變化 (reactive changes)。本病通常呈惰性病程 (indolent course),對切除 (excision) 或放射治療 (radiotherapy) 有反應。然而,於原處或遠處復發並不少見。偶有案例對治療相對抗拒,並以較為進展性的方式表現。因此建議進行長期追蹤。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
- 組織學上,PR 的特徵為幾乎完全位於表皮內的非典型單核細胞浸潤 (intraepidermal infiltrate of atypical mononuclear cells)。偶有報告記載腫瘤細胞表現 CLA 與 αEβ7 (CD103;一種與上皮細胞上 E-cadherin 結合的黏附分子),提示黏附分子 (adhesion molecules) 在此病特徵性的極度嗜表皮性 (epidermotropism) 中扮演重要角色。
- 表皮顯示角化過度 (hyperkeratosis) 及/或角化不全 (parakeratosis),並伴隨棘層肥厚 (acanthosis),後者常呈乾癬樣 (psoriasiform) 外觀。表皮(尤其是其下層部位)被中至大型淋巴球浸潤,這些細胞具有大而不規則的細胞核,以及豐富的空泡化細胞質 (vacuolated cytoplasm) (Figs 29.87–29.90)。核周暈 (perinuclear halo) 常見。
- 這些細胞可呈單細胞瀰漫性分布 (single-cell diffuse distribution)、呈現類 Pautrier 微膿瘍 (Pautrier microabscess-like) 的構形,或存在於大型腔隙 (large lacunae) 中。有絲分裂象 (mitotic figures) 有時相當明顯。附屬器上皮 (adnexal epithelium) 受侵犯常為一項特徵。表淺真皮含有血管周圍淋巴組織球性浸潤 (perivascular lymphohistiocytic infiltrate),但非典型細胞非常稀疏或缺如。
- PR 代表一種 CD45+ 造血細胞 (hematopoietic cells) 的增殖性病灶,這些細胞源自 T 細胞。它們表現全 T 細胞抗原 (pan-T-cell antigens) CD2、CD3 與 CD5,但 CD7 常喪失或下調 (Fig. 29.91)。T 輔助型 (CD4+) 與 T 抑制/細胞毒型 (CD8+) 兩種表型皆曾被報告。雖然亦曾有 CD4/CD8 雙陰性 (double negative) 型的描述,但此類案例可能代表 γ/δ T 細胞淋巴瘤的例子。部分作者曾記載 CD45RO (UCHL-1,一種記憶 T 細胞標記) 的喪失。CD30 (>50%) 與 Ki-67 (50%) 的高度表現亦可被證實。真皮浸潤由免疫表型正常的 T 細胞 (CD4+/CD8– 與 CD4–/CD8+) 組成,並混雜 B 細胞與巨噬細胞 (macrophages)。亦曾注意到角質形成細胞 (keratinocyte) 的 HLA-DR 表現。多數受測案例顯示 TCR 基因重排 (TCR gene rearrangement) 的單株性型態 (monoclonal pattern)。
鑑別診斷 (Differential Diagnosis)
- Pagetoid reticulosis 應與掌蹠蕈狀肉芽腫 (mycosis fungoides palmaris et plantaris) 區別。後者一律為 CD4+ 表型,臨床上以薄斑塊為特徵,與 PR 增厚且常呈疣狀的病灶形成對比。組織學上的區別主要依據後者(PR)存在顯著的嗜表皮性。
- 主要的鑑別診斷對象為原發性皮膚 CD8 陽性侵襲性嗜表皮性細胞毒性 T 細胞淋巴瘤 (primary cutaneous CD8-positive aggressive epidermotropic cytotoxic T-cell lymphoma)。其區別主要為臨床上的,因為後者為侵襲性疾病,伴有廣泛的皮膚病灶及不良預後。組織學上兩者外觀完全相同,但有若干 pagetoid reticulosis 案例具有 CD4 表型。然而,primary cutaneous CD8-positive aggressive epidermotropic cytotoxic T-cell lymphoma 傾向顯示較顯著的真皮浸潤。

圖 29-82:黏蛋白性禿髮 (alopecia mucinosa):眉部受侵犯顯示禿髮 (alopecia)。承蒙英國倫敦皮膚科研究所 (Institute of Dermatology, London, UK) 提供。
Fig. 29.82 Alopecia mucinosa: eyebrow involvement showing alopecia. By courtesy of the Institute of Dermatology, London, UK.
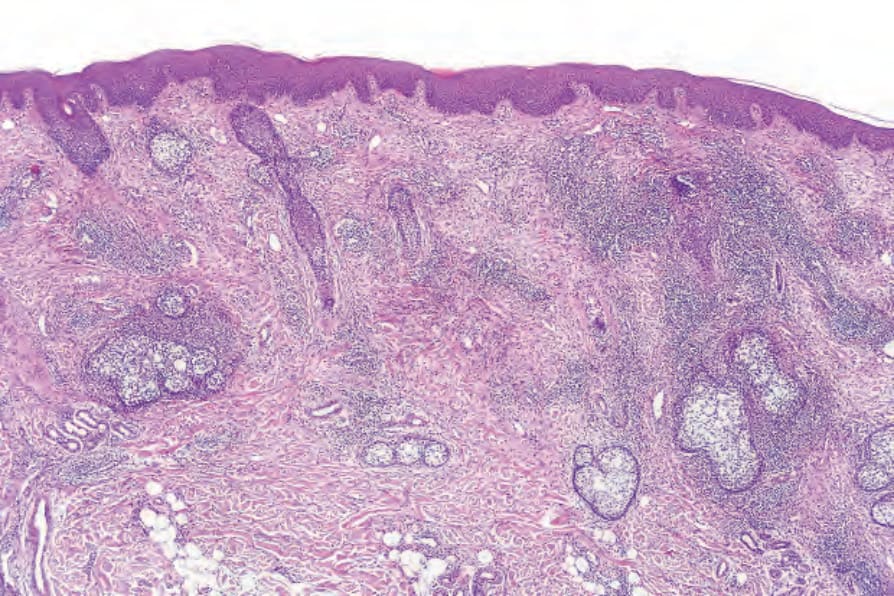
圖 29-83:黏蛋白性禿髮 (alopecia mucinosa):低倍視野顯示顯著的毛囊周圍浸潤 (perifollicular infiltrate)。此病人並無合併蕈狀肉芽腫 (mycosis fungoides),且此病灶之致病機轉未明。
Fig. 29.83 Alopecia mucinosa: low-power view showing a striking perifollicular infiltrate. The patient did not have associated mycosis fungoides and the pathogenesis of this lesion is unknown.
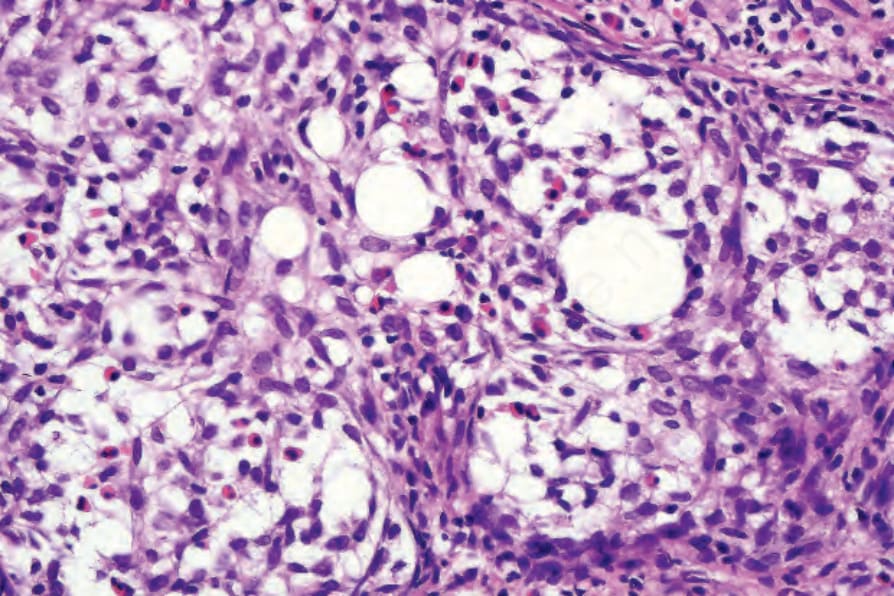
圖 29-84:黏蛋白性禿髮 (alopecia mucinosa):有毛囊黏蛋白沉積 (follicular mucinosis),並伴隨大量嗜酸性球浸潤 (eosinophil infiltrate)。
Fig. 29.84 Alopecia mucinosa: there is follicular mucinosis associated with a heavy eosinophil infiltrate.
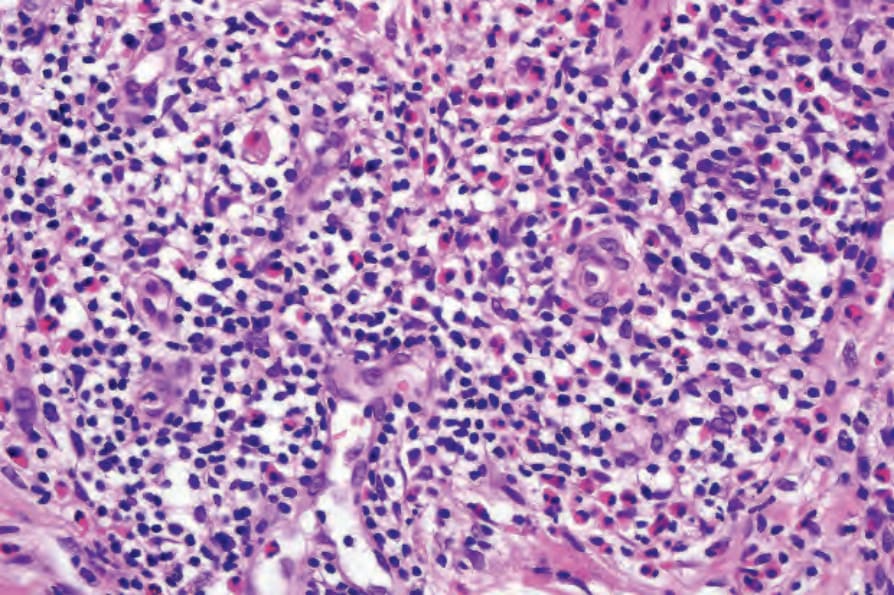
圖 29-85:黏蛋白性禿髮 (alopecia mucinosa):真皮內有緻密的淋巴組織球性與嗜酸性球浸潤 (dense lymphohistiocytic and eosinophil infiltrate)。並無非典型淋巴球 (atypical lymphocytes)。
Fig. 29.85 Alopecia mucinosa: within the dermis is a dense lymphohistiocytic and eosinophil infiltrate. There are no atypical lymphocytes.
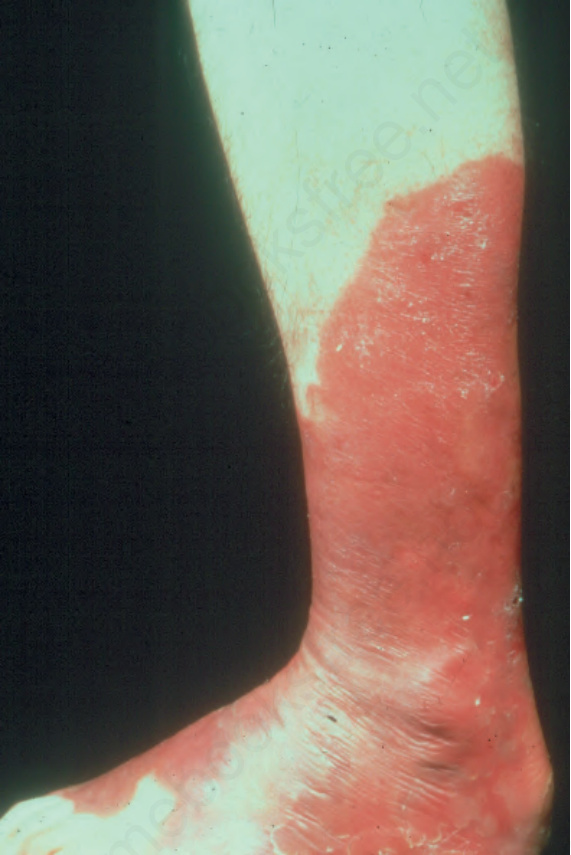
圖 29-86:佩吉特樣網狀細胞增生症 (pagetoid reticulosis):此廣泛的紅斑性病灶顯示鱗屑與清楚分明的邊界。承蒙 M.M. Black, MD,英國倫敦皮膚科研究所 (Institute of Dermatology, London, UK) 提供。
Fig. 29.86 Pagetoid reticulosis: this extensive erythematous lesion shows scaling and a sharply demarcated border. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.

圖 29-87:佩吉特樣網狀細胞增生症 (pagetoid reticulosis):掃描視野顯示特徵性的乾癬樣增生 (psoriasiform hyperplasia)。
Fig. 29.87 Pagetoid reticulosis: scanning view showing characteristic psoriasiform hyperplasia.
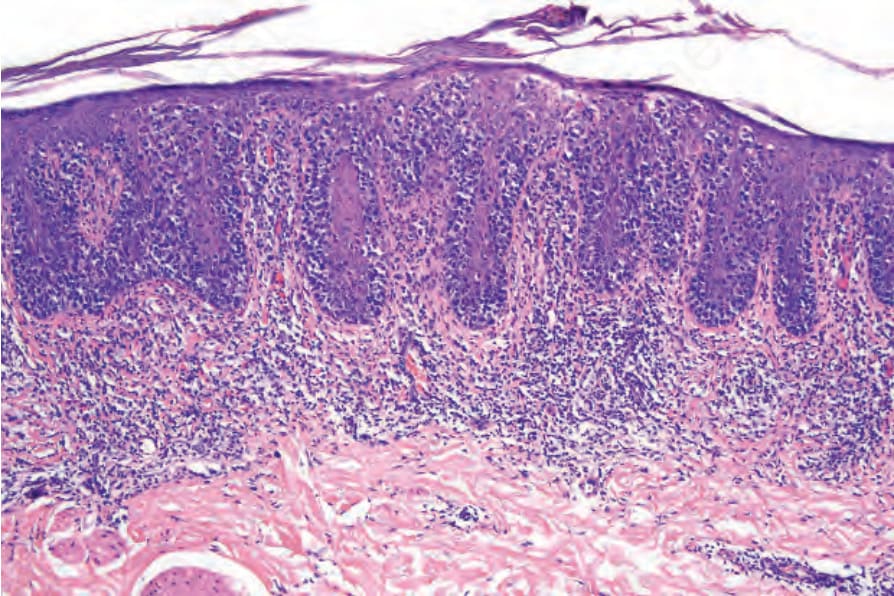
圖 29-88:佩吉特樣網狀細胞增生症 (pagetoid reticulosis):非典型單核細胞 (atypical mononuclear cells) 主要見於延長的表皮突 (epidermal ridges) 之下方部位。
Fig. 29.88 Pagetoid reticulosis: atypical mononuclear cells are predominantly seen in the lower aspects of the elongated epidermal ridges.
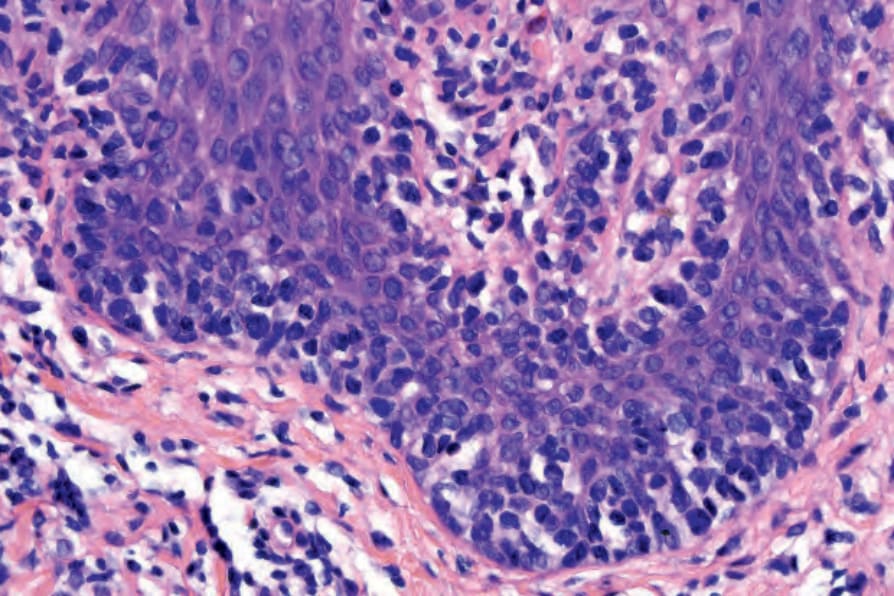
圖 29-89:佩吉特樣網狀細胞增生症 (pagetoid reticulosis):嗜表皮性 (epidermotropism) 的高倍視野。
Fig. 29.89 Pagetoid reticulosis: high-power view of epidermotropism.
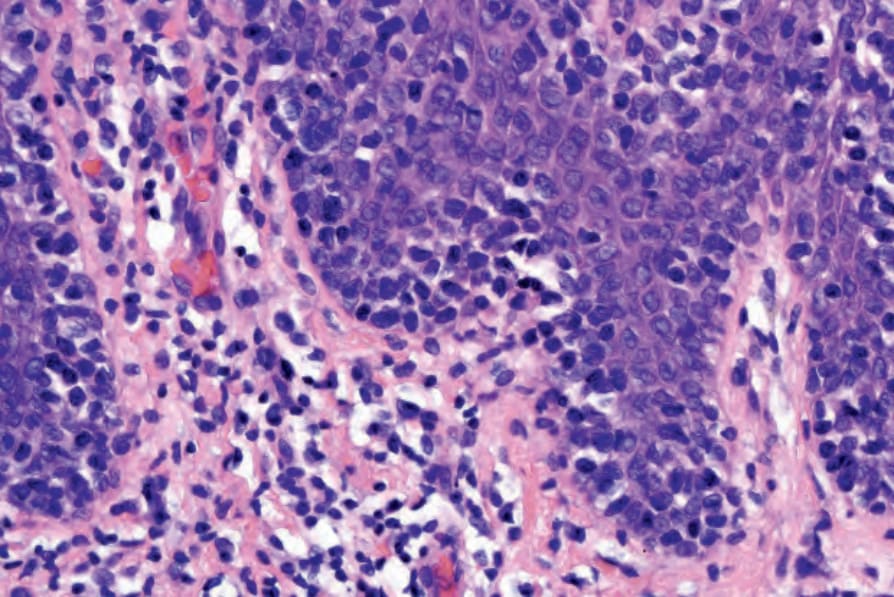
圖 29-90:佩吉特樣網狀細胞增生症 (pagetoid reticulosis):注意非典型淋巴球 (atypical lymphocytes) 大致侷限於表皮。
Fig. 29.90 Pagetoid reticulosis: note that the atypical lymphocytes are largely restricted to the epidermis.
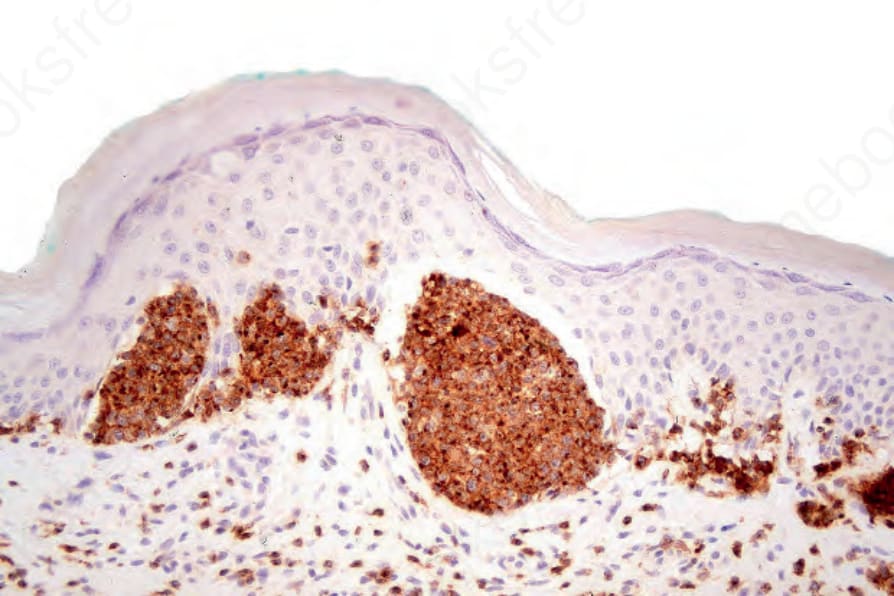
圖 29-91:佩吉特樣網狀細胞增生症 (pagetoid reticulosis):如本例所示,非典型淋巴球 (atypical lymphocytes) 可用 CD2 突顯出來。
Fig. 29.91 Pagetoid reticulosis: the atypical lymphocytes can be highlighted with CD2 as shown in this example.