Pagetoid reticulosis
Pagetoid reticulosis
Clinical features Pagetoid reticulosis (PR) is rare and characterized by localized lesions and a prominent intraepidermal proliferation of neoplastic lymphocytes.1
1428 Cutaneous lymphoproliferative diseases and related disorders
Historically, localized and disseminated forms of pagetoid reticulosis have been described under the names Woringer-Kolopp disease and Ketron- Goodman disease, respectively. However, most cases of disseminated pagetoid reticulosis are likely to represent examples of aggressive epidermotropic CD8-positive cutaneous T-cell lymphoma, cutaneous γ/δ T-cell lymphoma, or tumor stage mycosis fungoides, and the term pagetoid reticulosis should be reserved only for the localized form of the disease.1,2
Most cases present as a solitary, erythematous lesion which typically enlarges slowly to form a thick plaque or localized group of plaques, with evolution often taking many years. There is a marked predilection for the extremities. Plaques tend to be scaly and have sharply demarcated borders (Fig. 29.86). They can measure up to 30 cm in diameter.3 Ulceration, verrucosity, and tumor formation are frequent complications. The lesions can
1429 Distinct variants of mycosis fungoides
easily be clinically misdiagnosed as a plaque of Bowen disease, superficial basal cell carcinoma, discoid eczema, psoriasis, or even extramammary Paget disease.4 Regional lymph nodes may be enlarged, although histologically they show reactive changes only. The disorder usually has an indolent course and responds to excision or radiotherapy. However, recurrences either at the same or a distant site are not uncommon. Occasional cases are relatively resistant to therapy and behave in a more progressive fashion. Prolonged follow-up is therefore advisable.3
may adopt a single-cell diffuse distribution, show Pautrier microabscess-like configurations, or be present in large lacunae. Mitotic figures are sometimes conspicuous. Involvement of adnexal epithelium is often a feature. The superficial dermis contains a perivascular lymphohistiocytic infiltrate, but atypical cells are very sparse or absent.3,7
PR represents a proliferative lesion of CD45+ hematopoietic cells that are of T-cell derivation. They show expression of the pan-T-cell antigens CD2, CD3, and CD5, but CD7 is frequently lost or down-regulated (Fig. 29.91).3,6,8,9 Both T-helper (CD4+) and T-suppressor/cytotoxic (CD8+) phenotypes have been reported.6,8–11 Although CD4/CD8 double negative forms have also been described, such cases may represent examples of γ/δ T-cell lymphomas.4,8,12–14 Loss of CD45RO (UCHL-1), a marker of memory T cells, has been documented by some authors.3,8,14 High levels of expression of CD30 (>50%) and Ki-67 (50%) may be demonstrated.3,8,9 The dermal infiltrate consists of immunophenotypically normal T cells (CD4+/CD8– and CD4–/CD8+) with an admixture of B cells and macrophages.6 Keratinocyte HLA-DR expression has been noted.7 Most cases tested show a monoclonal pattern of TCR gene rearrangement.3,5,9,12
Pathogenesis and histologic features Histologically, PR is characterized by an almost completely intraepidermal infiltrate of atypical mononuclear cells. Occasional reports documenting expression of CLA and αEβ7 (CD103; an adhesion molecule that binds to E-cadherin on epithelial cells) by the tumor cells suggest an important role for adhesion molecules in the extreme epidermotropism characteristic of this condition.5,6
The epidermis shows hyperkeratosis and/or parakeratosis in association with acanthosis, which often adopts a psoriasiform appearance. The epithelium is infiltrated (particularly in the lower reaches) by medium to large lymphocytes with large and irregular nuclei, and abundant vacuolated cytoplasm (Figs 29.87–29.90). A perinuclear halo is commonly present. The cells
Differential diagnosis Pagetoid reticulosis should be distinguished from mycosis fungoides palmaris et plantaris. The latter is invariably of a CD4+ phenotype and is
1430 Cutaneous lymphoproliferative diseases and related disorders
clinically characterized by thin plaques in contrast to the thickened and often verrucous lesions of PR. Histologic distinction is mainly based in the presence of prominent epidermotropism in the latter. The main differential diagnosis is with primary cutaneous CD8-positive aggressive epidermotropic cytotoxic T-cell lymphoma. The distinction is mainly clinical as in the latter the disease is aggressive with widespread cutaneous lesions and poor prognosis. Histologically, the appearances are identical, but a number of cases of pagetoid reticulosis have a CD4 phenotype. However, primary cutaneous CD8-positive aggressive epidermotropic cytotoxic T-cell lymphoma tends to display a more prominent dermal infiltrate.

Fig. 29.82 Alopecia mucinosa: eyebrow involvement showing alopecia. By courtesy of the Institute of Dermatology, London, UK.
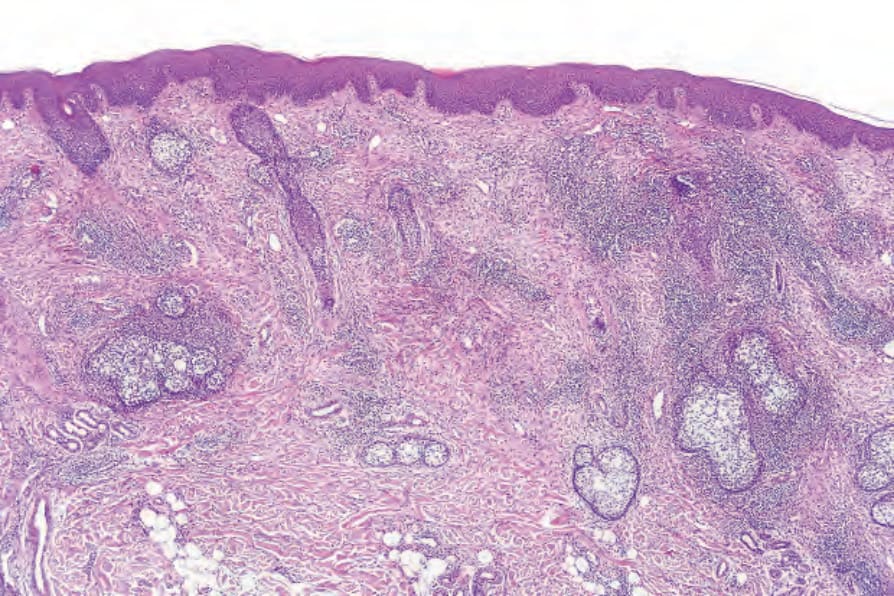
Fig. 29.83 Alopecia mucinosa: low-power view showing a striking perifollicular infiltrate. The patient did not have associated mycosis fungoides and the pathogenesis of this lesion is unknown.
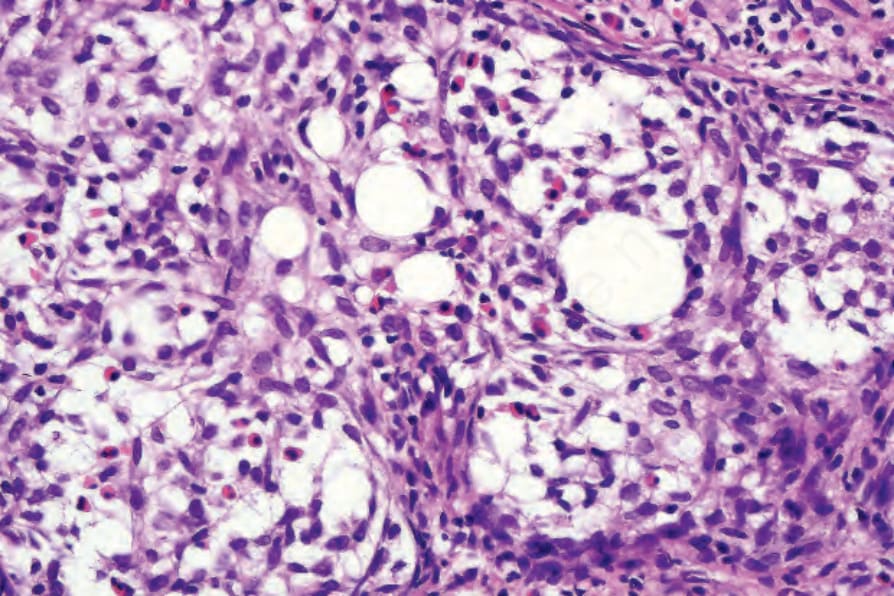
Fig. 29.84 Alopecia mucinosa: there is follicular mucinosis associated with a heavy eosinophil infiltrate.
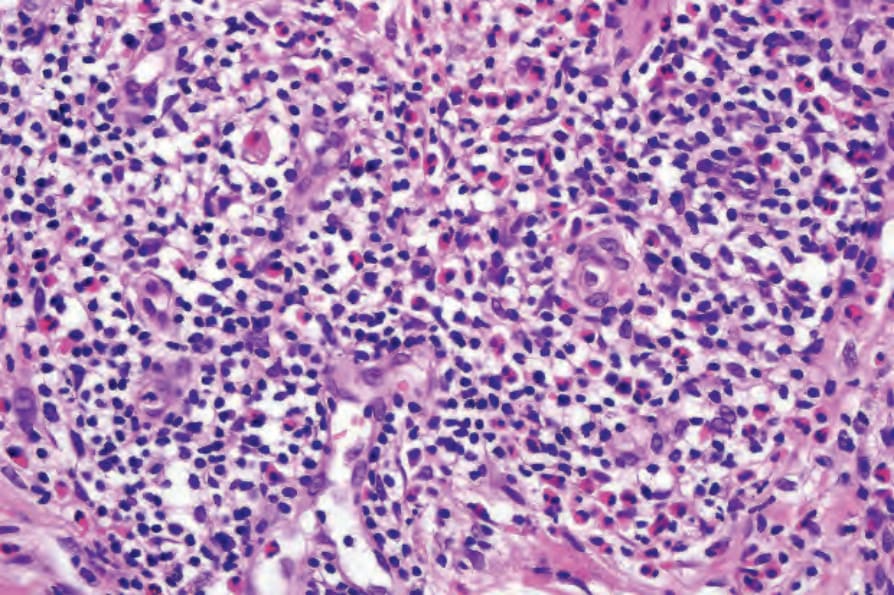
Fig. 29.85 Alopecia mucinosa: within the dermis is a dense lymphohistiocytic and eosinophil infiltrate. There are no atypical lymphocytes.
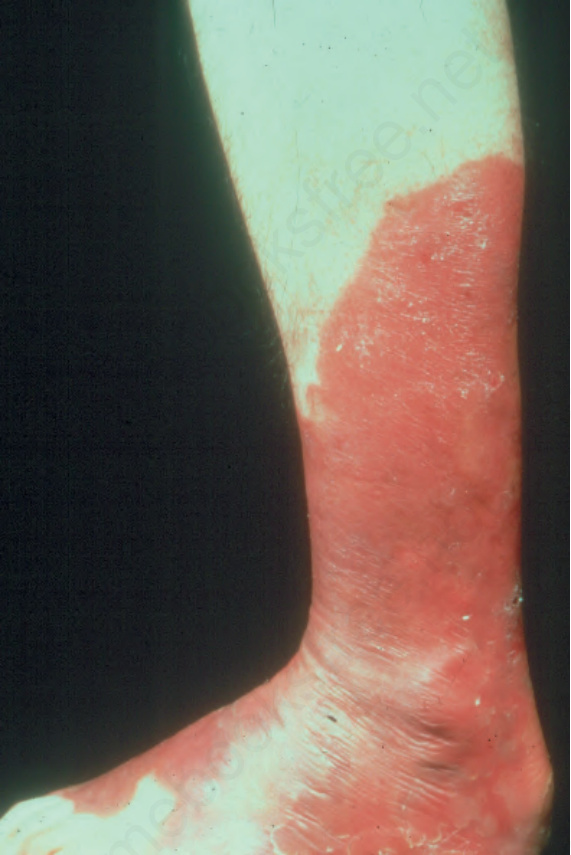
Fig. 29.86 Pagetoid reticulosis: this extensive erythematous lesion shows scaling and a sharply demarcated border. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.

Fig. 29.87 Pagetoid reticulosis: scanning view showing characteristic psoriasiform hyperplasia.
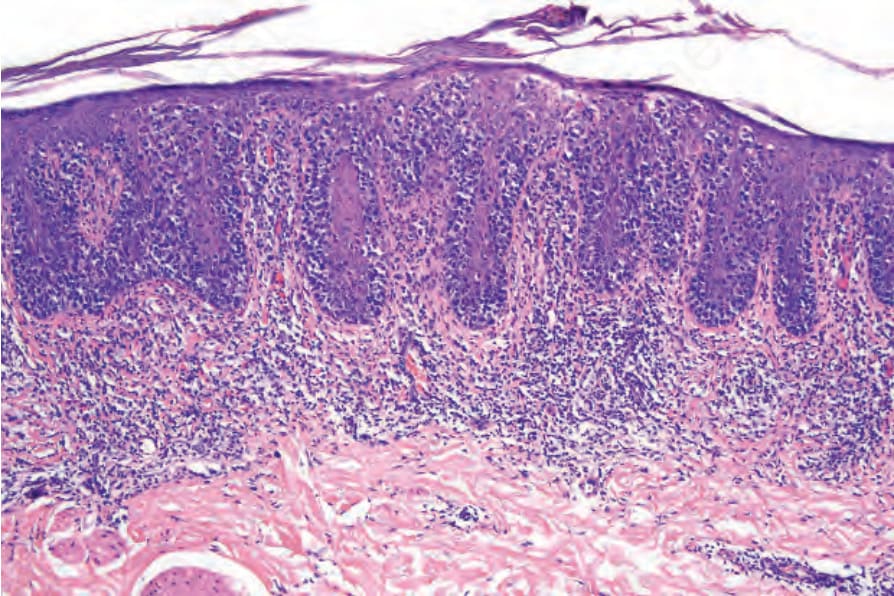
Fig. 29.88 Pagetoid reticulosis: atypical mononuclear cells are predominantly seen in the lower aspects of the elongated epidermal ridges.
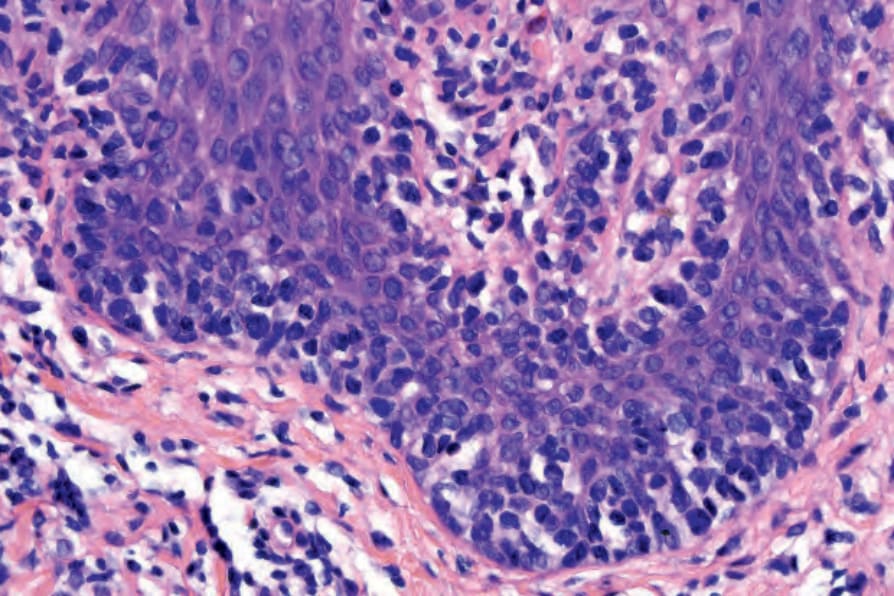
Fig. 29.89 Pagetoid reticulosis: high-power view of epidermotropism.
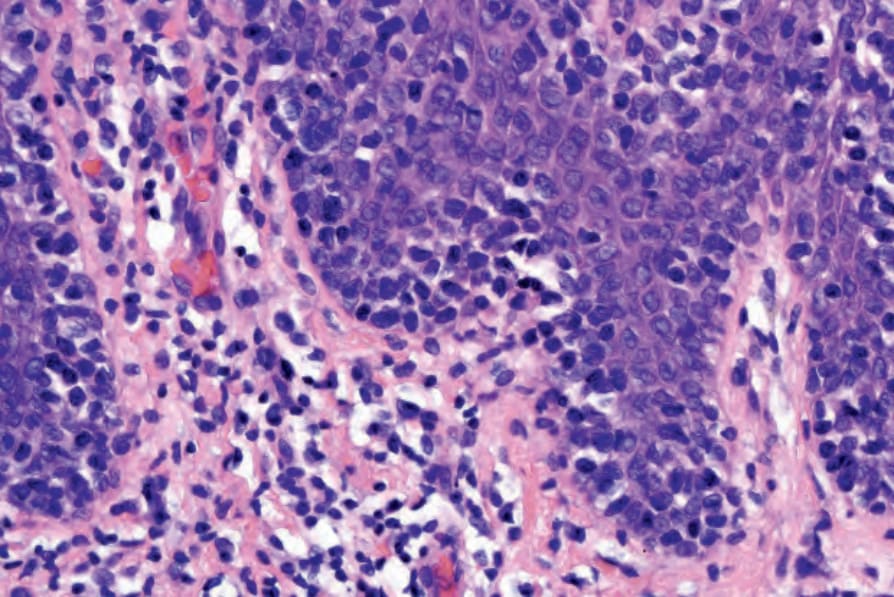
Fig. 29.90 Pagetoid reticulosis: note that the atypical lymphocytes are largely restricted to the epidermis.
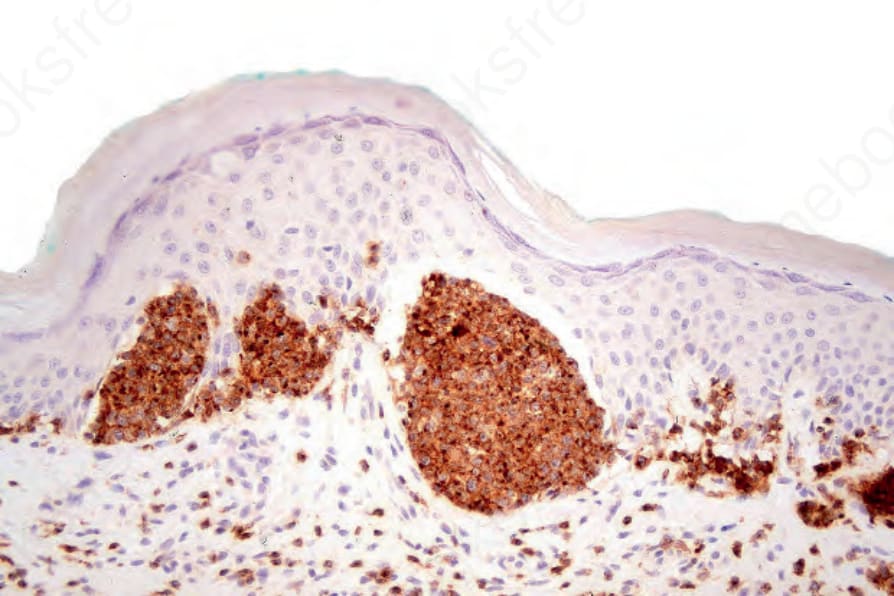
Fig. 29.91 Pagetoid reticulosis: the atypical lymphocytes can be highlighted with CD2 as shown in this example.