淋巴瘤的分類 (Classification of Lymphomas)
引言
-
自 Lukes 與 Collins、Rappaport 早期的年代,乃至其後的更新版 Kiel 分類 (Updated Kiel classification) 與工作分類方案 (Working Formulation) 以來,淋巴瘤與造血腫瘤 (hematopoietic neoplasms) 的分類在理念與診斷標準上已歷經根本性的變革。這些較早期的分類,多數主要依賴形態學 (morphology) 來區分各疾病實體,且設計上適用於淋巴結 (nodal) 病變,對淋巴結外 (extranodal) 部位(包括皮膚)或其他臨床面向幾乎或完全不予關注。
-
較近期,免疫組織化學 (immunohistochemistry) 的引入使得能辨識出 B 細胞與 T 細胞變異型,並迅速接續建立起更為詳盡且具鑑別力的標準,以診斷特定疾病實體。在與不同淋巴瘤亞型相關聯的一致性基因異常之發現(即濾泡性淋巴瘤 (follicular lymphoma) 中的 t(14:18) 轉位,以及未分化大細胞淋巴瘤 (anaplastic large cell lymphoma) 中的 t(2:5) 轉位),進一步強化了精確分類。其結果是,現代淋巴瘤分類體系乃依據共有的形態學、免疫表現型 (immunophenotypic)、基因及臨床特徵來認定各疾病實體,從而確保更具相關性的疾病分類與更高的診斷一致性。
-
⚠️【源檔此處有一段看似錯置/與上下文不連貫的文字,依鐵則原樣保留並譯出】:原發性皮膚濾泡中心細胞淋巴瘤 (primary cutaneous follicle center cell lymphoma),以及將腿部大 B 細胞淋巴瘤 (large B-cell lymphoma of the leg) 列為一獨立疾病實體之適切性。⁹,¹⁰ 對於使用 primary cutaneous ‘immunocytoma’ 一詞、而非 marginal zone lymphoma,也存在歧見;當時的 immunocytoma 涵蓋了 lymphoplasmacytic lymphoma,而後者乃是有別於 marginal zone lymphoma 的另一疾病實體。
-
隨著 1994 年修訂版歐美淋巴瘤 (revised European and American lymphoma, REAL) 分類的發表,這種更具系統性的方法獲得普遍接受。¹ 然而,儘管 REAL 分類認定某些皮膚淋巴增生性疾病 (cutaneous lymphoproliferative disorders) 為獨立疾病實體,它卻未能處理以下事實:某些主要發生於皮膚的淋巴瘤,在生物學上有別於發生於淋巴結、而形態學與表現型相似的腫瘤。由 EORTC 的皮膚淋巴瘤研究小組 (Cutaneous Lymphoma Study Group of the EORTC) 所提出的歐洲癌症研究與治療組織 (European Organisation for Research and Treatment of Cancer, EORTC) 分類,即試圖處理這些缺陷。此分類專為皮膚淋巴瘤而設計,更著重於某些原發性皮膚淋巴瘤 (primary cutaneous lymphomas) 獨特的臨床特徵,但在其他方面採用與 REAL 分類相似的理念。² 它最初係根據荷蘭皮膚淋巴瘤登記處 (Dutch Registry for Cutaneous Lymphoma) 紀錄中 626 名病人所得的資料,其後並於數項大型研究、以超過 1300 名病人的追蹤資料予以驗證。²⁻⁵ 此分類依據臨床經驗所確定的行為表現,將原發性皮膚病灶細分為惰性 (indolent)、侵襲性 (aggressive) 及暫定 (provisional) 類別(Table 29.1)。這是一大進展,因為它為若干原發性皮膚淋巴瘤提供了精確的定義,並認知到淋巴結原發病變與皮膚原發病變之間在生物學行為(從而潛在的治療需求)上的差異。例如,發生於淋巴結的 CD30 陽性(ALK 陰性)大 T 細胞淋巴瘤 (CD30-positive (ALK-negative) large T-cell lymphomas) 屬高惡性度 (high-grade) 腫瘤,死亡率高達 63%;而在形態學與免疫表現型上完全相同、卻原發於皮膚的腫瘤,臨床上則屬低惡性度 (low grade),死亡率低於 5%。⁶,⁷
-
這些差異在兩套分類系統的成員分別於 2003 年與 2004 年在 Lyon 與 Zurich 的會議之後獲得解決。其結果是一套共識性的 WHO-EORTC 分類,首次於 2005 年發表。¹¹,¹² 此系統所劃定的疾病實體,其後被納入 2008 年發表的《WHO 造血與淋巴組織腫瘤分類》(WHO classification of tumors of the hematopoietic and lymphoid tissue),其中對部分診斷標準作了精修並新增了新的疾病實體,並在 2016 年的修訂版中作了進一步修改。¹³,¹⁴ 本章將採用此最新更新版所使用的術語與標準。主要侵犯皮膚的淋巴瘤亞型,連同其預期的臨床行為,列於 Table 29.2。
Table 29.1 內容(EORTC 原發性皮膚淋巴瘤分類)
-
原發性 CTCL (Primary CTCL);原發性 CBCL (Primary CBCL)
-
惰性 (Indolent)
- Mycosis fungoides;Follicle center cell lymphoma
- Mycosis fungoides + follicular mucinosis
- Immunocytoma(marginal zone B-cell lymphoma)
- CD30+ large cell CTCL:Anaplastic、Immunoblastic、Pleomorphic
- Lymphomatoid papulosis
-
中間 (Intermediate)
- Large B-cell lymphoma of the leg
-
⚠️【源檔此段落穿插於表格文字之間,依原樣保留並譯出】:EORTC 分類所取得的許多進展,並未被 2001 年世界衛生組織 (World Health Organization, WHO) 與其聯合發表的 REAL 分類更新版所採納。⁸ 此事引發相當大的爭議,尤其是在 B 細胞腫瘤方面。反對 EORTC 取向的論點包括:抱怨其定義過於寬泛。
-
侵襲性 (Aggressive)
- Sézary syndrome
- CD30– large cell CTCL:Immunoblastic、Pleomorphic
-
暫定 (Provisional)
- Granulomatous slack skin;Intravascular large B-cell lymphoma
- CTCL, pleomorphic small/medium-sized
- Plasmacytoma
- Subcutaneous panniculitis-like T-cell lymphoma
-
縮寫:CTCL,cutaneous T-cell lymphoma(皮膚 T 細胞淋巴瘤);CBCL,cutaneous B-cell lymphoma(皮膚 B 細胞淋巴瘤);EORTC,European Organisation for Research and Treatment of Cancer。修改自:Willemze, R., et al. (1997) Blood, 90, 354–371。
Table 29.2 內容(WHO-EORTC 皮膚淋巴瘤分類所定義之淋巴瘤亞型與行為)
-
WHO-EORTC 亞型 (subtype);行為 (Behavior)
-
皮膚 T 細胞淋巴瘤 (Cutaneous T-cell lymphoma)
- Mycosis fungoides — 惰性 (Indolent)
- MF 變異型 (MF variants)
- Folliculotropic MF — 惰性 (Indolent)
- Pagetoid reticulosis — 惰性 (Indolent)
- Granulomatous slack skin — 惰性 (Indolent)
- Sézary syndrome — 侵襲性 (Aggressive)
- Adult T-cell leukemia/lymphoma — 侵襲性 (Aggressive)
-
原發性皮膚 CD30+ 淋巴增生性疾病 (Primary cutaneous CD30+ lymphoproliferative disorders)
- Primary cutaneous anaplastic large cell lymphoma — 惰性 (Indolent)
- Lymphomatoid papulosis — 惰性 (Indolent)
-
Subcutaneous panniculitis-like T-cell lymphoma — 惰性 (Indolent)
-
Extranodal NK/T-cell lymphoma, nasal type — 侵襲性 (Aggressive)
-
原發性皮膚 T 細胞淋巴瘤,未特指 (Primary cutaneous T-cell lymphoma, unspecified)
- Primary cutaneous aggressive epidermotropic CD8+ T-cell lymphoma* — 侵襲性 (Aggressive)
- Hydroa vacciniforme-like lymphoma — 侵襲性 (Aggressive)
- Cutaneous γ/δ T-cell lymphoma — 侵襲性 (Aggressive)
- Primary cutaneous acral CD8+ T-cell lymphoma* — 惰性 (Indolent)
- Primary cutaneous CD4+ small/medium-sized pleomorphic T-cell lymphoproliferative disorder* — 惰性 (Indolent)
-
皮膚 B 細胞淋巴瘤 (Cutaneous B-cell lymphoma)
- Primary cutaneous marginal zone lymphoma — 惰性 (Indolent)
- Primary cutaneous follicle center lymphoma — 惰性 (Indolent)
- Primary cutaneous large B-cell lymphoma, leg type — 中間 (Intermediate)
- Primary cutaneous large B-cell lymphoma, other — 中間 (Intermediate)
- Primary cutaneous intravascular large B-cell lymphoma — 中間 (Intermediate)
-
*暫定疾病實體 (Provisional entities)。縮寫:MF,mycosis fungoides;WHO-EORTC,World Health Organization-European Organisation for Research and Treatment of Cancer。修改自:Swerdlow S.H., et al. (2016). Blood, 127, 2375–2390。
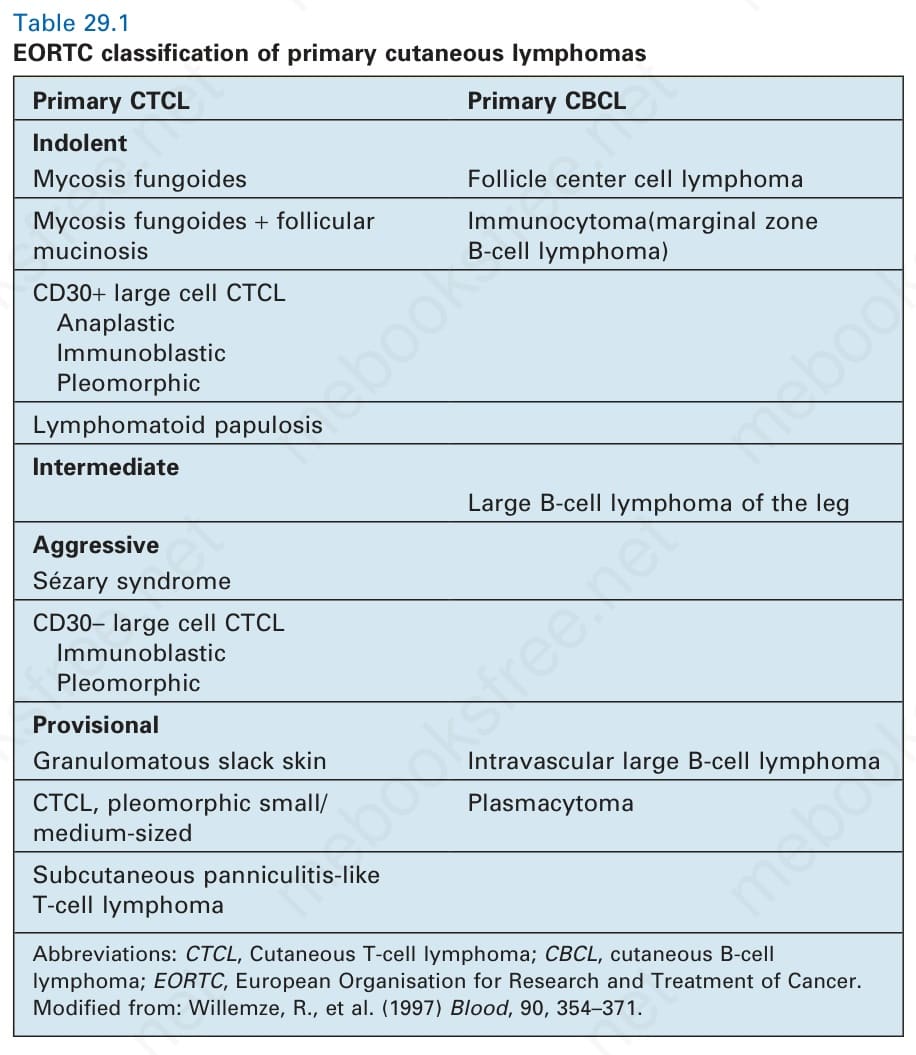
表 29-1:原發性皮膚淋巴瘤的 EORTC 分類 (EORTC classification of primary cutaneous lymphomas)。
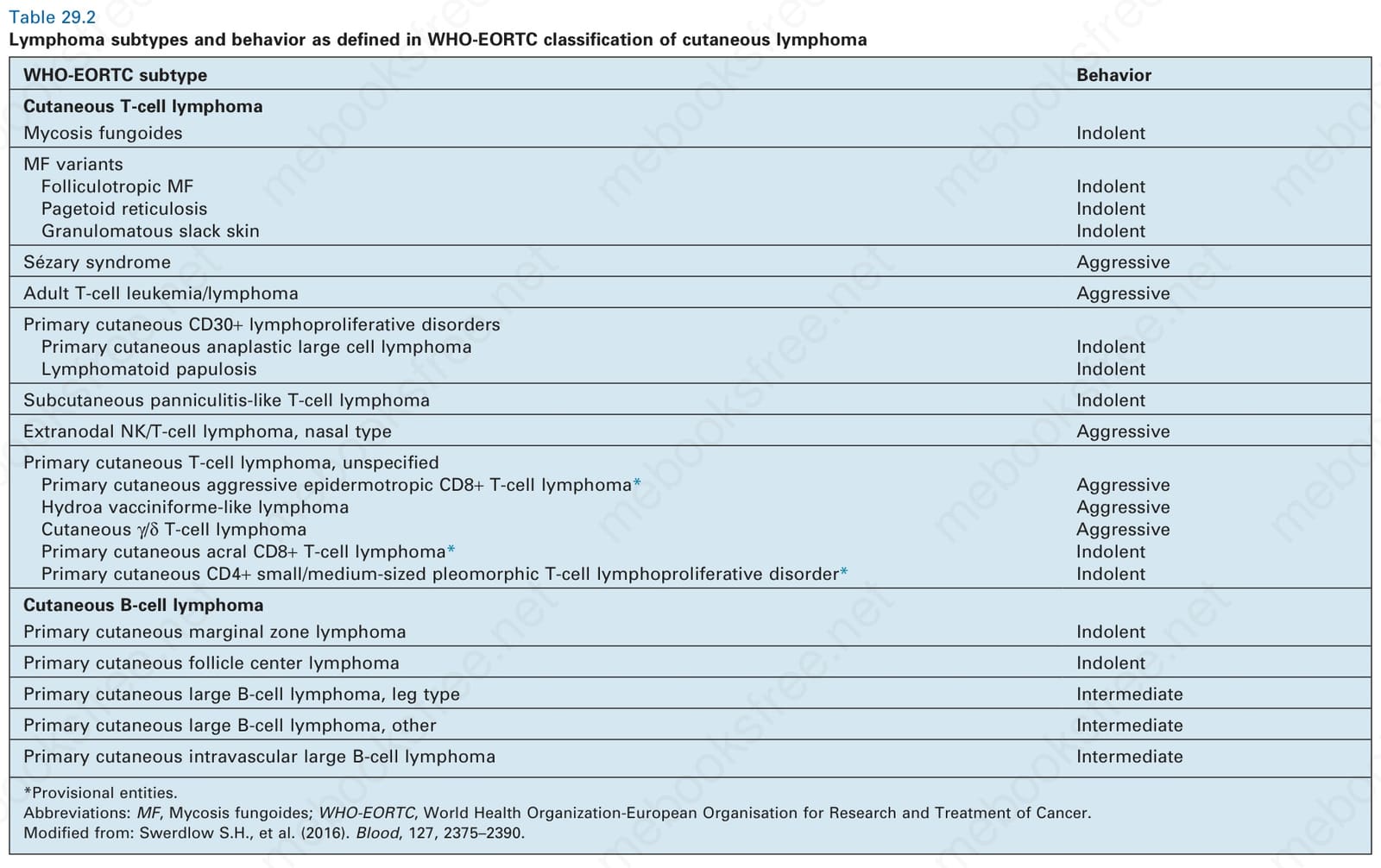
表 29-2:WHO-EORTC 皮膚淋巴瘤分類所定義之淋巴瘤亞型與行為 (Lymphoma subtypes and behavior as defined in WHO-EORTC classification of cutaneous lymphoma)。