Classification of lymphomas
Classification of lymphomas
The classification of lymphomas and hematopoietic neoplasms has undergone radical changes in philosophy and diagnostic criteria since the early days of Lukes and Collins, Rappaport, and the subsequent Updated Kiel classification and the Working Formulation. The majority of these earlier classifications relied mainly on morphology to differentiate between entities, and were designed to be applicable to nodal disease with little or no attention being paid to extranodal sites (including the skin) or other clinical considerations. More recently, the input of immunohistochemistry enabled recognition of B- and T-cell variants, rapidly followed by the establishment of more detailed and discriminatory criteria for the diagnosis of specific entities. The identification of consistent genetic abnormalities in association with distinct lymphoma subtypes (i.e., the t(14:18) translocation in follicular lymphoma and the t(2:5) translocation in anaplastic large cell lymphoma) has further strengthened precise classification. As a result, modern lymphoma classification schemes recognize entities on the basis of shared morphological, immunophenotypic, genetic, and clinical features, ensuring more relevant disease categories and greater diagnostic consistency.
of primary cutaneous follicle center cell lymphoma and the appropriateness of designating large B-cell lymphoma of the leg as a separate entity.9,10 Dissension also reigned over use of the term primary cutaneous ‘immunocytoma’ as opposed to marginal zone lymphoma, immunocytoma at that time being inclusive of lymphoplasmacytic lymphoma, an entity distinct from marginal zone lymphoma.
This more systematic approach achieved general acceptance with the publication of the revised European and American lymphoma (REAL) classification in 1994.1 However, although the REAL classification recognized certain cutaneous lymphoproliferative disorders as independent entities, it failed to address the fact that certain lymphomas arising primarily in the skin were biologically distinct from morphologically and phenotypically similar neoplasms occurring in lymph nodes. The European Organisation for Research and Treatment of Cancer (EORTC) classification, proposed by the Cutaneous Lymphoma Study Group of the EORTC, sought to address these deficiencies. This was designed for cutaneous lymphomas with a greater emphasis on the unique clinical features of some primary cutaneous lymphomas, but otherwise employed a similar philosophy to that used in the REAL classification.2 It was originally based on the data derived from 626 patients in the records of the Dutch Registry for Cutaneous Lymphoma, and later validated in several large studies with follow-up data from >1300 patients.2–5 This classification subdivided primary cutaneous lesions into indolent, aggressive, and provisional categories based on behavior as determined by clinical experience (Table 29.1). This was a major step forward because it provided a precise definition for a number of primary cutaneous lymphomas and recognized differences in biological behavior (and thus potential treatment requirements) between nodal and cutaneous primary disease. For example, CD30-positive (ALK-negative) large T-cell lymphomas arising in lymph nodes are high-grade tumors, with a mortality of up to 63%, whereas morphologically and immunophenotypically identical tumors arising primarily in the skin are clinically low grade, and have a mortality of less than 5%.6,7
These differences were resolved following meetings of members of both classification systems in Lyon and Zurich in 2003 and 2004, respectively. This resulted in a consensus WHO-EORTC classification first published in 2005.11,12 The entities delineated in this system were subsequently incorporated, with refinements of some diagnostic criteria and the addition of new entities, into the WHO classification of tumors of the hematopoietic and lymphoid tissue published in 2008, with further modifications in the 2016 revision.13,14 The terminology and criteria used in this latest update will be used in this chapter. The main lymphoma subtypes that primarily affect the skin are listed along with their expectant clinical behavior in Table 29.2.
Primary CTCL Primary CBCL
Indolent Mycosis fungoides Follicle center cell lymphoma
Mycosis fungoides + follicular mucinosis
Immunocytoma(marginal zone B-cell lymphoma)
CD30+ large cell CTCL Anaplastic Immunoblastic Pleomorphic
Lymphomatoid papulosis
Intermediate
Large B-cell lymphoma of the leg
Many of the advances made in the EORTC classification were not recognized in the update of the REAL classification published jointly with the World Health Organization (WHO) in 2001.8 This generated considerable controversy, particularly with respect to B-cell neoplasms. Arguments used against the EORTC approach included complaints of too broad a definition
Aggressive Sézary syndrome
CD30– large cell CTCL Immunoblastic Pleomorphic
Provisional Granulomatous slack skin Intravascular large B-cell lymphoma
CTCL, pleomorphic small/ medium-sized
Plasmacytoma
Subcutaneous panniculitis-like T-cell lymphoma
Abbreviations: CTCL, Cutaneous T-cell lymphoma; CBCL, cutaneous B-cell lymphoma; EORTC, European Organisation for Research and Treatment of Cancer. Modified from: Willemze, R., et al. (1997) Blood, 90, 354–371.
1405 Mycosis fungoides
WHO-EORTC subtype Behavior
Cutaneous T-cell lymphoma Mycosis fungoides Indolent
MF variants Folliculotropic MF Indolent Pagetoid reticulosis Indolent Granulomatous slack skin Indolent
Sézary syndrome Aggressive
Adult T-cell leukemia/lymphoma Aggressive
Primary cutaneous CD30+ lymphoproliferative disorders Primary cutaneous anaplastic large cell lymphoma Indolent Lymphomatoid papulosis Indolent
Subcutaneous panniculitis-like T-cell lymphoma Indolent
Extranodal NK/T-cell lymphoma, nasal type Aggressive
Primary cutaneous T-cell lymphoma, unspecified Primary cutaneous aggressive epidermotropic CD8+ T-cell lymphoma* Aggressive Hydroa vacciniforme-like lymphoma Aggressive Cutaneous γ/δ T-cell lymphoma Aggressive Primary cutaneous acral CD8+ T-cell lymphoma* Indolent Primary cutaneous CD4+ small/medium-sized pleomorphic T-cell lymphoproliferative disorder* Indolent
Cutaneous B-cell lymphoma Primary cutaneous marginal zone lymphoma Indolent
Primary cutaneous follicle center lymphoma Indolent
Primary cutaneous large B-cell lymphoma, leg type Intermediate
Primary cutaneous large B-cell lymphoma, other Intermediate
Primary cutaneous intravascular large B-cell lymphoma Intermediate
*Provisional entities. Abbreviations: MF, Mycosis fungoides; WHO-EORTC, World Health Organization-European Organisation for Research and Treatment of Cancer. Modified from: Swerdlow S.H., et al. (2016). Blood, 127, 2375–2390.
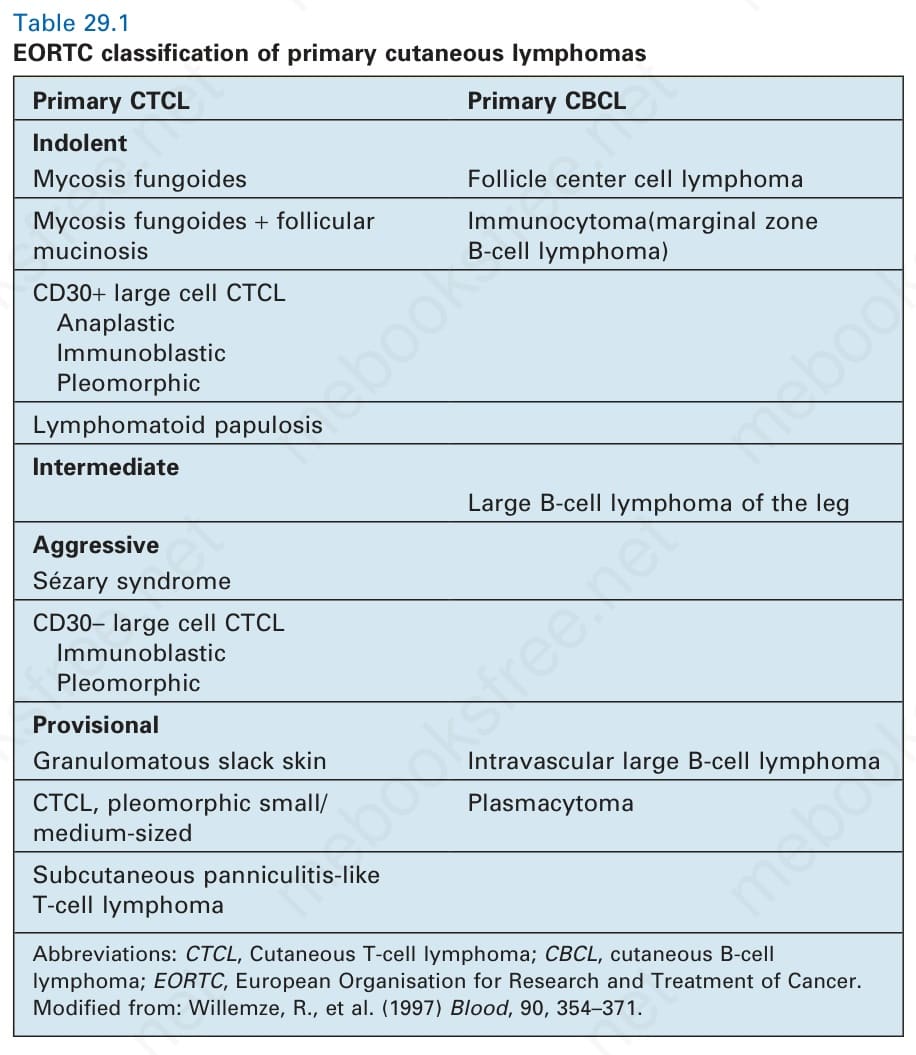
Table 29.1 EORTC classification of primary cutaneous lymphomas
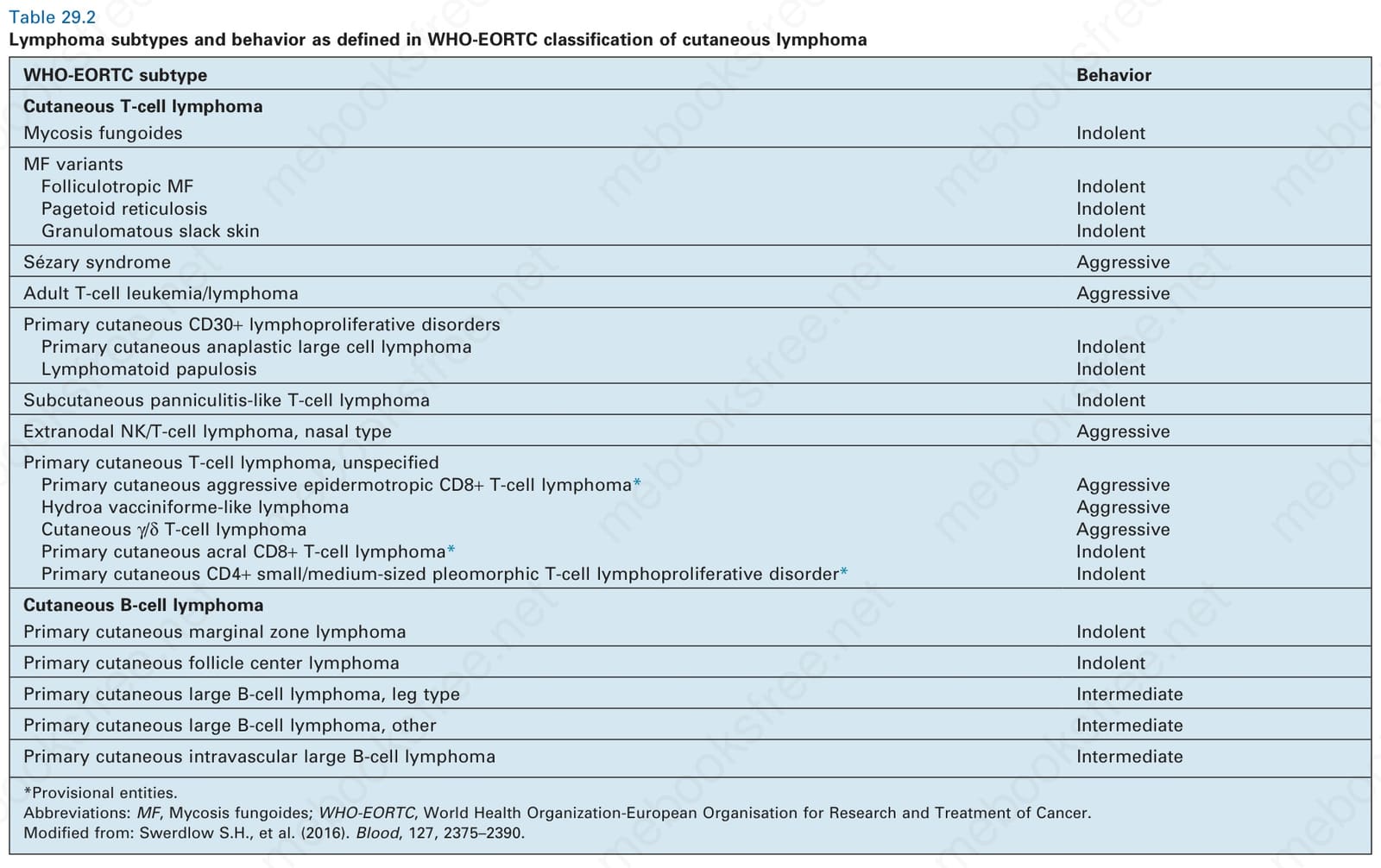
Table 29.2 Lymphoma subtypes and behavior as defined in WHO-EORTC classification of cutaneous lymphoma