結膜黑色素瘤 (Conjunctival Melanoma)
結膜黑色素瘤 (conjunctival melanoma) 是一種罕見、單側性的腫瘤,死亡率為百分之二十三至百分之三十。它常被與葡萄膜黑色素瘤 (uveal melanoma) 合併歸類,並統稱為「眼部黑色素瘤 (ocular melanoma)」。然而,這些腫瘤具有不同的臨床行為與組織學特徵,應被視為各自獨立的疾病實體加以處理。
在一項研究中,區域性轉移 (regional metastasis) 的十年累積發生率為百分之十一,而厚度大於 2 mm 的腫瘤呈現較高趨勢。其他轉移的危險因子包括:穹窿 (fornix)、瞼結膜 (palpebral conjunctiva) 或淚阜 (caruncle) 受侵犯;局部腫瘤復發;以及切緣陽性 (positive tumor margins)。
局部復發 (local recurrence) 很常見,發生於半數患者,通常在原發腫瘤治療後 5 年內出現。復發的平均時間為 2.5 年。與復發相關的危險因子包括黑色素瘤的位置 (未接觸角膜緣 limbus) 以及病理檢查時切除緣陽性。結膜黑色素瘤在區域性與全身性轉移之前,可能先在結膜內局部擴散。「途中 (in-transit)」轉移是指被認為由結膜內局部淋巴擴散所造成的小型次發性腫瘤結節。亦有報告指出,腫瘤切除過程中因黑色素瘤細胞播散而造成的「局部轉移 (local metastasis)」。
至腮腺 (parotid,即耳前 preauricular) 與下頷下 (submandibular) 區域的區域性淋巴結轉移發生於百分之二十至百分之四十的患者。侵犯鼻側結膜 (nasal conjunctiva) 的黑色素瘤傾向轉移至下頷下淋巴結,而侵犯顳側結膜 (temporal conjunctiva) 者則傾向轉移至腮腺 (耳前) 淋巴結。區域性轉移於原發結膜黑色素瘤診斷後中位數 23 個月 (範圍 12–108 個月) 發生。區域性轉移的危險因子包括:非角膜緣 (non-limbal) 位置、腫瘤厚度 > 2 mm、大的基底直徑、切除緣陽性、眼眶延伸 (orbital extension),以及結節狀腫瘤外形。對於黑色素瘤位於非角膜緣位置且厚度 > 2 mm 的患者,曾建議施行前哨淋巴結切片 (sentinel lymph node biopsy);然而其使用仍具爭議,因為對於整體存活效益仍有辯論。全身性轉移最常發生於腦、肝與肺。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
多數腫瘤發生於瞼裂間的球結膜 (interpalpebral bulbar conjunctiva);然而,並無明確證據顯示紫外線 (UV) 輻射會引起結膜黑色素瘤。
確定診斷有賴於組織學檢查。多數病例可使用光學顯微鏡準確診斷 (Figs 27.44–27.46)。組織學上,結膜黑色素瘤可能含有四種細胞型態的混合:小的多面體 (polyhedral) 細胞;梭形 (spindle) 細胞;氣球狀 (balloon) 細胞;以及具嗜伊紅性細胞質的圓形上皮樣 (epithelioid) 細胞 (Fig. 27.47)。黑色素瘤常伴隨上皮內帶有異型性的 PAM (intraepithelial PAM with atypia)。有時,黑色素瘤可能與結膜痣 (conjunctival nevus) 相關。偶爾可見硬纖維化間質 (desmoplastic stroma)。
預測不良預後的組織學特徵包括:腫瘤厚度與大小;手術切緣陽性;腫瘤位置;佩吉特樣擴散 (Pagetoid spread) 的存在;淋巴擴散的組織學證據;以及由 Ki-67 免疫組化所判定的腫瘤細胞增殖。多項試圖找出可作為結膜黑色素瘤預後因子之關鍵腫瘤厚度的研究,所得數值範圍為 0.8 至 4.0 mm。腫瘤厚度是使用經校準至工作顯微鏡的目鏡測微計 (ocular micrometer) 測量,自結膜上皮表面量至最深侵犯點。較大的腫瘤,大於 10 mm,亦與較差預後相關。與球結膜 (bulbar) 黑色素瘤相比,腫瘤位於瞼結膜 (palpebral conjunctiva)、穹窿 (fornix)、半月皺襞 (plica)、淚阜 (caruncle) 與眼瞼緣 (lid margin) 者,與較高死亡率相關。性別、年齡與腫瘤來源 (PAM、痣或原發 de novo) 並非有用的預後指標。病理報告應包含可指引眼科手術醫師治療患者的資訊,尤其是側向與深部切緣的充分性,以及腫瘤厚度。
瞼結膜或穹窿;以及 (3) 黏附於下方的鞏膜 (sclera)。支持黑色素瘤而非結膜痣的組織學特徵包括 (1) 上皮內、佩吉特樣 (pagetoid) 生長;(2) 上皮內增殖明顯延伸至上皮下成分邊緣的側方,代表帶有異型性的 PAM;(3) 病灶基底的發炎;(4) 有絲分裂 (mitoses);(5) 病灶基底缺乏細胞成熟 (cellular maturation);以及 (6) 病灶細胞於基底處有黑色素 (melanin) 的存在 (通常,基底處的痣細胞傾向為無黑色素 amelanotic)。
亦應考慮葡萄膜黑色素瘤或黑色素細胞瘤 (melanocytoma) 的眼球上方延伸 (epibulbar extension) (Fig. 27.48);在這些病例中,病灶的跨鞏膜 (trans-scleral) 性質可藉由高頻眼部超音波 (high-frequency ocular ultrasonography) 加以辨識。
BRAF 突變 (BRAF mutation) 可見於百分之五十的原發與轉移性結膜黑色素瘤。在一項研究中,BRAF V600E 突變於百分之八十二帶有 BRAF 突變的病例中被偵測到。BRAF 突變的存在於較年輕的患者以及由痣產生的黑色素瘤中較為常見,但與預後無關。以 BRAF 與 MEK 抑制劑進行的標靶治療,可改善帶有 BRAF 突變之轉移性皮膚黑色素瘤患者的存活率。對所有結膜黑色素瘤以免疫組化或分子分析常規檢測 BRAF V600E 突變,若患者發展為轉移性疾病,可能可預測對 Vemurafenib 的反應性。
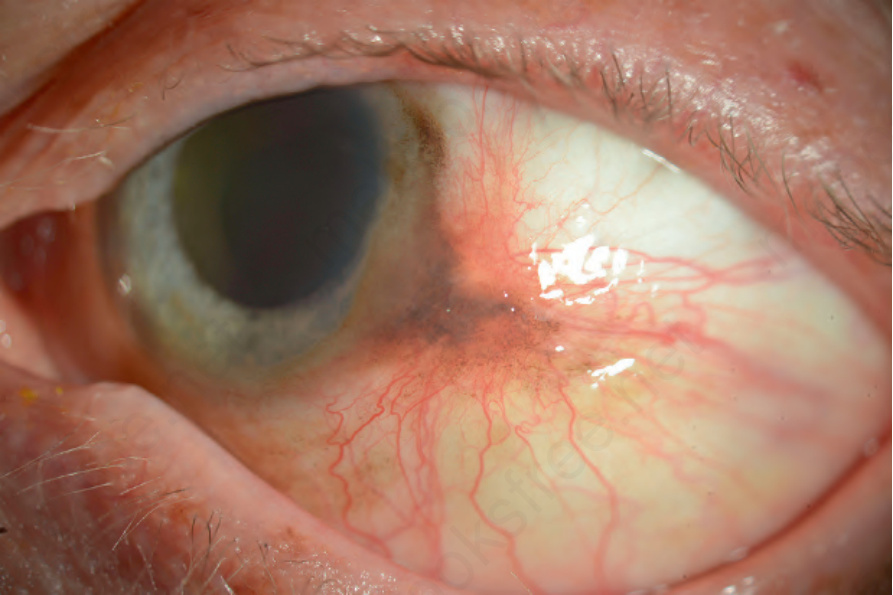
圖 27-41:結膜黑色素瘤 (conjunctival melanoma):此腫瘤偏粉棕色並伴血管增生。此白人 (Caucasian) 患者角膜緣周圍球結膜及周邊角膜上廣泛的色素沉著可能代表 PAM。
Fig. 27.41 Conjunctival melanoma: this tumor is more pink-brown with increased vascularity. The widespread pigmentation of the bulbar conjunctiva around the limbus and on the peripheral cornea likely represents PAM in this Caucasian patient.
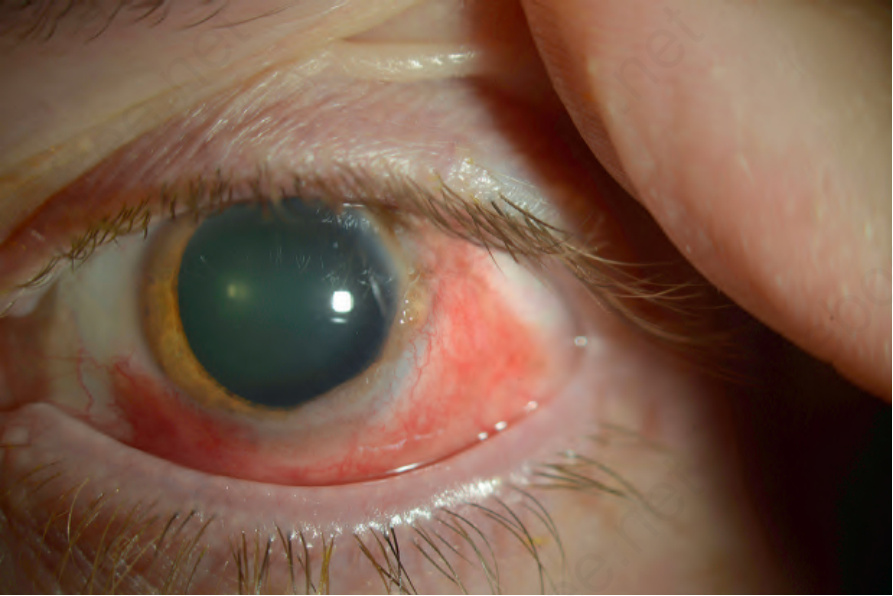
圖 27-42:結膜黑色素瘤 (conjunctival melanoma):此腫瘤較為瀰漫,環繞角膜緣 (limbus) 至少 180°。於 3 點鐘方向有些結節狀。腫瘤相對無黑色素 (amelanotic),伴隨發炎與明顯的內在血管性。
Fig. 27.42 Conjunctival melanoma: this tumor is more diffuse, surrounding the limbus for at least 180°. There is some nodularity at 3 o’clock. The tumor is relatively amelanotic with inflammation and prominent intrinsic vascularity.
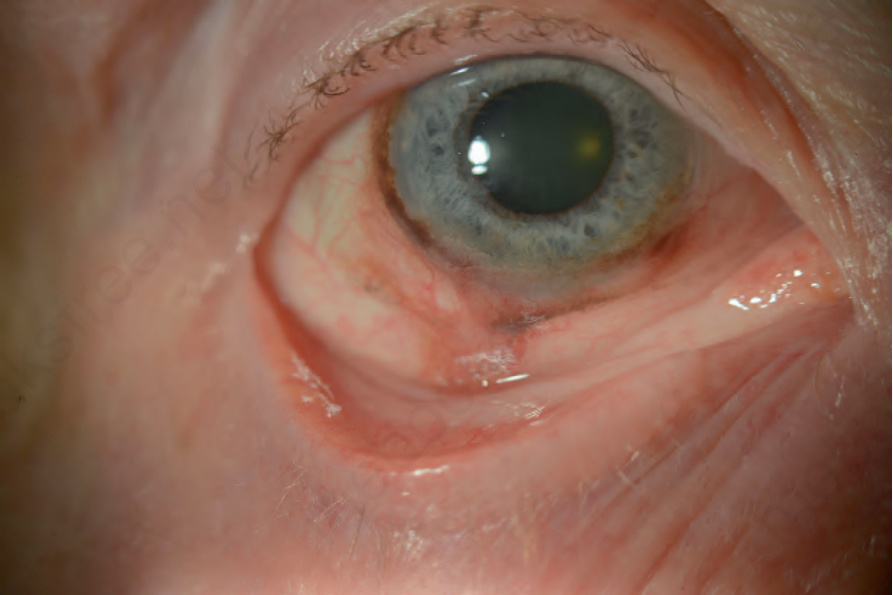
圖 27-43:結膜黑色素瘤 (conjunctival melanoma):有一黑色素瘤侵犯下方球結膜 (inferior bulbar conjunctiva),延伸至穹窿 (fornix)。
Fig. 27.43 Conjunctival melanoma: there is a melanoma involving the inferior bulbar conjunctiva, extending to the fornix.
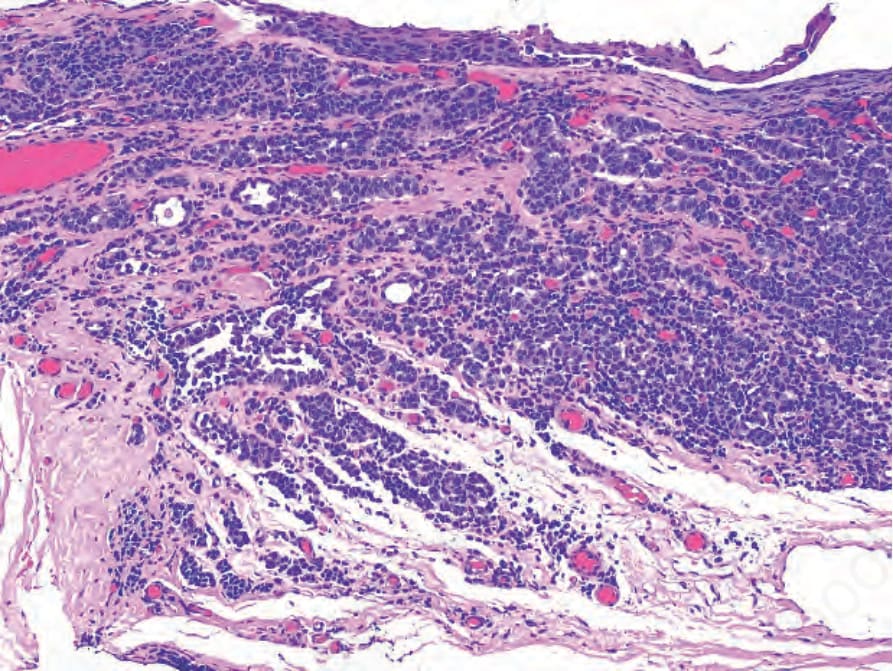
圖 27-44:結膜黑色素瘤 (conjunctival melanoma):Figure 27.42 的組織學。腫瘤在帶有異型性的原發性後天黑色素沉著 (primary acquired melanosis, PAM) 背景下產生,並顯示小型、多面體、無黑色素的黑色素瘤細胞巢侵犯固有層 (substantia propria)。腫瘤血管相當豐富,腫瘤細胞巢與慢性發炎交雜。
Fig. 27.44 Conjunctival melanoma: histology of Figure 27.42. The tumor arises in the context of primary acquired melanosis (PAM) with atypia, and shows nests of small, polyhedral, amelanotic melanoma cells invading the substantia propria. The tumor is quite vascular, and tumor nests intermingle with chronic inflammation.
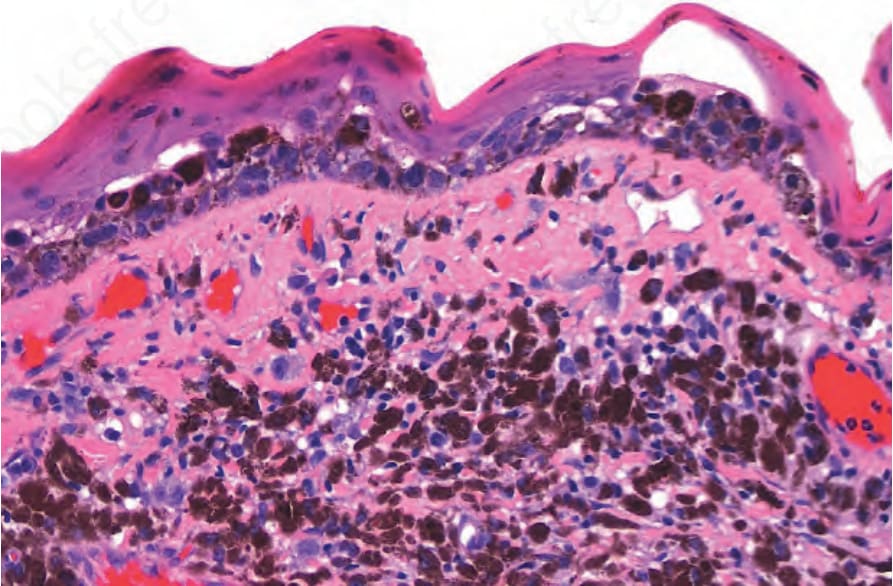
圖 27-45:結膜黑色素瘤 (conjunctival melanoma):鄰近角膜緣之黑色素瘤的低倍視野 (角膜位於影像右側)。注意上皮內成分如何遠遠延伸超出腫瘤的上皮下部分。
Fig. 27.45 Conjunctival melanoma: low-power view of a melanoma adjacent to the limbus (cornea is at the right of the image). Note how the intraepithelial component extends well beyond the subepithelial part of the tumor.
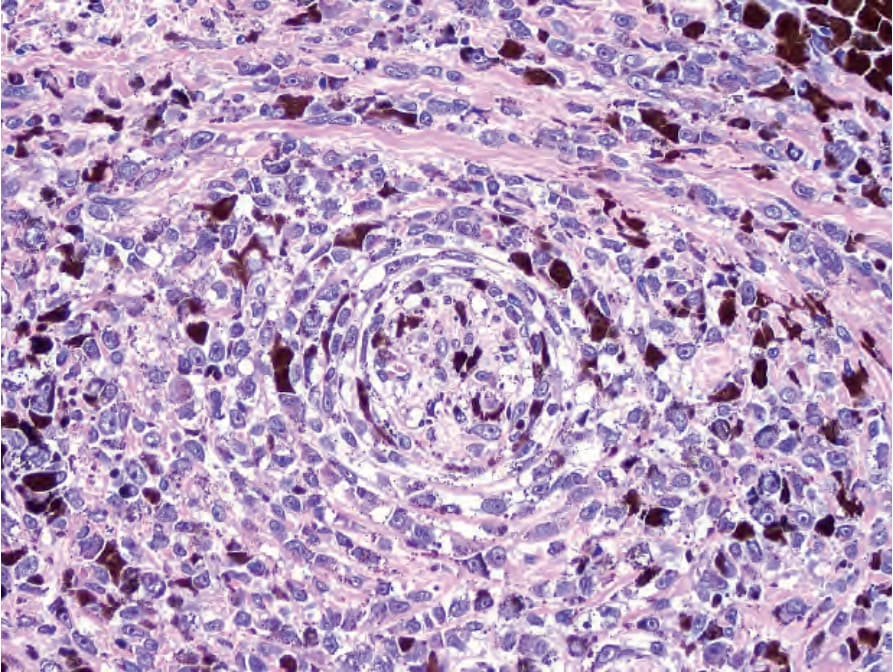
圖 27-46:結膜黑色素瘤 (conjunctival melanoma):有神經內與神經周圍 (intraneural and perineural) 侵犯。
Fig. 27.46 Conjunctival melanoma: there is intraneural and perineural involvement.
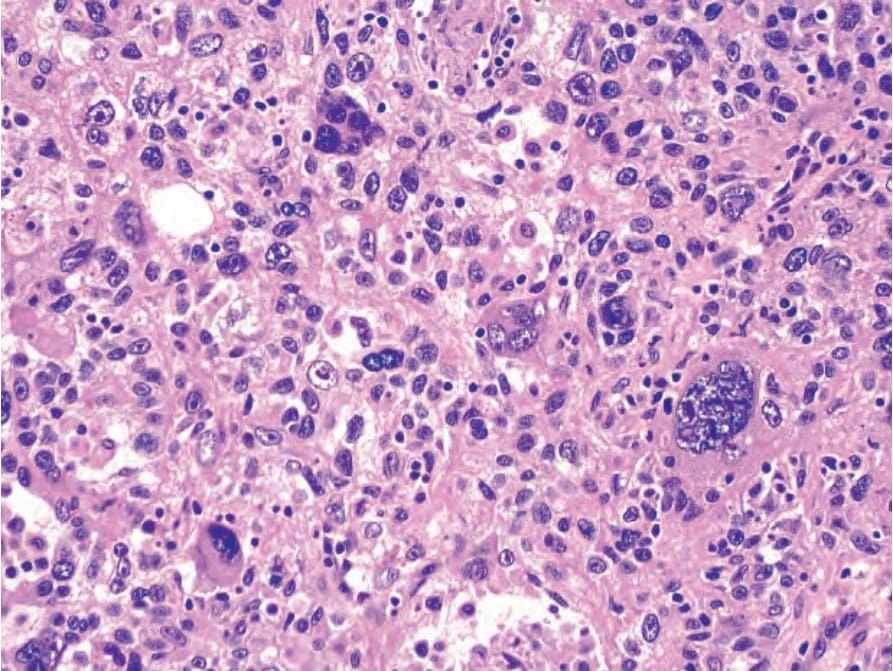
圖 27-47:結膜黑色素瘤 (conjunctival melanoma):在此範例中,有大型、多形性的上皮樣細胞 (pleomorphic epithelioid cells) 與腫瘤巨細胞 (tumor giant cells),具豐富的嗜伊紅性細胞質與帶有明顯核仁 (prominent nucleoli) 的細胞核。
Fig. 27.47 Conjunctival melanoma: in this example, there are large, pleomorphic epithelioid cells and tumor giant cells with abundant eosinophilic cytoplasm and nuclei with prominent nucleoli.

圖 27-48:睫狀體黑色素瘤 (ciliary body melanoma) 的眼外延伸。(A) 一顆棕黑色、多分葉的腫瘤帶有大型供血血管 (feeder vessels),鄰近角膜緣 (limbus)。眼內成分的一部分自前房角 (anterior chamber angle) 露出。(B) 組織學顯示一睫狀體黑色素瘤穿過鞏膜 (sclera) 侵犯至結膜下空間 (subconjunctival space)。
Fig. 27.48 Extraocular extension of a ciliary body melanoma. (A) A brown-black multilobulated tumor with large feeder vessels is adjacent to the limbus. A portion of the intraocular component peeks out from the anterior chamber angle. (B) Histology shows a ciliary body melanoma that invades through the sclera to the subconjunctival space.