Conjunctival melanoma
Conjunctival melanoma
Conjunctival melanoma is a rare, unilateral tumor with a mortality rate of 23% to 30%.1,2 It is often lumped together with uveal melanoma and referred to collectively as ‘ocular melanoma’. However, these tumors have distinct clinical behaviors and histologic features, and should be approached as separate entities.
In one study, the 10-year cumulative incidence of regional metastasis was 11% with a higher trend for tumors thicker than 2 mm.12 Other risk factors for metastasis include involvement of the fornix, palpebral conjunctiva, or caruncle; local tumor recurrence12; and positive tumor margins10.
Local recurrence is common and occurs in half of patients, usually within 5 years of treatment of the primary tumor.1 The mean time to recurrence is 2.5 years.1 Risk factors associated with recurrence include melanoma location (not touching the limbus) and positive resection margins on pathological examination.10 Conjunctival melanoma may spread locally in the conjunctiva before metastasizing regionally and systemically. ‘In-transit’ metastases are small secondary tumor nodules thought to be caused by local lymphatic spread within the conjunctiva.1 ‘Local metastasis’ due to melanoma cell dissemination during tumor excision has also been reported.1
1378 Tumors of the conjunctiva
Regional lymph node metastasis to parotid (preauricular) and submandibular regions occurs in 20% to 40% of patients.1,10,13,14 Melanomas involving the nasal conjunctiva tend to metastasize to submandibular lymph nodes, whereas those involving the temporal conjunctiva tend to metastasize to the parotid (preauricular) lymph nodes.15 Regional metastases occur at a median of 23 (range, 12–108) months after diagnosis of primary conjunctival melanoma.15 Risk factors for regional metastasis include non-limbal location, tumor thickness > 2 mm, large basal diameter, positive resection margins, orbital extension, and nodular tumor shape.13 Sentinel lymph node biopsy has been suggested for patients with melanoma in a non-limbal location and thickness > 2 mm13; however, its use is controversial because there is still debate over the overall survival benefit.16 Systemic metastasis most commonly occurs in the brain, liver, and lung.
Pathogenesis and histologic features Most tumors develop on the interpalpebral bulbar conjunctiva; however, there is no clear evidence that UV radiation causes conjunctival melanoma.
Definitive diagnosis depends on histologic examination. Most cases can be accurately diagnosed using light microscopy (Figs 27.44–27.46). Histologically, conjunctival melanoma may contain mixtures of four cell types: small, polyhedral; spindle; balloon; and round epithelioid cells with eosinophilic cytoplasm (Fig. 27.47).1,4,17 Melanoma is often accompanied by intraepithelial PAM with atypia. Sometimes, melanomas may be associated with a conjunctival nevus. Occasionally, desmoplastic stroma may be seen.
Histologic features that predict adverse prognosis include tumor thickness2 and size; positive surgical margins; tumor location18; presence of Pagetoid spread; histologic evidence of lymphatic spread18; and tumor cell proliferation as determined by immunohistochemistry for Ki-67. Various studies attempting to identify a critical tumor thickness that may serve as a prognostic factor for conjunctival melanoma have found values ranging from 0.8 to 4.0 mm.1,2,10,18 Tumor thickness is measured using an ocular micrometer, calibrated to the working microscope, going from the surface of the conjunctival epithelium to the point of deepest invasion.2 Larger tumors, greater than 10 mm, are also associated with worse prognosis.1 Tumor location in the palpebral, conjunctiva, fornix, plica, caruncle, and lid margin are associated with higher mortality compared with bulbar melanoma.1,18 Sex, age, and tumor origin (PAM, nevus, or de novo) are not useful prognostic indicators.18 The pathologist’s report should include information to guide the ophthalmic surgeon’s treatment of the patient, particularly the adequacy of the lateral and deep margins, and tumor thickness.
1379 Hematopoietic tumors
palpebral conjunctiva or fornix; and (3) adherence to underlying sclera.1 Histologic features that favor melanoma over conjunctival nevus include (1) intraepithelial, pagetoid growth; (2) intraepithelial proliferation that extends significantly lateral to the edge of the subepithelial component, which represents PAM with atypia; (3) inflammation at the base of the lesion; (4) mitoses; (5) absence of cellular maturation at the base of the lesion; and (6) presence of melanin within lesional cells toward the base (typically, nevus cells at the base tend to be amelanotic).4
Epibulbar extension of uveal melanoma or melanocytoma should also be considered (Fig. 27.48); in these cases, the trans-scleral nature of the lesion can be identified by high-frequency ocular ultrasonography.
BRAF mutation may be seen in 50% of primary and metastatic conjunctival melanomas. In one study, BRAF V600E mutation was detected in 82% of cases with BRAF mutation. The presence of BRAF mutation was more frequent in younger patients and in melanomas that arose from a nevus but was not associated with prognosis.19 Targeted therapies with BRAF and MEK inhibitors can improve survival in patients with BRAF-mutated metastatic cutaneous melanoma. Routine testing of all conjunctival melanomas for BRAF V600E mutation by immunohistochemistry or molecular analysis may predict responsiveness to Vemurafenib if the patient develops metastatic disease.20
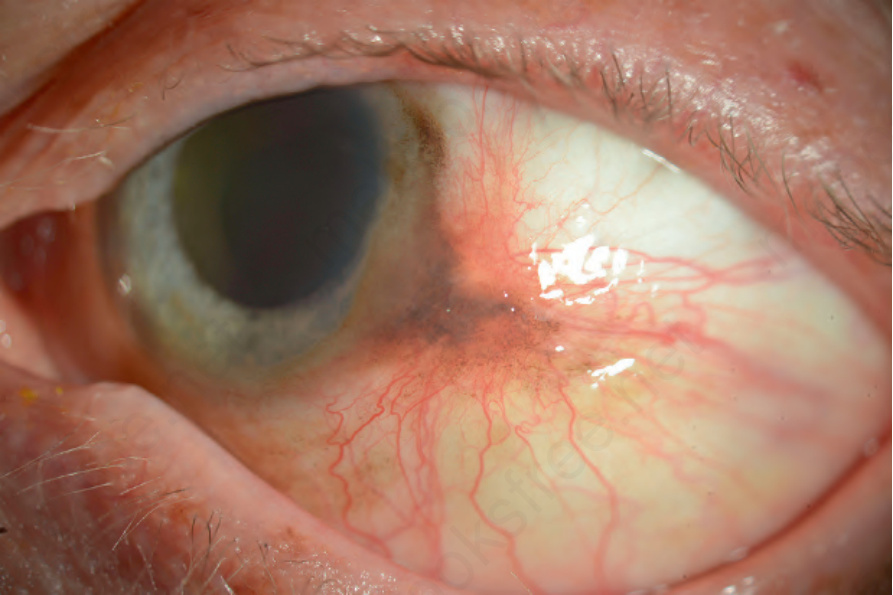
Fig. 27.41 Conjunctival melanoma: this tumor is more pink-brown with increased vascularity. The widespread pigmentation of the bulbar conjunctiva around the limbus and on the peripheral cornea likely represents PAM in this Caucasian patient.
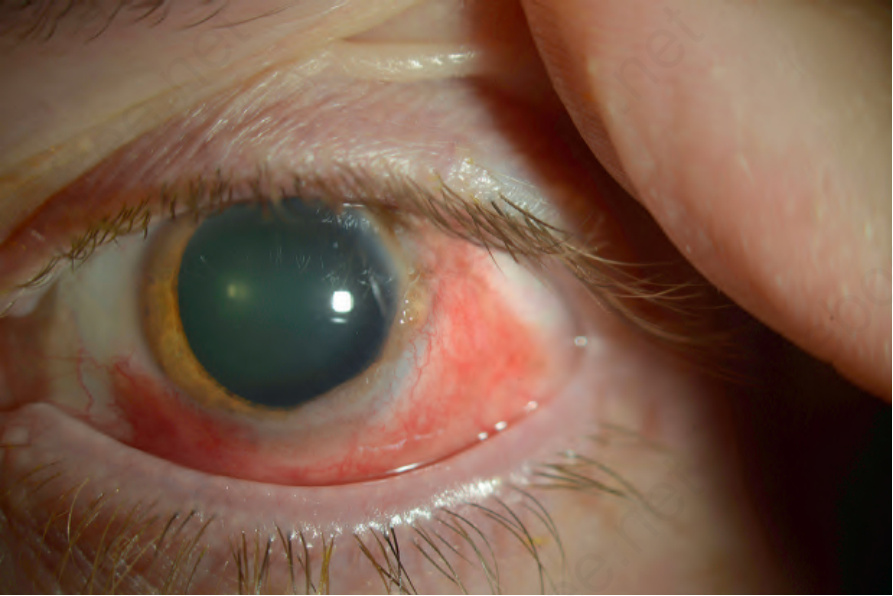
Fig. 27.42 Conjunctival melanoma: this tumor is more diffuse, surrounding the limbus for at least 180°. There is some nodularity at 3 o’clock. The tumor is relatively amelanotic with inflammation and prominent intrinsic vascularity.
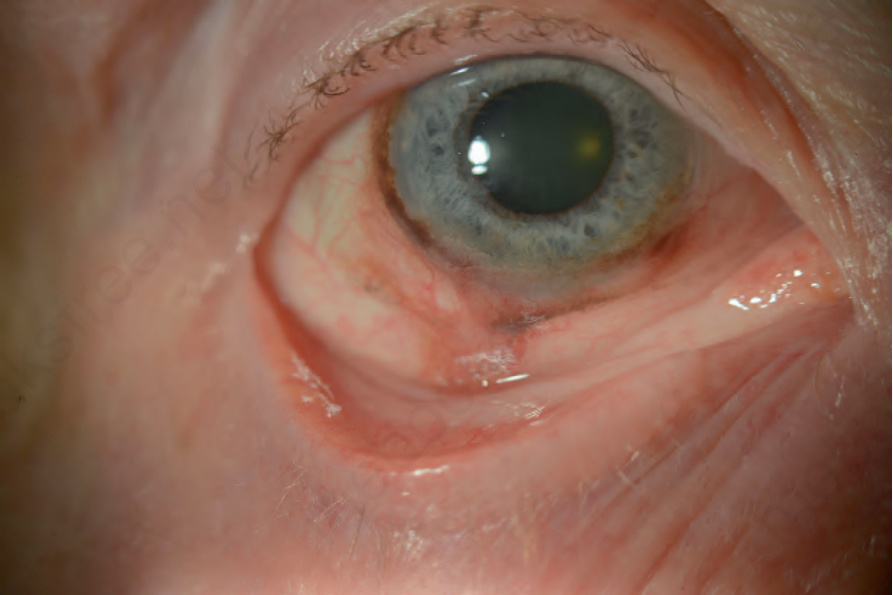
Fig. 27.43 Conjunctival melanoma: there is a melanoma involving the inferior bulbar conjunctiva, extending to the fornix.
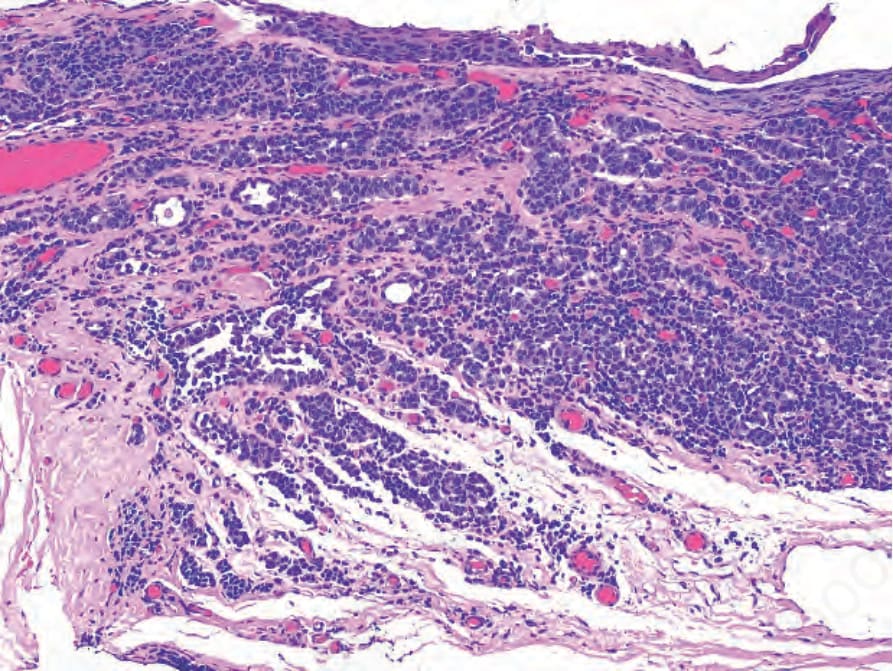
Fig. 27.44 Conjunctival melanoma: histology of Figure 27.42. The tumor arises in the context of primary acquired melanosis (PAM) with atypia, and shows nests of small, polyhedral, amelanotic melanoma cells invading the substantia propria. The tumor is quite vascular, and tumor nests intermingle with chronic inflammation.
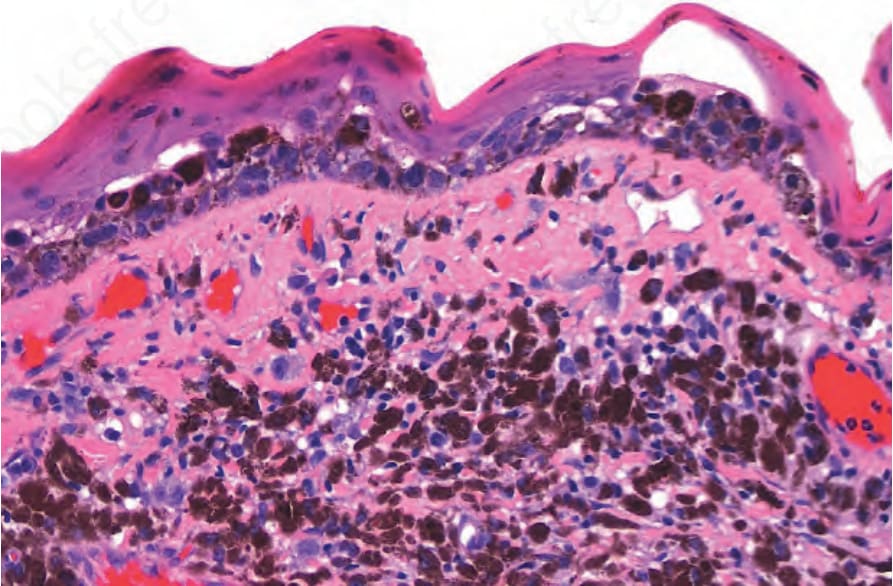
Fig. 27.45 Conjunctival melanoma: low-power view of a melanoma adjacent to the limbus (cornea is at the right of the image). Note how the intraepithelial component extends well beyond the subepithelial part of the tumor.
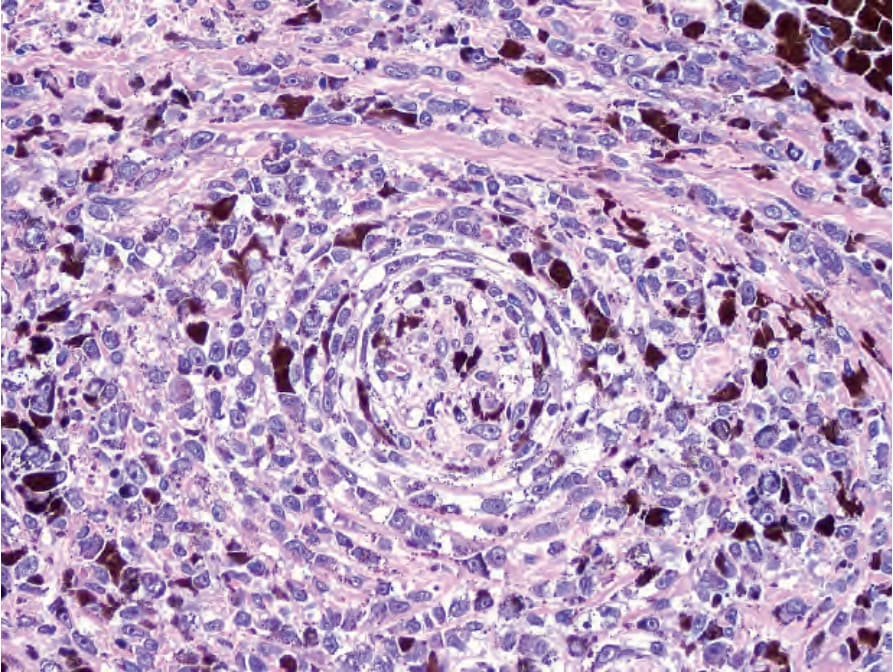
Fig. 27.46 Conjunctival melanoma: there is intraneural and perineural involvement.
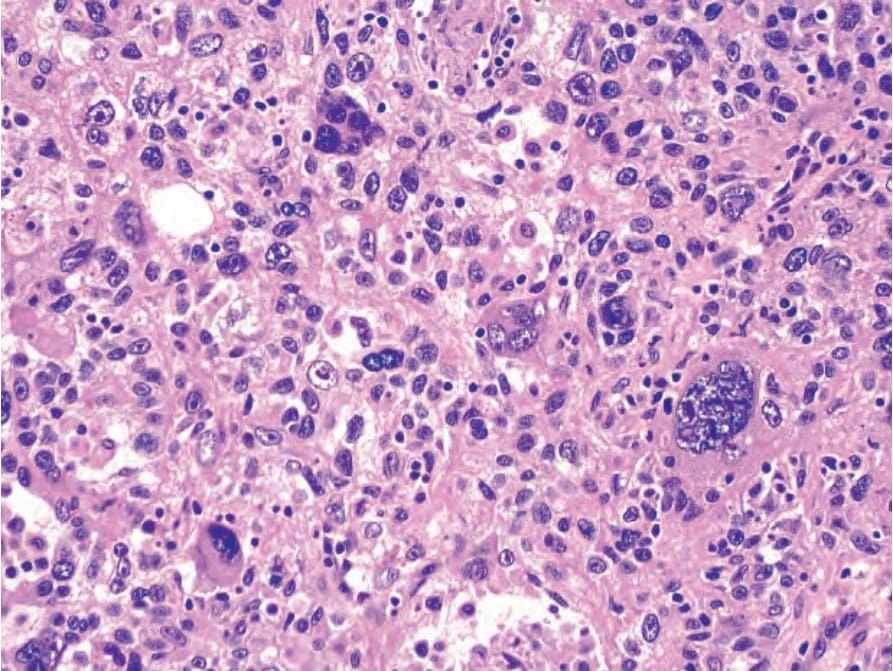
Fig. 27.47 Conjunctival melanoma: in this example, there are large, pleomorphic epithelioid cells and tumor giant cells with abundant eosinophilic cytoplasm and nuclei with prominent nucleoli.

Fig. 27.48 Extraocular extension of a ciliary body melanoma. (A) A brown-black multilobulated tumor with large feeder vessels is adjacent to the limbus. A portion of the intraocular component peeks out from the anterior chamber angle. (B) Histology shows a ciliary body melanoma that invades through the sclera to the subconjunctival space.