疾病定義與分類
- 紡錘細胞黑色素瘤 (spindled cell melanoma) 的促結締組織增生型 (desmoplastic) 與嗜神經型 (neurotropic) 變異是彼此相關的高惡性度腫瘤,常伴隨組織學診斷上的困難。
- 病史上常見被誤診為反應性纖維母細胞增生性病灶 (reactive fibroblastic proliferative lesion),此尤其與通常缺乏黑色素 (melanin pigment)、以及明顯表皮黑色素細胞侵犯相對少見有關,在復發性病灶中更是如此。
- desmoplastic melanoma 代表纖維母細胞性 (fibroblastic) 或肌纖維母細胞性 (myofibroblastic) 化生 (metaplasia) 的極端表現,並伴隨大量膠原合成。
- 在 neurotropic 變異中,化生可朝向 Schwann 細胞型 (Schwann cell-type) 分化。
- 雖然並非所有 desmoplastic melanoma 都具嗜神經性,也並非所有 neurotropic melanoma 都具促結締組織增生性,但許多作者將兩者視為同一主題的變化形式。
- 這些腫瘤一般而言伴隨高復發率、高轉移率與不良預後。
臨床特徵 (Clinical Features)
- 此腫瘤雖可發生於任何年齡,但多數發生於老年人(平均年齡 61 歲),並呈現男性偏多(男女比可高達 2.7 : 1),此點在明顯具嗜神經性的病灶中尤為明顯。
- 頭頸部最常受侵犯,但亦曾於多種部位被記載,包括軀幹及上、下肢。腿部在女性中特別容易受侵犯。
- 雖然這些腫瘤多數發生於日光損傷的皮膚、並以 lentigo maligna (melanoma) 為背景,但偶有發生於 superficial spreading melanoma 及 acral lentiginous melanoma(含甲下型,subungual variant)者被記載。
- desmoplastic melanoma 亦曾被描述發生於顎部 (palate)、牙齦 (gingiva)、唇 (lip)、外陰 (vulva)、肛門 (anus) 及結膜 (conjunctiva)。
- 雖然其上覆蓋的 lentigo maligna 色素性病灶可能引起對此腫瘤的注意,但更常見的是其表現為無色素性 (amelanotic)、膚色 (flesh-colored) 或紅斑性 (erythematous) 結節,或硬化斑塊 (indurated plaque)(圖 26.98 與 26.99)。
- 這些腫瘤以深部浸潤著稱,並常在診斷時已廣泛擴展。
- 除了造成高復發率外,嗜神經性 (neurotropism) 可導致周邊及顱神經病變 (peripheral and cranial neuropathy)。沿顱神經擴散進入顱底並最終侵犯腦膜 (meningeal involvement) 是一罕見但重要的併發症,其死亡率幾近 100%。
- 雖然多數 desmoplastic melanoma 發生於嚴重日光損傷的背景,但既往放射線照射(治療性或其他)偶具病因學重要性。罕見情況下,曾有併發於先天性黑色素細胞痣 (congenital melanocytic nevi) 甚至慢性燒傷疤痕 (chronic burns scarring) 的病例。
治療與預後 (Treatment & Prognosis)
- 復發常見(範圍 22–77%,平均 46%),且轉移(特別是轉移至肺)常隨之發生(範圍 11–56%,平均約 30%)。許多此類腫瘤發生的頭頸部區域,其局部控制尤其困難。
- 仔細評估手術邊緣 (surgical margins) 對局部控制至關重要。
- 令人意外的是,淋巴結擴散被記載的頻率非常低,因此有些人認為前哨淋巴結切片 (sentinel lymph node biopsy) 在此疾病中並非有效的分期工具。也有其他人未如此明顯地觀察到此現象,但這可能源於診斷標準的差異。
- 就此而言,謹慎界定 desmoplastic melanoma 很重要,須以純粹的促結締組織增生型 (pure desmoplastic pattern) 為主要型態,因為顯示有顯著(大於 10%)傳統型黑色素瘤成分的病例會表現出較具特徵性的淋巴結轉移。
- pure desmoplastic melanoma 在局部復發與轉移型態上表現得更像肉瘤 (sarcoma),其最常見的初始轉移部位為肺,而非區域淋巴結。
- 就疾病特異性存活率 (disease-specific survival) 而言,desmoplastic melanoma 的表現可能與典型黑色素瘤相似,其不良預後反映出絕大多數患者在就診時厚度增加(大於 1.5 mm)。也有其他人發現 desmoplastic melanoma 的疾病特異性存活率優於傳統黑色素瘤。
- 有些人報告 desmoplastic melanoma 的純型 (pure) 與混合型 (mixed) 變異具有相似的存活率。此議題仍有爭議,部分資料顯示 desmoplastic melanoma 患者的結果較佳。
- 不良預後指標包括高有絲分裂率 (high mitotic rate)、腫瘤厚度 (tumor thickness)、潰瘍 (ulceration) 與切除邊緣不足(< 1.0 cm)。
- 5 年存活率約為 70–80%,整體死亡率則由 11% 至 66% 不等。
組織病理特徵 (Histopathology)
- desmoplastic melanoma 的特徵為一瀰漫性浸潤、有時細胞稀疏 (paucicellular) 的惡性紡錘細胞腫瘤,伴隨顯著的間質纖維化 (interstitial fibrosis) 與膠原化 (collagenization)(圖 26.100 與 26.101)。其須與較常見、未伴隨顯著促結締組織增生 (desmoplasia) 的紡錘細胞黑色素瘤區分。
- 浸潤常使緊鄰表皮下的乳頭層真皮 (subepidermal papillary dermis) 不受影響,但在診斷時常已延伸至皮下脂肪或更深處。侵犯骨骼肌或下方骨骼並不少見。
- 腫瘤細胞學變化多端,細胞型態類似纖維母細胞 (fibroblasts)、平滑肌細胞 (smooth muscle cells) 或 Schwann 細胞。它們典型呈延長狀,具嗜酸性 (eosinophilic) 或更常見的嗜鹼性 (basophilic) 細胞質(圖 26.102)。
- 細胞核可能呈漸尖狀 (tapered) 且深染 (hyperchromatic),或呈雪茄狀 (cigar-shaped) 且為空泡狀 (vesicular),並具明顯的嗜酸性核仁 (eosinophilic nucleoli)(圖 26.103 與 26.104)。
- 有絲分裂稀少但可能明顯,有時可見異常型態(圖 26.105)。
- 最常見的是腫瘤呈明顯的束狀 (fascicular) 排列,但偶可見局灶性車輻狀 (storiform) 區域,此可導致被誤診為 dermatofibroma 或 dermatofibrosarcoma protuberans。
- 有時可見黏液樣變化 (myxoid change) 的病灶,使腫瘤呈現羽毛狀 (feathery) 外觀。
- 復發性腫瘤常為細胞稀疏,易被誤認為疤痕組織 (scar tissue)(圖 26.106 與 26.107)。
- 腫瘤巨細胞 (tumor giant cells) 為不常見的表現。
- 淋巴球浸潤 (lymphocytic infiltrates) 常以結節狀聚集 (nodular aggregates) 呈現,為一特徵性(但非診斷性)的表現(圖 26.108)。然而,它們在早期病灶中是有用的組織學指標。血管侵犯 (vascular invasion) 有時可見。
- 仔細審視其上覆蓋的表皮,並非少見地可顯示非典型黑色素細胞增生 (atypical melanocytic hyperplasia) 的特徵,最常為 lentigo maligna 型態。極偶爾可見 superficial spreading melanoma 的變化。
- 在相當比例的病例中未偵測到此類原位 (in situ) 變化(即所謂的 de novo 變異)(圖 26.109)。此是否代表退化 (regression)、取樣不足、原發性真皮腫瘤 (de novo dermal tumor),或先前已被治療過的原位成分,尚不確定。
- 在多數案例中,侵襲性腫瘤細胞群為無色素性 (amelanotic)。
- 罕見情況下可遇到血管變化,包括血管外皮細胞瘤樣特徵 (hemangiopericytomatous features) 與腎絲球樣血管病灶 (glomeruloid vascular lesions)。
- melanoma 的 neurotropic 變異可呈現一系列表現。顯微鏡下的神經周圍 (perineural) 或神經內 (endoneural) 侵犯在許多 desmoplastic melanoma 中常見(圖 26.110 與 26.111)。
- 然而,neurotropic(嗜神經性)一詞通常保留給神經侵犯非常顯著的病灶,更特別是當其導致神經不規則與增厚的臨床證據時。在罕見的例子中,腫瘤似乎局限於一神經幹 (nerve trunk),而對鄰近組織無可辨識的擴散。
- 偶爾,紡錘細胞群會顯示出令人聯想到 neurofibroma、schwannoma 或惡性神經鞘腫瘤 (malignant nerve sheath tumor) 的組織學特徵(有時稱為神經性轉化,neural transformation)(圖 26.112–26.114)。後者這些特徵常由較小的細胞構成,具淡嗜酸性細胞質與不規則波浪狀核 (irregular wavy nuclei),由不等量的膠原與基質 (ground substance) 分隔,有時使腫瘤呈現鬆散的黏液樣 (myxoid) 外觀。
- 有絲分裂活性變化多端,因此這些變異有時極具迷惑性,可導致被誤診為良性神經鞘腫瘤 (benign nerve sheath tumor)。
- 近期,有與深度血管浸潤相關的 neurotropic melanoma(即所謂的 angiotropic melanoma,血管趨向性黑色素瘤)被描述。
免疫組化與特殊染色 (Immunohistochemistry & Special Stains)
- 早期文獻曾記載某些陽性反應,但較近期的研究並未證實此觀察。
- p16 反應性喪失 (Loss of p16 reactivity) 在小型切片中需鑑別 desmoplastic melanoma 與 desmoplastic nevus 時可能有用,但並非所有 desmoplastic 病例都顯示喪失。
- P75 nerve growth factor receptor、WT1 與 nestin 等免疫組化標記亦被認為具臨床效用。
- desmoplastic melanoma 曾被描述與 MPNST 相關。MPNST 特徵性的 H3K27 細胞核染色喪失 (Loss of H3K27 nuclear staining),對於區分 MPNST 與黑色素瘤(無論是 desmoplastic 與否)並無幫助,因為部分黑色素瘤亦顯示此組蛋白三甲基化標記 (histone trimethylation marker) 的細胞核喪失。
- 評估疤痕 (scar) 與 desmoplastic melanoma 之間的鑑別可能很困難,因為 desmoplastic melanoma 中纖維化的程度可以非常廣泛,其間僅散布著零星的黑色素瘤細胞。同樣的問題也使邊緣 (margins) 的評估變得複雜。
- 在再切除 (re-excision) 的情況下使用多株 (polyclonal) S100 蛋白免疫組化可能很複雜,因為許多疤痕中由於散布的巨噬細胞 (macrophages) 與其他顯示 Schwann 細胞分化 (Schwannian differentiation) 的細胞而呈現局灶性 S100 反應性。
- 在這些情況下,謹慎評估這些紡錘細胞中細胞核深染 (nuclear hyperchromasia) 的程度至為重要。
致病機轉/分子 (Pathogenesis / Molecular)
- 轉移灶可能呈促結締組織增生性 (desmoplastic)、神經樣 (neuroid),或更明顯地呈黑色素細胞性 (melanocytic)。
- 雖然有些作者曾認為此促結締組織增生 (desmoplasia) 是反應性間質纖維母細胞增生 (reactive stromal fibroblast hyperplasia) 的結果,但現今一般已接受這些特徵源於黑色素細胞 (melanocytic derivation)。
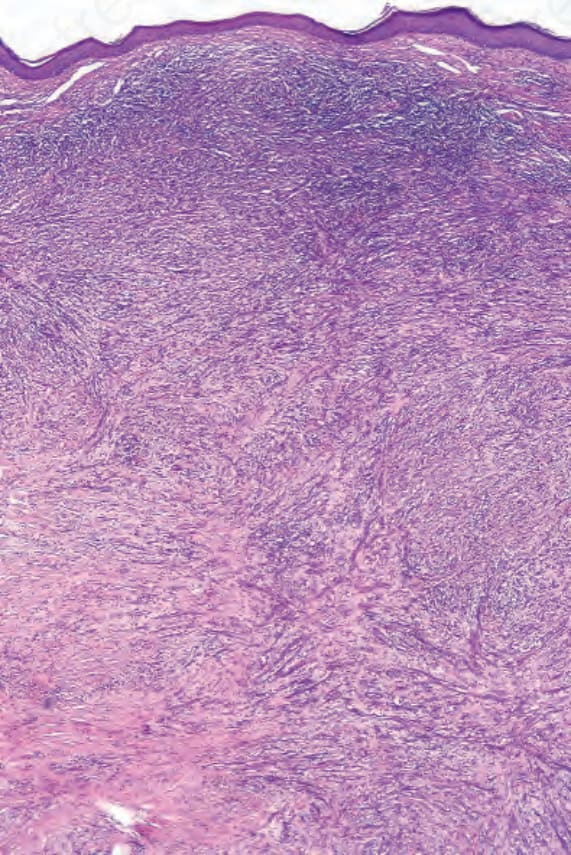
圖 26-100:促結締組織增生性黑色素瘤 (desmoplastic melanoma):低倍視野顯示一紡錘細胞腫瘤延伸貫穿真皮全層,並伴隨淺層淋巴樣浸潤 (superficial lymphoid infiltrates)。
Fig. 26.100 Desmoplastic melanoma: low-power view showing a spindle cell tumor extending throughout the full thickness of the dermis and associated with superficial lymphoid infiltrates.
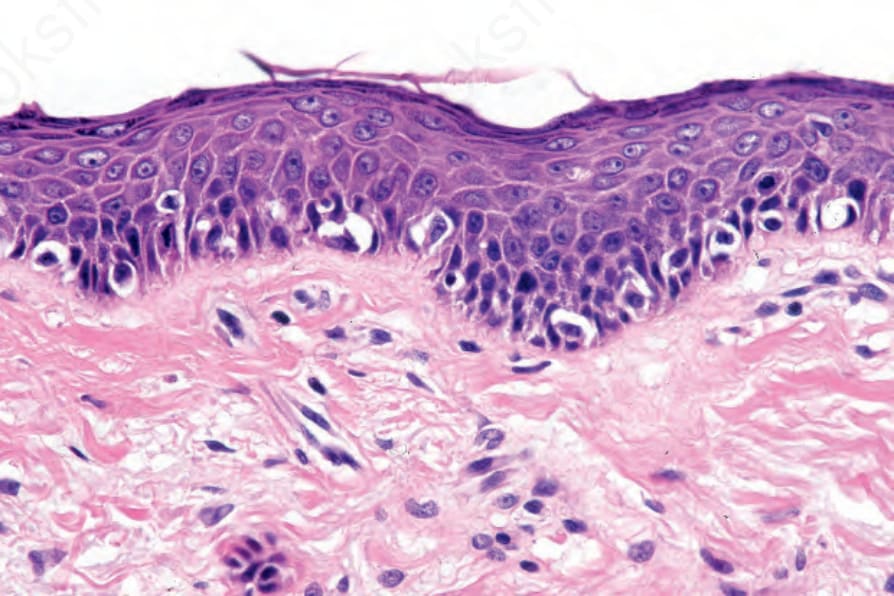
圖 26-101:促結締組織增生性黑色素瘤 (desmoplastic melanoma):其上覆蓋的表皮顯示非典型雀斑樣黑色素細胞增生 (atypical lentiginous melanocytic proliferation)。
Fig. 26.101 Desmoplastic melanoma: the overlying epidermis shows an atypical lentiginous melanocytic proliferation.
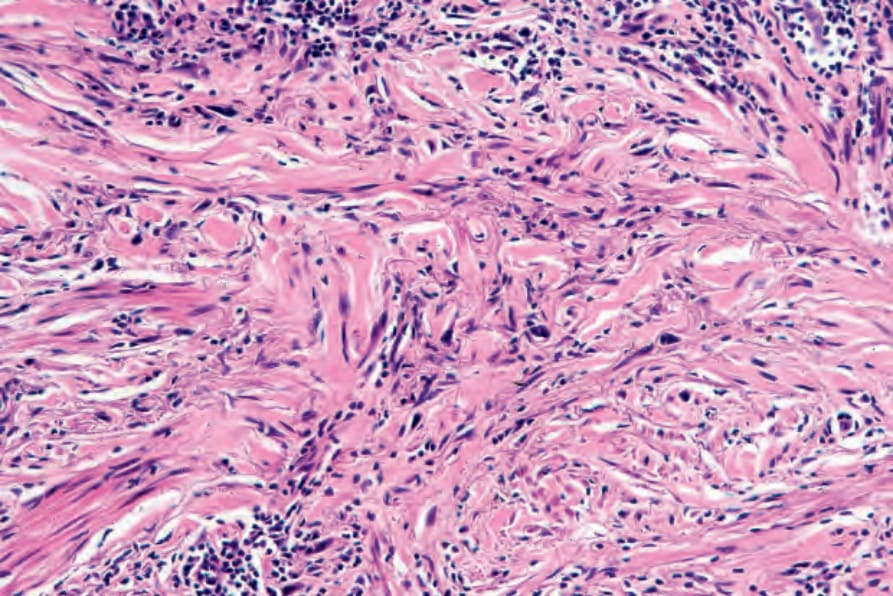
圖 26-102:促結締組織增生性黑色素瘤 (desmoplastic melanoma):腫瘤細胞具嗜鹼性細胞質 (basophilic cytoplasm),散布於緻密的膠原性間質中。
Fig. 26.102 Desmoplastic melanoma: the tumor cells have basophilic cytoplasm and are dispersed in a densely collagenous stroma.
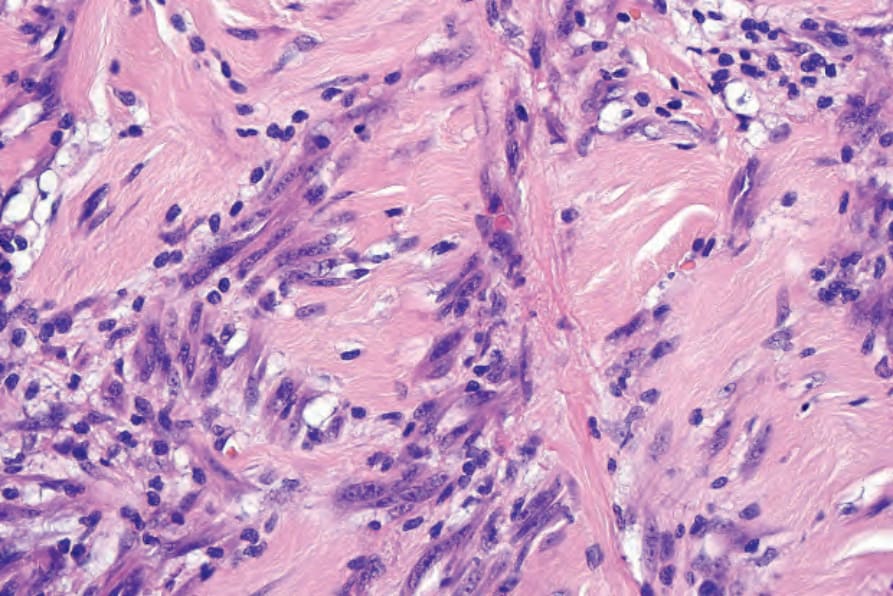
圖 26-103:促結締組織增生性黑色素瘤 (desmoplastic melanoma):細胞核呈空泡狀 (vesicular),核仁明顯。
Fig. 26.103 Desmoplastic melanoma: nuclei are vesicular and nucleoli are prominent.
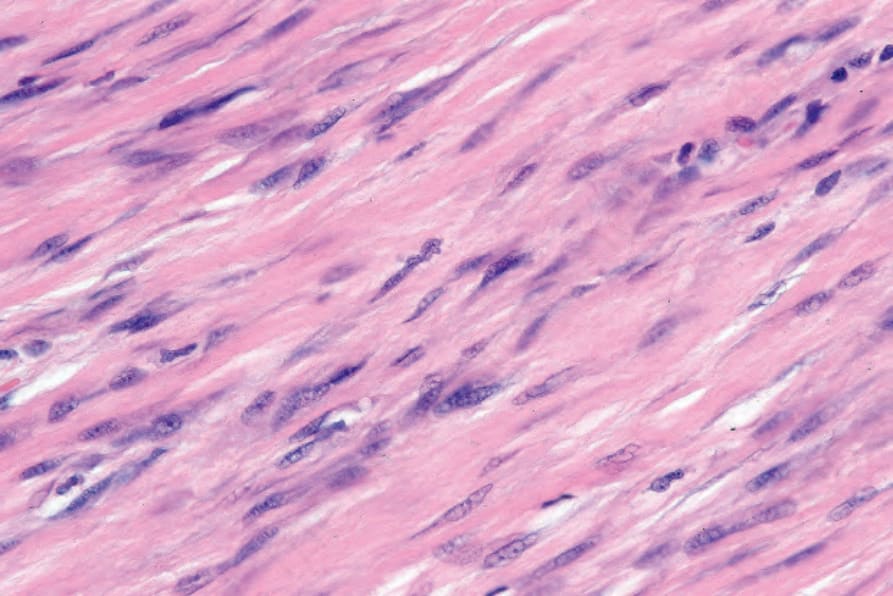
圖 26-104:促結締組織增生性黑色素瘤 (desmoplastic melanoma):腫瘤細胞受鄰近的硬化纖維性間質 (sclerotic fibrous stroma) 壓迫。
Fig. 26.104 Desmoplastic melanoma: the tumor cells are compressed by the adjacent sclerotic fibrous stroma.
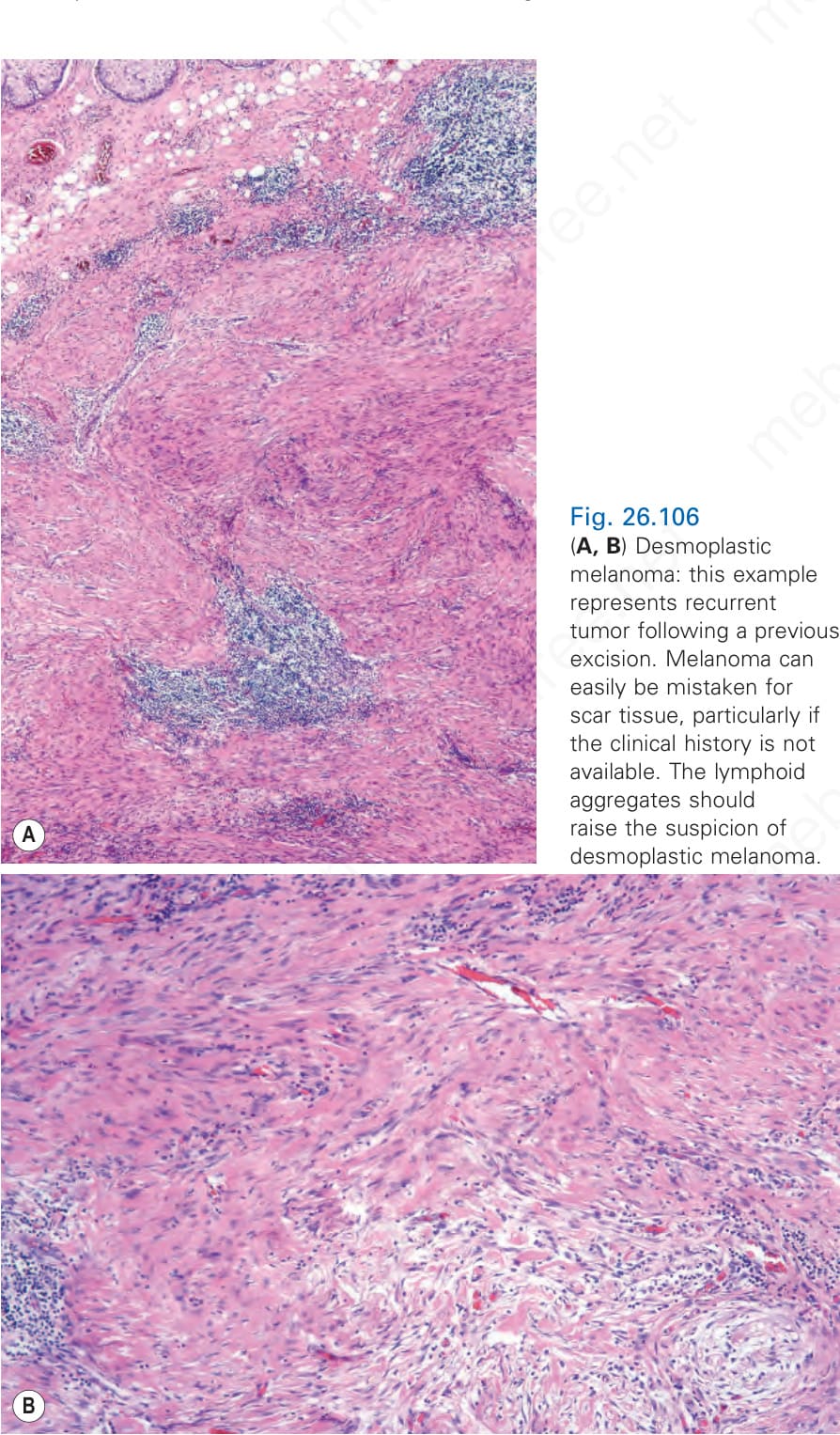
圖 26-105:促結締組織增生性黑色素瘤 (desmoplastic melanoma):注意中央的有絲分裂像 (mitotic figure)。
Fig. 26.105 Desmoplastic melanoma: note the central mitotic figure.
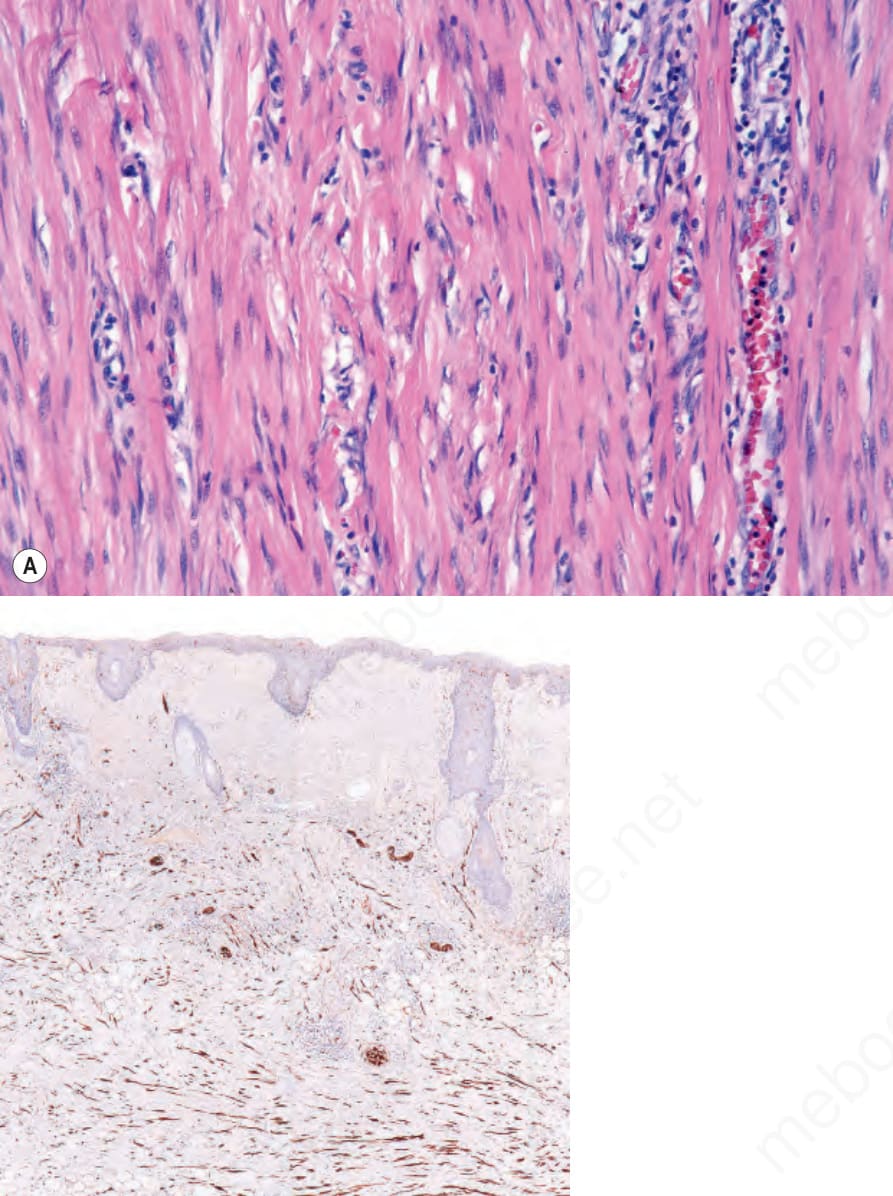
圖 26-106:(A, B) 促結締組織增生性黑色素瘤 (desmoplastic melanoma):此例代表先前切除後的復發性腫瘤。黑色素瘤可輕易被誤認為疤痕組織 (scar tissue),尤其在無臨床病史可參考時。淋巴樣聚集 (lymphoid aggregates) 應引起對 desmoplastic melanoma 的懷疑。
Fig. 26.106 (A, B) Desmoplastic melanoma: this example represents recurrent tumor following a previous excision. Melanoma can easily be mistaken for scar tissue, particularly if the clinical history is not available. The lymphoid aggregates should raise the suspicion of desmoplastic melanoma.
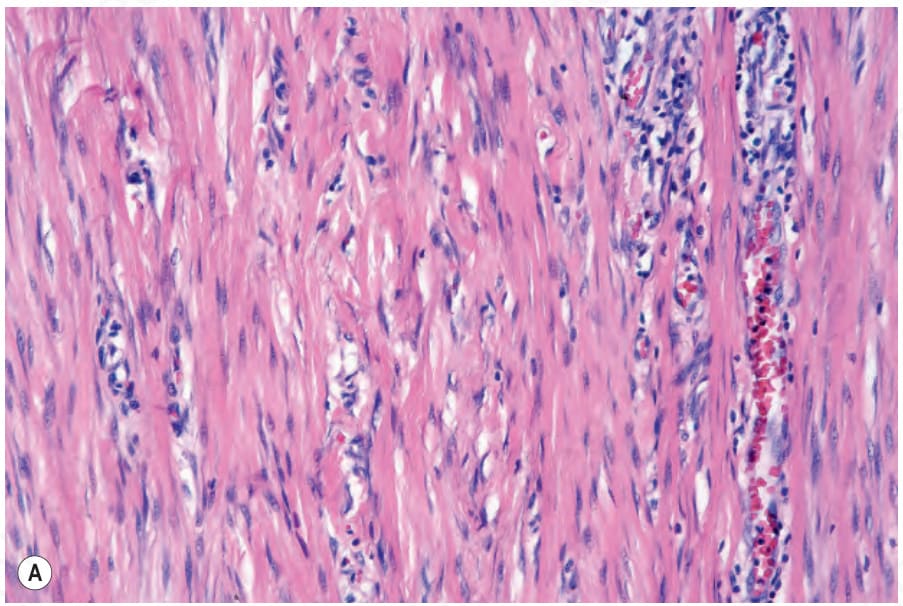
圖 26-107:促結締組織增生性黑色素瘤 (desmoplastic melanoma):(A) 圖 26.106 所示腫瘤的高倍視野;(B) S100 蛋白免疫組化突顯出可觀的腫瘤細胞群。
Fig. 26.107 Desmoplastic melanoma: (A) high-power view of tumor shown in Figure 26.106; (B) immunohistochemistry for S100 protein highlights the considerable tumor cell population.
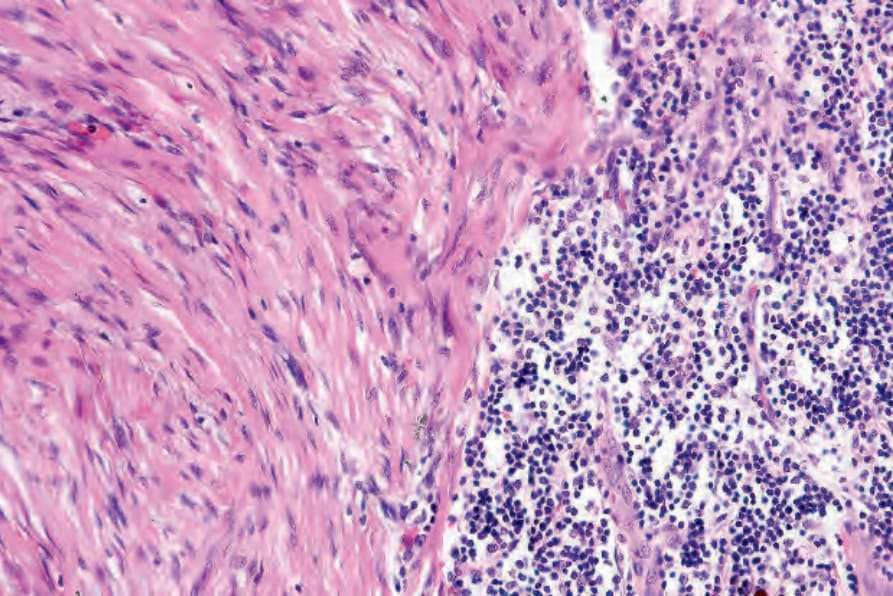
圖 26-108:促結締組織增生性黑色素瘤 (desmoplastic melanoma):淋巴球的結節狀聚集 (nodular aggregates of lymphocytes) 是有用的診斷線索。
Fig. 26.108 Desmoplastic melanoma: nodular aggregates of lymphocytes are a useful diagnostic clue.
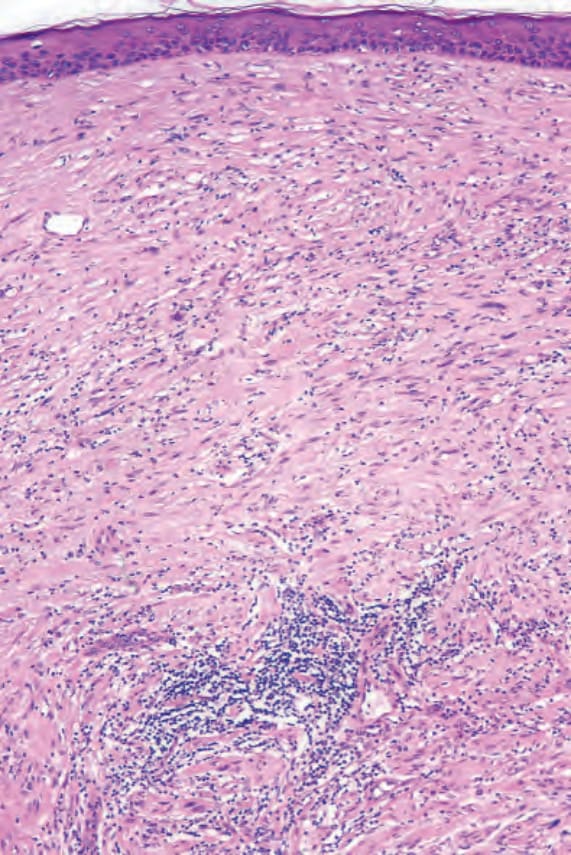
圖 26-109:促結締組織增生性黑色素瘤 (desmoplastic melanoma):此例中,其上覆蓋的表皮未顯示先前存在的非典型黑色素細胞增生性病灶之證據(即所謂的 de novo 變異)。
Fig. 26.109 Desmoplastic melanoma: in this example, the overlying epidermis shows no evidence of a pre-existent atypical melanocytic proliferative lesion (the so-called de novo variant).
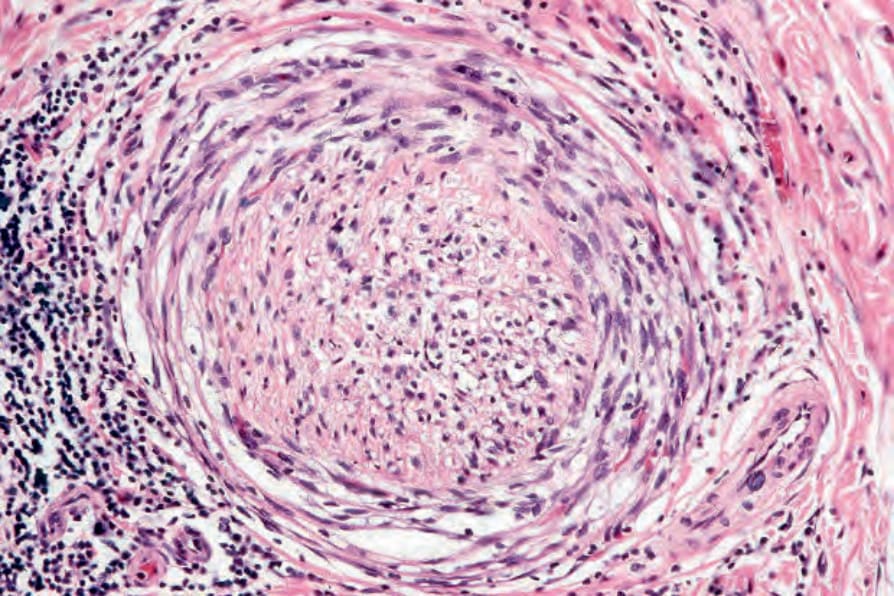
圖 26-110:促結締組織增生性黑色素瘤 (desmoplastic melanoma):神經周圍浸潤 (perineural infiltration) 非常常見,這在某種程度上解釋了此腫瘤的高復發率。
Fig. 26.110 Desmoplastic melanoma: perineural infiltration is very commonly present, accounting in part for the high recurrence rate of this tumor.
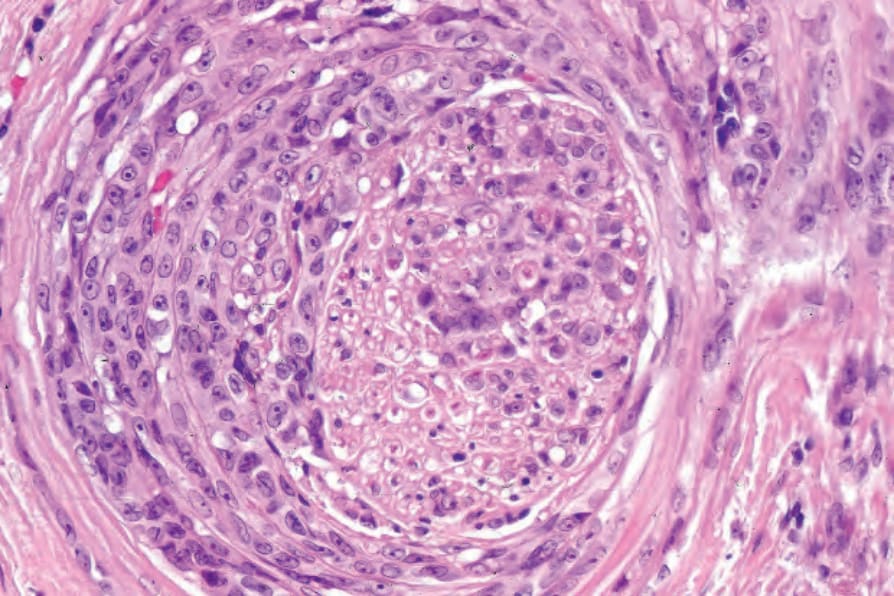
圖 26-111:促結締組織增生性黑色素瘤 (desmoplastic melanoma):腫瘤內有時可見上皮樣細胞 (epithelioid cells)。此例顯示廣泛的神經周圍與神經內擴散 (peri- and intraneural spread)。
Fig. 26.111 Desmoplastic melanoma: epithelioid cells are sometimes encountered within the tumor. This example shows extensive peri- and intraneural spread.
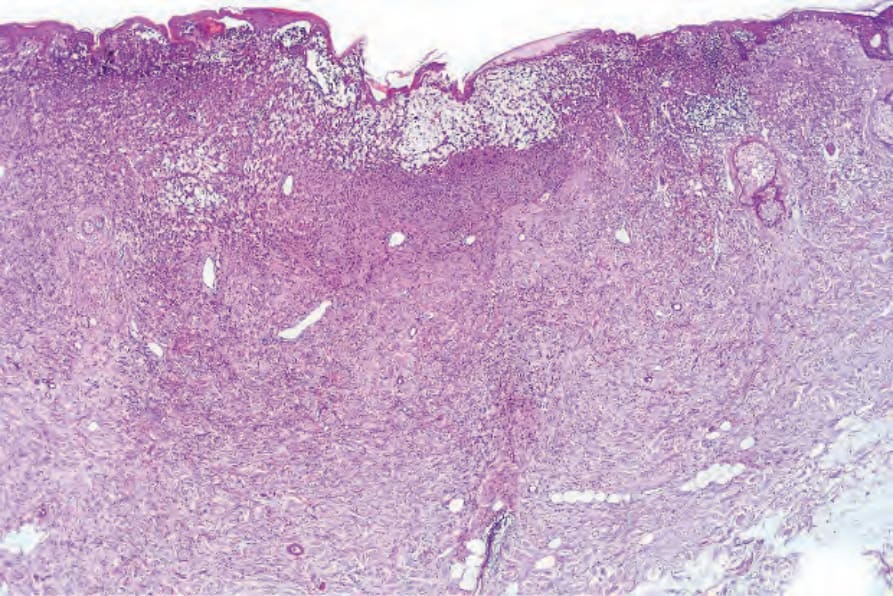
圖 26-112:促結締組織增生性黑色素瘤(神經性轉化,neural transformation):一已浸潤貫穿真皮全層之腫瘤的低倍視野。
Fig. 26.112 Desmoplastic melanoma (neural transformation): low-power view of a tumor which has infiltrated through the full thickness of the dermis.
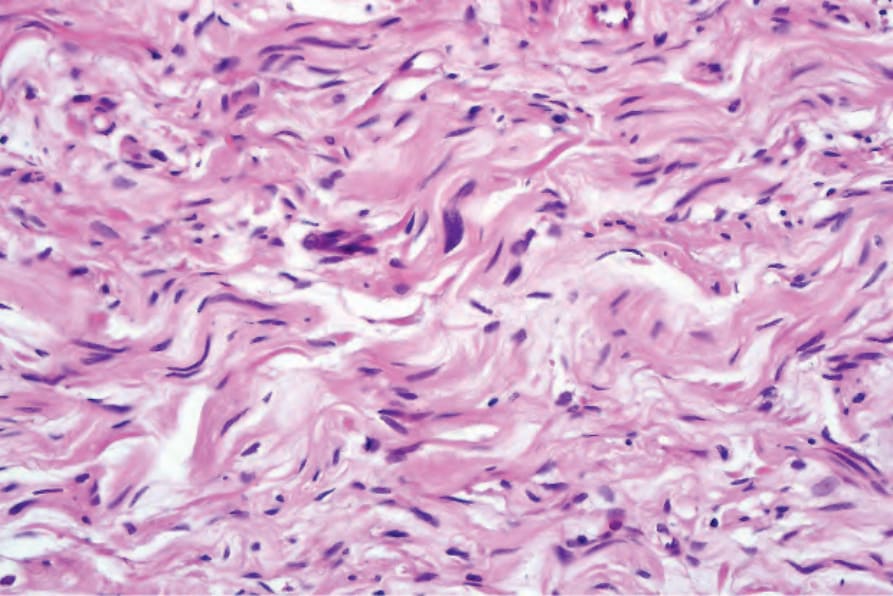
圖 26-113:促結締組織增生性黑色素瘤(神經性轉化,neural transformation):腫瘤細胞具小型、扭曲、逗點狀的細胞核,伴邊界不清的嗜酸性細胞質,令人聯想到周邊神經鞘腫瘤 (peripheral nerve sheath tumor)。注意細胞核深染 (nuclear hyperchromatism)。
Fig. 26.113 Desmoplastic melanoma (neural transformation): the tumor cells have small, twisted, and comma-shaped nuclei with ill-defined eosinophilic cytoplasm reminiscent of peripheral nerve sheath tumor. Note the nuclear hyperchromatism.
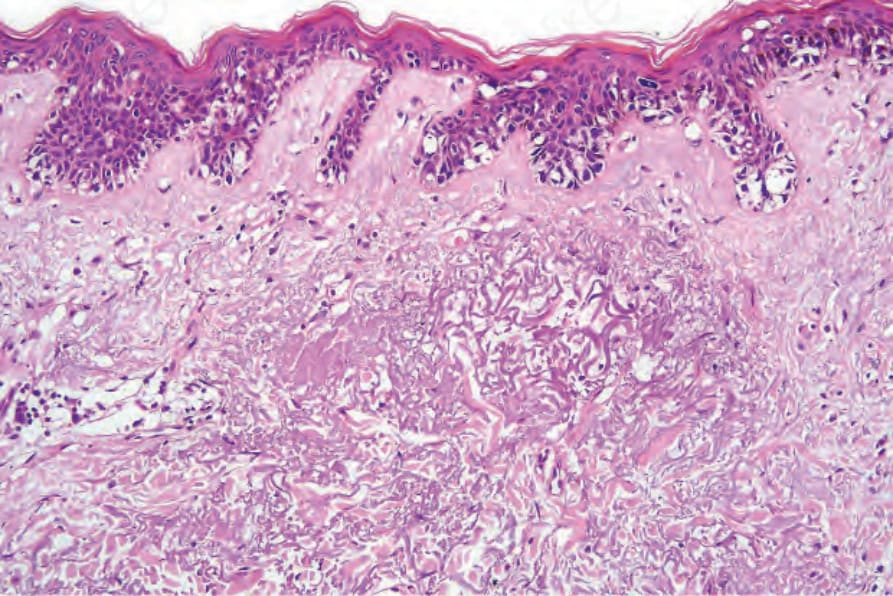
圖 26-114:促結締組織增生性黑色素瘤 (desmoplastic melanoma):鄰近的表皮顯示非典型黑色素細胞雀斑樣增生 (atypical melanocytic lentiginous hyperplasia)。
Fig. 26.114 Desmoplastic melanoma: the adjacent epidermis shows atypical melanocytic lentiginous hyperplasia.
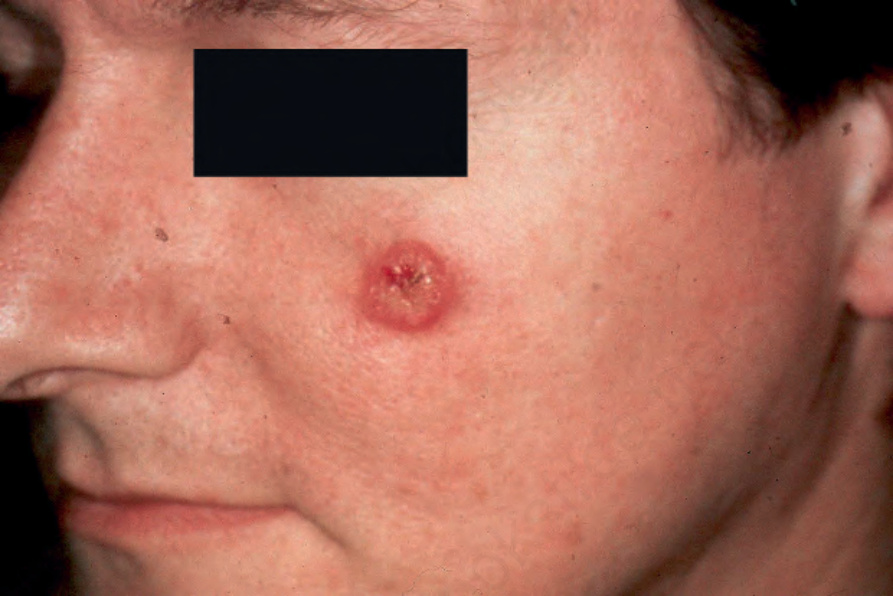
圖 26-98:促結締組織增生性黑色素瘤 (desmoplastic melanoma):這些腫瘤常為無色素性 (amelanotic),如此患者所見。承蒙 E. Wilson Jones, MD, Institute of Dermatology, London, UK 提供。
Fig. 26.98 Desmoplastic melanoma: these tumors are frequently amelanotic, as seen in this patient. By courtesy E. Wilson Jones, MD, Institute of Dermatology, London, UK.

圖 26-99:促結締組織增生性黑色素瘤 (desmoplastic melanoma):此腫瘤起初被認為代表一囊腫 (cyst)。承蒙 E. Wilson Jones, MD, Institute of Dermatology, London, UK 提供。
Fig. 26.99 Desmoplastic melanoma: this tumor was initially thought to represent a cyst. By courtesy of E. Wilson Jones, MD, Institute of Dermatology, London, UK.