Desmoplastic and neurotropic melanoma
Desmoplastic and neurotropic melanoma
Desmoplastic and neurotropic variants of spindled cell melanoma are inter-related high-grade tumors that are commonly associated with histologic
1345 Desmoplastic and neurotropic melanoma
diagnostic difficulty.1–7 A history of a mistaken diagnosis of reactive fibroblastic proliferative lesion is common and relates particularly to the usual absence of melanin pigment and the relative infrequency of obvious epidermal melanocytic involvement, particularly in recurrent lesions. Desmoplastic melanoma represents an extreme degree of fibroblastic or myofibroblastic metaplasia accompanied by abundant collagen synthesis. In the neurotropic variant, the metaplasia may be towards Schwann cell-type differentiation. Although not all desmoplastic melanomas are neurotropic and not all neurotropic melanomas are desmoplastic, many authors regard them as variations on a theme.8 These tumors are in general associated with a high incidence of recurrence and metastasis and a poor prognosis.
Clinical features Although the tumor may present at any age, the majority arise in the elderly (mean age 61 years) and show a male preponderance (as high as 2.7 : 1), which is particularly evident with the frankly neurotropic lesions.3,9–17 The head and neck are most frequently affected, but examples have been documented at a wide range of sites, including the trunk and upper or lower limbs.9,18 The leg is particularly involved in females.3 Although the majority of these neoplasms arise on sun-damaged skin in a background of lentigo maligna (melanoma), superficial spreading and acral lentiginous melanomas, including subungual variants, have occasionally been documented.12,13 Desmoplastic melanoma has also been described on the palate, gingiva, lip, vulva, anus, and conjunctiva.19 Although a superimposed pigmented lesion of lentigo maligna may draw attention to this tumor, more often they present as amelanotic, flesh-colored or erythematous nodules or indurated plaques (Figs 26.98 and 26.99). These tumors are notoriously deeply infiltrative and commonly have extended widely by the time of diagnosis. In addition to contributing to the high incidence of recurrence, neurotropism may result in peripheral and cranial neuropathy. Spread along the cranial nerves into the base of the skull with eventual meningeal involvement is a rare but important complication with an almost 100% mortality.18,20 Although most desmoplastic melanomas arise in a background of severe sun damage, previous irradiation (therapeutic or otherwise) is occasionally of etiological importance.9 Rarely, examples have complicated congenital melanocytic nevi and even chronic burns scarring.21,22
disease.3,24–30 Others have not observed this phenomenon as starkly, but this could be due to differences in diagnostic criteria.31–34 In this regard it is important to define desmoplastic melanoma carefully with the pure desmoplastic pattern being the predominant one, as cases showing a significant component (greater than 10%) of traditional melanoma show the more characteristic metastasis to lymph node.35–37 Pure desmoplastic melanoma appears to behave more like a sarcoma in terms of local recurrence and metastatic pattern with the lung being the most common initial site rather than regional lymph nodes. In regard to disease-specific survival, desmoplastic melanoma may behave similarly to classic melanoma, the poor prognosis reflecting an increased thickness of greater than 1.5 mm at presentation in the vast majority of patients.3,38 Others have found that disease-specific survival for desmoplastic melanoma is superior to conventional melanoma.28 Pure and mixed variants of desmoplastic melanoma are reported by some to have similar survival.39 There is some debate on this topic, with some data that indicate an improved outcome for desmoplastic melanoma patients.28,40–42 Poor prognostic indicators are high mitotic rate, tumor thickness, ulceration, and inadequate excision margins (< 1.0 cm).3,17,23,43 The 5-year survival rate is of the order of 70–80%, and the overall mortality varies from 11% to 66%.3,15,23
Histologic features Desmoplastic melanoma is characterized by a diffusely infiltrative, sometimes paucicellular, malignant spindle cell tumor with marked interstitial fibrosis and collagenization (Figs 26.100 and 26.101).1,2,9,19,44,45 It is to be distinguished from the more common spindled cell melanoma unassociated with significant desmoplasia.
Recurrence is common (range 22–77%, mean 46%) and metastasis (particularly to the lungs) frequently supervenes (range 11–56%, mean of approximately 30%).10,15 Local control in the head and neck region, where many of these tumors arise, is particularly problematic.23 Careful evaluation of surgical margins is critical for local control.17 Surprisingly, nodal spread has been documented very infrequently such that sentinel lymph node biopsy is not regarded by some as an effective staging tool in this
The infiltrate often leaves the immediate subepidermal papillary dermis unaffected, but frequently is found to extend into the subcutaneous fat or beyond at the time of diagnosis. Involvement of skeletal muscle or underlying bone is not uncommon. The tumor cytology is variable, the cells resembling fibroblasts, smooth muscle cells, or Schwann cells. They are typically elongated and have eosinophilic or more commonly basophilic cytoplasm (Fig. 26.102). Nuclei may be tapered and hyperchromatic or cigar-shaped and vesicular with prominent eosinophilic nucleoli (Figs 26.103 and 26.104). Mitoses are scanty but may be conspicuous, and sometimes abnormal forms are present (Fig. 26.105). Most commonly, the tumor has a distinctly fascicular arrangement, but focal storiform areas are occasionally evident, which can result in a mistaken diagnosis of dermatofibroma or dermatofibrosarcoma protuberans. Foci of myxoid change, giving the tumor a feathery appearance, are sometimes seen. Recurrent tumors are frequently paucicellular and are easily taken for scar tissue (Figs 26.106 and 26.107). Tumor giant cells are an infrequent manifestation. Lymphocytic infiltrates,
1346 Melanoma
often evident as nodular aggregates, are a characteristic (but not diagnostic) feature (Fig. 26.108). They are, however, a useful histologic pointer in early lesions.46,47 Vascular invasion is sometimes present.
Careful scrutiny of the overlying epidermis not uncommonly shows features of atypical melanocytic hyperplasia, most often of the lentigo maligna pattern.9 Very occasionally, the changes of superficial spreading melanoma are present. In a significant proportion of cases no such in situ change is detected (the so-called de novo variant) (Fig. 26.109). Whether this represents regression, inadequate sampling, a de novo dermal tumor, or a previously treated in situ component is uncertain. In most examples, the invasive tumor cell population is amelanotic.9
Vascular changes including hemangiopericytomatous features and glomeruloid vascular lesions may rarely be encountered.48
The neurotropic variant of melanoma may show a range of manifestations.2,9,19,48 Microscopic perineural or endoneural involvement is common
1347 Desmoplastic and neurotropic melanoma
A
A
B
B
1348 Melanoma
in many desmoplastic melanomas (Figs 26.110 and 26.111). The term neurotropic, however, is often reserved for lesions where nerve involvement is very marked or more particularly when it results in clinical evidence of nerve irregularity and thickening. In rare examples, the tumor appears to be limited to a nerve trunk with no discernible spread to the adjacent tissues.9 Occasionally, the spindled cell population displays histologic features reminiscent of neurofibroma, schwannoma, or malignant nerve sheath tumor (sometimes known as neural transformation) (Figs 26.112–26.114).18,49 These latter features often comprise smaller cells, with pale eosinophilic cytoplasm and irregular wavy nuclei separated by variable amounts of collagen and ground substance and sometimes giving the tumor a loose myxoid appearance. Mitotic activity is variable and therefore these variants can sometimes be very deceptive, resulting in a mistaken diagnosis of benign nerve sheath tumor. Recently, neurotropic melanoma associated with profound vascular infiltration (so-called angiotropic melanoma) has
1349 Desmoplastic and neurotropic melanoma
positivity was documented in the earlier literature, more recent studies have not confirmed this observation.70,71 Loss of p16 reactivity can be useful in distinguishing desmoplastic melanoma from desmoplastic nevus when this differential diagnosis arises in small biopsies, but not all desmoplastic cases show loss.72,73 P75 nerve growth factor receptor,WT1, and nestin immunohistochemical markers have also been suggested to have clinical utility.74–76 Desmoplastic melanoma has been described to MPNST. Loss of H3K27 nuclear staining characteristic of MPNST is not helpful for distinguishing MPNST from melanoma, desmoplastic, or otherwise, as a subset of melanomas also show nuclear loss of this histone trimethylation marker.77
Evaluation of scar versus desmoplastic melanoma can be difficult as the degree of fibrosis in desmoplastic melanoma can be extensive with only scattered melanoma cells. This same problem complicates the assessment of margins. Use of polyclonal S100 protein immunohistochemistry in the setting of re-excision can be complex given the focal S100 reactivity present in many scars due to scattered macrophages and other cells showing Schwannian differentiation.78 Careful assessment of the degree of nuclear hyperchromasia in these spindled cells is paramount in evaluating these situations.79
Metastases may be desmoplastic, neuroid, or more obviously melanocytic. Although some authors have suggested that the desmoplasia is a consequence of reactive stromal fibroblast hyperplasia, it is now generally accepted that these features are of melanocytic derivation.
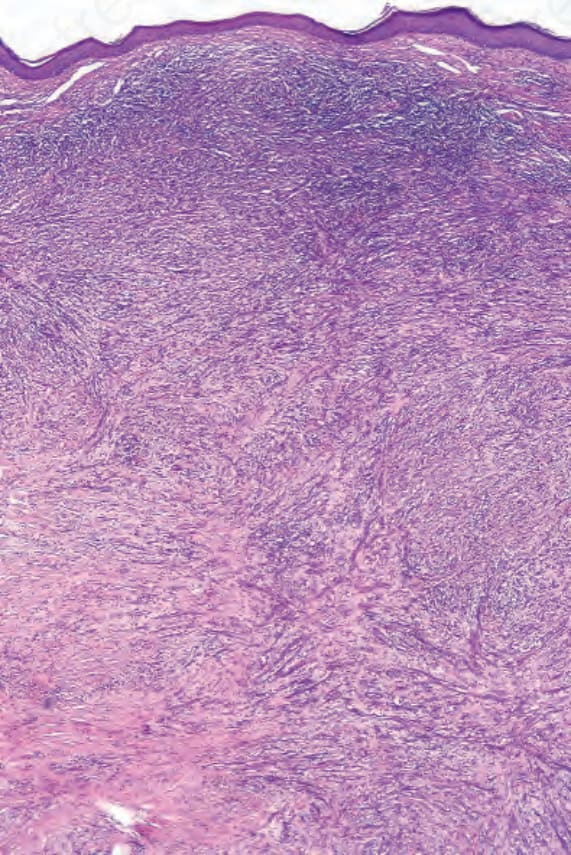
Fig. 26.100 Desmoplastic melanoma: low-power view showing a spindle cell tumor extending throughout the full thickness of the dermis and associated with superficial lymphoid infiltrates.
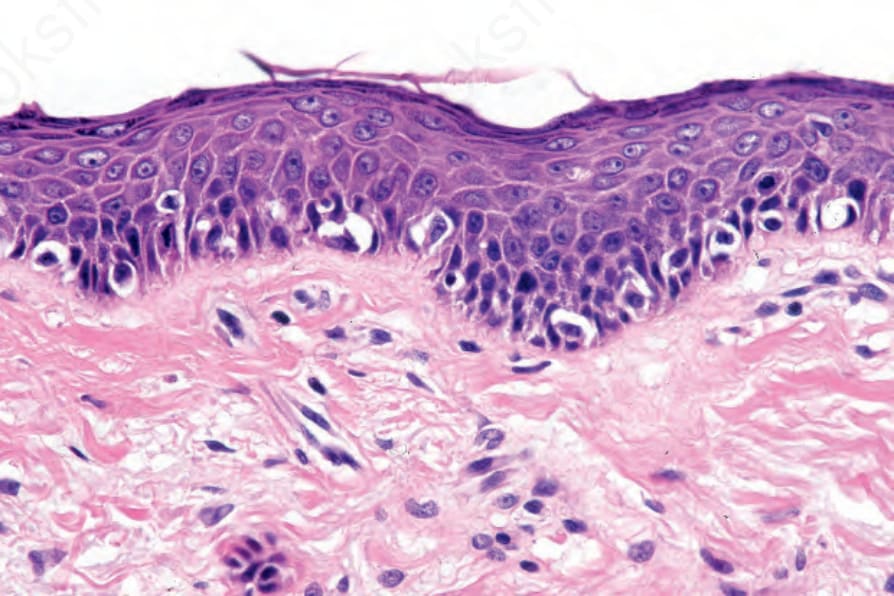
Fig. 26.101 Desmoplastic melanoma: the overlying epidermis shows an atypical lentiginous melanocytic proliferation.
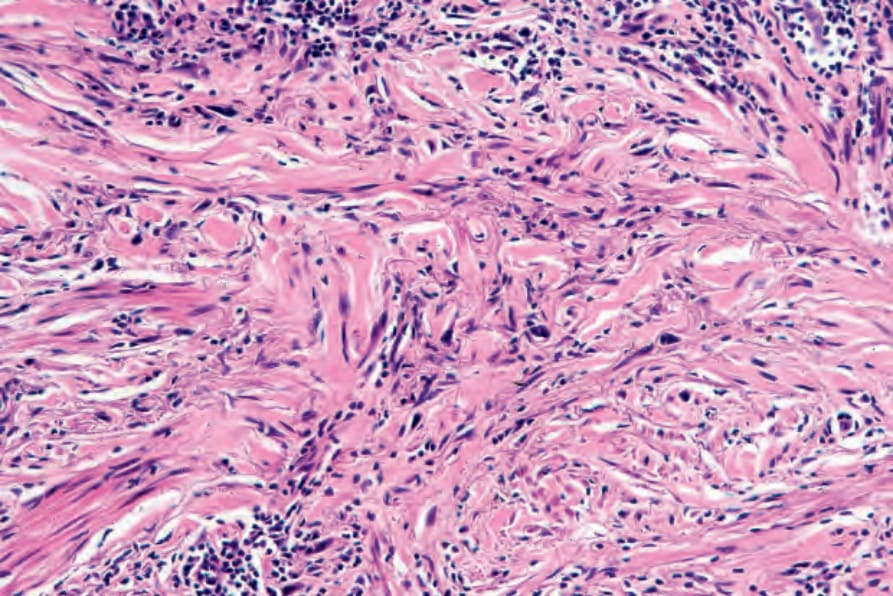
Fig. 26.102 Desmoplastic melanoma: the tumor cells have basophilic cytoplasm and are dispersed in a densely collagenous stroma.
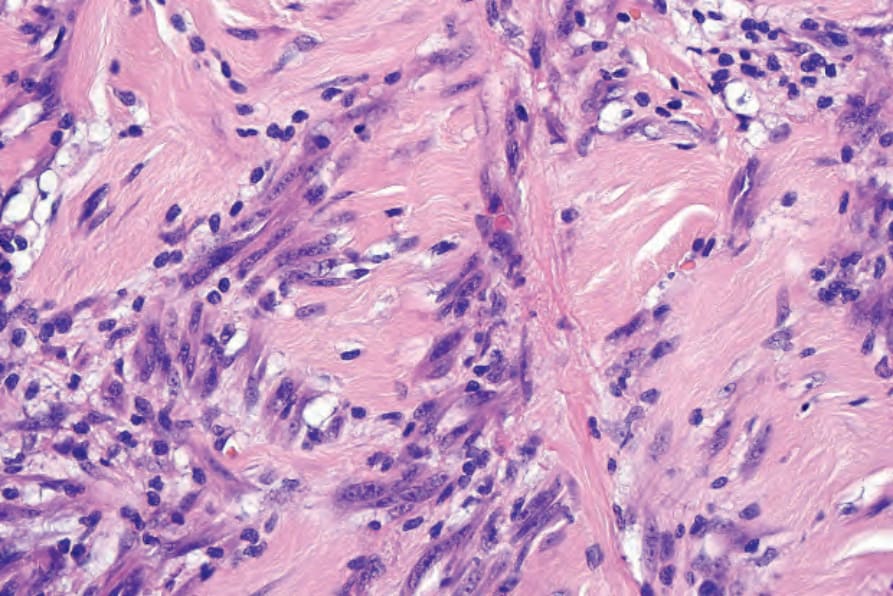
Fig. 26.103 Desmoplastic melanoma: nuclei are vesicular and nucleoli are prominent.
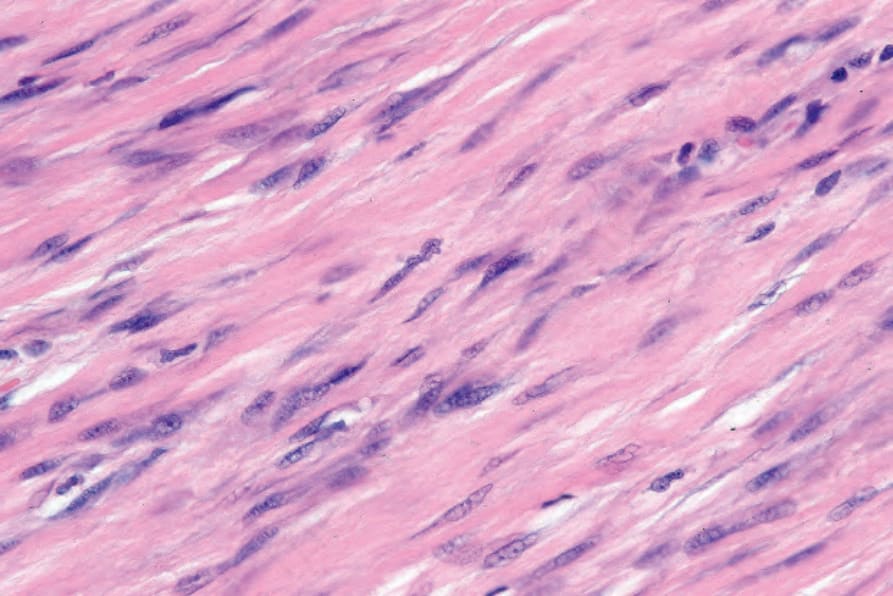
Fig. 26.104 Desmoplastic melanoma: the tumor cells are compressed by the adjacent sclerotic fibrous stroma.
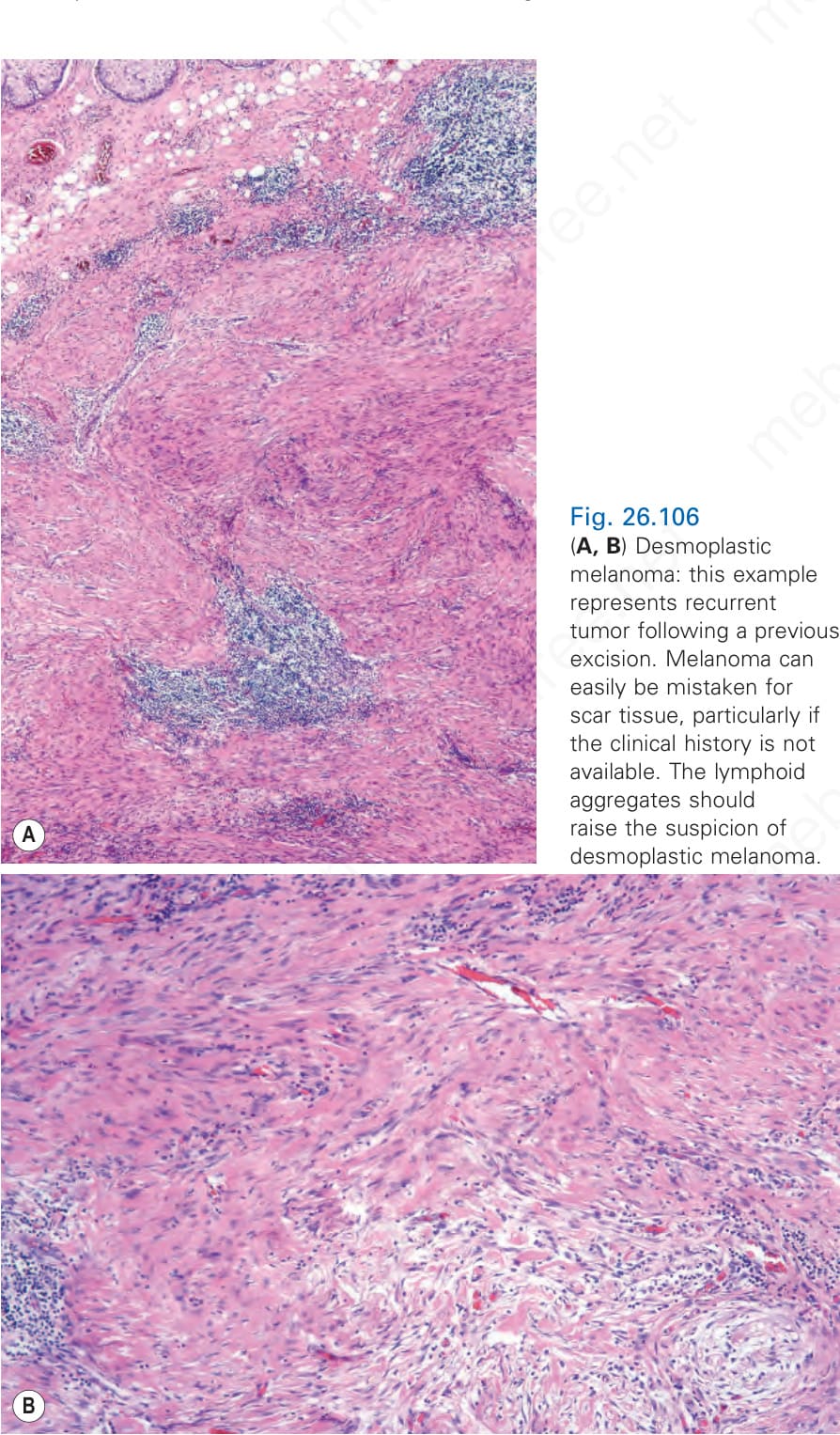
Fig. 26.105 Desmoplastic melanoma: note the central mitotic figure.
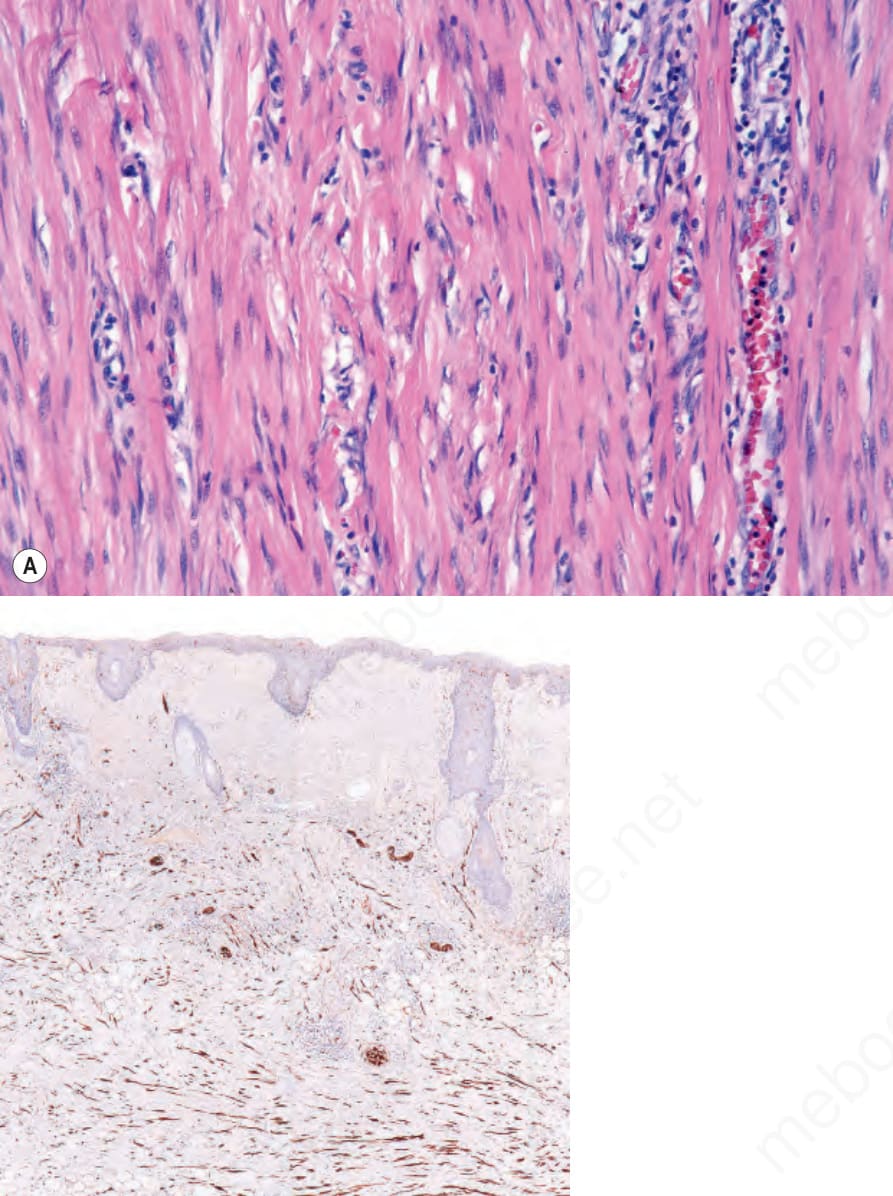
Fig. 26.106 (A, B) Desmoplastic melanoma: this example represents recurrent tumor following a previous excision. Melanoma can easily be mistaken for scar tissue, particularly if the clinical history is not available. The lymphoid aggregates should raise the suspicion of desmoplastic melanoma.
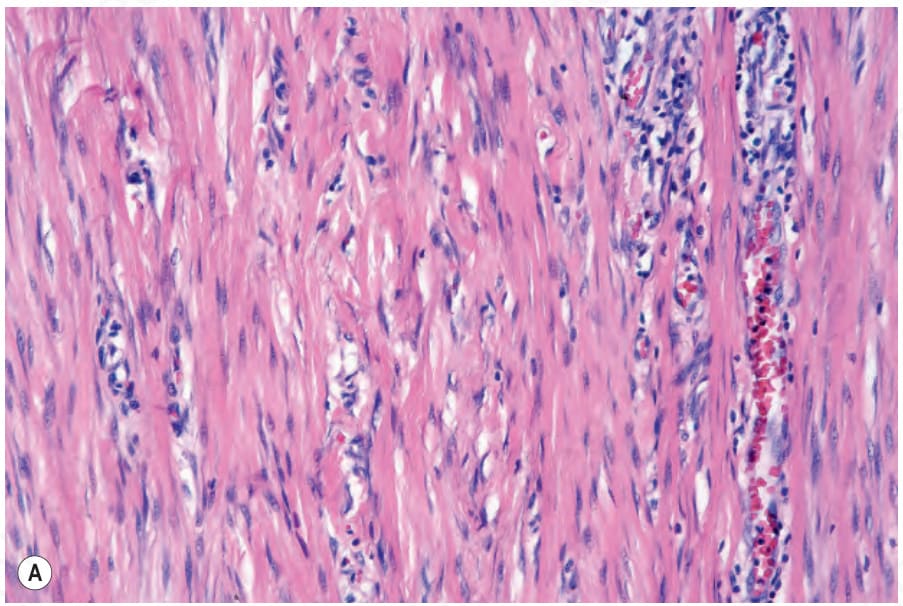
Fig. 26.107 Desmoplastic melanoma: (A) high-power view of tumor shown in Figure 26.106; (B) immunohistochemistry for S100 protein highlights the considerable tumor cell population.
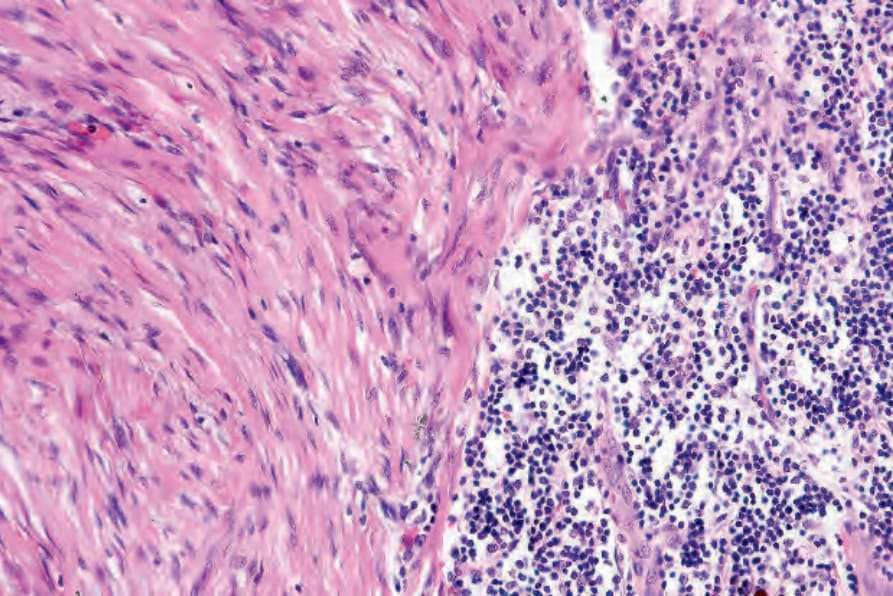
Fig. 26.108 Desmoplastic melanoma: nodular aggregates of lymphocytes are a useful diagnostic clue.
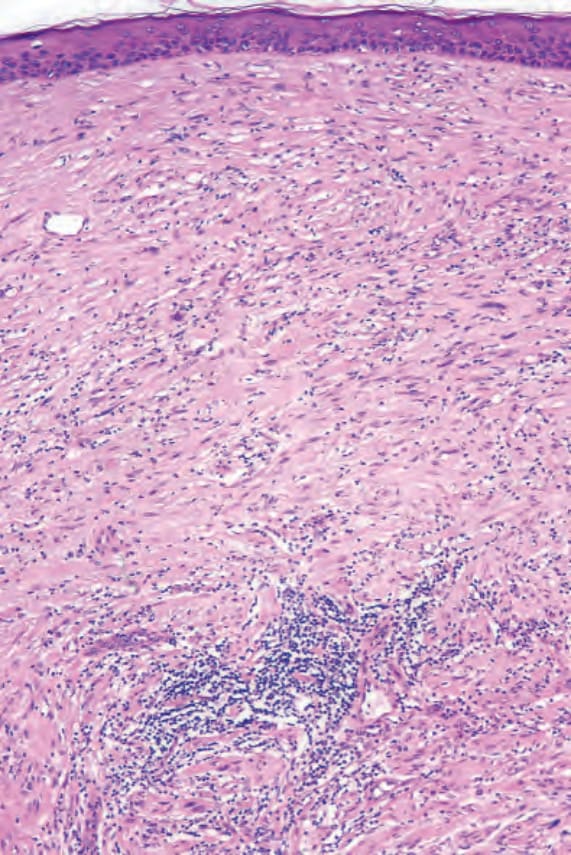
Fig. 26.109 Desmoplastic melanoma: in this example, the overlying epidermis shows no evidence of a pre-existent atypical melanocytic proliferative lesion (the so-called de novo variant).
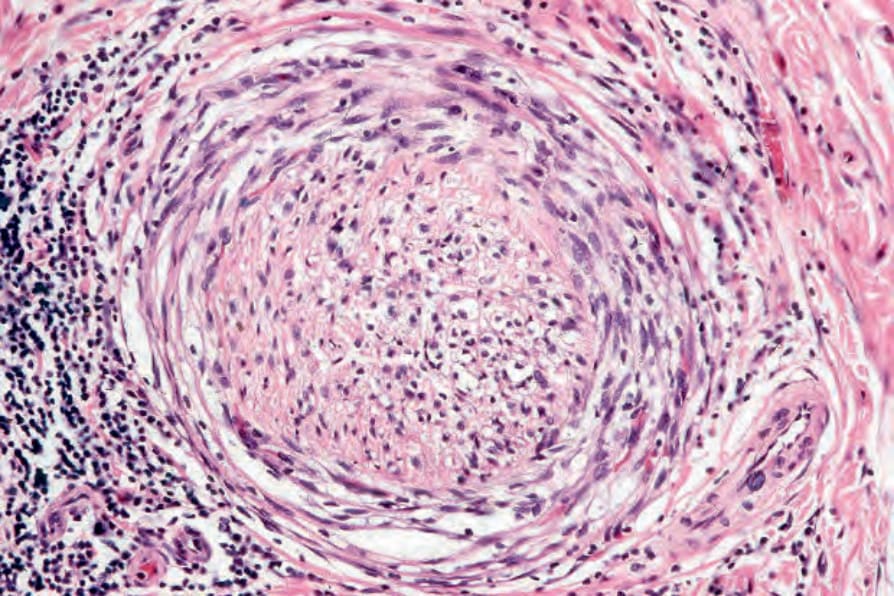
Fig. 26.110 Desmoplastic melanoma: perineural infiltration is very commonly present, accounting in part for the high recurrence rate of this tumor.
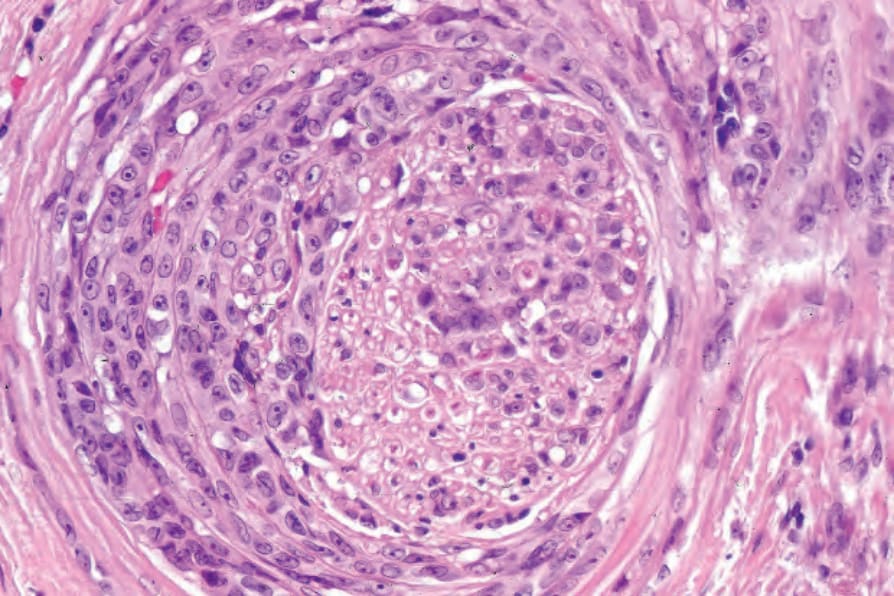
Fig. 26.111 Desmoplastic melanoma: epithelioid cells are sometimes encountered within the tumor. This example shows extensive peri- and intraneural spread.
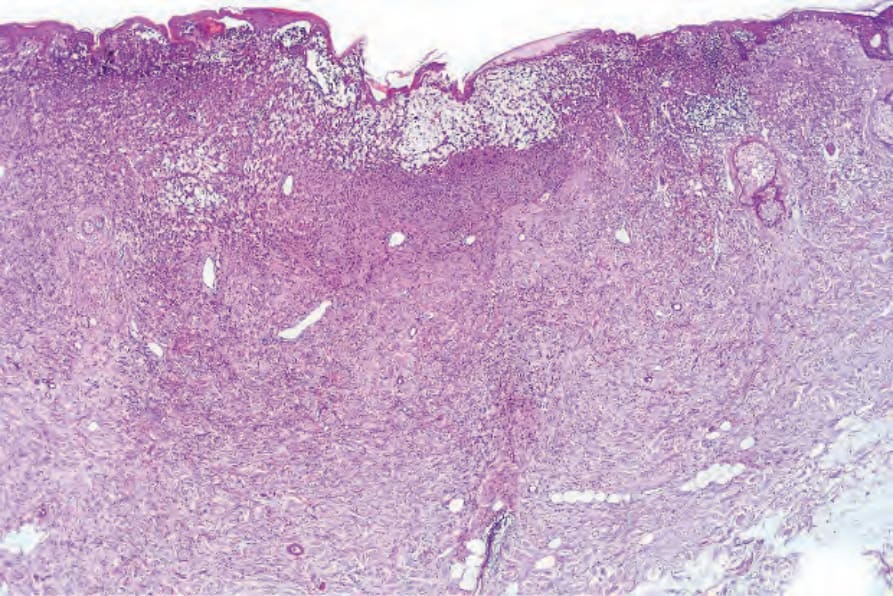
Fig. 26.112 Desmoplastic melanoma (neural transformation): low-power view of a tumor which has infiltrated through the full thickness of the dermis.
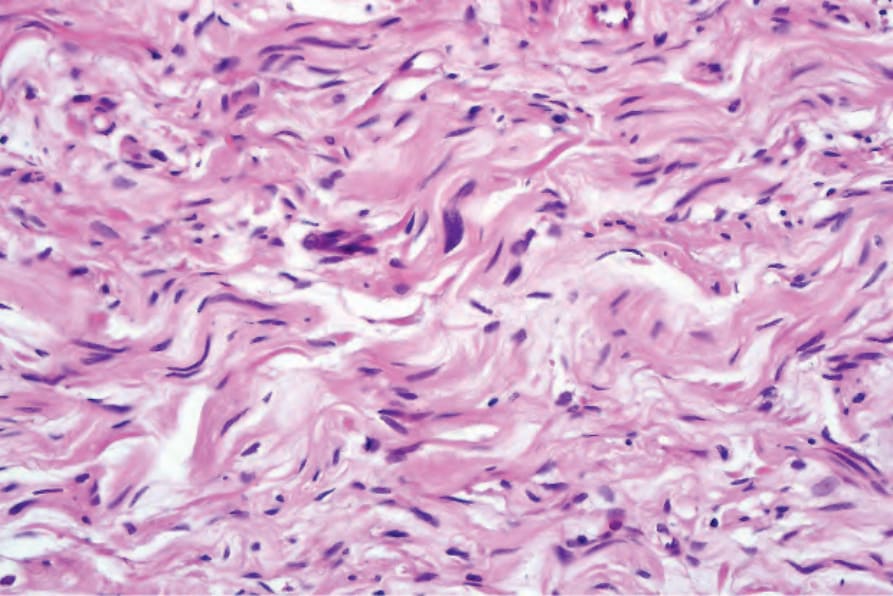
Fig. 26.113 Desmoplastic melanoma (neural transformation): the tumor cells have small, twisted, and comma-shaped nuclei with ill-defined eosinophilic cytoplasm reminiscent of peripheral nerve sheath tumor. Note the nuclear hyperchromatism.
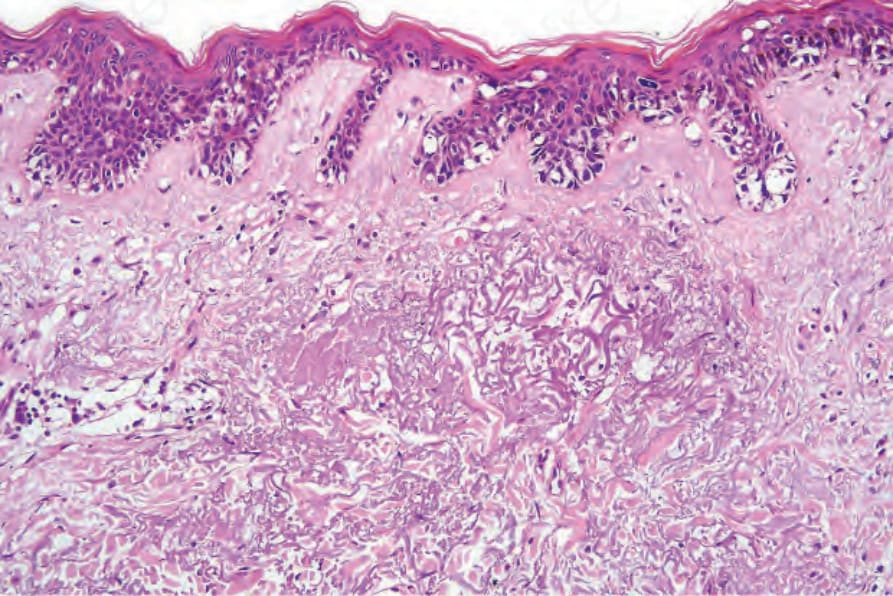
Fig. 26.114 Desmoplastic melanoma: the adjacent epidermis shows atypical melanocytic lentiginous hyperplasia.
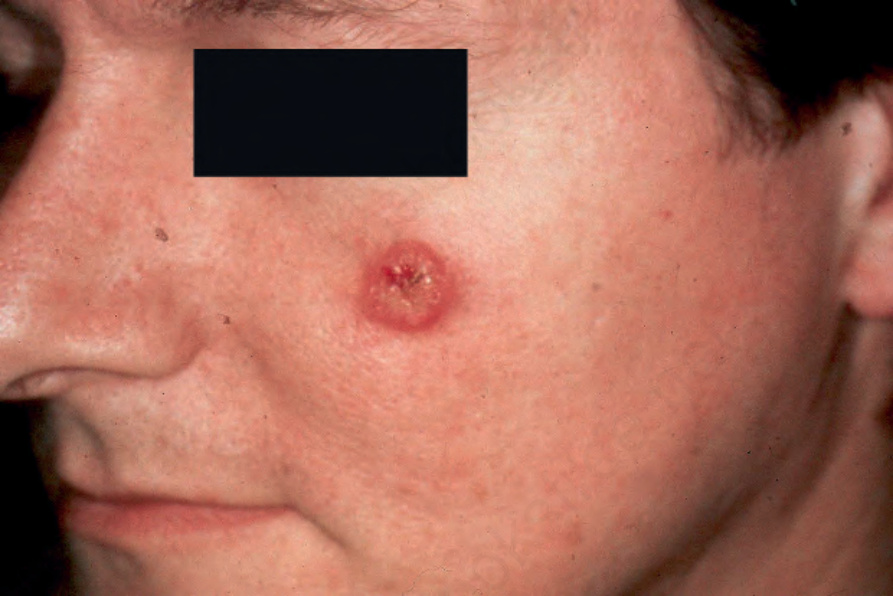
Fig. 26.98 Desmoplastic melanoma: these tumors are frequently amelanotic, as seen in this patient. By courtesy E. Wilson Jones, MD, Institute of Dermatology, London, UK.

Fig. 26.99 Desmoplastic melanoma: this tumor was initially thought to represent a cyst. By courtesy of E. Wilson Jones, MD, Institute of Dermatology, London, UK.