疾病定義與分類
- 藍痣樣黑色素瘤 (blue nevus-like melanoma)(惡性藍痣,malignant blue nevus)此名詞涵蓋多種病灶,包括在 cellular blue nevus 背景上發生的黑色素瘤,以及程度較低者在 common blue nevus 背景上發生、或在形態上與 blue nevus 有重疊的黑色素瘤。其變異型亦曾被記載併發於 nevi of Ito 與 nevi of Ota 以及 pilar neurocristic hamartoma。
- 此名詞也包括與 cellular blue nevi 在組織學上有重疊、但缺乏前驅病灶 (precursor lesion) 的黑色素瘤病例(de novo 變異型)。
- Pigmented epithelioid melanocytoma(先前稱為 animal-type 或 pigment-synthesizing melanoma;見下文)可具有高度相似的形態學光譜,但在基因體層面 (genomic level) 上與 blue nevus-like melanoma 有所區別。
臨床特徵 (Clinical Features)
- Malignant blue nevi 常為生長極為緩慢的病灶,臨床上常因突然出現的生長 (sudden onset of growth) 而被注意,且好發於頭皮 (scalp)(Fig. 26.80)。
- 男性受影響較女性為多。任何年齡層皆無豁免,極少數情況下兒童亦會受影響。
- 此為高惡性度 (high-grade) 病灶,其預後與分期相符 (stage-matched) 的傳統黑色素瘤病例相似。轉移性疾病最常侵犯肺、肝與淋巴結。
組織病理特徵 (Histopathology)
- 在既存 blue nevus 背景上發生的腫瘤,典型表現為從良性前驅病灶突然轉變 (abrupt transition) 為明顯的黑色素瘤(Figs 26.81 與 26.82)。後者表現為一個或多個由 epithelioid 或 spindled melanocytes 組成的結節,呈瀰漫性生長型態,並具有明顯的惡性細胞學特徵(Figs 26.83 與 26.84)。
- 模擬 cellular blue nevus、但無法辨識出前驅病灶的腫瘤,常呈現膨脹性生長型態 (expansile growth pattern),邊界通常為推擠性 (pushing borders),並向下延伸進入皮下脂肪 (subcutaneous fat)(Fig. 26.85)。偶爾可見啞鈴狀 (dumbbell) 的掃描下形態,罕見情況下可見肺泡狀生長型態 (alveolar growth pattern)。
- 典型上,在低倍鏡 (low-power magnification) 下會預期是良性 cellular nevus 的診斷。腫瘤細胞最常為 spindled cell 形態,但有時亦會遇到 epithelioid 與混合型變異。
- 然而高倍鏡 (high-power) 細節顯示核質比 (nuclear-to-cytoplasmic ratio) 增加、輕至中度核多形性 (nuclear pleomorphism)、深染 (hyperchromatism)、核仁顯著 (nucleolar prominence) 以及有絲分裂活性增加(Figs 26.86 與 26.87)。亦可能出現壞死 (necrosis),有時呈地圖樣型態 (geographic pattern),而神經周圍浸潤 (perineural infiltration) 為偶見的特徵。
- 在此第二種變異型中常見散在的樹突狀細胞 (dendritic cells)。這究竟代表殘餘的良性前驅病灶、或是顯示惡性樹突狀細胞,仍有疑義。支持後者可能性的依據為轉移灶中亦出現樹突狀細胞 (Fig. 26.88)。
- 一部分黑色素細胞增生病灶難以明確分類為良性或惡性。這些被稱為 atypical cellular blue nevi 或 cellular blue melanocytic proliferation of uncertain malignant potential。對於整個 blue nevus 光譜的惡性診斷標準,似乎缺乏共識。
致病機轉/分子 (Pathogenesis / Molecular)
- Blue nevus 與 blue nevus-like melanoma 皆與 GNAQ、或較少見的 GNA11 之突變有關,此二者編碼一種異三聚體 G 蛋白 (heterotrimeric G-protein) 的 alpha 次單元。
- 與眼部黑色素瘤 (ocular melanoma) 相似,BAP1、SF3B1 與 EIF1AX 之突變在 blue nevus-like melanoma 中常被遇到,其存在或有助於確立惡性診斷。
- 標準的多探針 FISH assay (multi-probe FISH assay) 有助於區分 blue nevus-like melanoma 與非典型的 cellular blue nevus,但目前可用的資料有限。

圖 26-80:Malignant blue nevus:注意此年長病人前額上,色素濃重的原發腫瘤併隨多發衛星病灶 (satellite lesions)。由 Institute of Dermatology, London, UK 提供。
Fig. 26.80 Malignant blue nevus: note the heavily pigmented primary tumor associated with multiple satellite lesions on this elderly patient’s forehead. By courtesy of the Institute of Dermatology, London, UK.
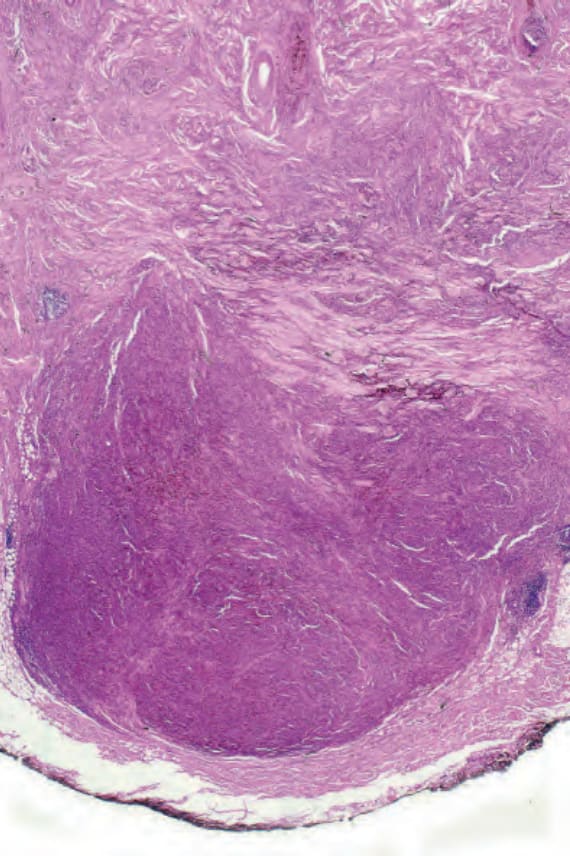
圖 26-81:Malignant blue nevus:此腫瘤發生於頭皮。有一緻密的膨脹性腫瘤結節 (expansile tumor nodule),已延伸進入皮下脂肪。
Fig. 26.81 Malignant blue nevus: this tumor arose on the scalp. There is a dense expansile tumor nodule which has extended into the subcutaneous fat.
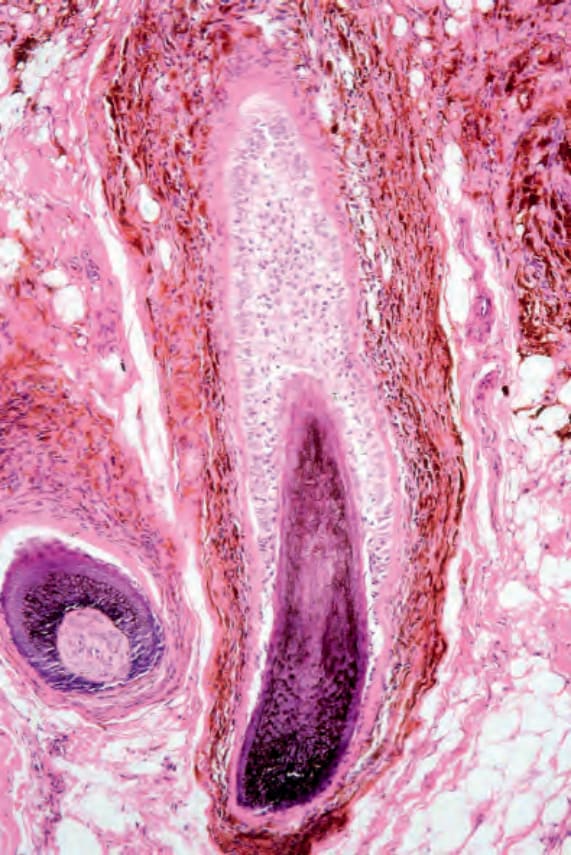
圖 26-82:Malignant blue nevus:鄰近皮膚中可見明顯的 pilar blue nevus。
Fig. 26.82 Malignant blue nevus: a pilar blue nevus was evident in the adjacent skin.
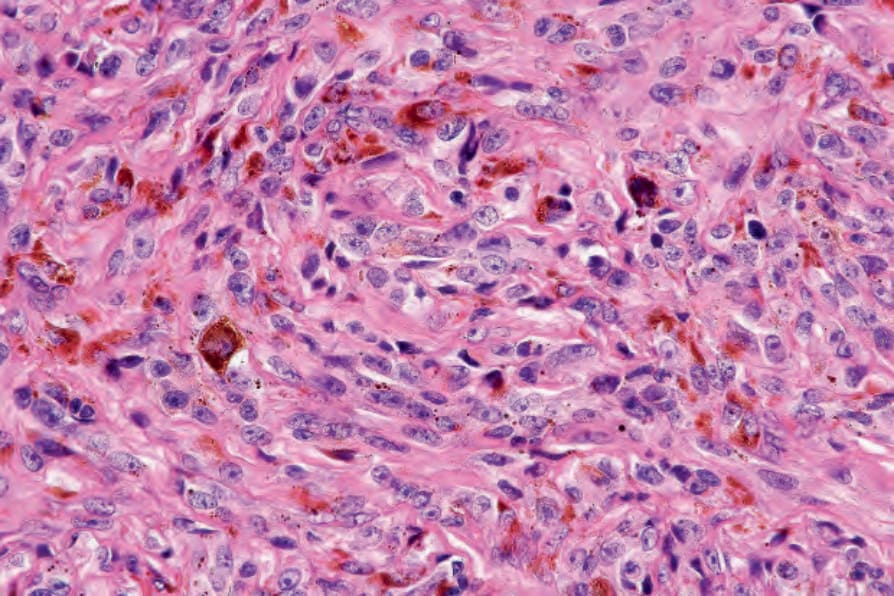
圖 26-83:Malignant blue nevus:腫瘤細胞具有泡狀核 (vesicular nuclei) 及顯著核仁 (prominent nucleoli)。
Fig. 26.83 Malignant blue nevus: the tumor cells have vesicular nuclei with prominent nucleoli.
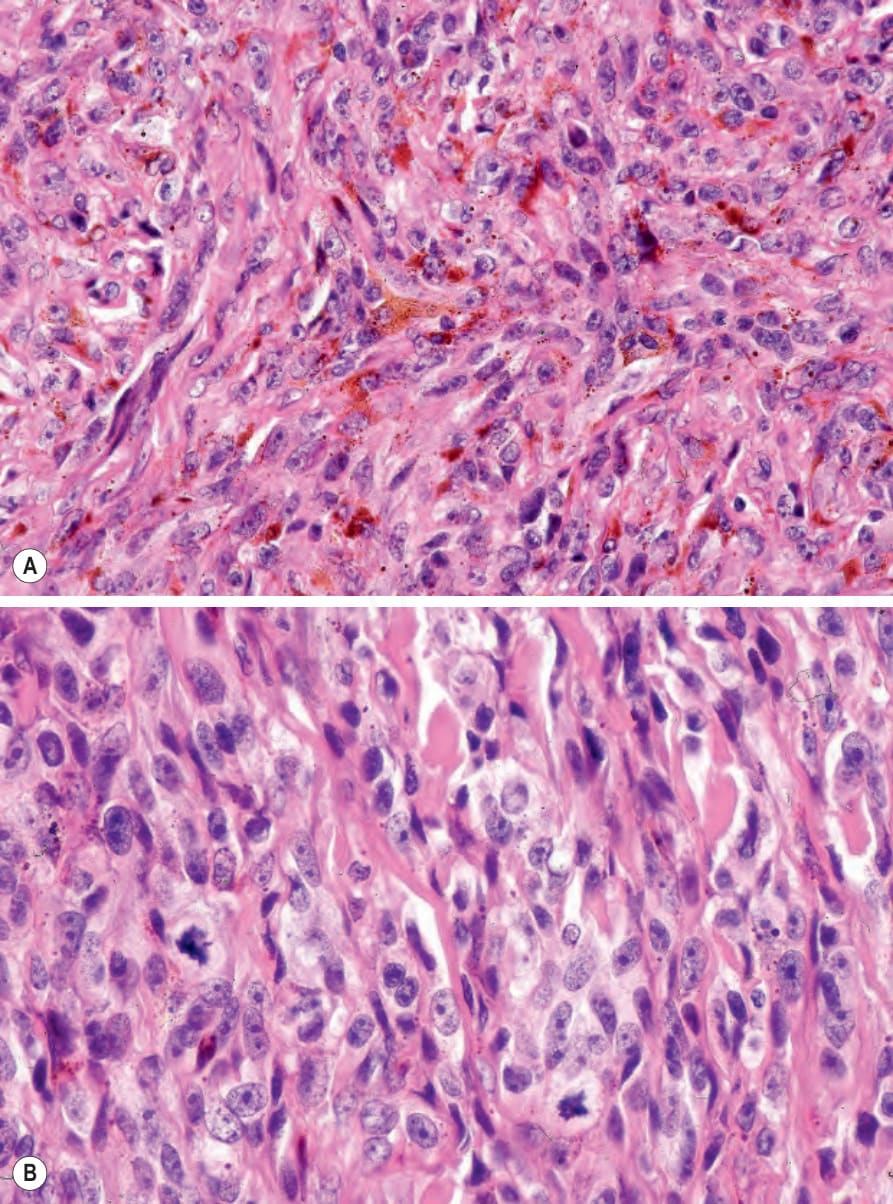
圖 26-84:Malignant blue nevus:(A) 有多個樹突狀細胞 (dendritic cells);(B) 注意兩個有絲分裂相 (mitoses)。
Fig. 26.84 Malignant blue nevus: (A) there are multiple dendritic cells; (B) note the two mitoses.
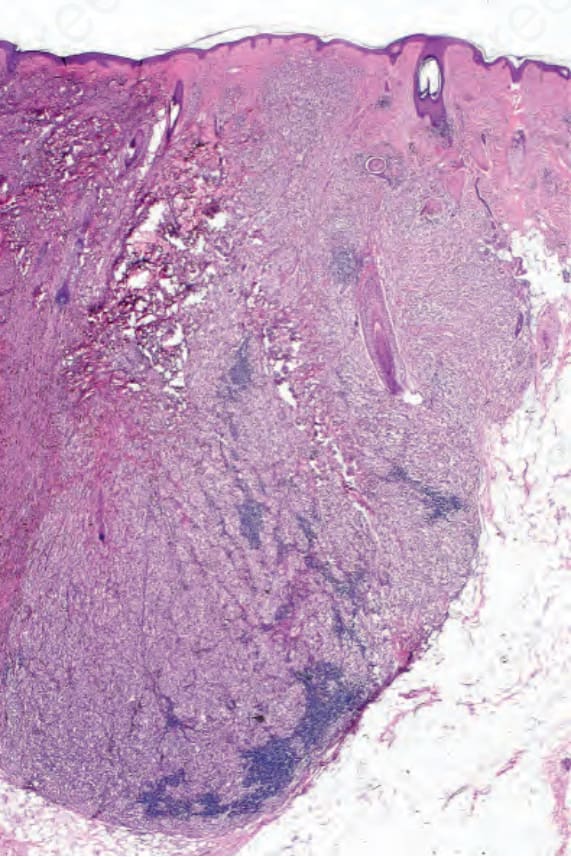
圖 26-85:Malignant blue nevus:此病例中未辨識出前驅病灶 (precursor lesion)。
Fig. 26.85 Malignant blue nevus: a precursor lesion was not identified in this case.
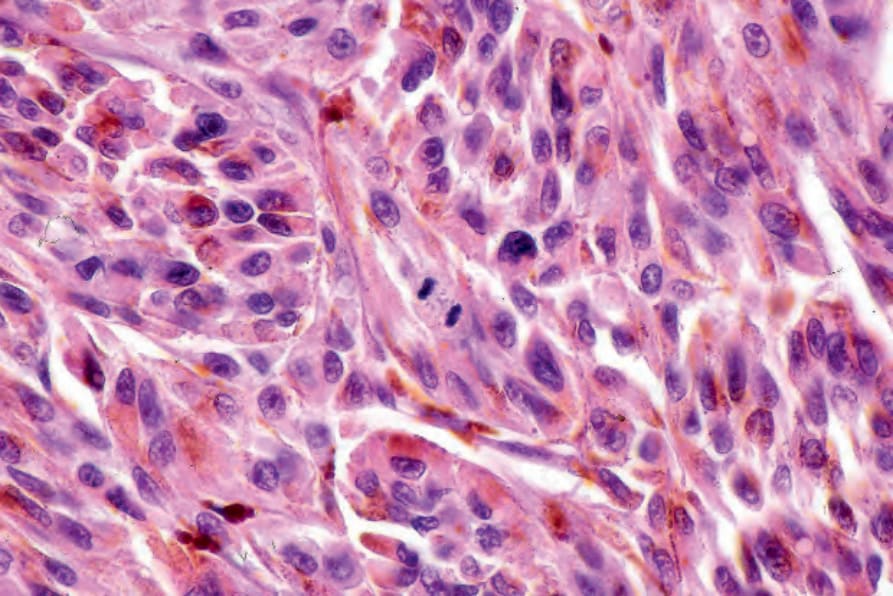
圖 26-86:Malignant blue nevus:注意中央的有絲分裂相 (mitotic figure)。
Fig. 26.86 Malignant blue nevus: note the central mitotic figure.
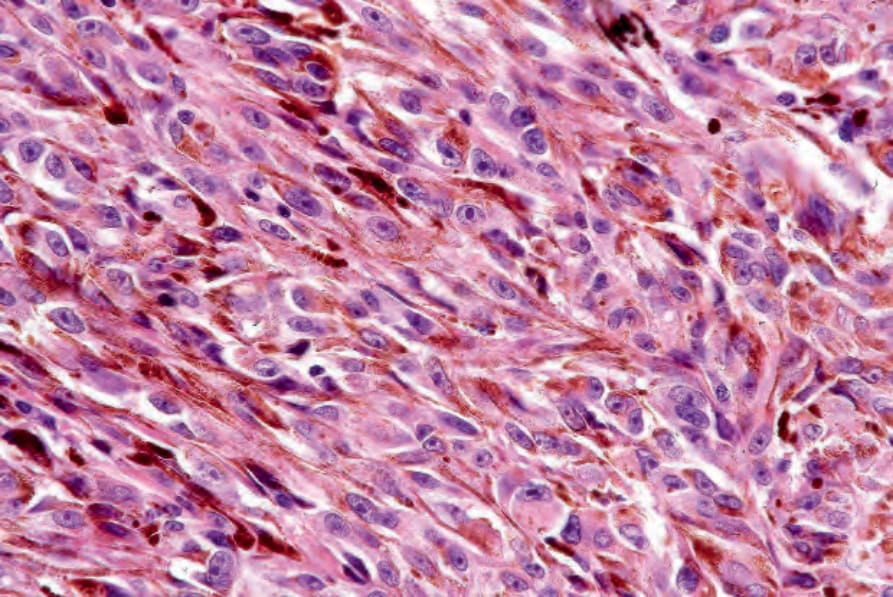
圖 26-87:Malignant blue nevus:此視野中樹突狀細胞 (dendritic cells) 明顯可見。
Fig. 26.87 Malignant blue nevus: dendritic cells are conspicuous in this field.
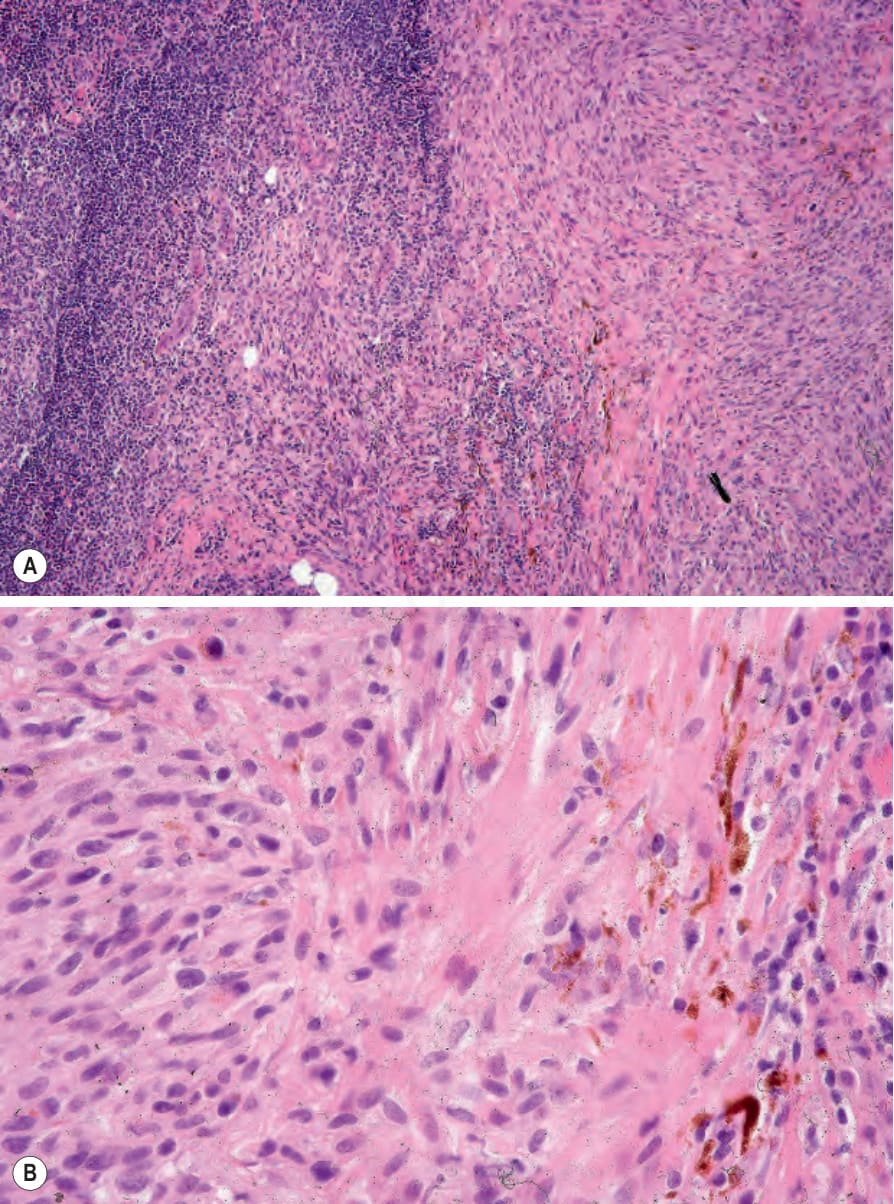
圖 26-88:(A, B) Malignant blue nevus:前哨淋巴結 (sentinel node) 含有轉移性黑色素瘤。可見少數樹突狀細胞 (dendritic cells)。此為與 Figures 26.81–26.84 所示相同之病例。
Fig. 26.88 (A, B) Malignant blue nevus: the sentinel node contained metastatic melanoma. A small number of dendritic cells are present. This is the same case as illustrated in Figures 26.81–26.84.