黏液樣黑色素瘤 (Myxoid Melanoma)
疾病定義與分類
- 黑色素瘤中的黏液樣間質變化 (myxoid stromal change) 非常罕見,可見於原發 (primary)、復發 (recurrent) 與轉移 (metastatic) 病灶。此變化不具預後意義 (of no prognostic significance)。
組織病理特徵 (Histopathology)
- 黏液樣變化 (myxoid change) 是垂直生長期 (vertical growth phase) 黑色素瘤的特徵。它可能僅以腫瘤的次要成分呈現,也可能瀰漫存在於整個腫瘤。後者(瀰漫型)可造成相當大的診斷困難:上皮樣 (epithelioid) 病例會讓人聯想到癌 (carcinoma),而梭形細胞 (spindle cell) 病例則模仿肉瘤 (sarcoma)。它也曾被描述為光療 (phototherapy) 後的反應性變化 (reactive change)。
- 典型上,腫瘤細胞比非黏液樣區域內的細胞為小,外觀上可呈上皮樣 (epithelioid)、梭形 (spindled) 或星狀 (stellate)(Fig. 26.77)。黑色素沉積 (melanin pigmentation) 程度不一。
- 黏液 (mucin) 表現為嗜鹼性 (basophilic) 的「絲狀 (stringy)」物質,通常 PAS 陰性 (PAS negative)、colloidal iron 與 Alcian blue 陽性,且對 hyaluronidase 敏感(與間質性黏液 stromal mucin 一致)。
- 黑色素瘤細胞常以失黏附 (discohesive) 的團塊 (clumps)、條索 (cords) 與細股 (strands) 形式存在,以致有時可形成假腺樣 (pseudoglandular) 或「假棘層鬆解樣 (acantholytic)」外觀(Figs 26.78 與 26.79)。偶爾可見假腺泡分化 (pseudoacinar differentiation) 與細胞間鑲嵌 (intercellular molding),令人聯想到腺癌 (adenocarcinoma)。
免疫組化與特殊染色 (Immunohistochemistry & Special Stains)
- 免疫組化表現為黑色素瘤的典型表現,腫瘤細胞對 S100 protein 恆為陽性 (invariably positive),且通常對 HMB-45 陽性。不過,亦曾記錄到 HMB-45 陰性的情形。
鑑別診斷 (Differential Diagnosis)
- 黏液樣變化有時可見於促結締組織增生性黑色素瘤 (desmoplastic melanoma) 的間質中,但通常仍會出現其他較典型的傳統 desmoplastic melanoma 區域。
- Myxoid melanoma 可能與分泌黏液的腺癌 (mucus-secreting adenocarcinoma)、黏液樣惡性周邊神經鞘瘤 (myxoid malignant peripheral nerve sheath tumor, MPNST) 或其他肉瘤 (sarcomas) 混淆。
- 前者(adenocarcinoma)可依 keratin 免疫細胞化學陰性 (negative keratin immunocytochemistry) 及缺乏 PAS 陽性黏液 (absence of PAS-positive mucin) 加以排除。
- Myxoid malignant peripheral nerve sheath tumor 通常顯示弱很多且僅局部的 S100 protein 表現,且 HMB-45 為陰性。此外,僅侷限於真皮 (dermis) 的 MPNST 極為罕見。
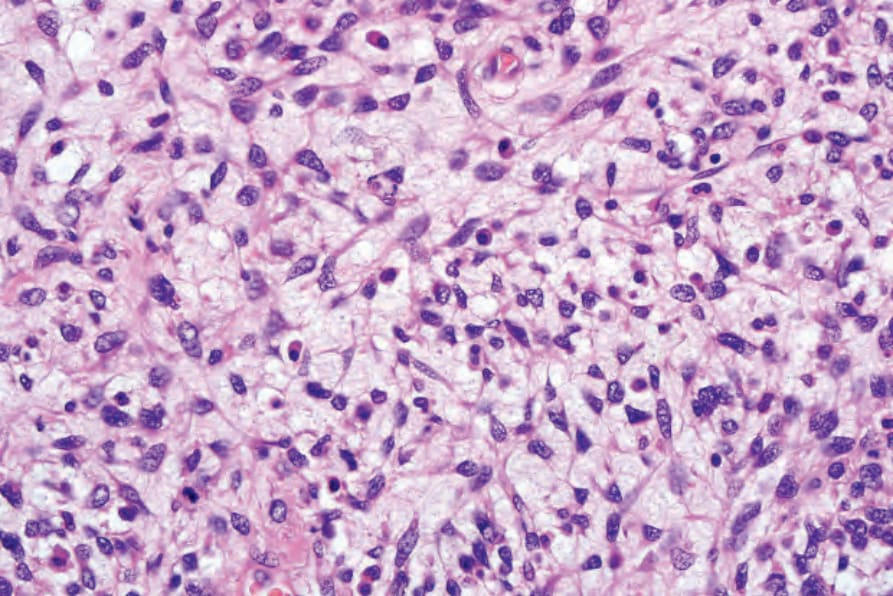
圖 26.77:黏液樣黑色素瘤 (myxoid melanoma):此罕見變異型可造成相當大的診斷困難。注意與豐富黏液樣間質 (myxoid stroma) 相關的「未分化 (undifferentiated)」不規則細胞。
Fig. 26.77 Myxoid melanoma: this rare variant can be a source of considerable diagnostic difficulty. Note the ‘undifferentiated’ irregular cells associated with an abundant myxoid stroma.
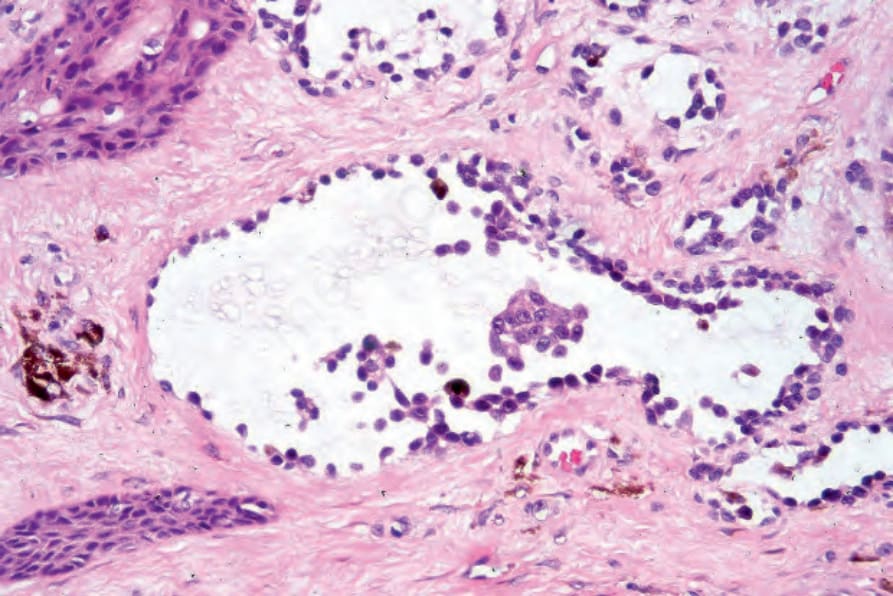
圖 26.78:腺樣(假腺樣)黑色素瘤 (adenoid (pseudoglandular) melanoma):此變異型亦伴隨過量黏液沉積 (excess mucin deposition),若缺乏交界成分 (junctional component) 或色素 (pigment),可能輕易被誤診為棘層鬆解性鱗狀細胞癌 (acantholytic squamous carcinoma) 或腺癌 (adenocarcinoma)。診斷常仰賴免疫組化 (immunohistochemistry)。By courtesy of R. Margolis, MD, St Elizabeth’s Medical Center, Boston, USA.
Fig. 26.78 Adenoid (pseudoglandular) melanoma: this variant also associated with excess mucin deposition may easily be misdiagnosed as an acantholytic squamous carcinoma or adenocarcinoma if a junctional component or pigment is absent. Diagnosis often depends upon immunohistochemistry. By courtesy of R. Margolis, MD, St Elizabeth’s Medical Center, Boston, USA.