引言
雖然絕大多數薄型黑色素瘤 (thin melanomas) 不會轉移,但已知有百分之一至百分之二會發生轉移。反之,偶有厚型黑色素瘤 (thick melanomas) 並未發生擴散。有鑑於此,學界投入大量研究,努力界定哪些腫瘤具有擴散並導致死亡的能力,期望輔助性化療 (adjuvant chemotherapy)、免疫療法 (immunotherapy) 或其他治療形式最終能造福相當數量的病人。預後指標包括臨床參數、形態學觀察與測量,此外尚有細胞增殖、細胞調控等的免疫組化標記。許多形態學觀察已歷經反覆驗證,但對於難以捉摸的轉移潛能免疫組化標記之尋找,迄今尚未有豐碩成果。基因體生物標記 (genomic biomarkers) 亦正被探討中,特別是有限的基因表現面板 (limited gene expression panels)。171–173
臨床預後指標包括年齡、性別與原發腫瘤的部位。174–180 年長病人預後較年輕者差,男性的展望較女性差。7,176,177,181–184 後者與腫瘤厚度及部位無關。176 特別高風險的部位包括背部、上臂、頸部與頭皮 (back, upper arm, neck, and scalp; BANS)。185 肢端部位 (acral sites) 一般也被認為與較差的預後相關。186
報告黑色素瘤時,全球普遍認為記錄並評述下列變項是必要的:176,187–193
- 腫瘤厚度 (tumor thickness, Breslow method),
- 侵犯層級 (level of invasion, Clark method),
- 生長期 (growth phase,垂直或放射狀),
- 有絲分裂率 (mitotic rate),
- 潰瘍 (ulceration),
- 淋巴血管侵犯 (lymphovascular invasion),
- 神經周圍浸潤 (perineural infiltration),
- 退行 (regression),
- 微衛星病灶 (microsatellitosis),
- 腫瘤浸潤淋巴球 (tumor infiltrating lymphocytes)。生長期亦會被註記,惟須強調,在將一個黑色素瘤歸入微侵襲性 (microinvasive) 之放射狀 (水平) 生長期類別之前,必須極為審慎。真皮內有絲分裂 (dermal mitoses) 會自動將腫瘤歸入垂直生長期 (vertical growth phase)(見 Fig. 26.14)。這些要素已成為病人正確分期與預後判定的關鍵,但遺憾的是,即便在皮膚黑色素瘤發生率高且警覺性敏銳的國家,上述許多要素仍常缺漏於例行報告中。194
Breslow 腫瘤厚度是原發性皮膚黑色素瘤單一最重要的預後指標。195,196 它是從顆粒細胞層 (granular cell layer) 最表淺處量至腫瘤侵犯最深點。在潰瘍性腫瘤中,應從潰瘍基底開始測量。附屬器周圍 (periadnexal) 擴展的意義較不明確。若後者大於傳統的 Breslow 厚度,除了傳統的 Breslow 測量值外,亦應記錄此資訊(Fig. 26.43)。息肉狀腫瘤 (polypoid tumors) 不應有不同處理方式,應通過最厚的區域測量。197 因此,腫瘤體積 (tumor volume) 是影響垂直生長期黑色素瘤結局的最重要因素。仔細評估最大腫瘤厚度可提供極有用的預後指引。198–201 在美國癌症聯合委員會 (American Joint Committee on Cancer; AJCC) 分期系統的最新版 (第 8 版,2017 年發布、2018 年生效) 中,厚度閾值維持與第 7 版相同的 1.0、2.0 與 4.0 mm,惟 T1 組另以 0.8 mm 細分(Table 26.1)。196,202–206 第 7 版分期仍在此提供以供比較(Table 26.2)。新分期系統的一個令人欣喜的特點是,Breslow 厚度現在僅報告至小數點後一位有效數字,簡化了以測微計 (micrometer) 進行的測量。雖然當然並不完美,但黑色素瘤的臨床、尤其是顯微病理分期極為強大,並可作為其他癌症的範式。
依 Clark 層級分類的腫瘤侵犯層級如下:
- Level I:原位黑色素瘤 (in situ melanoma),
- Level II:單一細胞或小巢侵犯乳頭層真皮 (papillary dermis),
- Level III:侵襲性腫瘤通常呈擴張性結節 (expansile nodule) 緊貼網狀真皮 (reticular dermal) 界面,
- Level IV:侵犯網狀真皮 (reticular dermis),
- Level V:侵犯皮下脂肪 (subcutaneous fat)。真皮界面可藉表淺微血管叢 (superficial capillary plexus) 的位置來辨識。它也對應於水平走向的網狀真皮彈性纖維轉變為垂直排列之乳頭層真皮彈性纖維的轉換帶。Clark level II 與 III 之間,乃至於 III 與 IV 之間 (或許更甚) 的區分,在實務上頗難應用,且具觀察者依賴性 (observer dependent)。207 過去認為 Clark level 對薄型腫瘤 (厚度 1.0 mm 或以下) 可提供獨立的預後資訊,但對較厚的黑色素瘤則否。208,209 最新資料指出,若薄型黑色素瘤的有絲分裂率可評估,則 Clark level 不再提供額外的預後資訊。2017 年 (第 8 版) AJCC 分期系統不再建議使用 Clark level,即使對薄型黑色素瘤亦然,這與前一版不同。196,203,204,206 原發黑色素瘤的有絲分裂率與前哨淋巴結 (sentinel lymph node) 之轉移陽性相關。210
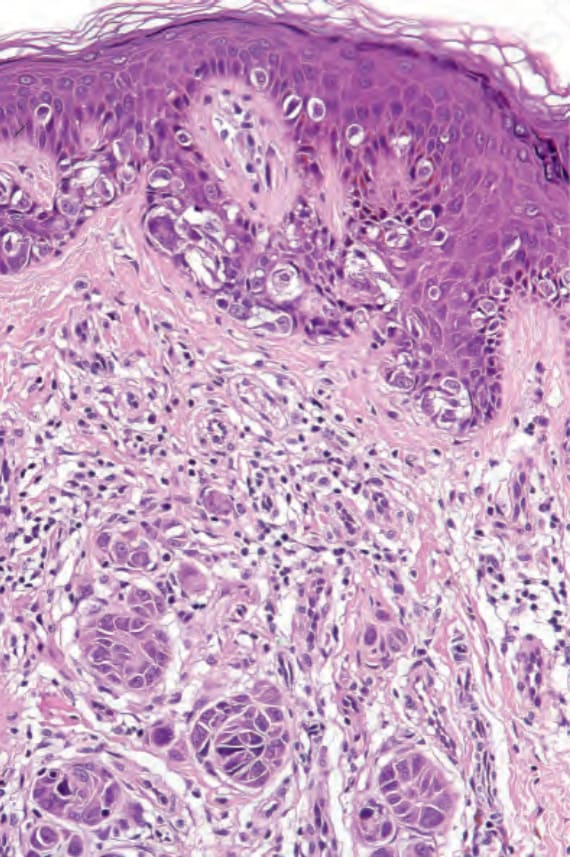
圖 26-14:黑色素瘤:垂直生長期。除了原位 (放射狀生長期) 腫瘤之外,真皮內有多個巢。這些巢大於表皮內的巢。 (Melanoma: vertical growth phase. In addition to in situ (radial growth phase) tumor, there are multiple nests in the dermis. These are larger than the epidermal ones.)
Fig. 26.14 Melanoma: vertical growth phase. In addition to in situ (radial growth phase) tumor, there are multiple nests in the dermis. These are larger than the epidermal ones.
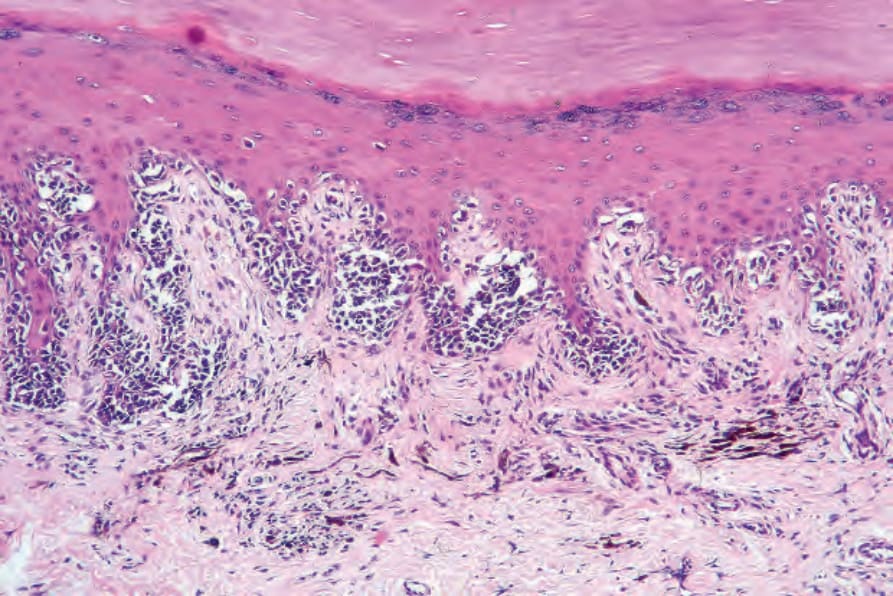
圖 26-33:肢端雀斑樣黑色素瘤 (acral lentiginous melanoma):在此原位病灶中,有不規則棘層肥厚 (irregular acanthosis)、顆粒層增厚 (hypergranulosis) 與角化過度 (hyperkeratosis)。腫瘤細胞深染 (hyperchromatic),呈雀斑樣 (lentiginous) 及巢狀分布。真皮有瘢痕化,並有明顯的噬黑色素細胞 (melanophages) 與慢性發炎細胞。 (Acral lentiginous melanoma: in this in situ lesion, there is irregular acanthosis, hypergranulosis, and hyperkeratosis. Tumor cells are hyperchromatic and distributed in a lentiginous and nested pattern. The dermis is scarred and there are conspicuous melanophages and chronic inflammatory cells.)
Fig. 26.33 Acral lentiginous melanoma: in this in situ lesion, there is irregular acanthosis, hypergranulosis, and hyperkeratosis. Tumor cells are hyperchromatic and distributed in a lentiginous and nested pattern. The dermis is scarred and there are conspicuous melanophages and chronic inflammatory cells.
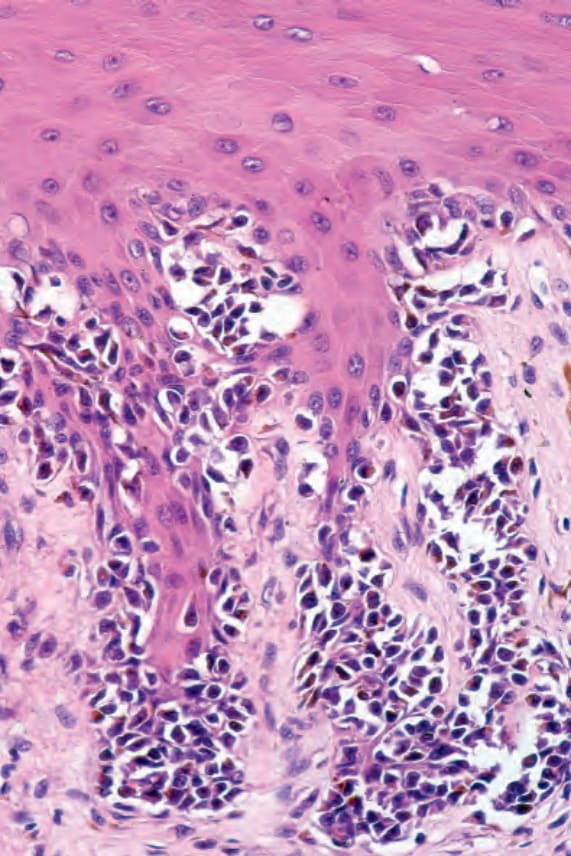
圖 26-34:肢端雀斑樣黑色素瘤 (acral lentiginous melanoma):有明顯的細胞質收縮 (cytoplasmic retraction)、深染與核異型 (nuclear atypia)。 (Acral lentiginous melanoma: there is conspicuous cytoplasmic retraction, hyperchromatism, and nuclear atypia.)
Fig. 26.34 Acral lentiginous melanoma: there is conspicuous cytoplasmic retraction, hyperchromatism, and nuclear atypia.
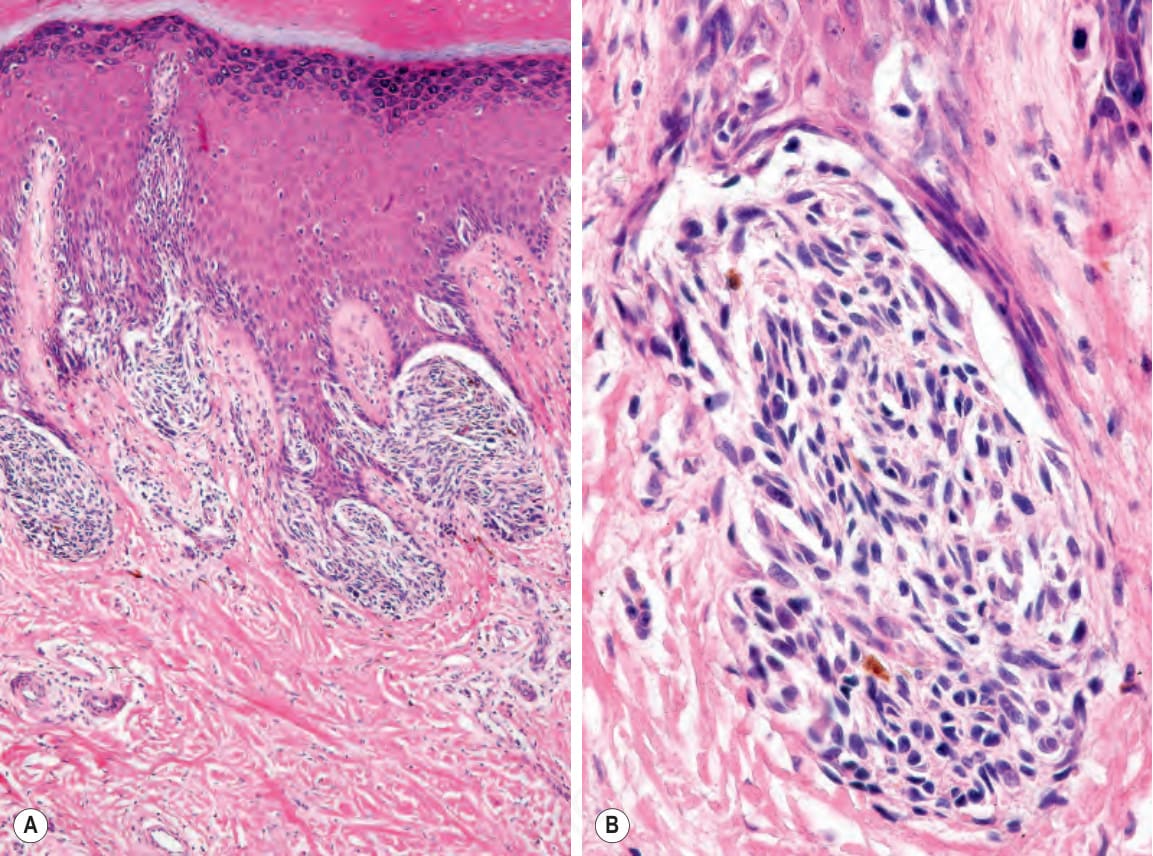
圖 26-35:(A, B) 肢端雀斑樣黑色素瘤 (acral lentiginous melanoma):表皮突 (rete) 頂端可見大型交界處巢 (junctional nests)。 (Acral lentiginous melanoma: large junctional nests are present at the tips of the rete.)
Fig. 26.35 (A, B) Acral lentiginous melanoma: large junctional nests are present at the tips of the rete.
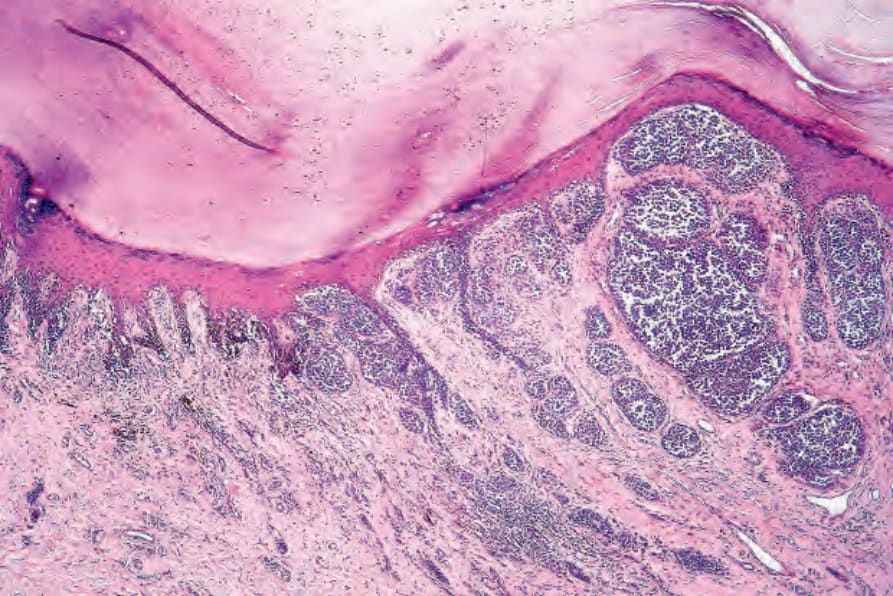
圖 26-36:肢端雀斑樣黑色素瘤 (acral lentiginous melanoma):在此例中,侵襲成分為上皮樣 (epithelioid)、梭形細胞 (spindled cell) 與促結締組織增生性 (desmoplastic) 混合型。 (Acral lentiginous melanoma: in this example, the invasive component is mixed epithelioid, spindled cell, and desmoplastic.)
Fig. 26.36 Acral lentiginous melanoma: in this example, the invasive component is mixed epithelioid, spindled cell, and desmoplastic.
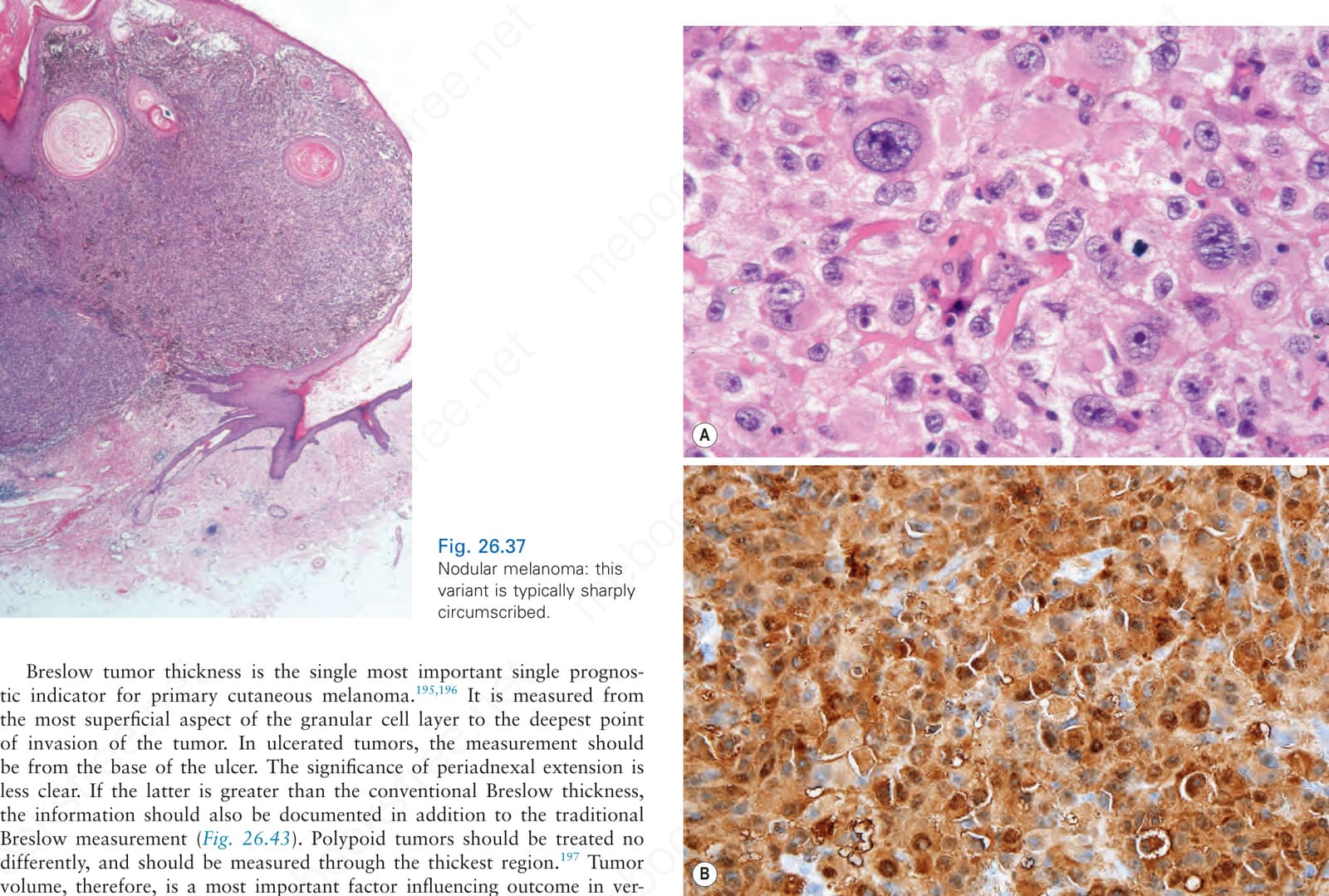
圖 26-37:結節型黑色素瘤 (nodular melanoma):此變異型通常界線清晰 (sharply circumscribed)。 (Nodular melanoma: this variant is typically sharply circumscribed.)
Fig. 26.37 Nodular melanoma: this variant is typically sharply circumscribed.
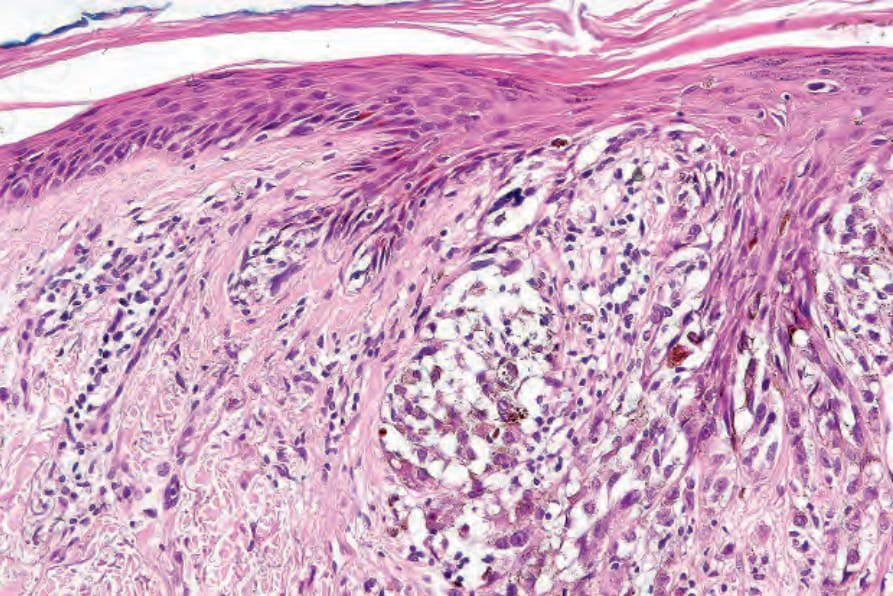
圖 26-38:結節型黑色素瘤 (nodular melanoma):依定義,相鄰表皮中無黑色素細胞增殖活性。 (Nodular melanoma: by definition, there is no melanocytic proliferative activity in the adjacent epidermis.)
Fig. 26.38 Nodular melanoma: by definition, there is no melanocytic proliferative activity in the adjacent epidermis.
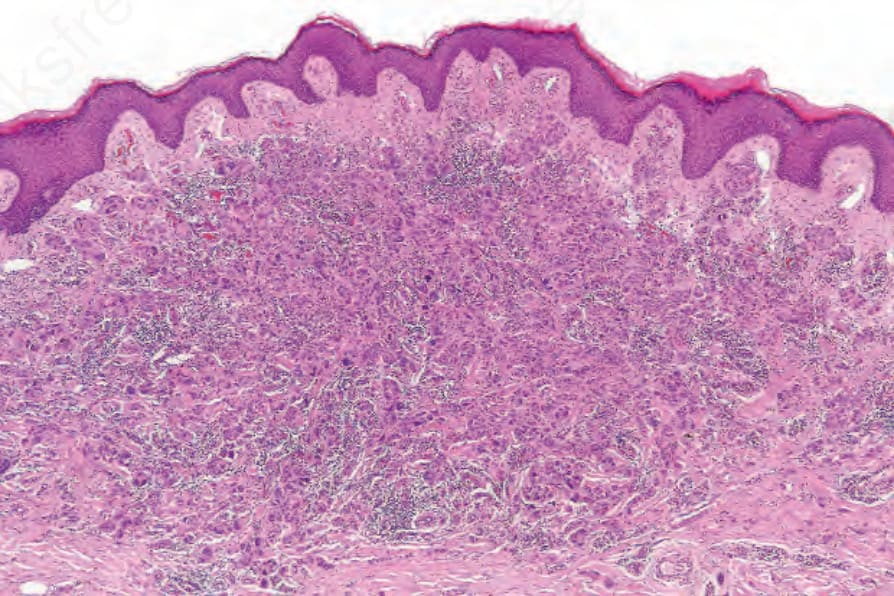
圖 26-40:巨細胞黑色素瘤 (giant cell melanoma):真皮內為一處轉移性黑色素瘤沉積。 (Giant cell melanoma: within the dermis is a deposit of metastatic melanoma.)
Fig. 26.40 Giant cell melanoma: within the dermis is a deposit of metastatic melanoma.
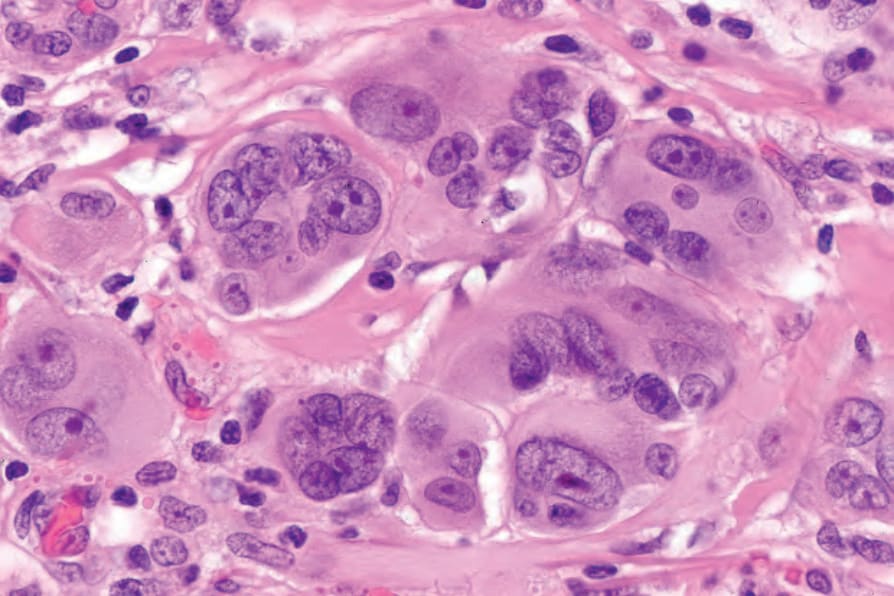
圖 26-41:巨細胞黑色素瘤 (giant cell melanoma):腫瘤細胞為多核且極具多形性 (pleomorphic),具有豐富的細胞質與大型囊泡狀核,核內含顯著的嗜伊紅核仁 (eosinophilic nucleoli)。 (Giant cell melanoma: the tumor cells are multinucleate and very pleomorphic with abundant cytoplasm and large vesicular nuclei containing prominent eosinophilic nucleoli.)
Fig. 26.41 Giant cell melanoma: the tumor cells are multinucleate and very pleomorphic with abundant cytoplasm and large vesicular nuclei containing prominent eosinophilic nucleoli.
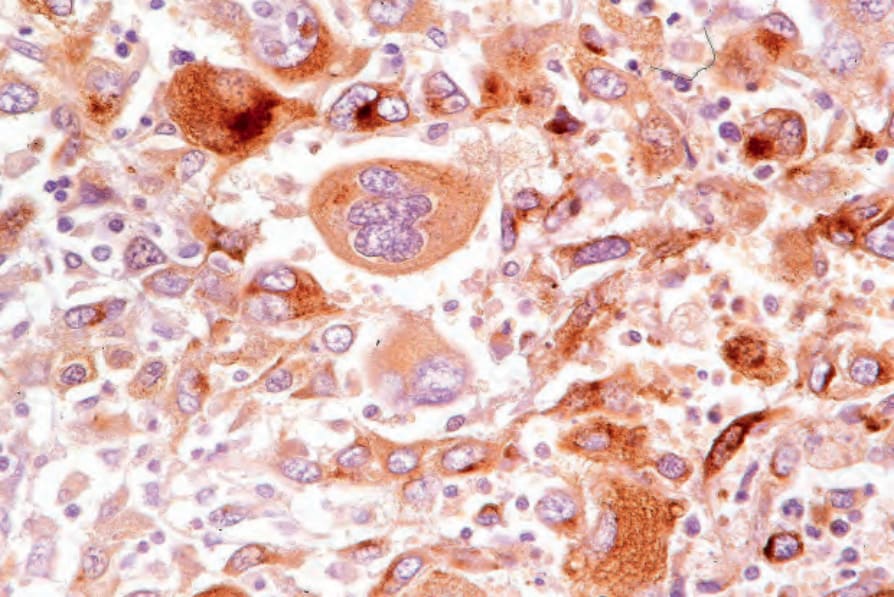
圖 26-42:巨細胞黑色素瘤 (giant cell melanoma):腫瘤細胞呈 HMB-45 陽性。此病人數年前曾切除一個黑色素瘤。 (Giant cell melanoma: the tumor cells are HMB-45 positive. The patient had a melanoma excised several years earlier.)
Fig. 26.42 Giant cell melanoma: the tumor cells are HMB-45 positive. The patient had a melanoma excised several years earlier.
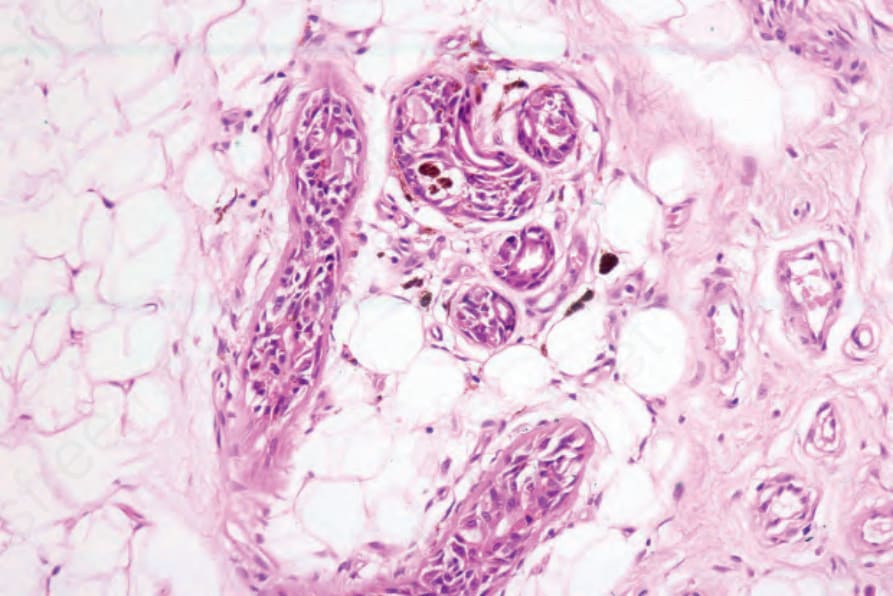
圖 26-43:黑色素瘤:附屬器周圍 (periadnexal) 擴展之生物學意義不明確,惟它是切除不全腫瘤復發的潛在來源。在此例中,外分泌汗腺 (eccrine sweat glands) 有深部侵犯。 (Melanoma: periadnexal extension is of uncertain biological significance except that it is a potential source for recurrence of inadequately excised tumors. In this example, there is deep involvement of the eccrine sweat glands.)
Fig. 26.43 Melanoma: periadnexal extension is of uncertain biological significance except that it is a potential source for recurrence of inadequately excised tumors. In this example, there is deep involvement of the eccrine sweat glands.
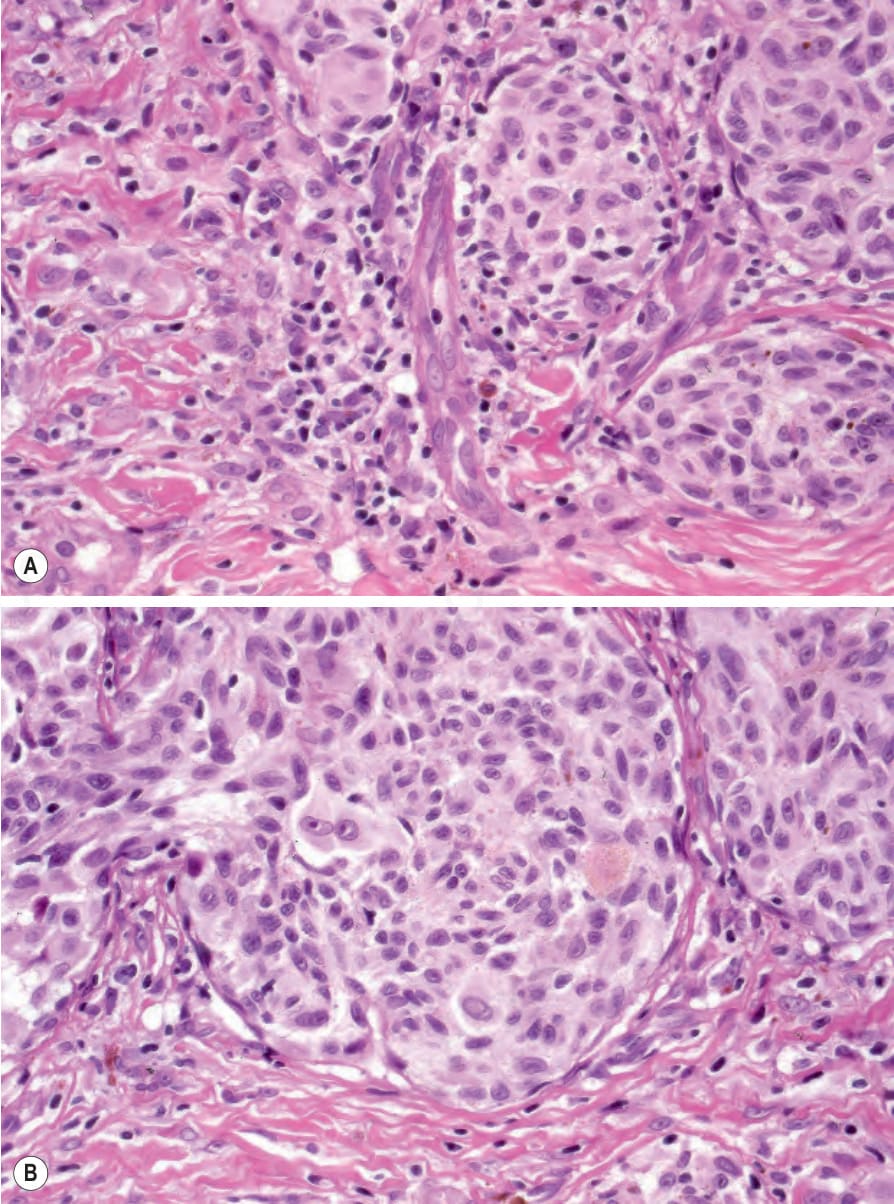
圖 26-45:(A, B) 黑色素瘤:腫瘤浸潤淋巴球 (tumor infiltrating lymphocytes)。Category B – Nonbrisk:淋巴球僅浸潤腫瘤的一部分。 (Melanoma: tumor infiltrating lymphocytes. Category B – Nonbrisk: the lymphocytes infiltrate only part of the tumor.)
Fig. 26.45 (A, B) Melanoma: tumor infiltrating lymphocytes. Category B – Nonbrisk: the lymphocytes infiltrate only part of the tumor.
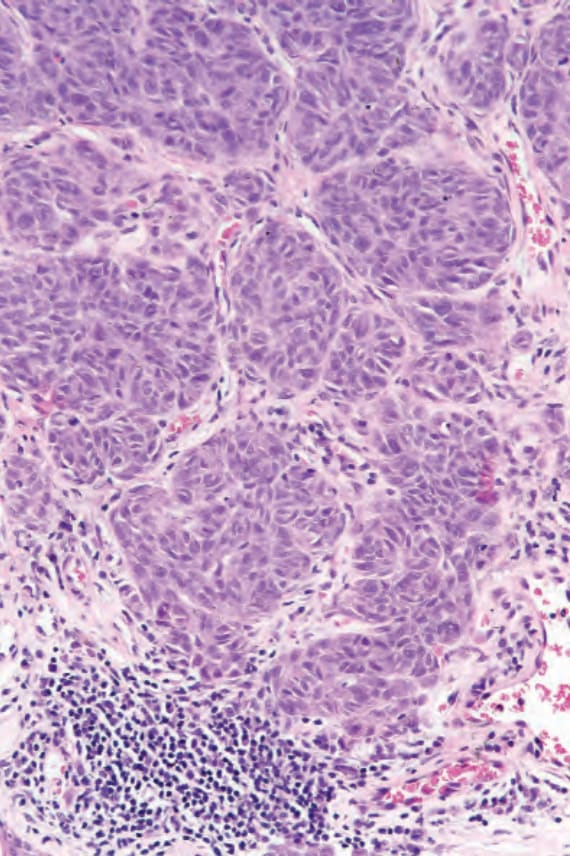
圖 26-46:黑色素瘤:腫瘤浸潤淋巴球 (tumor infiltrating lymphocytes)。Category C – Absent:淋巴球存在但不侵入腫瘤。此類別亦包括完全沒有淋巴球的情形。 (Melanoma: tumor infiltrating lymphocytes. Category C – Absent: lymphocytes are present but they do not invade the tumor. The category also includes complete absence of lymphocytes.)
Fig. 26.46 Melanoma: tumor infiltrating lymphocytes. Category C – Absent: lymphocytes are present but they do not invade the tumor. The category also includes complete absence of lymphocytes.
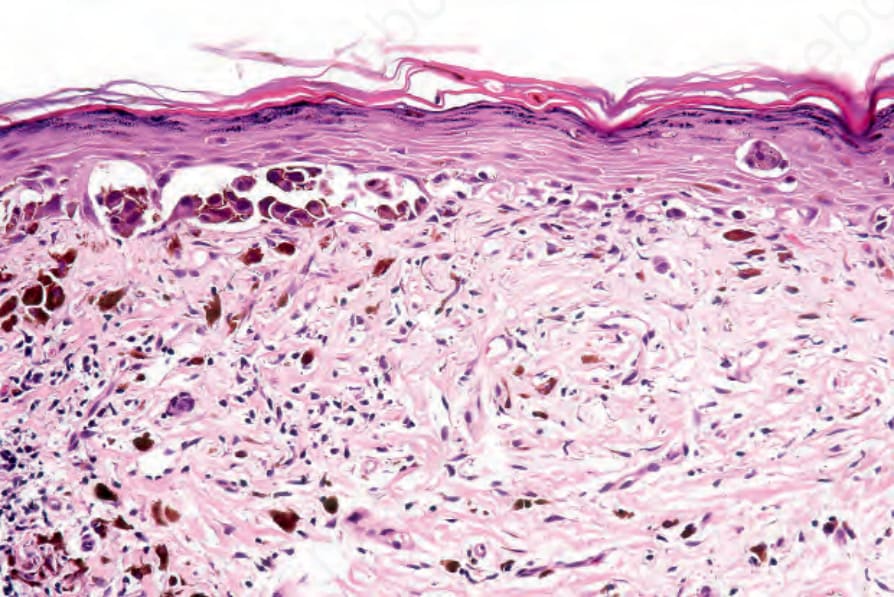
圖 26-48:部分退行 (partial regression):在此變異型中,交界處成分 (junctional component) 仍存在。其意義較不確定。 (Partial regression: in this variant, the junctional component is still present. Its significance is less certain.)
Fig. 26.48 Partial regression: in this variant, the junctional component is still present. Its significance is less certain.
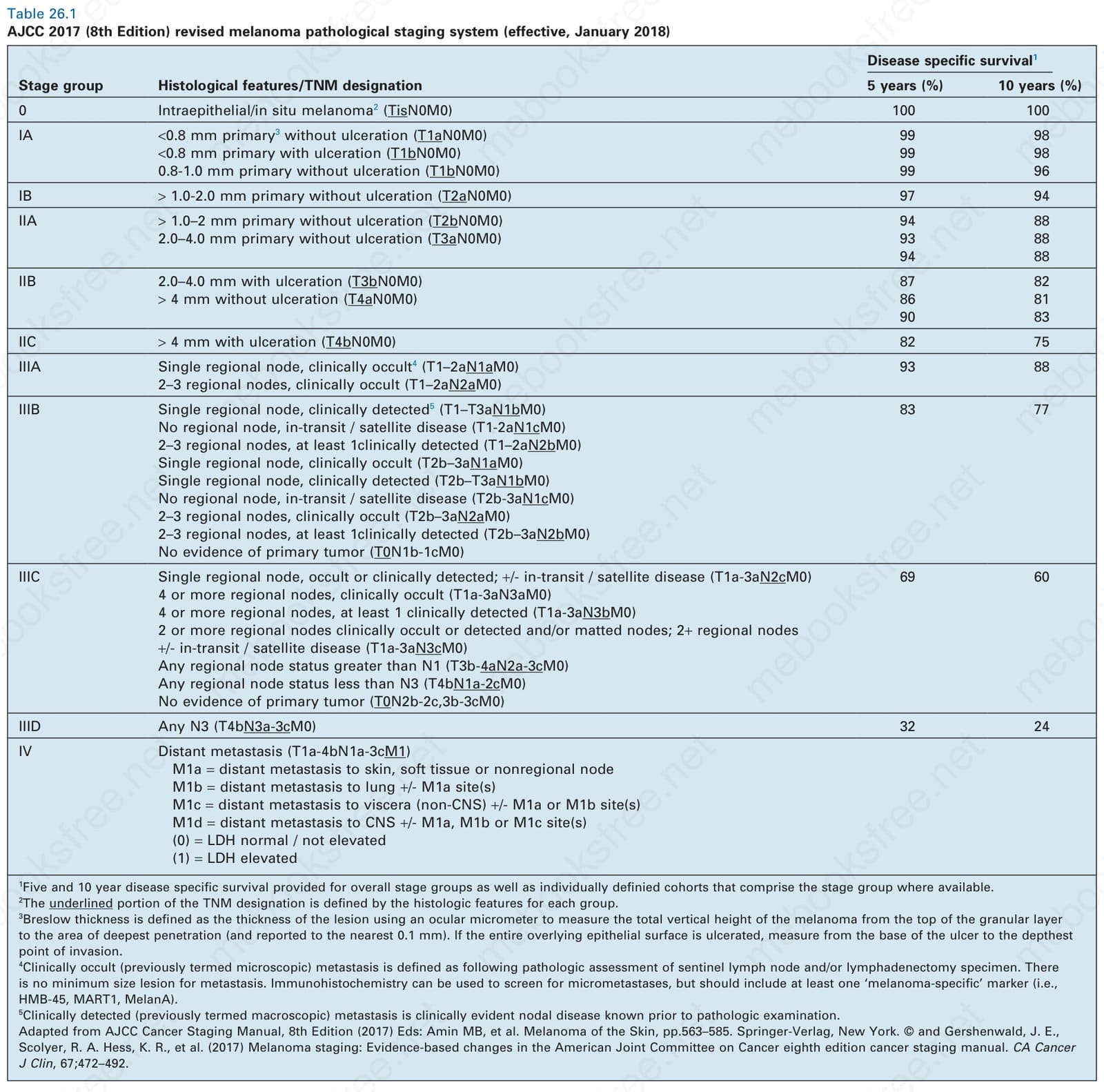
表 26-1:AJCC 2017 (第 8 版) 修訂版黑色素瘤病理分期系統 (2018 年 1 月生效)。 (AJCC 2017 (8th Edition) revised melanoma pathological staging system (effective, January 2018))
Table 26.1 AJCC 2017 (8th Edition) revised melanoma pathological staging system (effective, January 2018)
2017 AJCC 黑色素瘤分期系統的主要變更與澄清
- 資料庫完全來自已知前哨淋巴結狀態的病人,因而建立更同質的分期組
- T0 表示無原發腫瘤證據;Tis 表示原位疾病;TX 表示腫瘤厚度無法測定
- T 類別維持,但 T1 採用新的 0.8 mm 閾值
- 腫瘤厚度現在僅報告至最接近的 0.1 mm
- 原發腫瘤的有絲分裂 (mitoses) 記錄於預後用途,但不再用於分期
- Clark level 不再用於原發腫瘤分期
- 對於區域淋巴結侵犯,為求明確,「microscopic(顯微)」現改稱「clinically occult(臨床隱匿)」,「macroscopic(巨觀)」改稱「clinically detected(臨床偵測)」
- 前哨淋巴結的疾病負荷量 (disease burden) 具預後意義,因而應予記錄,但目前不用於分期
- N 類別現有 4 個亞組,而非三個
- 原發腫瘤狀態 (Breslow 厚度與潰瘍) 大幅修飾第 III 期 (stage III) 的分組
- 移行中 (in transit)、衛星 (satellite) 與微衛星 (microsatellite) 轉移,現依其他受累區域淋巴結數目 (若有),分別歸類為 N1c、N2c、N3c
- 鑑於全身性治療版圖快速演進,第 IV 期 (Stage IV) 不再細分;轉移部位標示與 LDH 升高僅用於界定臨床相關的病人分群
依下表內容(Table 26.1 對應之疾病特異性存活率資料):
| 分期組 (Stage group) | 組織學特徵/TNM 標示 | 5 年 (%) | 10 年 (%) |
|---|---|---|---|
| 0 | 表皮內/原位黑色素瘤² (TisN0M0) | 100 | 100 |
| IA | <0.8 mm 原發³ 無潰瘍 (T1aN0M0) | 99 | 98 |
| IA | <0.8 mm 原發 有潰瘍 (T1bN0M0) | 99 | 98 |
| IA | 0.8-1.0 mm 原發 無潰瘍 (T1bN0M0) | 99 | 96 |
| IB | > 1.0-2.0 mm 原發 無潰瘍 (T2aN0M0) | 97 | 94 |
| IIA | > 1.0–2 mm 原發 無潰瘍 (T2bN0M0) | 94 | 88 |
| IIA | 2.0–4.0 mm 原發 無潰瘍 (T3aN0M0) | 93 | 88(整組 94 / 88) |
| IIB | 2.0–4.0 mm 有潰瘍 (T3bN0M0) | 87 | 82 |
| IIB | > 4 mm 無潰瘍 (T4aN0M0) | 86 | 81(整組 90 / 83) |
| IIC | > 4 mm 有潰瘍 (T4bN0M0) | 82 | 75 |
| IIIA | 單一區域淋巴結,臨床隱匿⁴ (T1–2aN1aM0);2–3 個區域淋巴結,臨床隱匿 (T1–2aN2aM0) | 93 | 88 |
| IIIB | 單一區域淋巴結,臨床偵測⁵ (T1–T3aN1bM0);無區域淋巴結,移行中/衛星病灶 (T1-2aN1cM0);2–3 個區域淋巴結,至少 1 個臨床偵測 (T1–2aN2bM0);單一區域淋巴結,臨床隱匿 (T2b–3aN1aM0);單一區域淋巴結,臨床偵測 (T2b–T3aN1bM0);無區域淋巴結,移行中/衛星病灶 (T2b-3aN1cM0);2–3 個區域淋巴結,臨床隱匿 (T2b–3aN2aM0);2–3 個區域淋巴結,至少 1 個臨床偵測 (T2b–3aN2bM0);無原發腫瘤證據 (T0N1b-1cM0) | 83 | 77 |
| IIIC | 單一區域淋巴結,隱匿或臨床偵測;±移行中/衛星病灶 (T1a-3aN2cM0);4 個或以上區域淋巴結,臨床隱匿 (T1a-3aN3aM0);4 個或以上區域淋巴結,至少 1 個臨床偵測 (T1a-3aN3bM0);2 個或以上臨床隱匿或偵測之區域淋巴結,及/或融合結 (matted nodes);2 個以上區域淋巴結 ±移行中/衛星病灶 (T1a-3aN3cM0);任何大於 N1 之區域淋巴結狀態 (T3b-4aN2a-3cM0);任何小於 N3 之區域淋巴結狀態 (T4bN1a-2cM0);無原發腫瘤證據 (T0N2b-2c,3b-3cM0) | 69 | 60 |
| IIID | 任何 N3 (T4bN3a-3cM0) | 32 | 24 |
| IV | 遠端轉移 (T1a-4bN1a-3cM1)。M1a = 遠端轉移至皮膚、軟組織或非區域淋巴結;M1b = 遠端轉移至肺 ±M1a 部位;M1c = 遠端轉移至內臟 (非 CNS) ±M1a 或 M1b 部位;M1d = 遠端轉移至 CNS ±M1a、M1b 或 M1c 部位。(0) = LDH 正常/未升高;(1) = LDH 升高 |
¹ 提供整體分期組之 5 年與 10 年疾病特異性存活率,並於有資料時提供構成該分期組之個別定義世代。² TNM 標示中加底線的部分由各組的組織學特徵所定義。³ Breslow 厚度定義為使用接目測微計 (ocular micrometer) 測量黑色素瘤從顆粒層頂端至侵犯最深處之總垂直高度(並報告至最接近的 0.1 mm)。若整個上覆上皮表面均潰瘍,則從潰瘍基底量至侵犯最深點。⁴ 臨床隱匿 (clinically occult,前稱 microscopic) 轉移定義為前哨淋巴結及/或淋巴結廓清標本經病理評估後所見。轉移病灶無最小尺寸限制。免疫組化可用於篩檢微轉移 (micrometastases),但應至少包括一個「melanoma-specific」標記 (即 HMB-45、MART1、MelanA)。⁵ 臨床偵測 (clinically detected,前稱 macroscopic) 轉移指病理檢查前即已知的臨床明顯淋巴結疾病。改編自 AJCC Cancer Staging Manual, 8th Edition (2017) Eds: Amin MB, et al. Melanoma of the Skin, pp.563–585. Springer-Verlag, New York. © and Gershenwald, J. E., Scolyer, R. A. Hess, K. R., et al. (2017) Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin, 67;472–492.
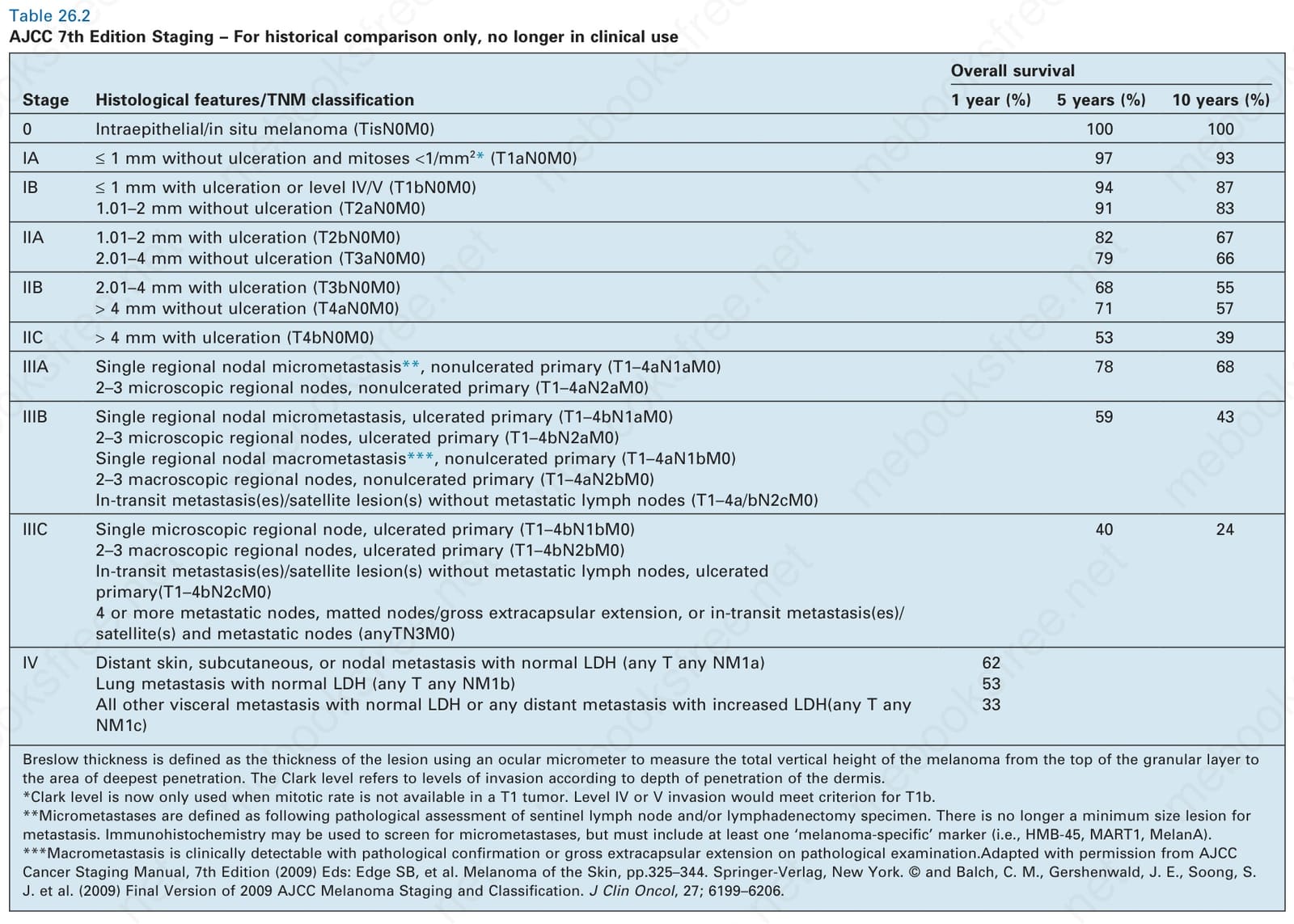
表 26-2:AJCC 第 7 版分期 — 僅供歷史比較,已不再用於臨床。 (AJCC 7th Edition Staging – For historical comparison only, no longer in clinical use)
Table 26.2 AJCC 7th Edition Staging – For historical comparison only, no longer in clinical use
依下表內容(Table 26.2,整體存活率資料):
| 分期 (Stage) | 組織學特徵/TNM 分類 | 1 年 (%) | 5 年 (%) | 10 年 (%) |
|---|---|---|---|---|
| 0 | 表皮內/原位黑色素瘤 (TisN0M0) | 100 | 100 | |
| IA | ≤ 1 mm 無潰瘍且有絲分裂 <1/mm²* (T1aN0M0) | 97 | 93 | |
| IB | ≤ 1 mm 有潰瘍或 level IV/V (T1bN0M0) | 94 | 87 | |
| IB | 1.01–2 mm 無潰瘍 (T2aN0M0) | 91 | 83 | |
| IIA | 1.01–2 mm 有潰瘍 (T2bN0M0) | 82 | 67 | |
| IIA | 2.01–4 mm 無潰瘍 (T3aN0M0) | 79 | 66 | |
| IIB | 2.01–4 mm 有潰瘍 (T3bN0M0) | 68 | 55 | |
| IIB | > 4 mm 無潰瘍 (T4aN0M0) | 71 | 57 | |
| IIC | > 4 mm 有潰瘍 (T4bN0M0) | 53 | 39 | |
| IIIA | 單一區域淋巴結微轉移**,非潰瘍原發 (T1–4aN1aM0);2–3 個顯微區域淋巴結,非潰瘍原發 (T1–4aN2aM0) | 78 | 68 | |
| IIIB | 單一區域淋巴結微轉移,潰瘍原發 (T1–4bN1aM0);2–3 個顯微區域淋巴結,潰瘍原發 (T1–4bN2aM0);單一區域淋巴結巨轉移***,非潰瘍原發 (T1–4aN1bM0);2–3 個巨觀區域淋巴結,非潰瘍原發 (T1–4aN2bM0);移行中轉移/衛星病灶但無轉移淋巴結 (T1–4a/bN2cM0) | 59 | 43 | |
| IIIC | 單一顯微區域淋巴結,潰瘍原發 (T1–4bN1bM0);2–3 個巨觀區域淋巴結,潰瘍原發 (T1–4bN2bM0);移行中轉移/衛星病灶但無轉移淋巴結,潰瘍原發 (T1–4bN2cM0);4 個或以上轉移淋巴結、融合結/肉眼可見之囊外擴展,或移行中轉移/衛星病灶併轉移淋巴結 (anyTN3M0) | 40 | 24 | |
| IV | 遠端皮膚、皮下或淋巴結轉移併 LDH 正常 (any T any NM1a) | 62 | ||
| IV | 肺轉移併 LDH 正常 (any T any NM1b) | 53 | ||
| IV | 所有其他內臟轉移併 LDH 正常,或任何遠端轉移併 LDH 升高 (any T any NM1c) | 33 |
Breslow 厚度定義為使用接目測微計 (ocular micrometer) 測量黑色素瘤從顆粒層頂端至侵犯最深處之總垂直高度。Clark level 指依真皮侵犯深度而分的侵犯層級。*Clark level 現在僅在 T1 腫瘤無法取得有絲分裂率時使用。Level IV 或 V 侵犯符合 T1b 的標準。**微轉移 (micrometastases) 定義為前哨淋巴結及/或淋巴結廓清標本經病理評估後所見。轉移病灶不再有最小尺寸限制。免疫組化可用於篩檢微轉移,但必須至少包括一個「melanoma-specific」標記 (即 HMB-45、MART1、MelanA)。***巨轉移 (macrometastasis) 為臨床可偵測並經病理確認,或病理檢查見肉眼可見之囊外擴展。經授權改編自 AJCC Cancer Staging Manual, 7th Edition (2009) Eds: Edge SB, et al. Melanoma of the Skin, pp.325–344. Springer-Verlag, New York. © and Balch, C. M., Gershenwald, J. E., Soong, S. J. et al. (2009) Final Version of 2009 AJCC Melanoma Staging and Classification. J Clin Oncol, 27; 6199–6206.
潰瘍 (ulceration) 的有無及潰瘍寬度是獨立的預後指標,應予記錄。175,211 潰瘍定義為「依組織切片之顯微檢查,原發黑色素瘤大部分表面上覆完整表皮的缺失」。203 必須排除外傷與人工假象造成的表皮缺失。潰瘍與顯著升高的轉移風險相關,最早在 AJCC 第 6 版被納入為 T 分類的第二項決定因素,並在現行第 8 版中保留。196,203,206,208,209,212
腫瘤浸潤淋巴球 (tumor-infiltrating lymphocytes) 是重要的獨立預後變項,應記錄為 brisk、nonbrisk 或 absent(Figs 26.44–26.46)。145,206,213–215 brisk 類別意指淋巴球存在於整個垂直生長期,或延伸橫跨其整個基底。Nonbrisk 腫瘤浸潤淋巴球意指僅有局部浸潤。Absent 包含兩種類別:要嘛完全沒有淋巴球,要嘛淋巴球存在但未浸潤黑色素瘤。Brisk 淋巴球反應傾向為薄型黑色素瘤的特徵,而淋巴球反應缺如一般見於厚型黑色素瘤。200,214 在一項針對 285 個垂直生長期腫瘤的研究中,brisk、nonbrisk 與 absent 腫瘤浸潤淋巴球的 10 年存活率分別為百分之五十五、百分之四十五與百分之二十七。214 近期有研究指出,腫瘤浸潤淋巴球受性別影響,且僅在男性而非女性中與前哨淋巴結狀態相關。216 不令人意外的是,在一項對 887 名病人進行完整多變項分析的世代中,腫瘤浸潤淋巴球的缺如亦與前哨淋巴結轉移相關,作為黑色素瘤風險的替代標記。215 影像分析 (image analysis) 與特徵擷取 (feature extraction) 已被用於評估腫瘤浸潤淋巴球,並獲得良好結果。217 評估淋巴結轉移中的腫瘤浸潤淋巴球亦具預測價值。218,219
在薄型黑色素瘤中,辨識退行 (regression) 的特徵很重要,這在真皮成分中可能特別明顯(Figs 26.47 與 26.48)。145,220 這些特徵包括惡性黑色素細胞 (malignant melanocytes) 缺如或數目減少、退化 (凋亡, apoptotic) 形態,以及慢性發炎細胞浸潤(Fig. 26.49)。221–223 噬黑色素細胞 (melanophages)、水平瘢痕化、孤立的腫瘤島 (tumor islands) 與毛細血管擴張性血管 (telangiectatic vessels) 在較晚期亦常出現。臨床上,退行表現為斑狀的灰、白或粉紅色區域。
雖然退行作為生物學行為決定因素的重要性在文獻上一直是相當有爭議的議題,但若干作者認為,在薄型腫瘤中,它與較差的預後相關,惟此一貢獻在許多病例中相對於其他因素可能較為次要。223–232 一個未診斷之原發黑色素瘤的完全退行 (complete regression),可能是某些病人以未知原發 (unknown primary) 之轉移性腫瘤表現的原因(Fig. 26.50)。233 部分作者建議,若有廣泛 (> 50%) 退行的證據,薄型黑色素瘤應接受前哨淋巴結切片,而其他系列研究則未顯示退行與淋巴結狀態之間的關聯。176,234
有絲分裂率 (mitotic rate) 由腫瘤中有絲分裂最活躍區域之每 1 mm² 有絲分裂相 (mitotic figures) 數目來決定。已明確的是,呈現高有絲分裂率的腫瘤與較差的預後相關,且有絲分裂為比潰瘍更穩健的結局預測因子,因此有絲分裂率被納入第 7 版 AJCC 分期系統。145,204,235–240 雖然有絲分裂仍被認可為預後因子,但現行第 8 版 AJCC 分期系統因分期組穩定性之故,依賴潰瘍而非有絲分裂。196,206 儘管早先有相反的證據,且腫瘤厚度、潰瘍與有絲分裂率之間有複雜的相互關係,有絲分裂率似乎攜帶獨立於另兩個因素的預後資訊。176,241,242
顯微衛星 (microscopic satellite) 的存在定義為:與主原發腫瘤團塊不連續、由正常組織 (無瘢痕化、纖維化或廣泛發炎) 分隔、位於任何距離之任何大小的獨立腫瘤結節。206 它見於較厚的腫瘤,並與局部復發、區域淋巴結轉移風險增加及存活率降低相關。243–246 在 2017 年 AJCC 黑色素瘤分期系統中,微衛星的存在會使分期升級:若無區域淋巴結侵犯則升級至 N1c,而若分別有一個或多於一個淋巴結受累則升級至 N2c 或 N3c。206
淋巴侵犯 (lymphatic invasion) 的存在與移行中轉移 (in-transit metastases) 的發生相關(Fig. 26.51)。247 在若干研究中,淋巴血管侵犯 (lymphovascular invasion) 已被證實為黑色素瘤存活率降低的預測因子。215,248–253 使用 D2-40 免疫組化可顯著提高偵測淋巴侵犯的敏感度,並與淋巴結轉移及存活相關。254–257 尚需更多研究與前瞻性試驗來驗證此技術的應用與判讀。反之,在若干研究中,厚型黑色素瘤缺乏血管侵犯與存活率增加相關。258,259 神經周圍 (perineural) 與神經內 (intraneural) 浸潤最常見於促結締組織增生性 (desmoplastic) 變異型,因而部分解釋了其局部復發風險增加的原因(Fig. 26.52)。在此情境下,CD57 免疫組化有助於辨識殘留神經(Fig. 26.53)。
血管新生 (angiogenesis) 定義為黑色素瘤基底處新生血管日益增多的發展,其與腫瘤厚度的增加呈平行關係。260–265 因此,血管新生增加與厚型腫瘤、潰瘍、復發及腫瘤相關死亡相關。263,266 或許與淋巴血管侵犯的可能性有關,以 D2-40 或 VEGF-C 測得的腫瘤內 (intratumoral) 及腫瘤周圍 (peritumoral) 淋巴管新生 (lymphangiogenesis) 增加,亦與前哨淋巴結轉移及疾病特異性存活率降低相關。267,268
前哨淋巴結切片 (sentinel node biopsy) 亦提供極有價值的預後資訊。269–273 它已被證實為決定第 I 期與第 II 期疾病腫瘤復發可能性及病人存活的最重要因素。270 隨著 MSLT-II 試驗未能顯示完成性淋巴結廓清 (completion lymph node dissection) 的存活益處,對前哨淋巴結陽性者施行該完成性術式預期將變得較不常見。274,275 最新的 AJCC 分期系統要求,在前哨淋巴結資料能影響治療決策的病例中應納入該資料,因為此術式可顯著提高分期組的準確性與鑑別力。204,206 淋巴結沿其長軸對半剖開 (bivalved) 或連續切片,除了檢查蘇木精-伊紅 (hematoxylin and eosin) 染色切片外,在最初切片陰性的病例中,應一律執行免疫組化 — 例如 S100 protein、HMB-45 及/或 MART-1 (melanoma antigen recognized by T cells 1)。使用針對「melanoma-specific」抗原 (如 HMB-45 或 MART1) 的抗體偵測單一或微小細胞群,現已納入 AJCC 分期系統。較近期,有人提議採用分子技術,包括針對 tyrosinase messenger RNA 的反轉錄酶聚合酶連鎖反應 (reverse transcriptase polymerase chain reaction)。276,277 此類術式的一大缺點是可能出現偽陽性結果,因為常有良性的囊膜痣 (capsular nevi) 存在,惟使用對黑色素瘤較痣細胞更具特異性的標記,或可緩解此問題。278
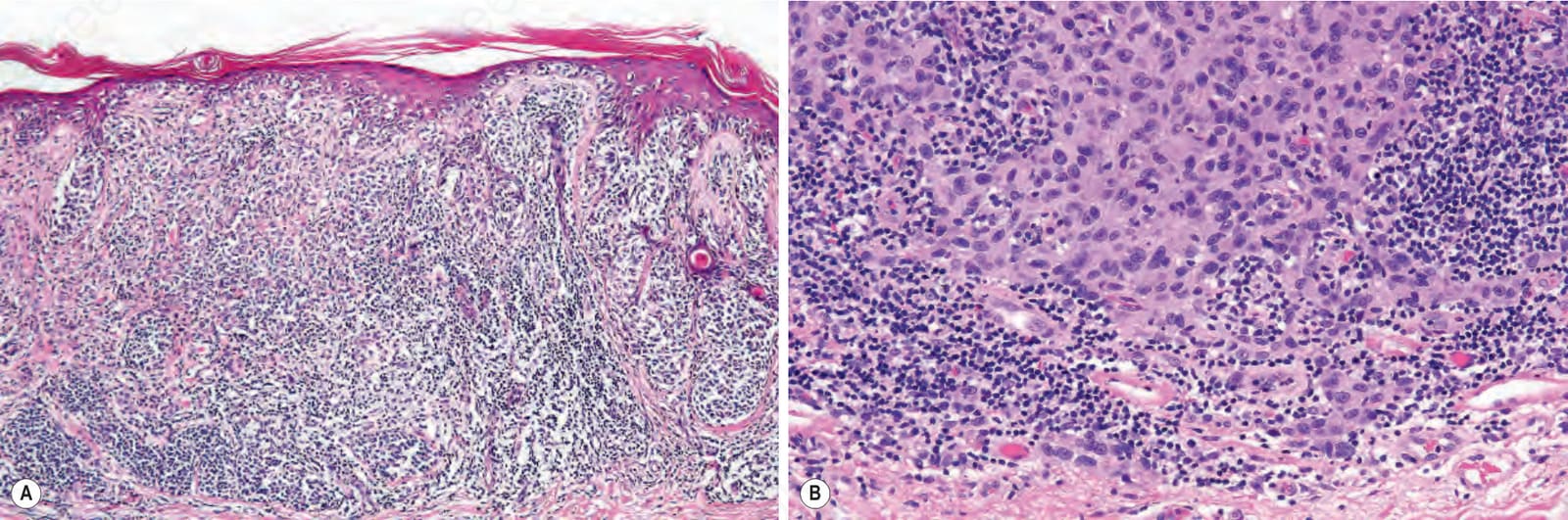
圖 26-44:(A, B) 黑色素瘤:腫瘤浸潤淋巴球 (tumor infiltrating lymphocytes)。Category A – Brisk:淋巴球浸潤腫瘤並延伸至病灶整個基底。 (Melanoma: tumor infiltrating lymphocytes. Category A – Brisk: the lymphocytes infiltrate the tumor and extend along the whole of the base of the lesion.)
Fig. 26.44 (A, B) Melanoma: tumor infiltrating lymphocytes. Category A – Brisk: the lymphocytes infiltrate the tumor and extend along the whole of the base of the lesion.
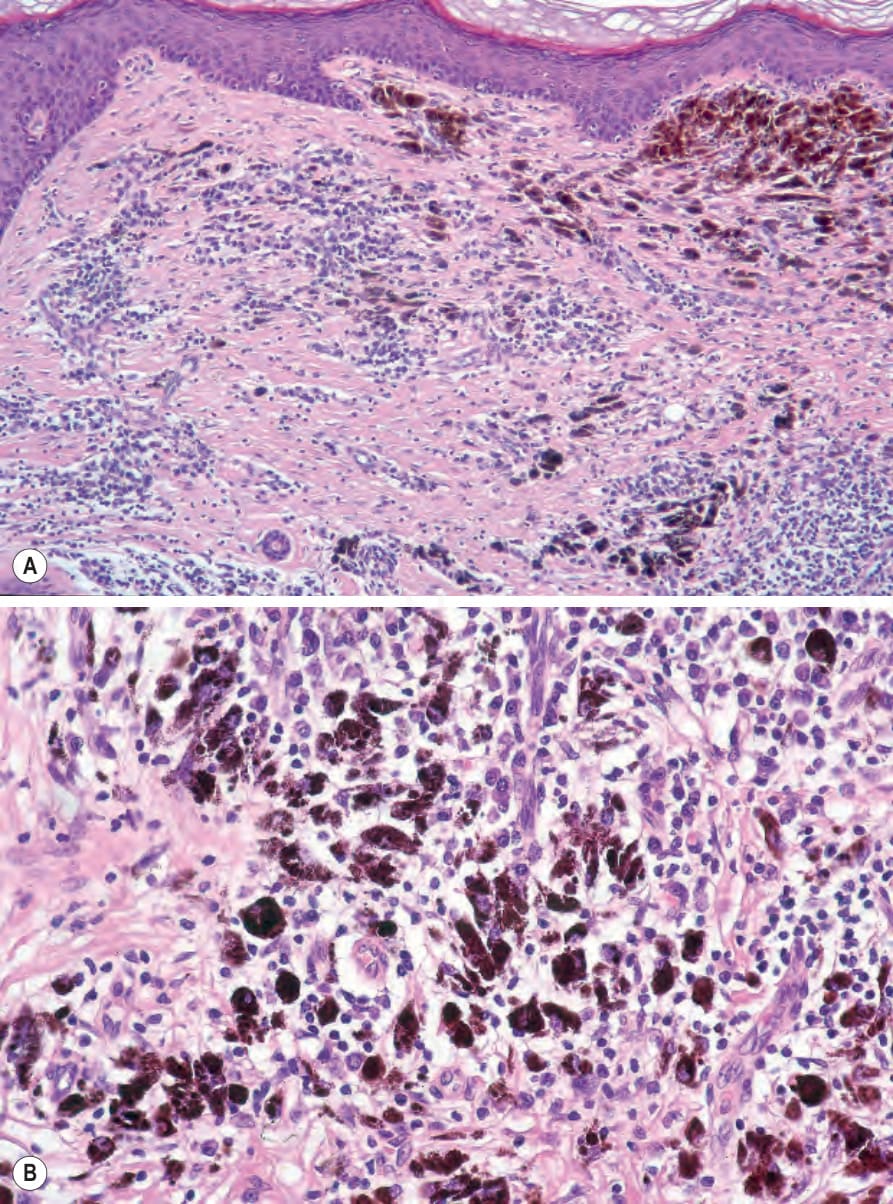
圖 26-47:(A, B) 退行 (regression):無殘留的表皮成分。注意淋巴球浸潤、漿細胞 (plasma cells)、豐富的含黑色素巨噬細胞 (melanin-containing macrophages)、瘢痕化與明顯的血管。 (Regression: no residual epidermal component is present. Note the lymphocytic infiltrate, plasma cells, abundant melanin-containing macrophages, scarring, and conspicuous vasculature.)
Fig. 26.47 (A, B) Regression: no residual epidermal component is present. Note the lymphocytic infiltrate, plasma cells, abundant melanin-containing macrophages, scarring, and conspicuous vasculature.
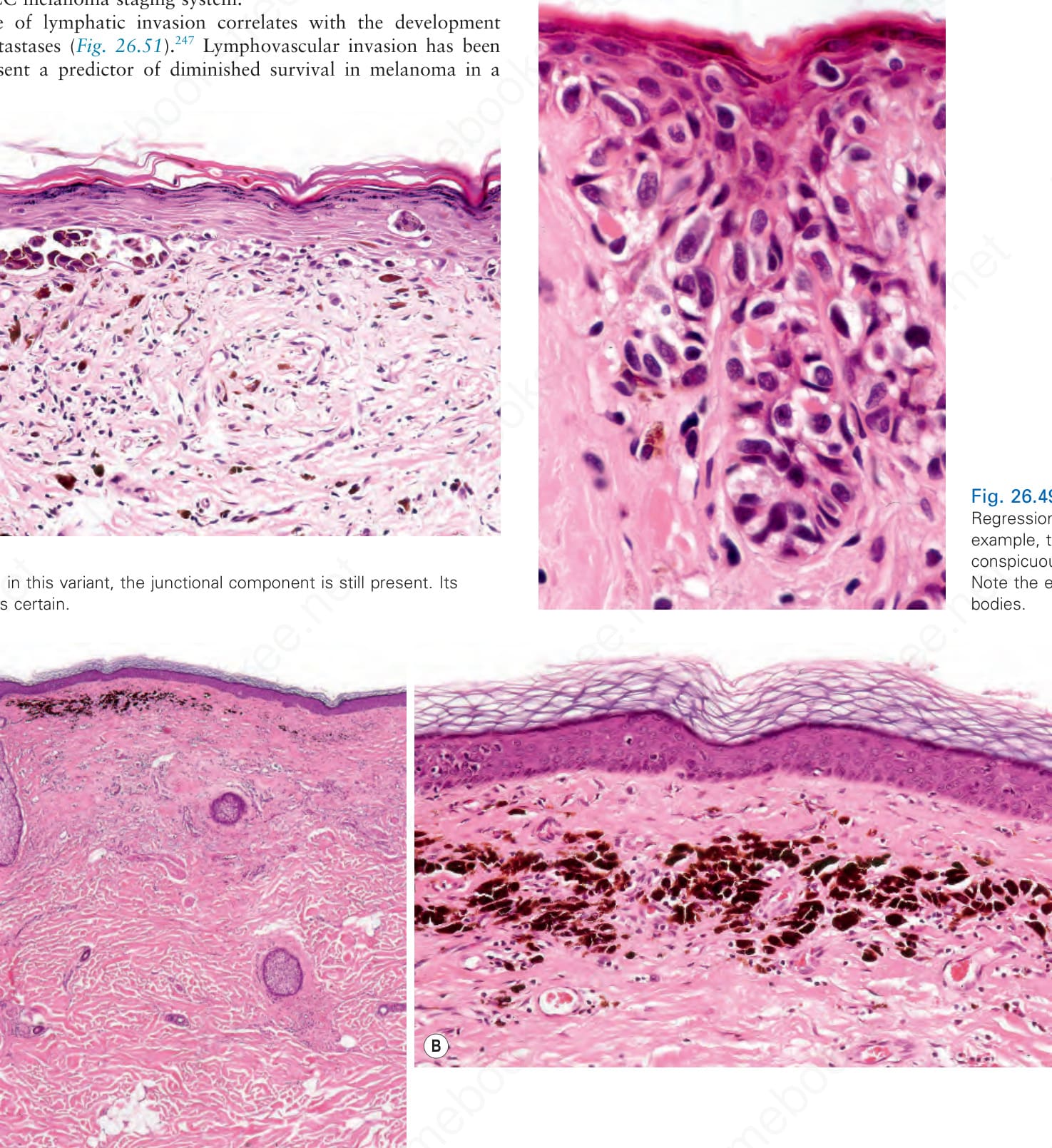
圖 26-49:退行 (regression):在此例中,有明顯的凋亡 (apoptosis)。注意嗜伊紅小體 (eosinophilic bodies)。 (Regression: in this example, there is conspicuous apoptosis. Note the eosinophilic bodies.)
Fig. 26.49 Regression: in this example, there is conspicuous apoptosis. Note the eosinophilic bodies.
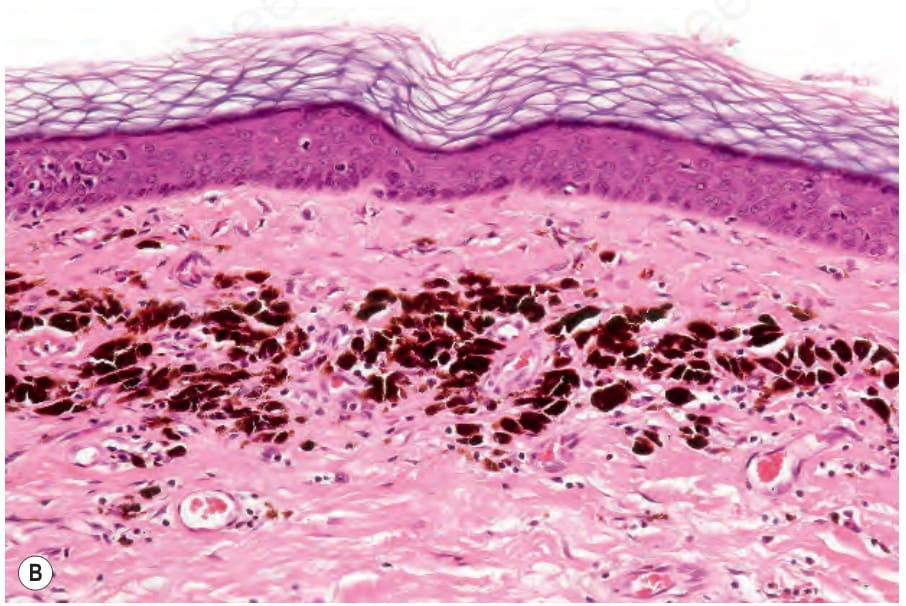
圖 26-50:(A, B) 退行 (regression):在此例中,無殘留腫瘤。真皮有瘢痕化,並有豐富的黑色素 (melanin pigment)。病人以未知原發 (unknown primary) 表現。承蒙 M. Forder, MD, St Anne’s Medical Center, Pietermaritzburg, South Africa 提供。 (Regression: in this example, there is no residual tumor. The dermis is scarred and there is abundant melanin pigment. The patient presented with an unknown primary. By courtesy of M. Forder, MD, St Anne’s Medical Center, Pietermaritzburg, South Africa.)
Fig. 26.50 (A, B) Regression: in this example, there is no residual tumor. The dermis is scarred and there is abundant melanin pigment. The patient presented with an unknown primary. By courtesy of M. Forder, MD, St Anne’s Medical Center, Pietermaritzburg, South Africa.
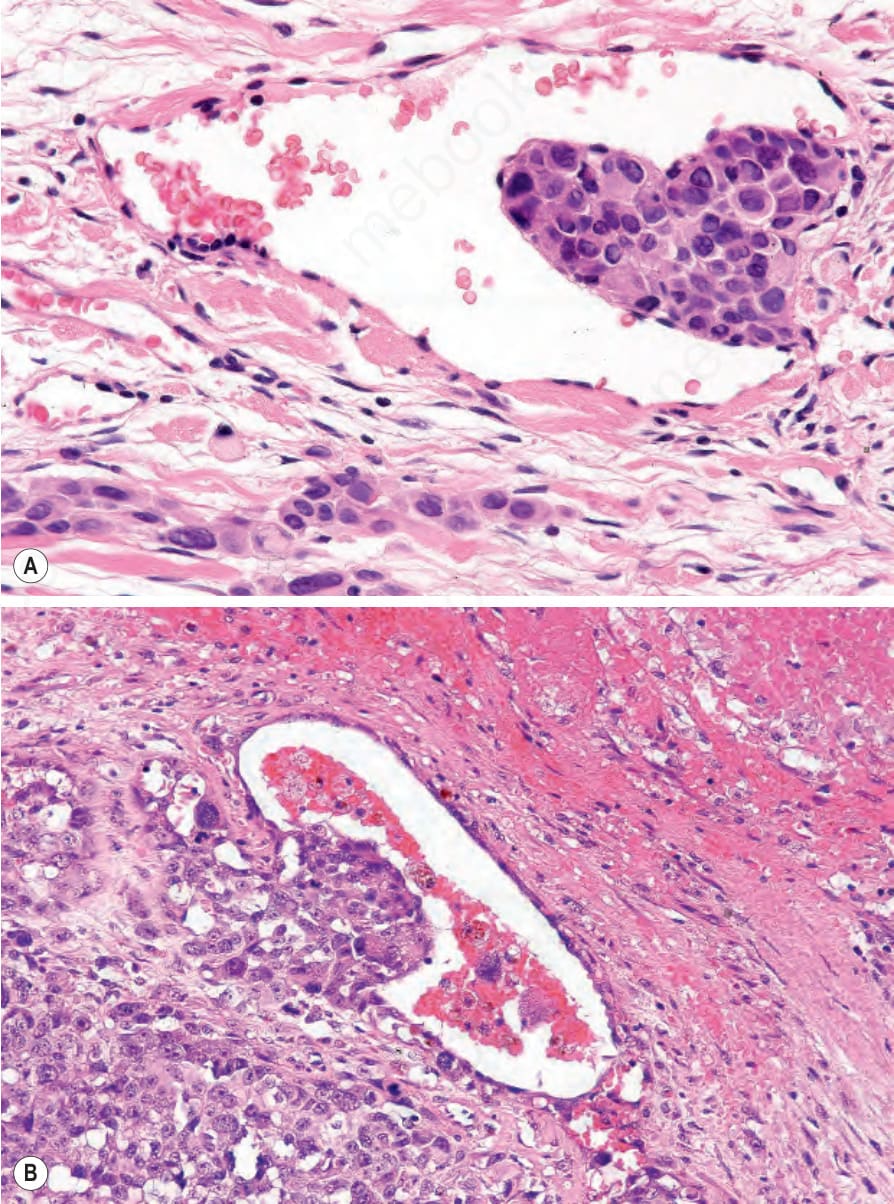
圖 26-51:黑色素瘤:血管侵犯 (vascular invasion):(A) 多形性腫瘤細胞黏附於內皮 (endothelium);(B) 腫瘤細胞長入管腔內。 (Melanoma: vascular invasion: (A) pleomorphic tumor cells are adherent to the endothelium; (B) tumor cells are growing into the lumen.)
Fig. 26.51 Melanoma: vascular invasion: (A) pleomorphic tumor cells are adherent to the endothelium; (B) tumor cells are growing into the lumen.
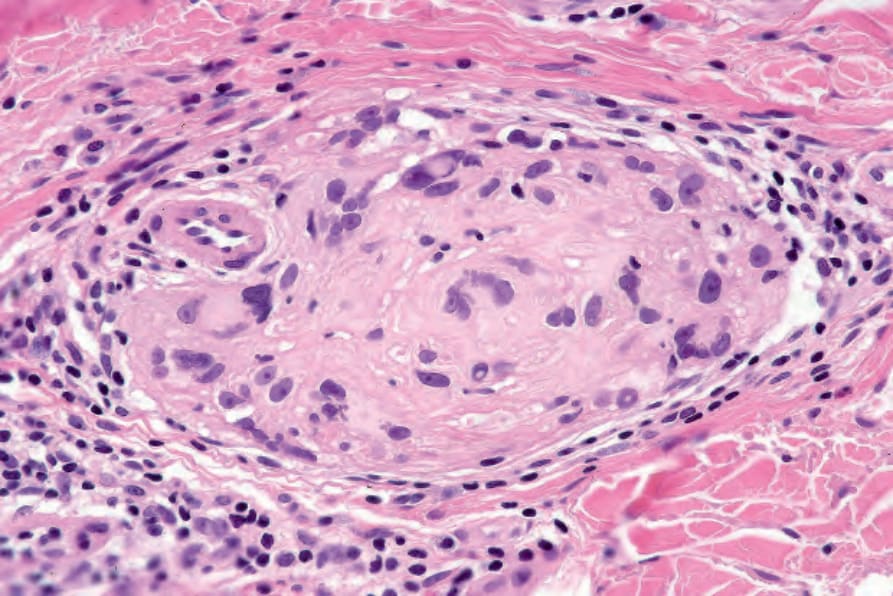
圖 26-52:黑色素瘤:神經內侵犯 (intraneural invasion)。注意此神經幹 (nerve trunk) 內的多形性腫瘤核。 (Melanoma: intraneural invasion. Note the pleomorphic tumor nuclei within this nerve trunk.)
Fig. 26.52 Melanoma: intraneural invasion. Note the pleomorphic tumor nuclei within this nerve trunk.
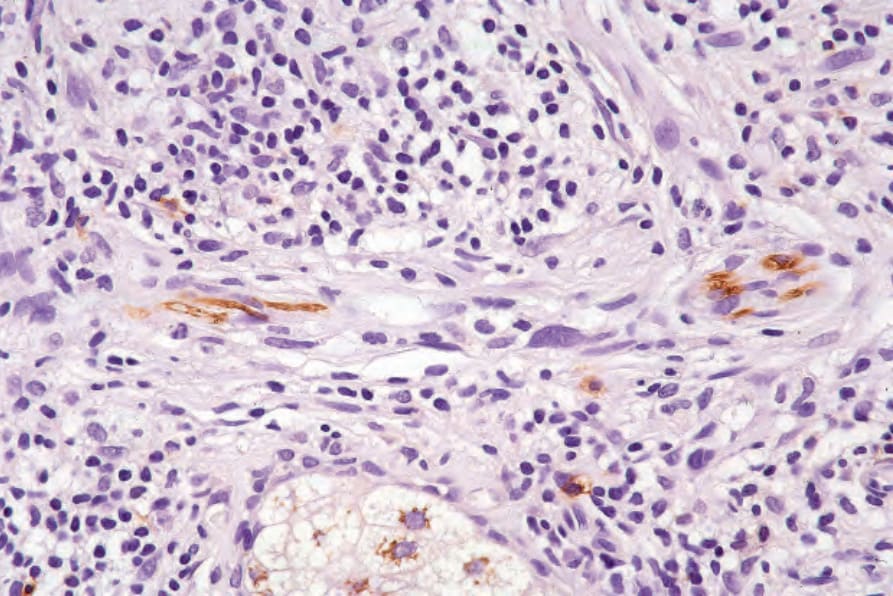
圖 26-53:黑色素瘤:當腫瘤生長大致破壞神經時,CD57 免疫組化可能特別有價值。 (Melanoma: CD57 immunohistochemistry may be particularly valuable when tumor growth has largely destroyed the nerve.)
Fig. 26.53 Melanoma: CD57 immunohistochemistry may be particularly valuable when tumor growth has largely destroyed the nerve.
前哨淋巴結切片目前建議用於所有厚度為 1.00 mm 或以上的腫瘤。其他可能的適應症包括潰瘍性腫瘤、退行達 50% 或以上的腫瘤、已達垂直生長期的腫瘤,以及那些已被切片且侵犯深部邊緣 (deep margin) 的病灶。176,272,279,280 對於厚度小於 1.00 mm 但呈現顯著有絲分裂活性的腫瘤,亦應考慮施行此術式。281