Prognostic indicators
Prognostic indicators
While the vast majority of thin melanomas do not metastasize, between 1% and 2% are known to do so. Conversely, occasional thick melanomas fail to disseminate. With this in mind, there has been intensive research in an effort to define those tumors that have the capacity for spread with
resultant death, in the hope that adjuvant chemotherapy, immunotherapy, or other forms of treatment might eventually benefit significant numbers of patients. Prognostic indicators include clinical parameters, morphological observations, and measurements in addition to immunohistochemical markers of cell proliferation, cell regulation, and so on. Many of the morphological observations are tried and tested, but the search for the elusive immunohistochemical marker of metastatic potential has not yet been fruitful. Genomic biomarkers are also being explored, in particular limited gene expression panels.171–173
Clinical prognostic indicators include age, sex, and site of the primary tumor.174–180 Older patients fare worse than younger ones, and males have a poorer outlook than females.7,176,177,181–184 The latter is independent of tumor thickness and site.176 Particularly high-risk sites include the back, upper arm, neck, and scalp (BANS).185 The acral sites are also thought to be associated with a poorer prognosis.186
When reporting melanoma, it is generally accepted as essential worldwide to record and comment on the following variables:176,187–193
• tumor thickness (Breslow method),
• level of invasion (Clark method),
• growth phase (vertical or radial),
• mitotic rate,
• ulceration,
• lymphovascular invasion,
• perineural infiltration,
• regression,
• microsatellitosis,
• tumor infiltrating lymphocytes. Growth phase is also noted although it should be emphasized that great care must be taken before allocating a melanoma to the microinvasive category of radial (horizontal) growth phase. Dermal mitoses automatically place a tumor in the vertical growth phase (see Fig. 26.14). These elements have become critical for proper staging and prognostic assignment of patients, but unfortunately even in countries with a high incidence and acute awareness of cutaneous melanoma, many of the above elements are absent from routine reports.194
A
B
1321 Prognostic indicators
A
Breslow tumor thickness is the single most important single prognostic indicator for primary cutaneous melanoma.195,196 It is measured from the most superficial aspect of the granular cell layer to the deepest point of invasion of the tumor. In ulcerated tumors, the measurement should be from the base of the ulcer. The significance of periadnexal extension is less clear. If the latter is greater than the conventional Breslow thickness, the information should also be documented in addition to the traditional Breslow measurement (Fig. 26.43). Polypoid tumors should be treated no differently, and should be measured through the thickest region.197 Tumor volume, therefore, is a most important factor influencing outcome in vertical growth phase melanoma. Careful evaluation of the greatest tumor thickness provides very useful prognostic guidance.198–201 In the latest (8th) edition of the American Joint Committee on Cancer (AJCC) staging system (2017, effective in 2018), the thickness thresholds have been maintained as in the 7th Edition at 1.0, 2.0, and 4.0 mm, though the T1 group is subdivided 0.8 mm as well (Table 26.1).196,202–206 The 7th edition staging is still
B
1322 Melanoma
Major changes and clarifications of the 2017 AJCC melanoma staging system
• Database completely derived from patients of known sentinel lymph node status thus creating more homogeneous stage groups
• T0 designates no evidence of primary tumor; Tis designates in situ disease; TX designates tumor thickness that cannot be determined
• T categories maintained, but T1 with new 0.8 mm threshold
• Tumor thickness now reported only to nearest 0.1 mm
• Mitoses in primary tumor are recorded for prognosis, but no longer used for staging
• Clark level no longer used for staging primary
• For regional lymph node involvement, “microscopic” is now termed “clinically occult” and “macroscopic” termed “clinically detected” for clarity
• Sentinel lymph node is disease burden is prognostic and thus to be recorded, but not currently used for staging
• N category now has 4 subgroups rather than three
• Status of the primary (Breslow thickness and ulceration) extensively modifies stage III groupings
• In transit, satellite and microsatellite metastases are now categorized as N1c, N2c, N3c based on how many other regional nodes are involved (if any)
• Given the rapidly evolving systemic therapy landscape, Stage IV is no longer subdivided; metastatic site designation and LDH elevation are used solely to define clinically relevant patient groupings
provided here for purposes of comparison (Table 26.2). A pleasant feature of the new staging system is that Breslow thickness is now only reported to one significant digit after the decimal point, simplifying measurement with the micrometer. While certainly not perfect, clinical and particularly micropathological staging in melanoma is exceedingly powerful and serves as a model for other cancers.
The level of tumor invasion when classified according to Clark levels is as follows:
• Level I: in situ melanoma,
• Level II: invasion of the papillary dermis by single cells or small nests,
• Level III: invasive tumor usually as an expansile nodule abutting on the reticular dermal interface,
• Level IV: invasion of the reticular dermis,
• Level V: invasion of the subcutaneous fat. The dermal interface may be identified by the site of the superficial capillary plexus. It also corresponds to the zone of transformation of the horizontally orientated reticular dermis elastic fibers to the vertically aligned ones of the papillary dermis. The distinction between Clark level II and III and perhaps
1323 Prognostic indicators
Stage group Histological features/TNM designation
Disease specific survival1
5 years (%) 10 years (%)
0 Intraepithelial/in situ melanoma2 (TisN0M0) 100 100
IA <0.8 mm primary3 without ulceration (T1aN0M0) 99 98 <0.8 mm primary with ulceration (T1bN0M0) 99 98 0.8-1.0 mm primary without ulceration (T1bN0M0) 99 96
IB > 1.0-2.0 mm primary without ulceration (T2aN0M0) 97 94
IIA > 1.0–2 mm primary without ulceration (T2bN0M0) 94 88 2.0–4.0 mm primary without ulceration (T3aN0M0) 93 88 94 88
IIB 2.0–4.0 mm with ulceration (T3bN0M0) 87 82 > 4 mm without ulceration (T4aN0M0) 86 81 90 83
IIC > 4 mm with ulceration (T4bN0M0) 82 75
IIIA Single regional node, clinically occult4 (T1–2aN1aM0) 2–3 regional nodes, clinically occult (T1–2aN2aM0)
IIIB Single regional node, clinically detected5 (T1–T3aN1bM0) No regional node, in-transit / satellite disease (T1-2aN1cM0) 2–3 regional nodes, at least 1clinically detected (T1–2aN2bM0) Single regional node, clinically occult (T2b–3aN1aM0) Single regional node, clinically detected (T2b–T3aN1bM0) No regional node, in-transit / satellite disease (T2b-3aN1cM0) 2–3 regional nodes, clinically occult (T2b–3aN2aM0) 2–3 regional nodes, at least 1clinically detected (T2b–3aN2bM0) No evidence of primary tumor (T0N1b-1cM0)
93 88
83 77
IIIC Single regional node, occult or clinically detected; +/- in-transit / satellite disease (T1a-3aN2cM0) 4 or more regional nodes, clinically occult (T1a-3aN3aM0) 4 or more regional nodes, at least 1 clinically detected (T1a-3aN3bM0) 2 or more regional nodes clinically occult or detected and/or matted nodes; 2+ regional nodes +/- in-transit / satellite disease (T1a-3aN3cM0) Any regional node status greater than N1 (T3b-4aN2a-3cM0) Any regional node status less than N3 (T4bN1a-2cM0) No evidence of primary tumor (T0N2b-2c,3b-3cM0)
69 60
IIID Any N3 (T4bN3a-3cM0) 32 24
IV Distant metastasis (T1a-4bN1a-3cM1) M1a = distant metastasis to skin, soft tissue or nonregional node M1b = distant metastasis to lung +/- M1a site(s) M1c = distant metastasis to viscera (non-CNS) +/- M1a or M1b site(s) M1d = distant metastasis to CNS +/- M1a, M1b or M1c site(s) (0) = LDH normal / not elevated (1) = LDH elevated
1Five and 10 year disease specific survival provided for overall stage groups as well as individually definied cohorts that comprise the stage group where available. 2The underlined portion of the TNM designation is defined by the histologic features for each group. 3Breslow thickness is defined as the thickness of the lesion using an ocular micrometer to measure the total vertical height of the melanoma from the top of the granular layer to the area of deepest penetration (and reported to the nearest 0.1 mm). If the entire overlying epithelial surface is ulcerated, measure from the base of the ulcer to the depthest point of invasion. 4Clinically occult (previously termed microscopic) metastasis is defined as following pathologic assessment of sentinel lymph node and/or lymphadenectomy specimen. There is no minimum size lesion for metastasis. Immunohistochemistry can be used to screen for micrometastases, but should include at least one ‘melanoma-specific’ marker (i.e., HMB-45, MART1, MelanA). 5Clinically detected (previously termed macroscopic) metastasis is clinically evident nodal disease known prior to pathologic examination. Adapted from AJCC Cancer Staging Manual, 8th Edition (2017) Eds: Amin MB, et al. Melanoma of the Skin, pp.563–585. Springer-Verlag, New York. © and Gershenwald, J. E., Scolyer, R. A. Hess, K. R., et al. (2017) Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin, 67;472–492.
more so between III and IV is somewhat difficult to apply in practice and is observer dependent.207 Clark level was believed to provide independent prognostic information for thin tumors (1.0 mm or less in thickness) but not for thicker melanomas.208,209 The latest data indicate that if mitotic rate is assessable in thin melanomas, then Clark level no longer provides additional prognostic information. The 2017 (8th) AJCC staging system no longer recommends the use of the Clark level, even for thin melanomas, as in the previous edition.196,203,204,206 Mitotic rate in the primary melanoma correlates with sentinel lymph node positivity for metastasis.210
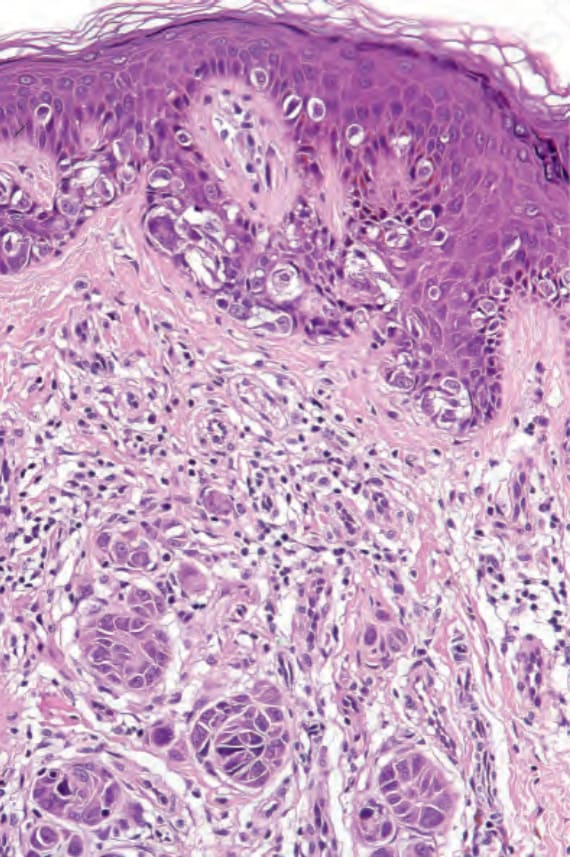
Fig. 26.14 Melanoma: vertical growth phase. In addition to in situ (radial growth phase) tumor, there are multiple nests in the dermis. These are larger than the epidermal ones.
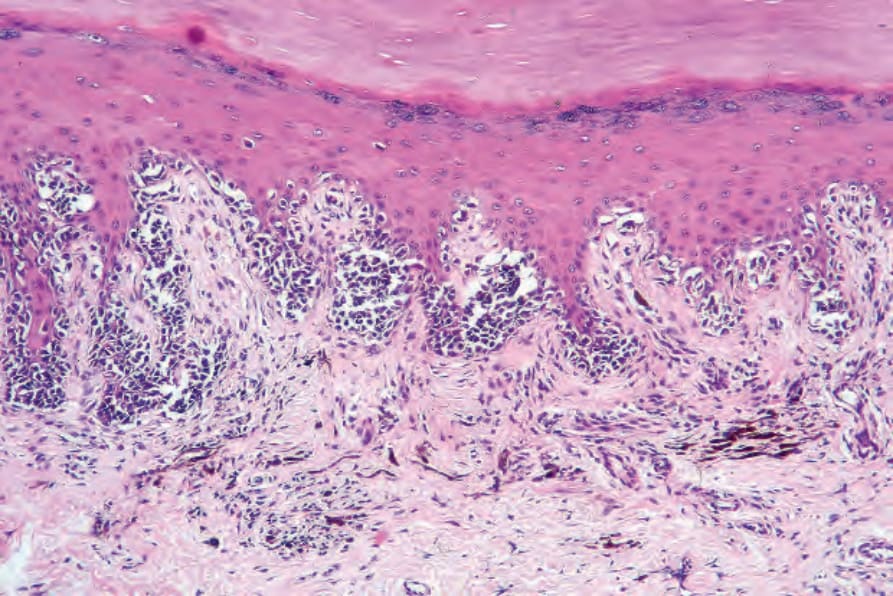
Fig. 26.33 Acral lentiginous melanoma: in this in situ lesion, there is irregular acanthosis, hypergranulosis, and hyperkeratosis. Tumor cells are hyperchromatic and distributed in a lentiginous and nested pattern. The dermis is scarred and there are conspicuous melanophages and chronic inflammatory cells.
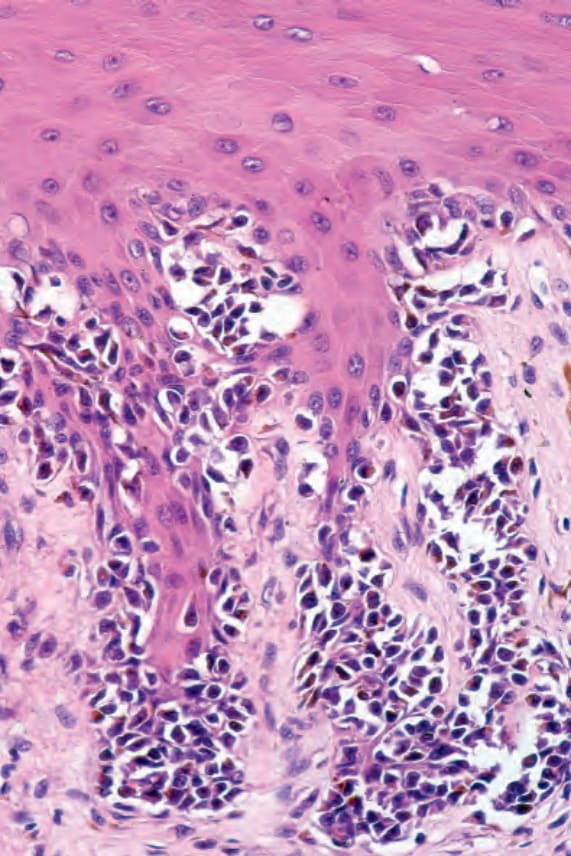
Fig. 26.34 Acral lentiginous melanoma: there is conspicuous cytoplasmic retraction, hyperchromatism, and nuclear atypia.
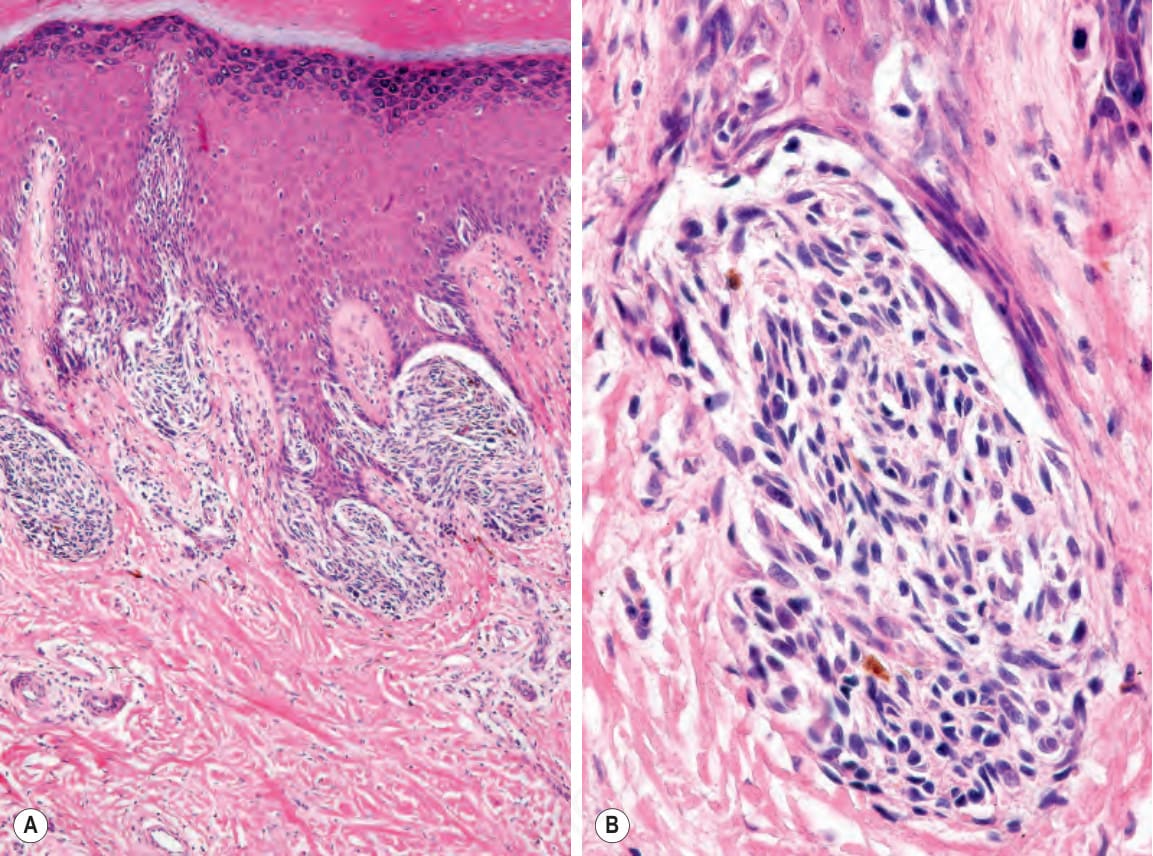
Fig. 26.35 (A, B) Acral lentiginous melanoma: large junctional nests are present at the tips of the rete.
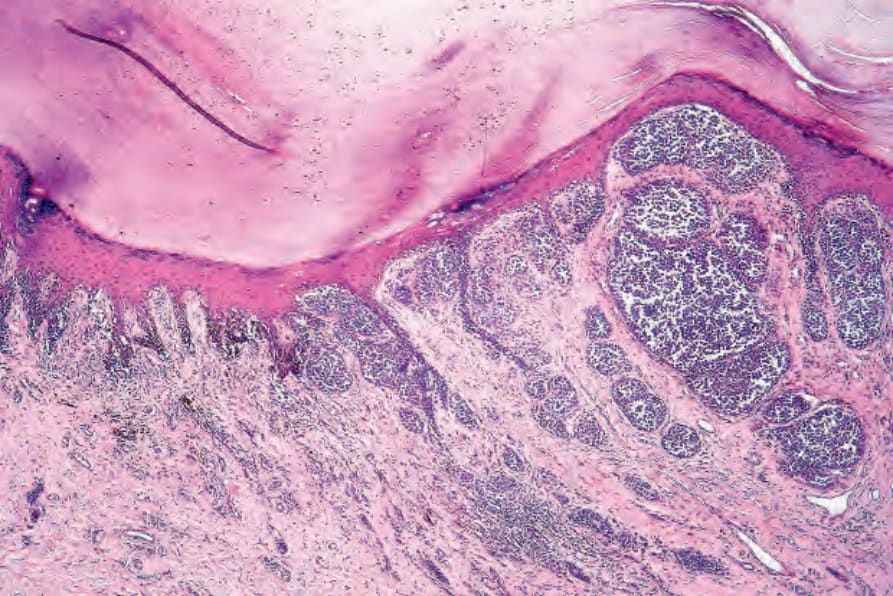
Fig. 26.36 Acral lentiginous melanoma: in this example, the invasive component is mixed epithelioid, spindled cell, and desmoplastic.
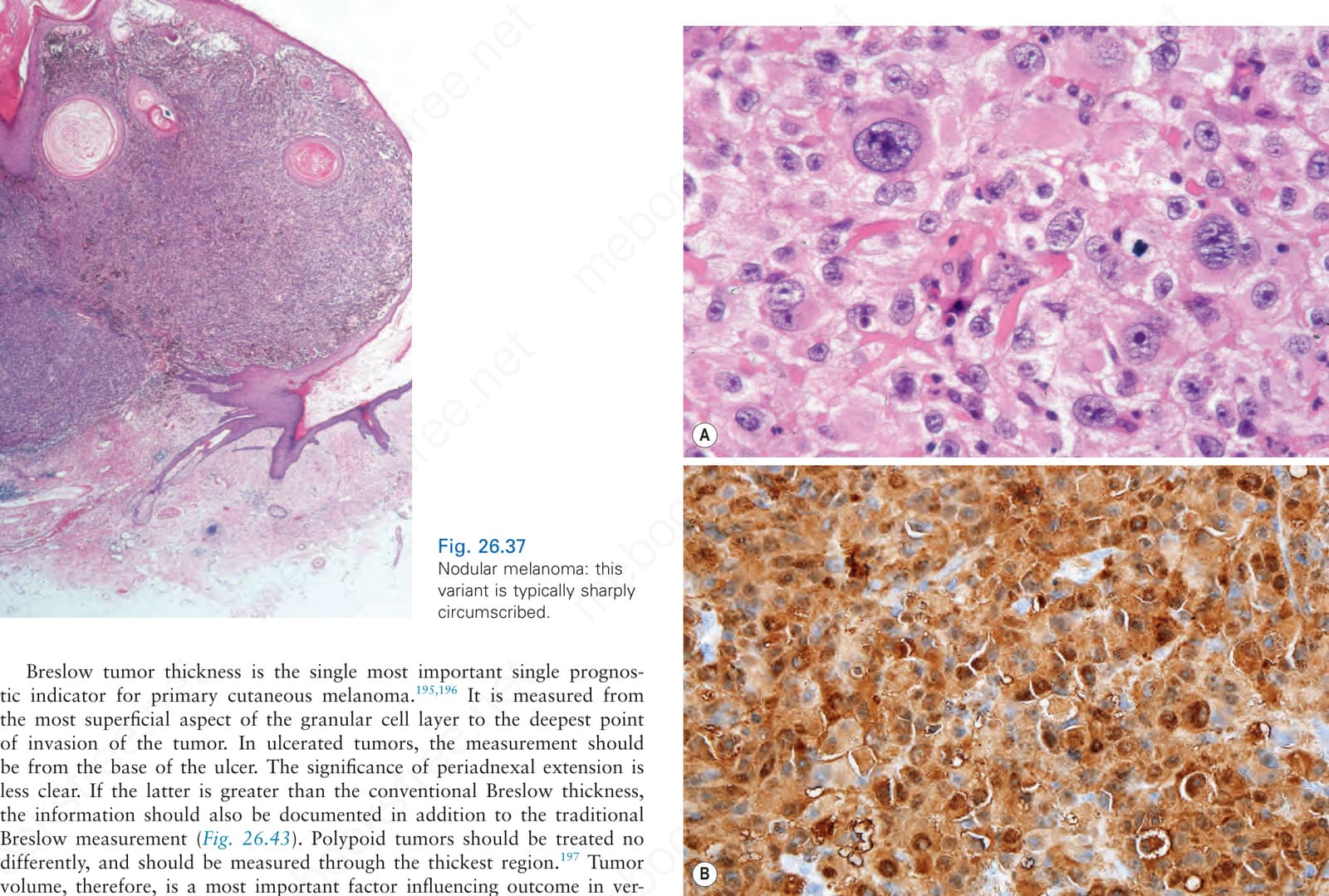
Fig. 26.37 Nodular melanoma: this variant is typically sharply circumscribed.
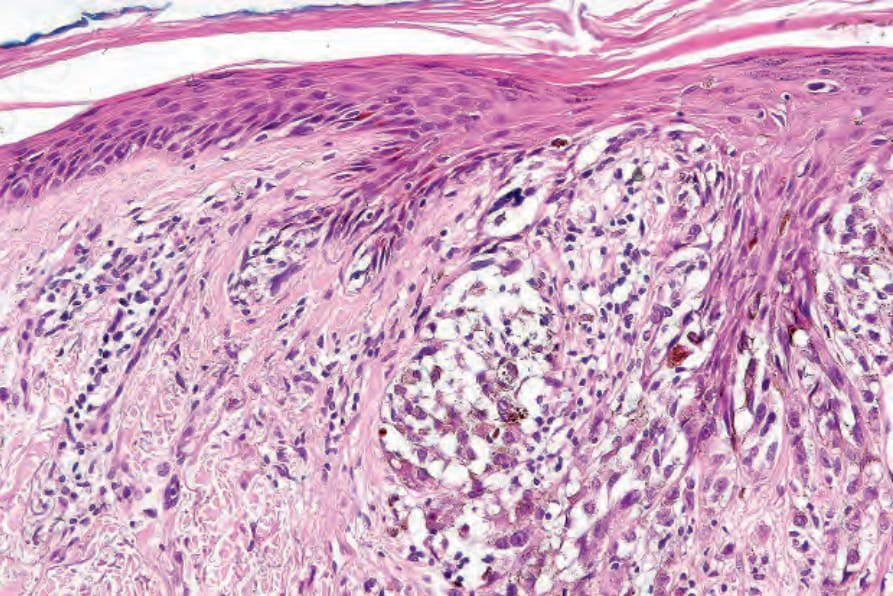
Fig. 26.38 Nodular melanoma: by definition, there is no melanocytic proliferative activity in the adjacent epidermis.
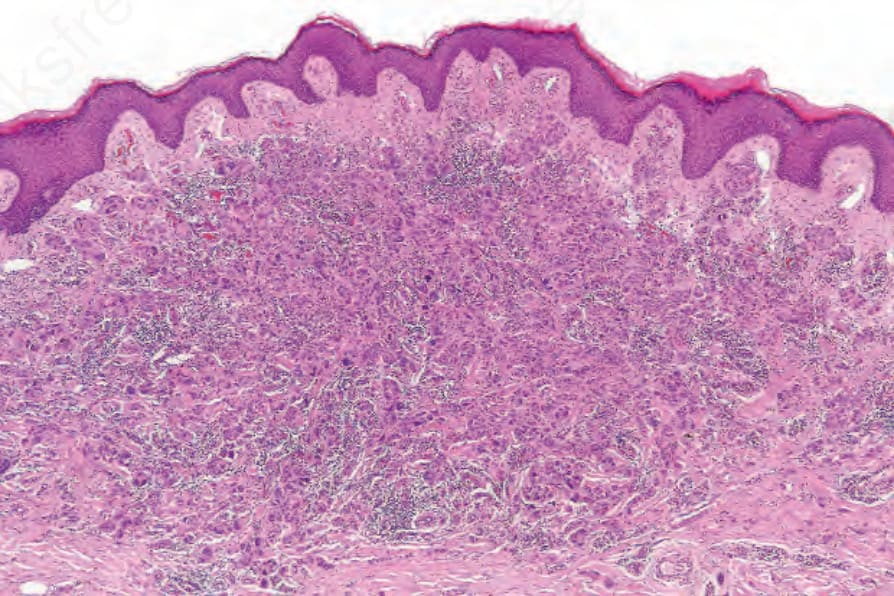
Fig. 26.40 Giant cell melanoma: within the dermis is a deposit of metastatic melanoma.
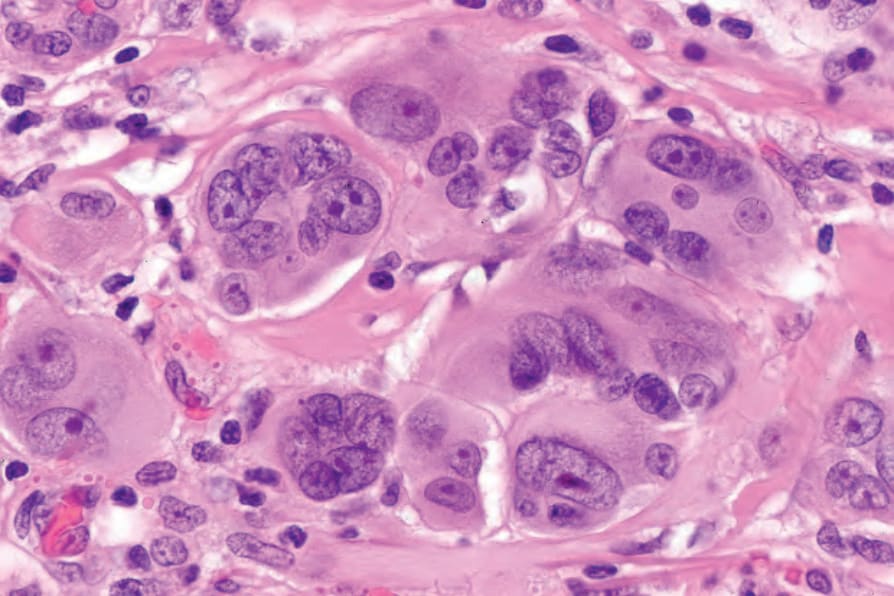
Fig. 26.41 Giant cell melanoma: the tumor cells are multinucleate and very pleomorphic with abundant cytoplasm and large vesicular nuclei containing prominent eosinophilic nucleoli.
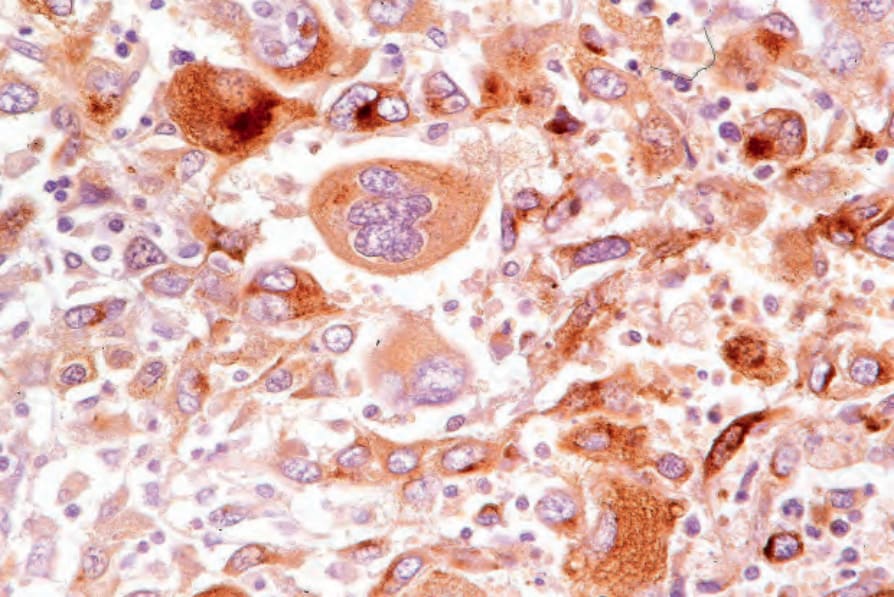
Fig. 26.42 Giant cell melanoma: the tumor cells are HMB-45 positive. The patient had a melanoma excised several years earlier.
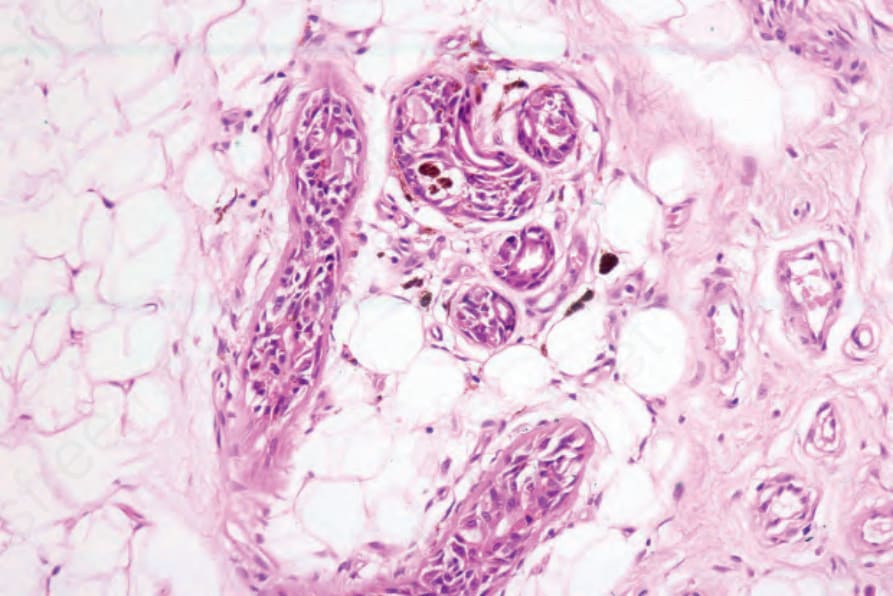
Fig. 26.43 Melanoma: periadnexal extension is of uncertain biological significance except that it is a potential source for recurrence of inadequately excised tumors. In this example, there is deep involvement of the eccrine sweat glands.
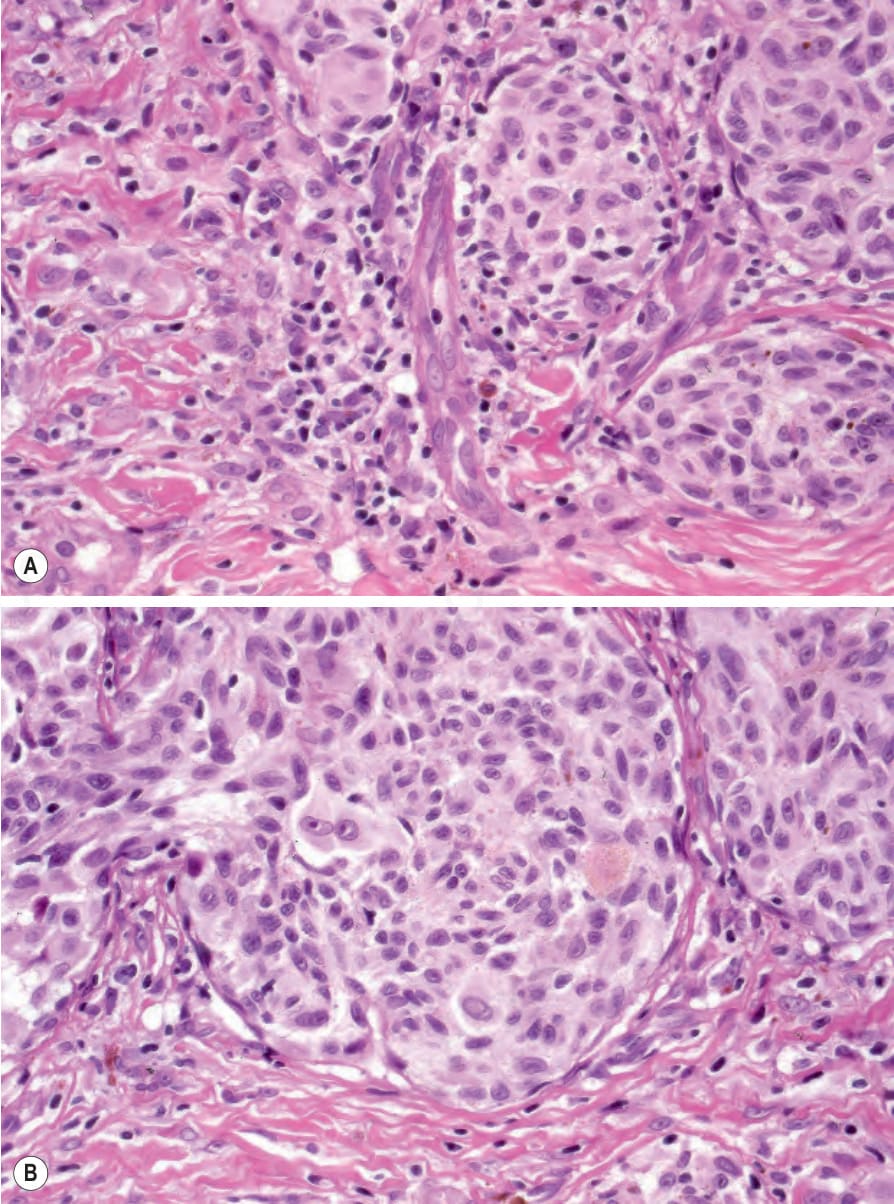
Fig. 26.45 (A, B) Melanoma: tumor infiltrating lymphocytes. Category B – Nonbrisk: the lymphocytes infiltrate only part of the tumor.
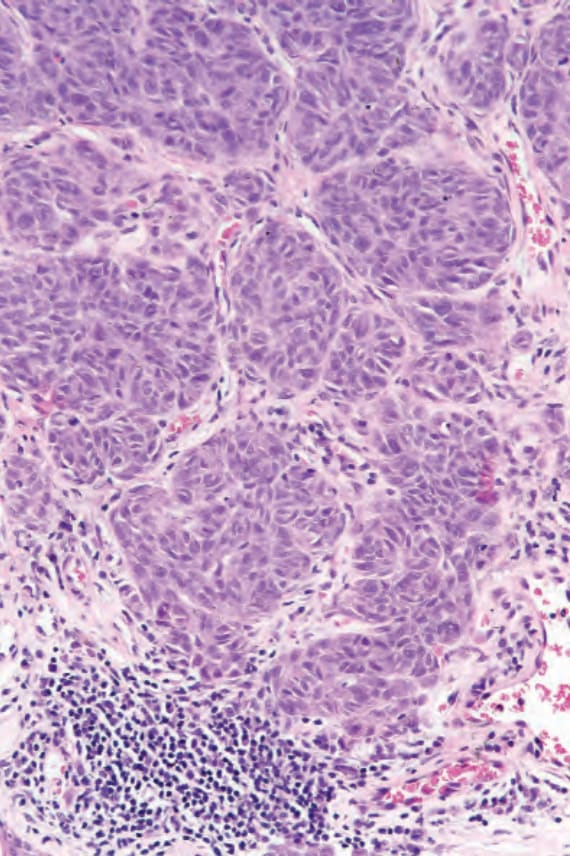
Fig. 26.46 Melanoma: tumor infiltrating lymphocytes. Category C – Absent: lymphocytes are present but they do not invade the tumor. The category also includes complete absence of lymphocytes.
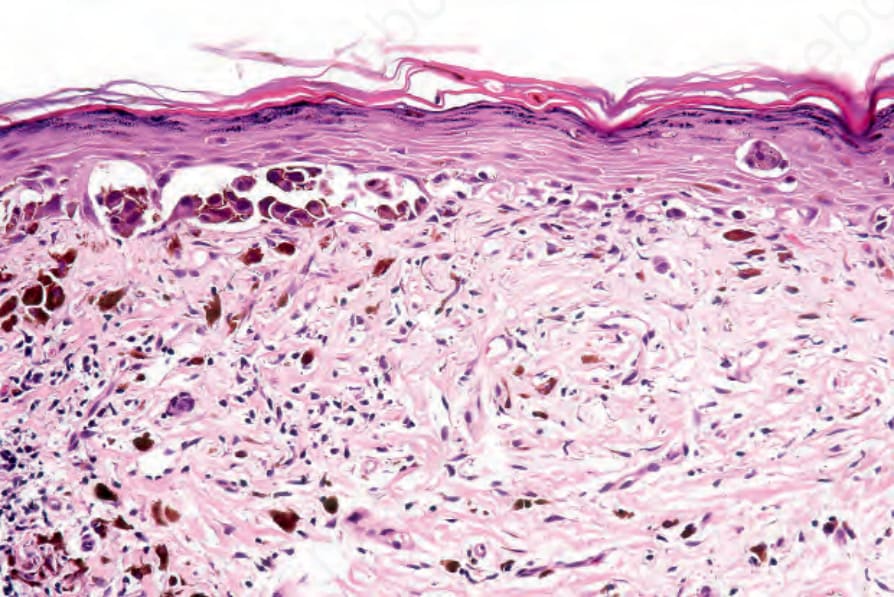
Fig. 26.48 Partial regression: in this variant, the junctional component is still present. Its significance is less certain.
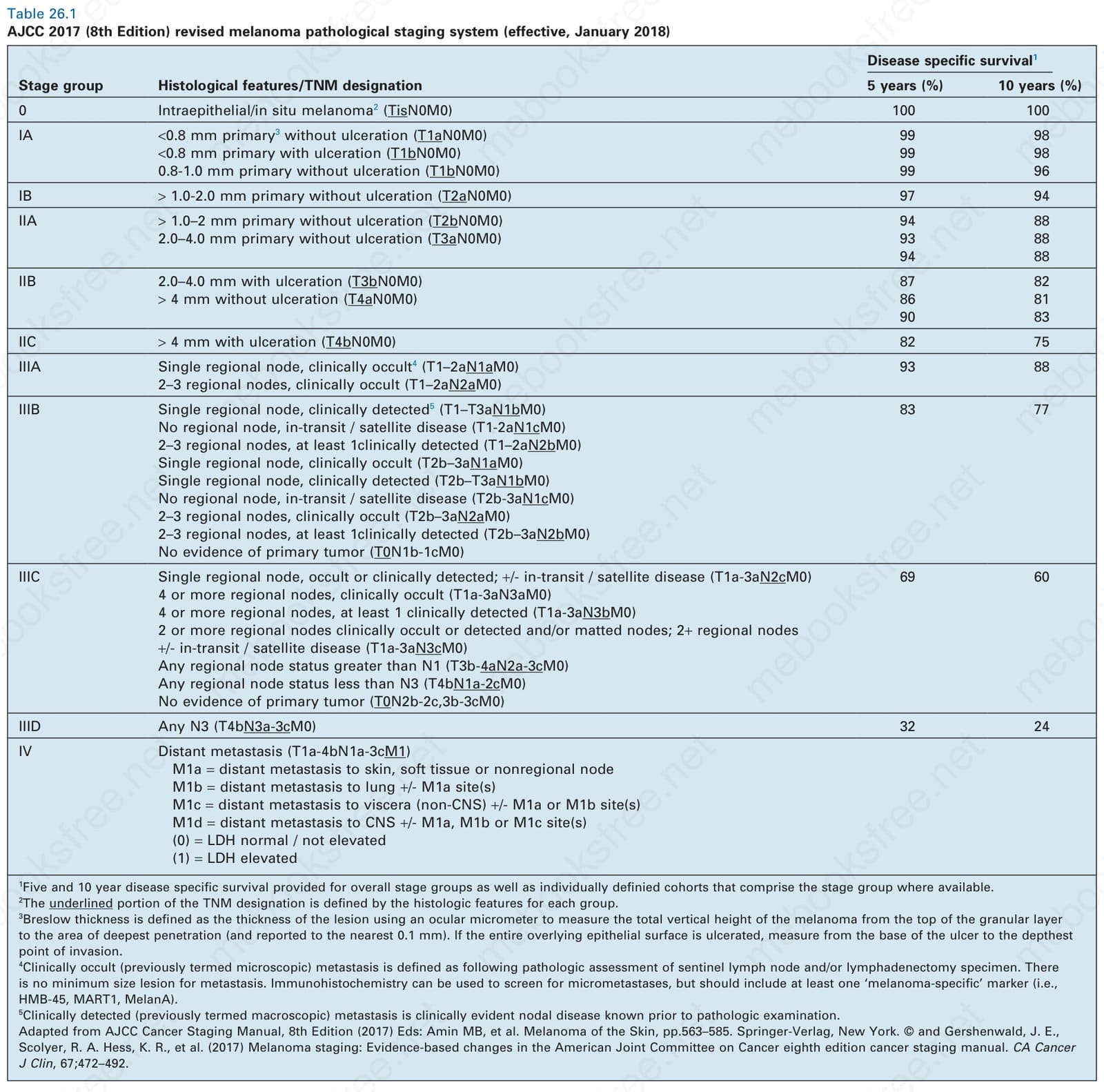
Table 26.1 AJCC 2017 (8th Edition) revised melanoma pathological staging system (effective, January 2018)
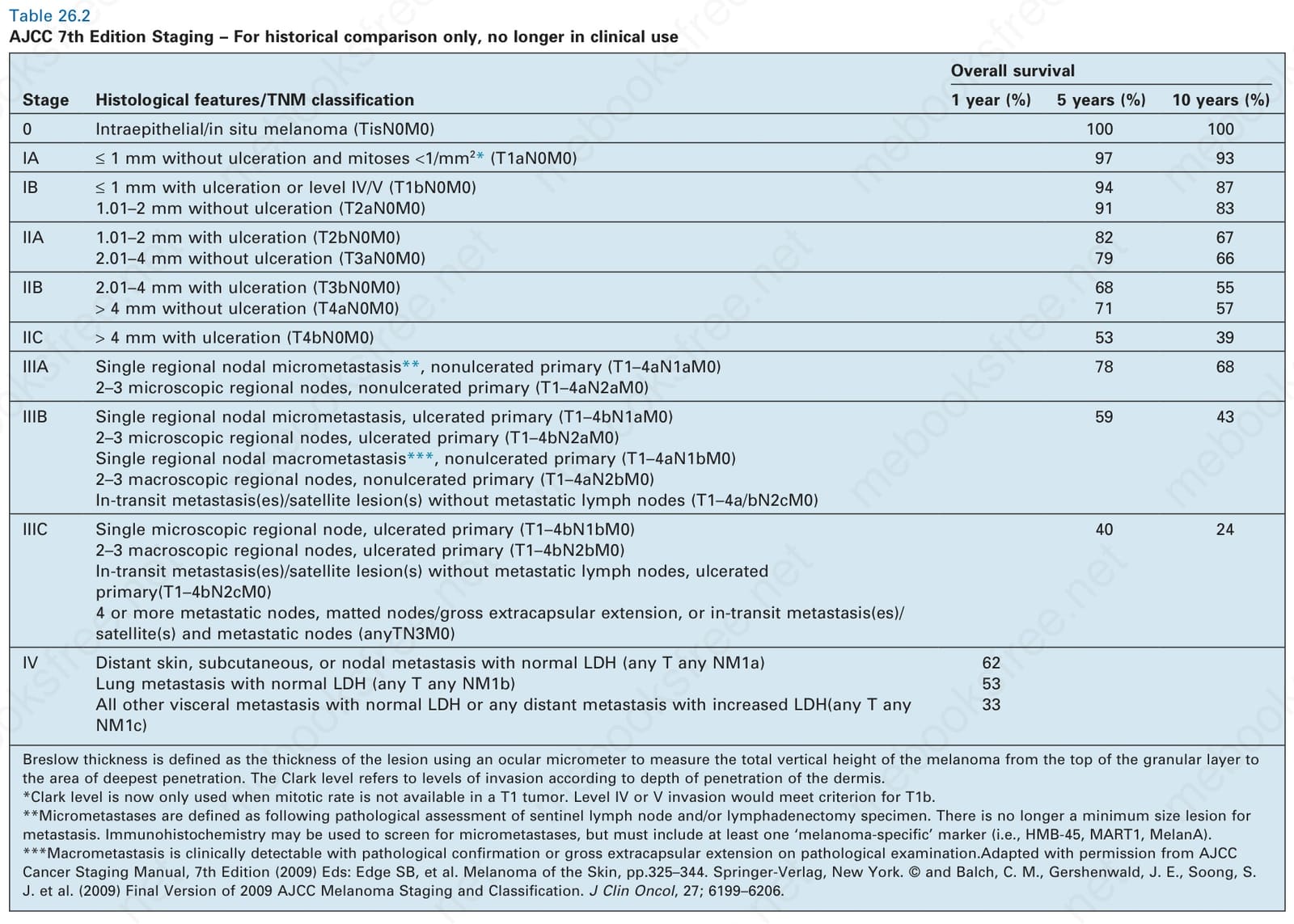
Table 26.2 AJCC 7th Edition Staging – For historical comparison only, no longer in clinical use
The presence or absence of ulceration and the width of the ulcer are independent prognostic indicators and should be recorded.175,211 Ulceration
is defined as ‘the absence of an intact epidermis overlying a major portion of the primary melanoma based on microscopic examination of the histologic sections’.203 Trauma and artifactual loss of the epidermis must be excluded. Ulceration is associated with a very significant increased risk of metastasis and was first included as a second determinant in the T classification in the AJCC 6th Edition and retained in the current 8th Edition.196,203,206,208,209,212
Tumor-infiltrating lymphocytes are an important independent prognostic variable and should be recorded as brisk, nonbrisk, or absent (Figs 26.44–26.46).145,206,213–215 The brisk category implies lymphocytes present throughout the whole vertical growth phase or extending across its entire base. Nonbrisk tumor infiltrating lymphocytes implies focal infiltration
1324 Melanoma
Overall survival
Stage Histological features/TNM classification 1 year (%) 5 years (%) 10 years (%)
0 Intraepithelial/in situ melanoma (TisN0M0) 100 100
IA ≤ 1 mm without ulceration and mitoses <1/mm2* (T1aN0M0) 97 93
IB ≤ 1 mm with ulceration or level IV/V (T1bN0M0) 94 87 1.01–2 mm without ulceration (T2aN0M0) 91 83
IIA 1.01–2 mm with ulceration (T2bN0M0) 82 67 2.01–4 mm without ulceration (T3aN0M0) 79 66
IIB 2.01–4 mm with ulceration (T3bN0M0) 68 55 > 4 mm without ulceration (T4aN0M0) 71 57
IIC > 4 mm with ulceration (T4bN0M0) 53 39
IIIA Single regional nodal micrometastasis**, nonulcerated primary (T1–4aN1aM0) 2–3 microscopic regional nodes, nonulcerated primary (T1–4aN2aM0)
78 68
IIIB Single regional nodal micrometastasis, ulcerated primary (T1–4bN1aM0) 2–3 microscopic regional nodes, ulcerated primary (T1–4bN2aM0) Single regional nodal macrometastasis***, nonulcerated primary (T1–4aN1bM0) 2–3 macroscopic regional nodes, nonulcerated primary (T1–4aN2bM0) In-transit metastasis(es)/satellite lesion(s) without metastatic lymph nodes (T1–4a/bN2cM0)
59 43
IIIC Single microscopic regional node, ulcerated primary (T1–4bN1bM0) 2–3 macroscopic regional nodes, ulcerated primary (T1–4bN2bM0) In-transit metastasis(es)/satellite lesion(s) without metastatic lymph nodes, ulcerated primary(T1–4bN2cM0) 4 or more metastatic nodes, matted nodes/gross extracapsular extension, or in-transit metastasis(es)/ satellite(s) and metastatic nodes (anyTN3M0)
40 24
IV Distant skin, subcutaneous, or nodal metastasis with normal LDH (any T any NM1a) 62 Lung metastasis with normal LDH (any T any NM1b) 53 All other visceral metastasis with normal LDH or any distant metastasis with increased LDH(any T any NM1c)
33
Breslow thickness is defined as the thickness of the lesion using an ocular micrometer to measure the total vertical height of the melanoma from the top of the granular layer to the area of deepest penetration. The Clark level refers to levels of invasion according to depth of penetration of the dermis. *Clark level is now only used when mitotic rate is not available in a T1 tumor. Level IV or V invasion would meet criterion for T1b. **Micrometastases are defined as following pathological assessment of sentinel lymph node and/or lymphadenectomy specimen. There is no longer a minimum size lesion for metastasis. Immunohistochemistry may be used to screen for micrometastases, but must include at least one ‘melanoma-specific’ marker (i.e., HMB-45, MART1, MelanA). ***Macrometastasis is clinically detectable with pathological confirmation or gross extracapsular extension on pathological examination.Adapted with permission from AJCC Cancer Staging Manual, 7th Edition (2009) Eds: Edge SB, et al. Melanoma of the Skin, pp.325–344. Springer-Verlag, New York. © and Balch, C. M., Gershenwald, J. E., Soong, S. J. et al. (2009) Final Version of 2009 AJCC Melanoma Staging and Classification. J Clin Oncol, 27; 6199–6206.
A
B
only. Absent includes two categories: either no lymphocytes at all or lymphocytes are present but do not infiltrate the melanoma. Brisk lymphocytic responses tend to be a feature of thin melanomas whereas absence of a lymphocytic response is generally seen in thick melanomas.200,214 In a study of 285 vertical growth phase tumors, the 10-year survival rates for brisk, nonbrisk, and absent tumor-infiltrating lymphocytes were 55%, 45%, and
27%, respectively.214 Recently, it has been suggested that tumor-infiltrating lymphocytes are influenced by sex and sentinel lymph node status only correlated in men and not in women.216 Not surprisingly, the absence of tumor-infiltrating lymphocytes also correlated with metastasis to sentinel lymph nodes as a surrogate marker of melanoma risk in a cohort of 887 patients with full multivariate analysis.215 Image analysis and feature
1325 Prognostic indicators
A
A
B
B
extraction have been used to assess tumor-infiltrating lymphocytes with salutary results.217 Assessing tumor-infiltrating lymphocytes in lymph node metastases also has predictive value.218,219
In thin melanoma it is important to recognize the features of regression, which may be particularly evident in the dermal component (Figs 26.47 and 26.48).145,220 These include absence or reduced numbers of malignant melanocytes, degenerate (apoptotic) forms, and a chronic inflammatory cell infiltrate (Fig. 26.49).221–223 Melanophages, horizontal scarring, isolated tumor islands, and telangiectatic vessels are also commonly present in the later stage. Clinically, regression presents as macular gray, white, or pink areas.
Although the importance of regression as a determinant of biological behavior has been the subject of considerable argument in the literature, a number of authors believe that, in thin tumors, it correlates with an impaired prognosis, though this contribution may be minor relative to other factors in many cases.223–232 Complete regression of an undiagnosed primary melanoma may be the explanation for patients presenting with metastatic tumor of unknown primary (Fig. 26.50).233 Some authors recommend sentinel node biopsy for thin melanomas if there is evidence of extensive (> 50%) regression, while other series do not show an association between regression and nodal status.176,234
Mitotic rate is determined by the number of mitotic figures/1 mm2 of tumor in the most mitotically active area. It has become clear that tumors displaying a high mitotic rate are associated with a poorer prognosis and that mitoses are a more robust predictor of outcome than ulceration and thus mitotic rate was incorporated into the 7th AJCC staging system.145,204,235–240 While mitoses are still recognized as a prognostic factor, the current 8th
1326 Melanoma
AJCC staging system relies on ulceration rather than mitoses due to stage group stability.196,206 Despite earlier contrary evidence and the complex interrelations of tumor thickness, ulceration, and mitotic rate, mitotic rate appears to carry prognostic information independent of both of the other factors.176,241,242
The presence of a microscopic satellite is defined by a distinct tumor nodule of any size at any distance discontinuous from the main primary tumor mass separated by normal tissue (no scarring, fibrosis or extensive inflammation).206 It is found in thicker tumors and is associated with an increased risk of local recurrence, regional lymph node metastases, and diminished survival.243–246 The presence of microsatellites results in upstaging to N1c if there is no regional lymph node involvement, and upstaging to N2c or N3c with one or more than one lymph nodes involved, respectively, in the 2017 AJCC melanoma staging system.206
number of studies.215,248–253 The use of immunohistochemistry for D2-40 significantly increases the sensitivity for detection of lymphatic invasion and also correlates with lymph node metastasis and survival.254–257 More study and a prospective trial is needed to validate the application and interpretation of the technique. Contrariwise, absence of vascular involvement in thick melanomas correlates with increased survival in a number of studies.258,259 Perineural and intraneural infiltration are most often encountered in desmoplastic variants, thereby accounting, in part, for the increased risk of local recurrence (Fig. 26.52). In this context, CD57 immunohistochemistry can be helpful in identifying residual nerve (Fig. 26.53).
The presence of lymphatic invasion correlates with the development of in-transit metastases (Fig. 26.51).247 Lymphovascular invasion has been shown to represent a predictor of diminished survival in melanoma in a
Angiogenesis, which is defined as the increasing development of new blood vessels at the base of the melanoma, parallels increases in tumor
B
A
1327 Differential diagnosis
A
B
thickness.260–265 Increasing angiogenesis therefore correlates with thick tumors, ulceration, relapse, and tumor-associated death.263,266 Perhaps related to the likelihood of lymphovascular invasion, increased intratumoral and peritumoral lymphangiogenesis as measured by D2-40 or VEGF-C also correlates with metastasis to sentinel lymph nodes and reduced disease-specific survival.267,268
Sentinel node biopsy also adds extremely valuable prognostic information.269–273 It has been shown to represent the most important factor in determining likelihood of tumor recurrence and patient survival in stage I and stage II disease.270 Completion lymph node dissection for positive sentinel lymph nodes is expected to become less common with the MSLT-II trial failing to show a survival benefit of the completion procedure.274,275 The latest AJCC staging system requires incorporation of sentinel lymph node data in cases where it would inform management, as this procedure significantly increases the accuracy and discriminatory power of the stage groups.204,206 Lymph nodes are bivalved or serially sectioned along their long axis and in addition to the examination of hematoxylin and eosin stained sections, immunohistochemistry – such as S100 protein, HMB-45, and/or MART-1 (melanoma antigen recognized by T cells 1) – should invariably be performed in those cases where the initial sections are negative. Detection of single or tiny groups of cells using an antibody against a ‘melanoma-specific’ antigen such as HMB-45 or MART1 is now incorporated into the AJCC staging system. More recently, molecular techniques including reverse transcriptase polymerase chain reaction for tyrosinase messenger RNA have been proposed.276,277 A major disadvantage of such procedures is the likelihood of false-positive results due to the common presence of banal capsular nevi, though the use of markers more specific to melanoma over nevus cells could potentially alleviate this problem.278
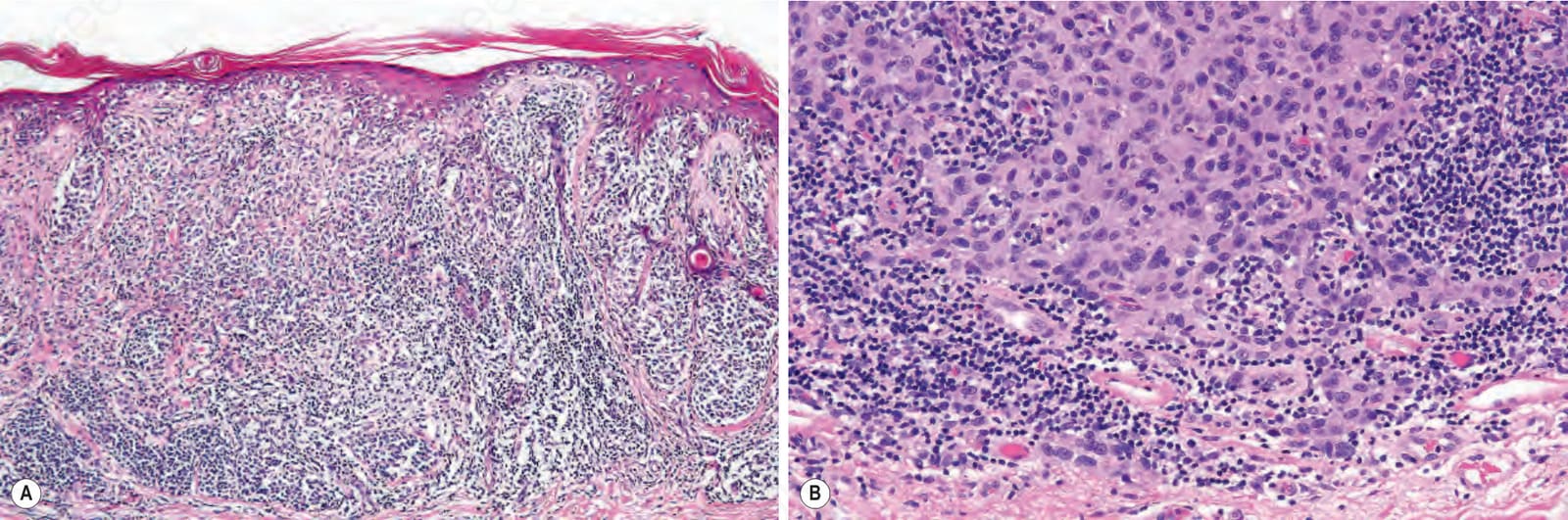
Fig. 26.44 (A, B) Melanoma: tumor infiltrating lymphocytes. Category A – Brisk: the lymphocytes infiltrate the tumor and extend along the whole of the base of the lesion.
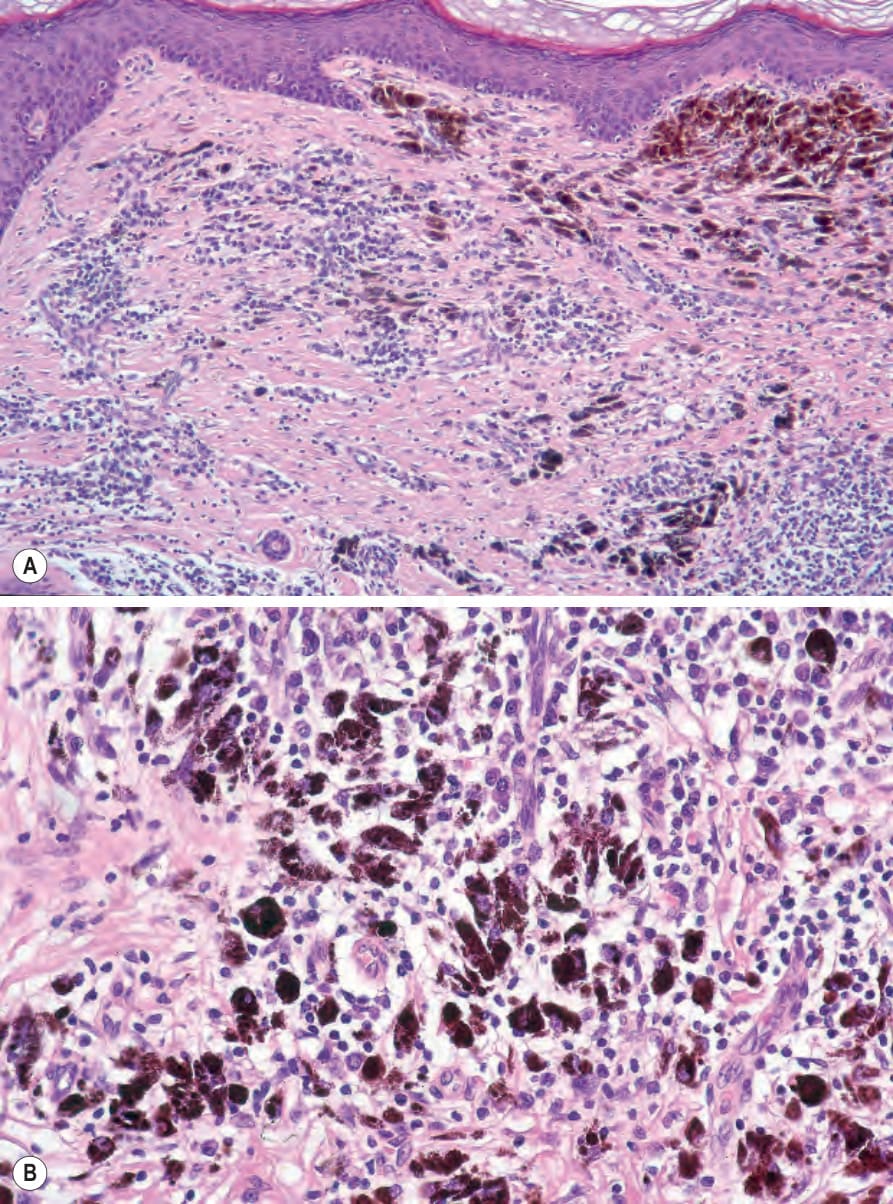
Fig. 26.47 (A, B) Regression: no residual epidermal component is present. Note the lymphocytic infiltrate, plasma cells, abundant melanin-containing macrophages, scarring, and conspicuous vasculature.
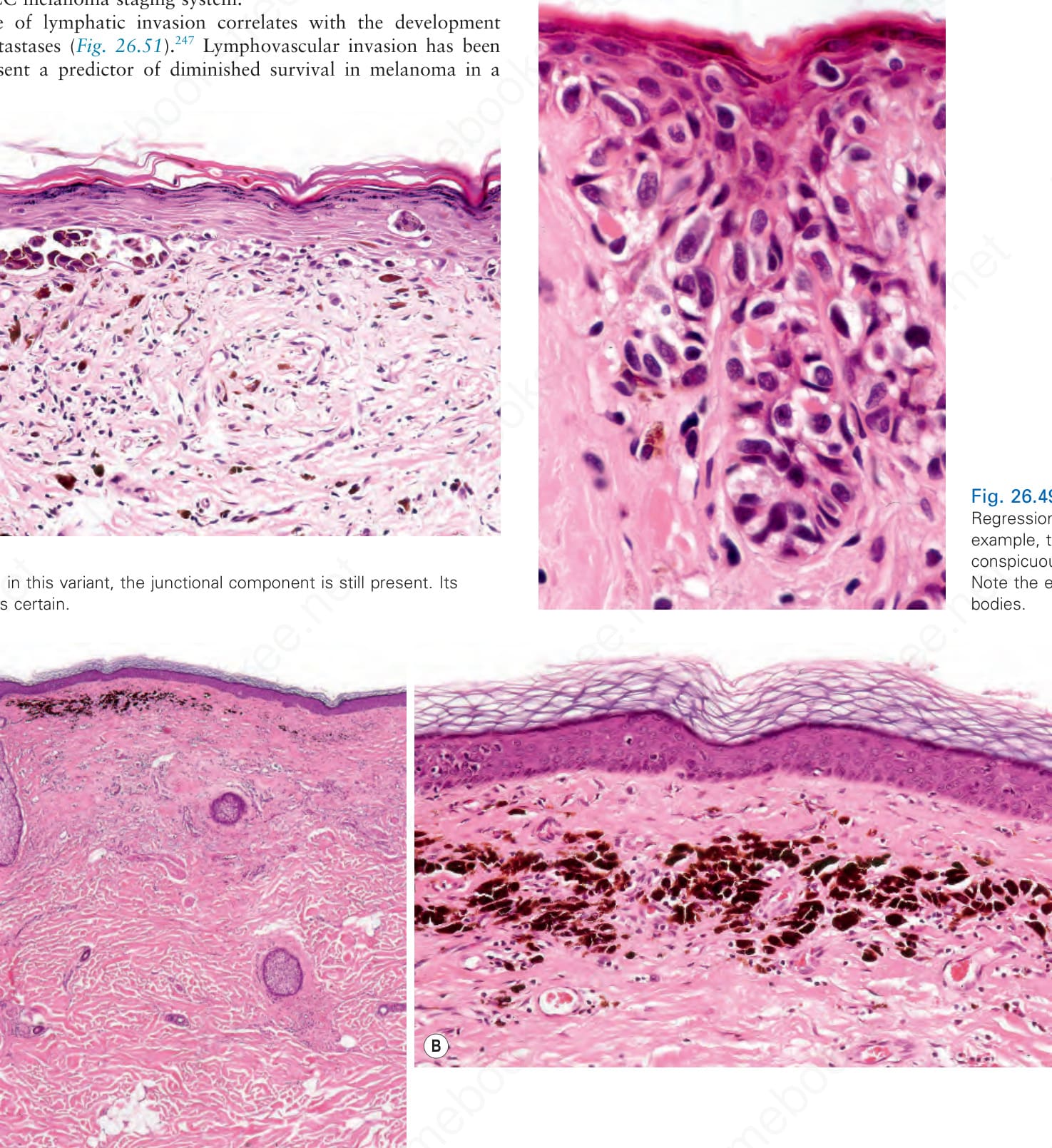
Fig. 26.49 Regression: in this example, there is conspicuous apoptosis. Note the eosinophilic bodies.
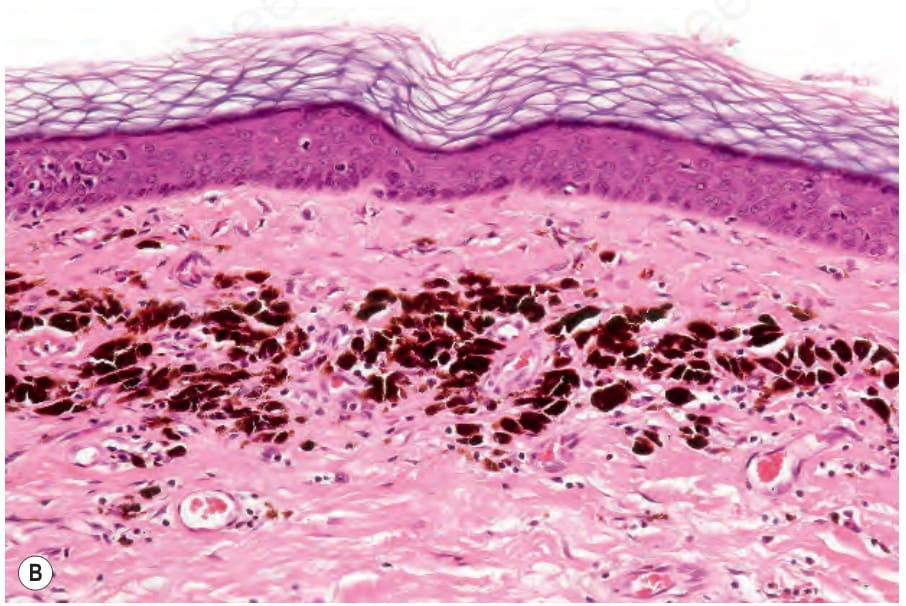
Fig. 26.50 (A, B) Regression: in this example, there is no residual tumor. The dermis is scarred and there is abundant melanin pigment. The patient presented with an unknown primary. By courtesy of M. Forder, MD, St Anne’s Medical Center, Pietermaritzburg, South Africa.
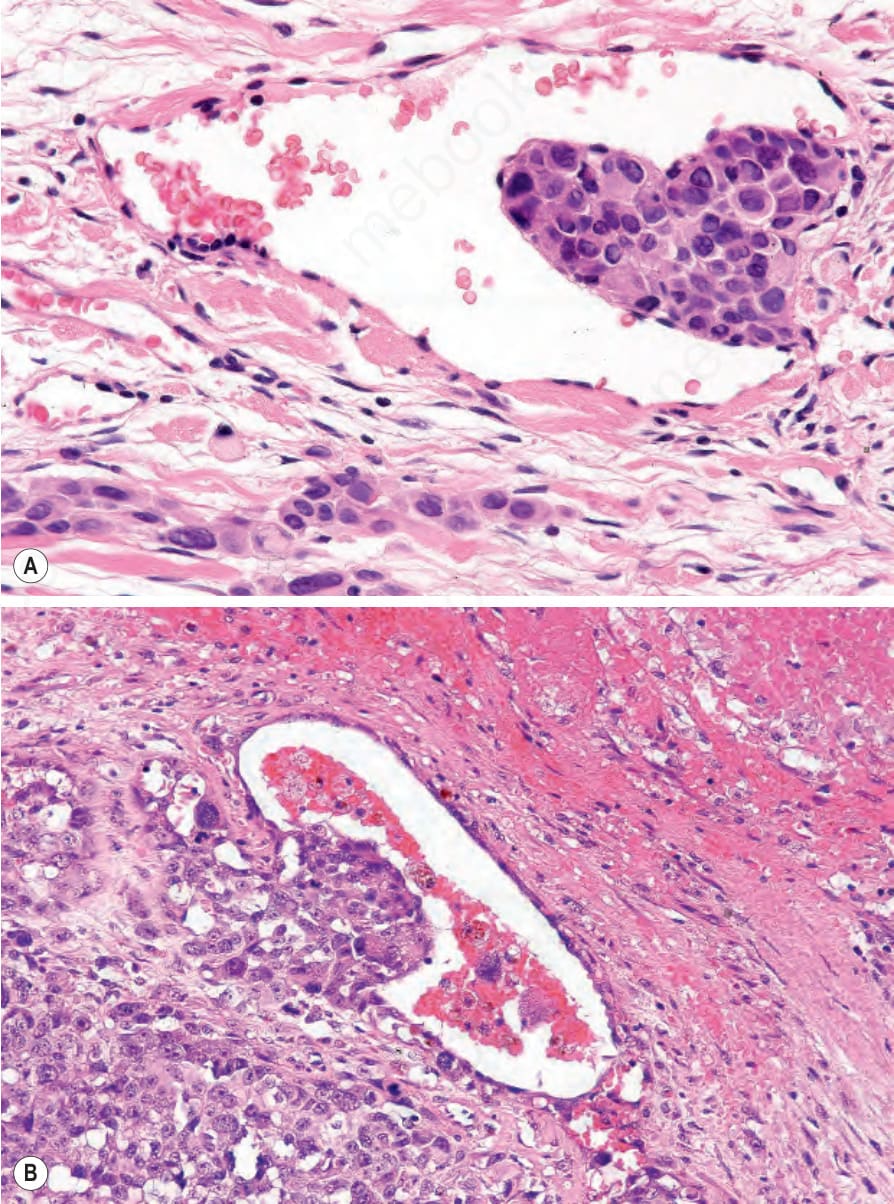
Fig. 26.51 Melanoma: vascular invasion: (A) pleomorphic tumor cells are adherent to the endothelium; (B) tumor cells are growing into the lumen.
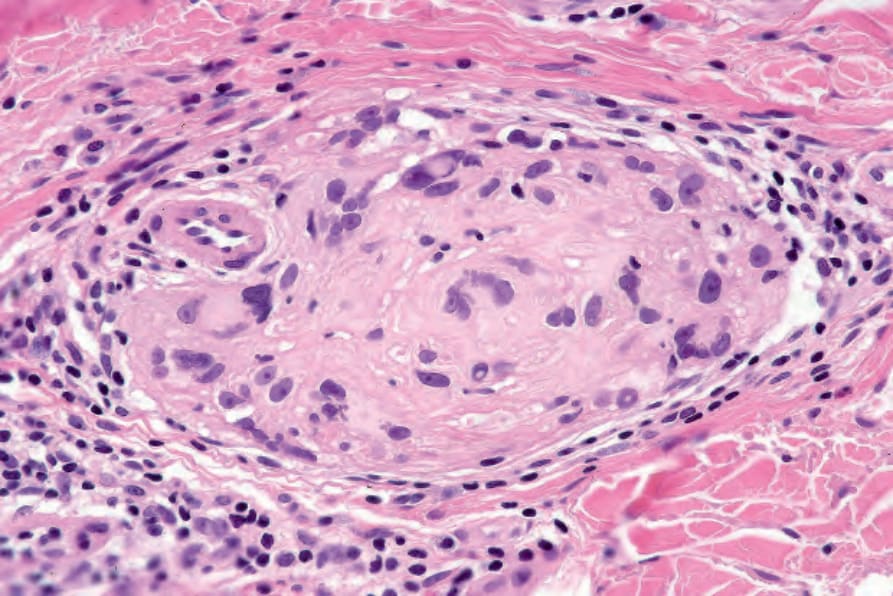
Fig. 26.52 Melanoma: intraneural invasion. Note the pleomorphic tumor nuclei within this nerve trunk.
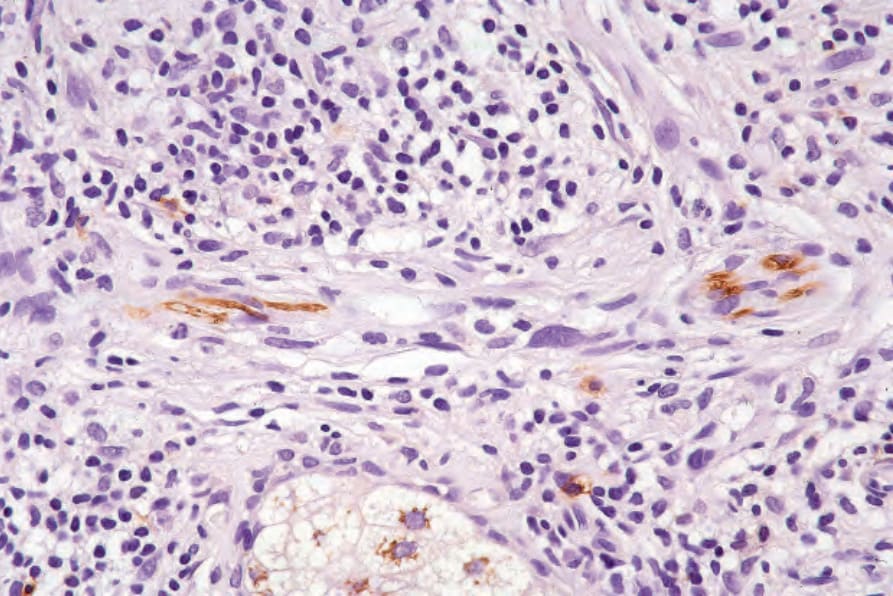
Fig. 26.53 Melanoma: CD57 immunohistochemistry may be particularly valuable when tumor growth has largely destroyed the nerve.
Sentinel node biopsy is currently recommended for all tumors measuring 1.00 mm or more in thickness. Other possible indications include ulcerated tumors, tumors with 50% or more regression, tumors having achieved the vertical growth phase, and those lesions which have been biopsied and involve the deep margin.176,272,279,280 The procedure should also be considered for tumors that are less than 1.00 mm thick but display conspicuous mitotic activity.281