惡性小痣與惡性小痣黑色素瘤 (Lentigo Maligna and Lentigo Maligna Melanoma)
惡性小痣 (lentigo maligna) 的特徵為非典型黑色素細胞 (atypical melanocytes) 的增生,主要位於真皮–表皮交界處 (dermal–epidermal junction)(圖 26.15 與 26.16)。慢性日光損傷 (chronic sun damage) 常表現為廣泛的日光性彈力纖維變性 (solar elastosis),且常相當顯著,尤其在來自頭頸部 (head and neck) 區域的病例。腫瘤細胞常顯示明顯的細胞質固定回縮假象 (cytoplasmic fixation retraction artifact),並含有多形性、不規則、深染、有時呈角狀的細胞核。這些細胞常呈垂直於表面的排列方向,而毛囊 (hair follicles) 與汗管上皮 (sweat duct epithelium) 的侵犯則是其特徵性發現(圖 26.17)。這有時會造成評估腫瘤厚度上的困難,尤其在檢視斜切切片 (obliquely cut sections) 時,腫瘤細胞與附屬器上皮 (adnexal epithelium) 之間的關係可能並不清楚。在較進展的病灶中,可見交界處巢狀結構 (junctional nests),且常可見多核腫瘤巨細胞 (multinucleate tumor giant cells)(圖 26.18–26.20)。色素沉著程度不一,但常相當豐富,有時侵犯表皮的全層,包括角質層 (stratum corneum)。極偶爾會出現明顯的表皮內 (pagetoid) 擴散,可能造成與表淺擴散性黑色素瘤 (superficial spreading melanoma) 在組織學上的重疊,不過 lentigo maligna 中的交界處巢狀結構通常較不顯著。在此變異型中評估切除邊緣是否殘留非典型黑色素細胞往往充滿困難。為避免不必要的手術,重要的是不要將日光損傷的細胞核 (actinically damaged nuclei) 與殘留的 lentigo maligna 混淆(圖 26.21),不過分子研究顯示,鑑於即使在型態正常的黑色素細胞中也存在基因組異常 (genomic aberration) 的場效應 (field effect),要純粹依型態學標準做出此鑑別可能並不可行。這很可能是這些病灶局部復發風險升高的根本原因。在困難病例或小檢體中評估表皮侵犯的範圍,可藉由免疫組織化學 (immunohistochemistry) 進行,最理想的是使用能凸顯細胞核的標記,包括 MITF 與 SOX10。
Lentigo maligna 發生於顯示日光損傷的部位;因此表皮通常呈萎縮 (atrophic),而真皮則顯示 solar elastosis。真皮乳頭層 (papillary dermis) 通常含有噬黑色素細胞 (melanophages) 與散在的慢性發炎細胞。後者的發現,尤其當數量眾多時,常與侵犯有關,因此應促使仔細檢查檢體的多個切面 (multiple levels)。侵襲性腫瘤(惡性小痣黑色素瘤,lentigo maligna melanoma)可為多病灶性 (multifocal),且通常為梭形細胞型 (spindled cell type)(圖 26.22–26.24)。由於對鄰近毛囊的廣泛侵犯及橫切面 (cross-sectioning) 的影響,判定是否存在早期侵犯可能非常困難,偶爾甚至不可能。促結締組織增生 (desmoplasia),常伴有親神經性 (neurotropism),存在於相當比例的病例中。極偶爾會出現編織狀 (storiform) 生長模式,若腫瘤為無色素性 (amelanotic),則可能與隆突性皮膚纖維肉瘤 (dermatofibrosarcoma protuberans) 混淆,尤其在小切片中(圖 26.25)。更常見的是,相關的黑色素瘤為促結締組織增生型 (desmoplastic),帶有不明顯的梭形細胞,可能被誤認為纖維化或瘢痕 (scar),而非侵襲性腫瘤。
極罕見地,lentigo maligna 與 lentigo maligna melanoma 在臨床與組織學上均表現為無色素性病灶(無色素性惡性小痣,amelanotic lentigo maligna,與無色素性惡性小痣黑色素瘤,amelanotic lentigo maligna melanoma)。臨床上,這些病灶表現為紅斑性、脫屑性病灶,類似日光性角化症 (actinic keratoses)、原位鱗狀細胞癌 (squamous cell carcinoma in situ) 或濕疹 (eczema)。因此可能需要免疫細胞化學 (immunocytochemistry) 才能得到正確診斷(圖 26.26)。
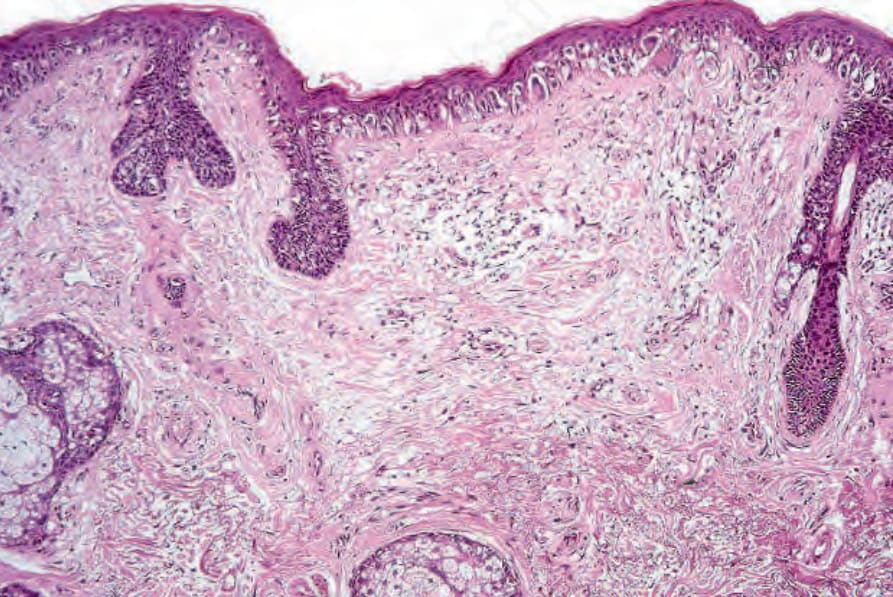
圖 26-15:惡性小痣 (lentigo maligna):表皮呈萎縮且扁平化。非典型黑色素細胞 (atypical melanocytes) 位於基底層,淺層真皮顯示明顯的日光性彈力纖維變性 (solar elastosis)。
Fig. 26.15 Lentigo maligna: the epidermis is atrophic and flattened. Atypical melanocytes are basally located and the superficial dermis shows marked solar elastosis.
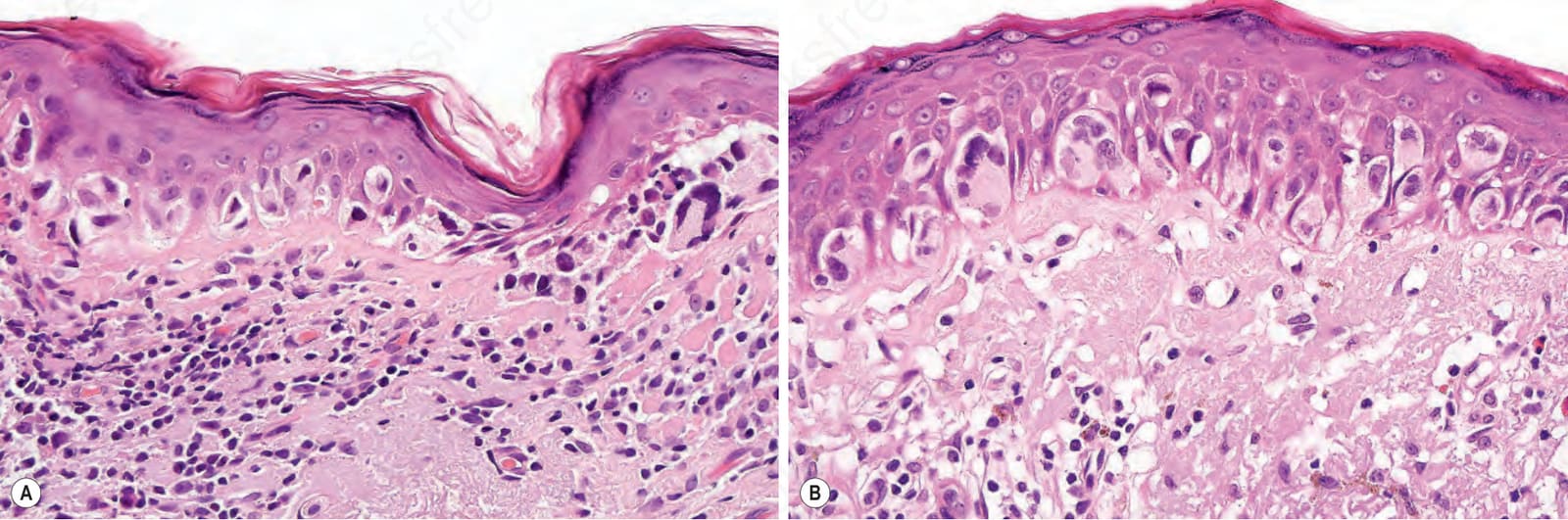
圖 26-16:惡性小痣 (lentigo maligna):(A) 高倍視野下,黑色素細胞顯示明顯的固定假象 (fixation artifact)。細胞核不規則、呈角狀且深染;(B) 在此例中,腫瘤細胞具有豐富的嗜伊紅性細胞質 (eosinophilic cytoplasm),並有早期的 pagetoid 擴散。
Fig. 26.16 Lentigo maligna: (A) viewed with higher power, the melanocytes demonstrate a prominent fixation artifact. The nuclei are irregular, angular, and hyperchromatic; (B) in this example, the tumor cells have abundant eosinophilic cytoplasm and there is early pagetoid spread.
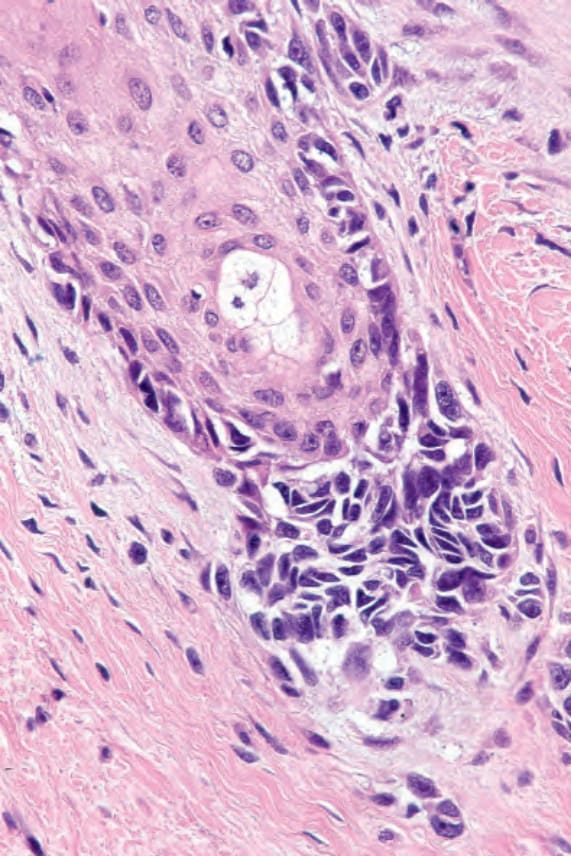
圖 26-17:惡性小痣 (lentigo maligna):注意毛囊外側部分內存在非典型黑色素細胞 (atypical melanocytes)。對此類病灶進行削除切片 (shave biopsy) 會伴隨高復發率。
Fig. 26.17 Lentigo maligna: note the presence of atypical melanocytes within the outer aspect of a hair follicle. Shave biopsy of such lesions is accompanied by a high recurrence rate.
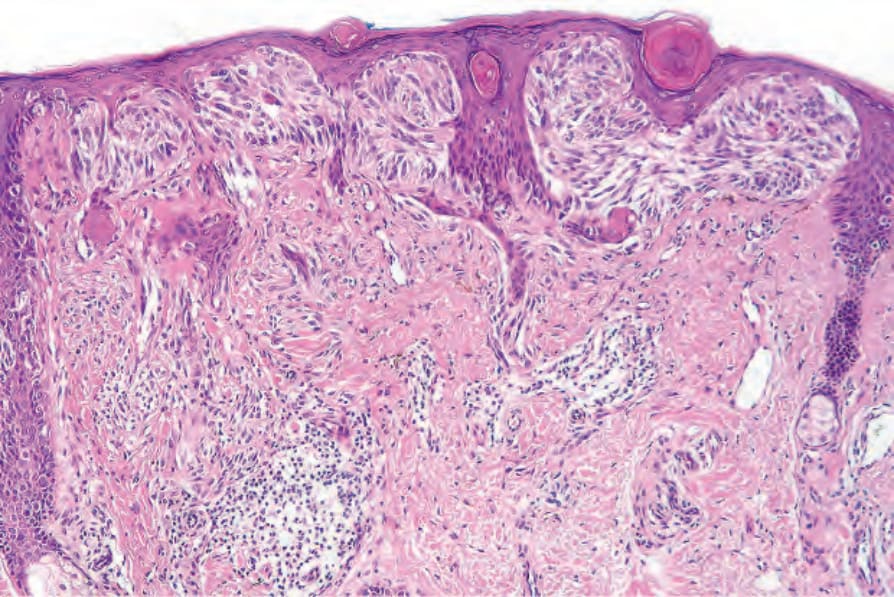
圖 26-18:惡性小痣 (lentigo maligna):在此例中有明顯的交界處巢狀結構 (junctional nests)。腫瘤細胞具有梭形 (spindled) 型態。
Fig. 26.18 Lentigo maligna: in this example there are conspicuous junctional nests. The tumor cells have a spindled morphology.
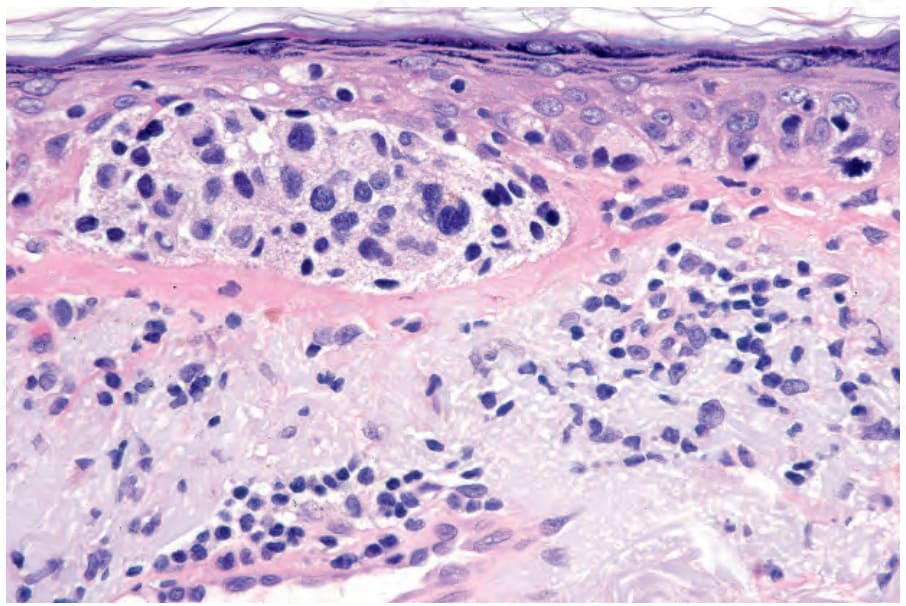
圖 26-19:惡性小痣 (lentigo maligna):腫瘤細胞呈多形性 (pleomorphic) 並顯示非常明顯的核深染 (nuclear hyperchromatism)。
Fig. 26.19 Lentigo maligna: the tumor cells are pleomorphic and show very marked nuclear hyperchromatism.
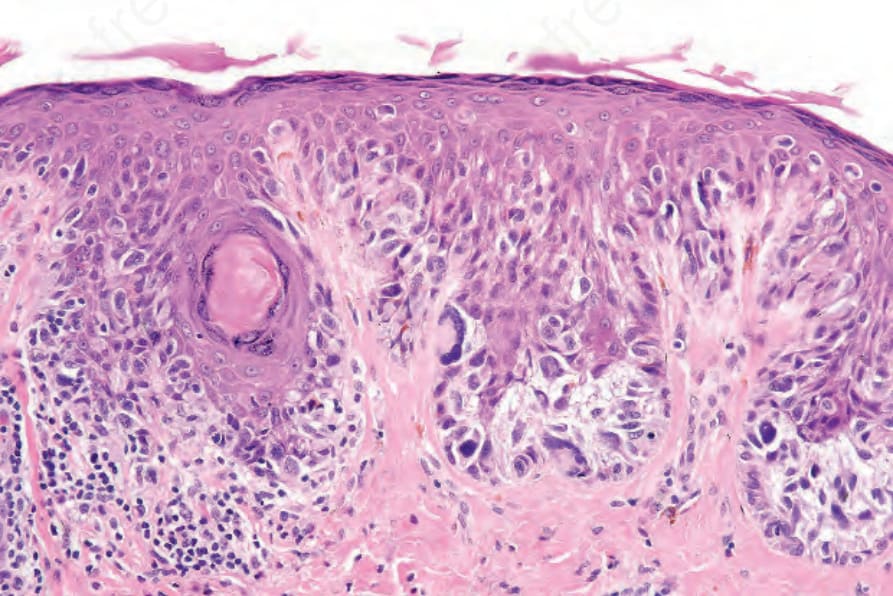
圖 26-20:惡性小痣 (lentigo maligna):如本例所示的多核腫瘤細胞 (multinucleate tumor cells) 是常見特徵,也是有用的診斷線索。
Fig. 26.20 Lentigo maligna: multinucleate tumor cells as shown in this example are a common feature and a useful diagnostic clue.
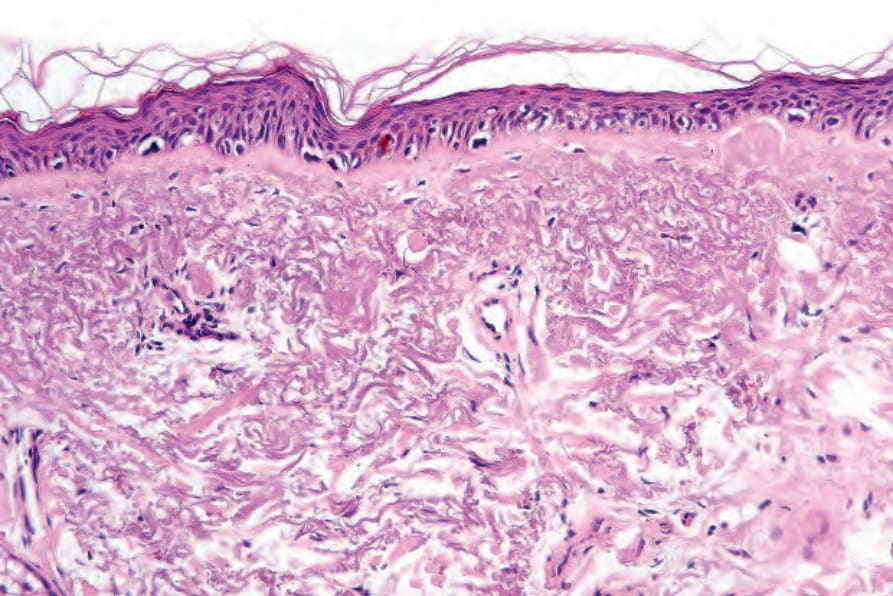
圖 26-21:日光性核非典型 (actinic nuclear atypia):有時要區分前者與如本視野所示的殘留腫瘤細胞可能是個真正的難題。然而前者顯示細胞核很少增大,且缺乏核仁 (nucleoli)。此外,這些細胞不會形成如 lentigo maligna 典型的核柵欄狀排列 (nuclear palisades)。
Fig. 26.21 Actinic nuclear atypia: sometimes distinguishing between the former and residual tumor cells as shown in this field can be a real problem. The former, however, show little nuclear enlargement and nucleoli are absent. In addition, such cells do not form nuclear palisades as is typical of lentigo maligna.
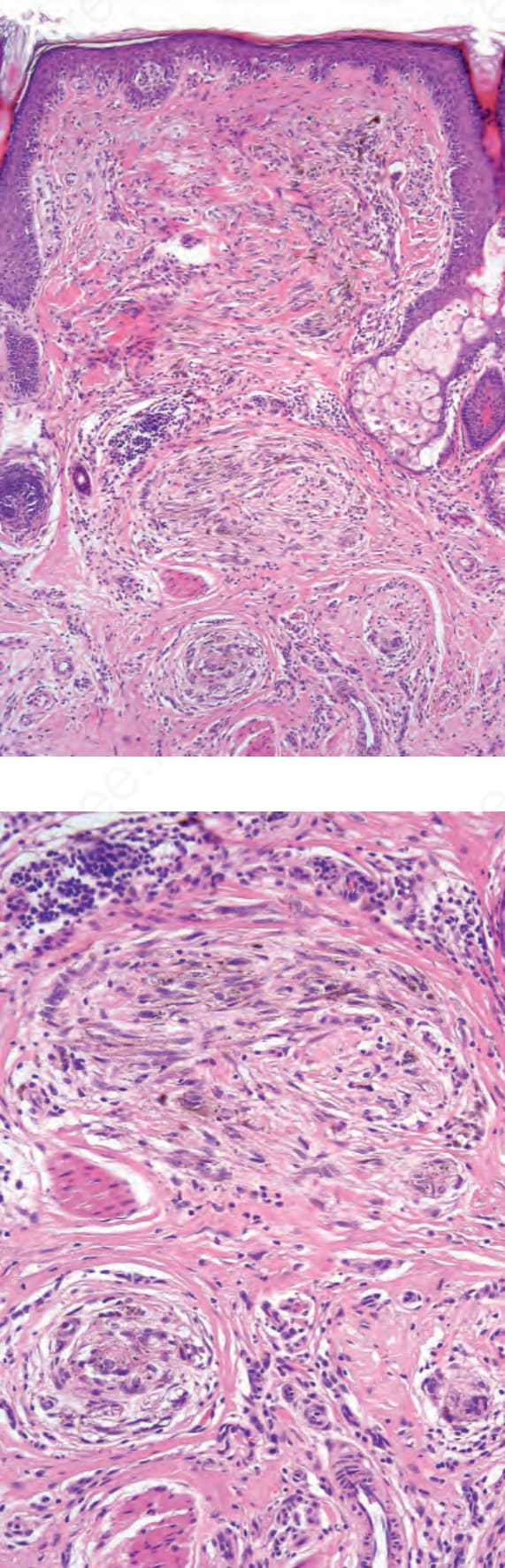
圖 26-22:惡性小痣黑色素瘤 (lentigo maligna melanoma):在此黑色素瘤變異型中,侵襲性成分常為梭形細胞型 (spindle cell type)。
Fig. 26.22 Lentigo maligna melanoma: in this variant of melanoma, the invasive component is often of the spindle cell type.
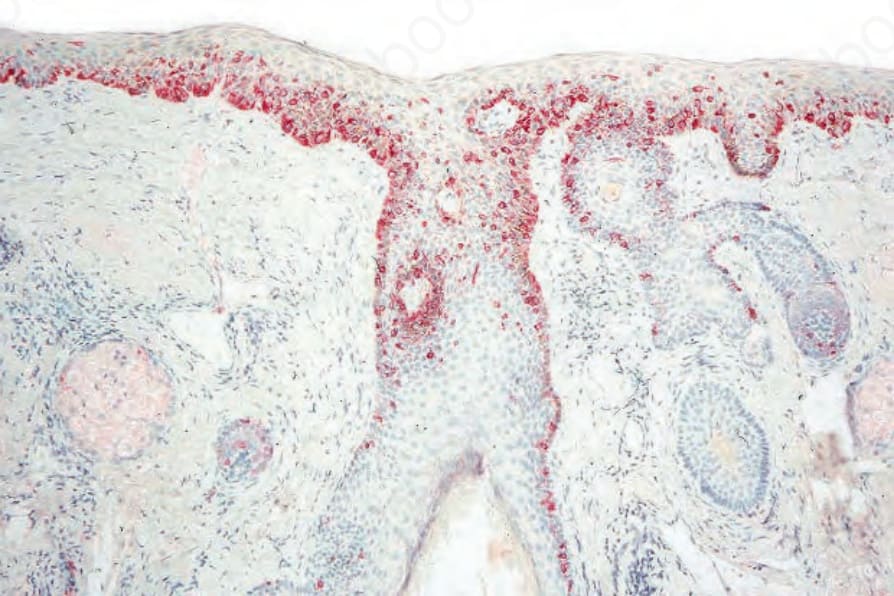
圖 26-25:惡性小痣黑色素瘤 (lentigo maligna melanoma):偶爾腫瘤呈現編織狀模式 (storiform pattern)。當為無色素性 (amelanotic) 時,可能與隆突性皮膚纖維肉瘤 (dermatofibrosarcoma protuberans) 或梭形細胞鱗狀細胞癌 (spindle cell squamous carcinoma) 混淆。
Fig. 26.25 Lentigo maligna melanoma: occasionally the tumor adopts a storiform pattern. When amelanotic, this may be confused with dermatofibrosarcoma protuberans or spindle cell squamous carcinoma.
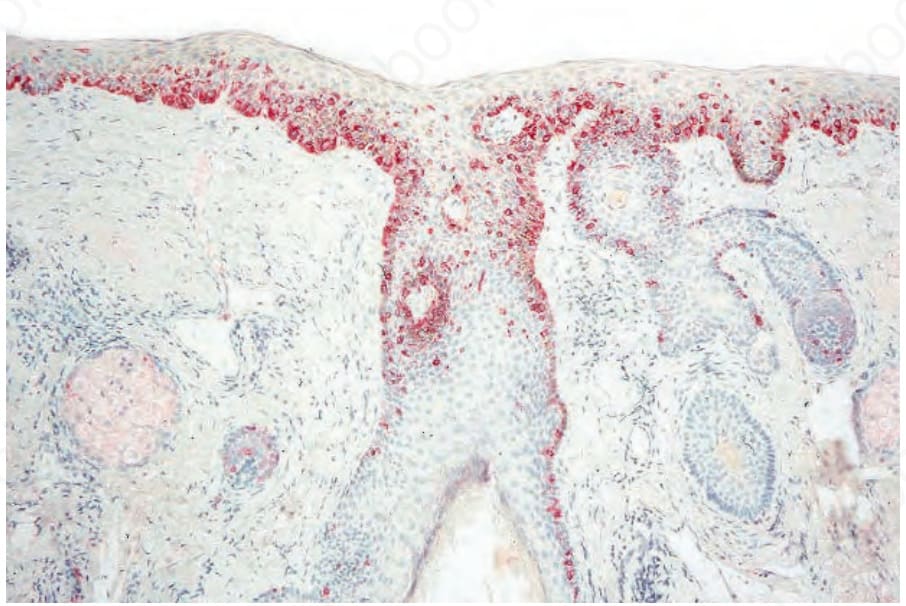
圖 26-26:惡性小痣 (lentigo maligna):偶爾難以區分日光性角化症 (actinic keratosis) 與 lentigo maligna。在此類病例中,使用紅色顯色劑 (red chromogen)(此例為鹼性磷酸酶,alkaline phosphatase)的免疫組織化學可使鑑別變得容易。
Fig. 26.26 Lentigo maligna: occasionally it is difficult to distinguish between actinic keratosis and lentigo maligna. In such cases, immunohistochemistry using a red chromogen (in this case alkaline phosphatase) can make the distinction easy.