Lentigo maligna and lentigo maligna melanoma
Lentigo maligna and lentigo maligna melanoma
Lentigo maligna is characterized by proliferation of atypical melanocytes predominantly located along the dermal–epidermal junction (Figs 26.15 and 26.16).158 Chronic sun damage evidenced as extensive solar elastosis is often prominent, particularly in cases from the head and neck region.159 The tumor cells often show a conspicuous cytoplasmic fixation retraction artifact and contain pleomorphic irregular hyperchromatic, sometimes angular, nuclei. The cells are frequently orientated perpendicular to the surface, and involvement of hair follicles and sweat duct epithelium is a characteristic finding (Fig. 26.17). This may sometimes result in difficulties in assessing
tumor thickness, particularly if obliquely cut sections are examined, when the relationship of the tumor cells to the adnexal epithelium may not be clear. In more advanced lesions, junctional nests are apparent and multinucleate tumor giant cells are commonly seen (Figs 26.18–26.20). Pigmentation is variable, but is often abundant, sometimes involving the full thickness of the epidermis, including the stratum corneum. The very occasional presence of marked intraepidermal (pagetoid) spread may result in histologic overlap with superficial spreading melanoma, though junctional nesting is usually less prominent in lentigo maligna. Assessing excision margins for residual atypical melanocytes in this variant is often fraught with difficulty. To avoid unnecessary surgery it is important not to confuse actinically damaged nuclei from residual lentigo maligna (Fig. 26.21), though molecular studies suggest that this may not be possible on strictly morphological grounds given the field effect of genomic aberration present in even morphologically normal melanocytes.160 This likely underlies the elevated risk of local recurrence in
1316 Melanoma
A
B
these lesions. Evaluation of the extent of epidermal involvement in difficult cases or small samples can be done by immunohistochemistry ideally with markers that highlight nuclei including MITF and SOX10.
Lentigo maligna arises at sites showing actinic damage; the epidermis is therefore typically atrophic and the dermis shows solar elastosis. Usually the papillary dermis contains melanophages and scattered chronic inflammatory cells. The finding of the latter, particularly when present in large numbers, is often associated with invasion and should therefore prompt careful examination of multiple levels of the specimen. Invasive tumor (lentigo maligna melanoma) can be multifocal and is usually of the spindled cell type (Figs 26.22–26.24). Due to the extensive involvement of neighboring hair follicles and cross-sectioning, determining the presence or absence of early invasion can be very challenging and occasionally, impossible. Desmoplasia, often with neurotropism, is present in a significant percentage of cases. Very occasionally, a storiform growth pattern is evident and if the tumor is amelanotic there may be confusion with dermatofibrosarcoma protuberans, particularly
1317 Histologic features
in small biopsies (Fig. 26.25). More often, the associated melanoma is desmoplastic with subtle spindle cells and can be mistaken for fibrosis or scar rather than invasive tumor.
Exceptionally, lentigo maligna and lentigo maligna melanoma present as amelanotic lesions (amelanotic lentigo maligna and amelanotic lentigo maligna melanoma), both clinically and histologically.161–164 Clinically, these appear as erythematous scaly lesions resembling actinic keratoses, squamous cell carcinoma in situ or eczema.162 Immunocytochemistry may therefore be necessary to arrive at the correct diagnosis (Fig. 26.26).165
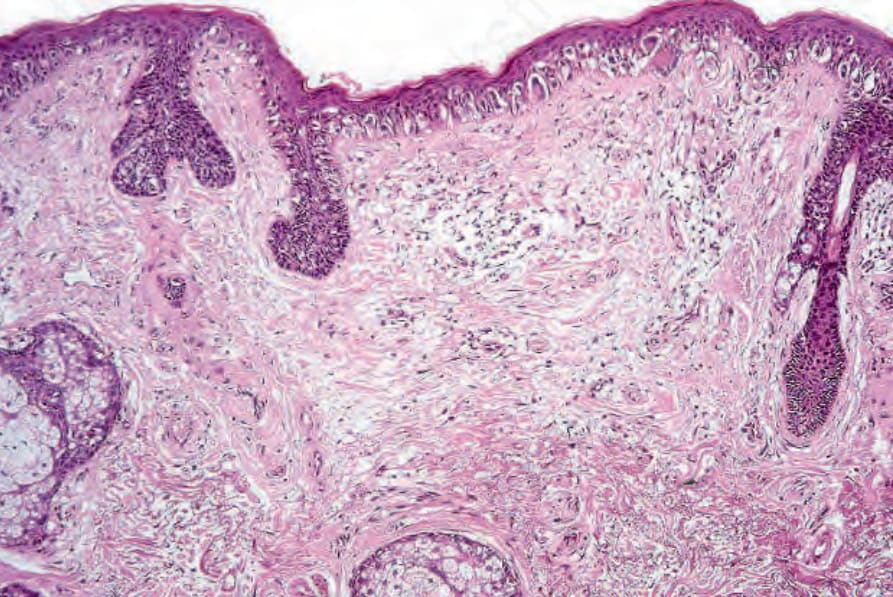
Fig. 26.15 Lentigo maligna: the epidermis is atrophic and flattened. Atypical melanocytes are basally located and the superficial dermis shows marked solar elastosis.
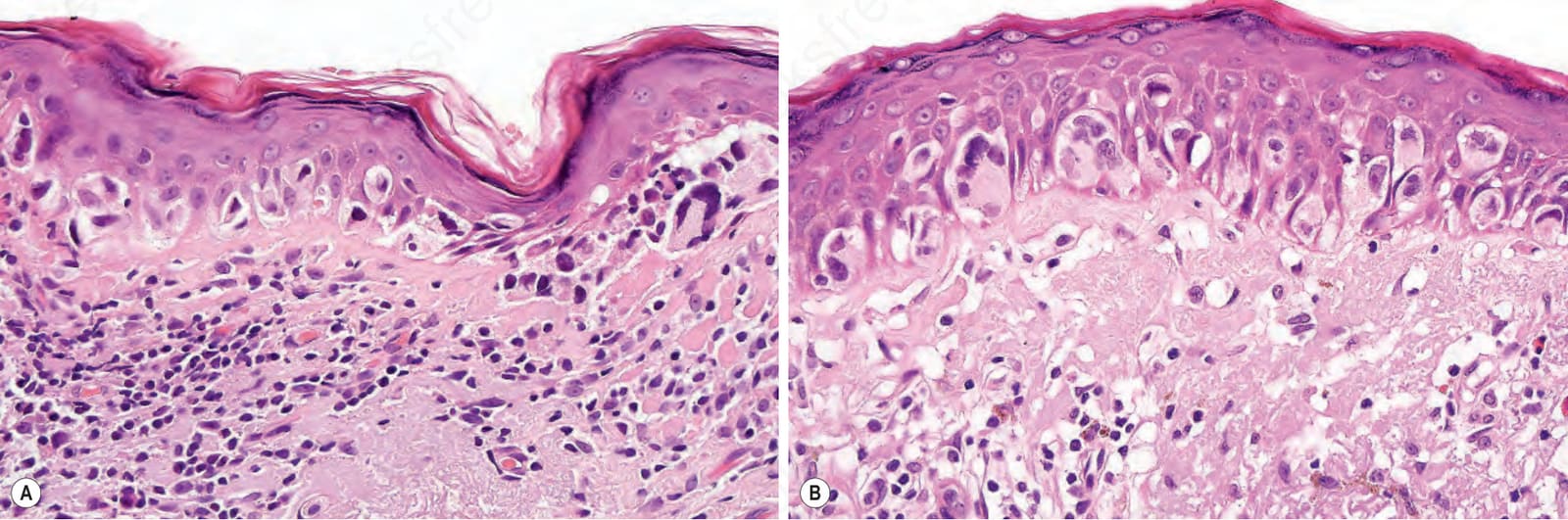
Fig. 26.16 Lentigo maligna: (A) viewed with higher power, the melanocytes demonstrate a prominent fixation artifact. The nuclei are irregular, angular, and hyperchromatic; (B) in this example, the tumor cells have abundant eosinophilic cytoplasm and there is early pagetoid spread.
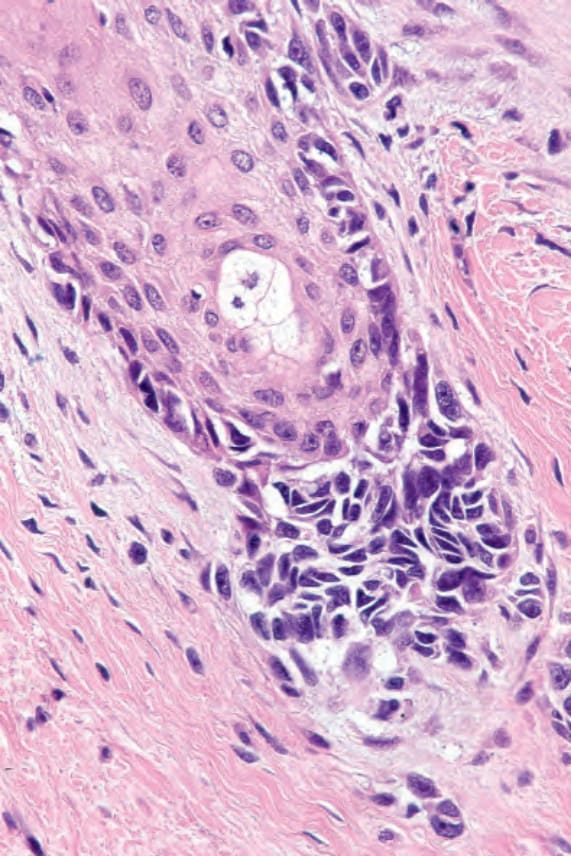
Fig. 26.17 Lentigo maligna: note the presence of atypical melanocytes within the outer aspect of a hair follicle. Shave biopsy of such lesions is accompanied by a high recurrence rate.
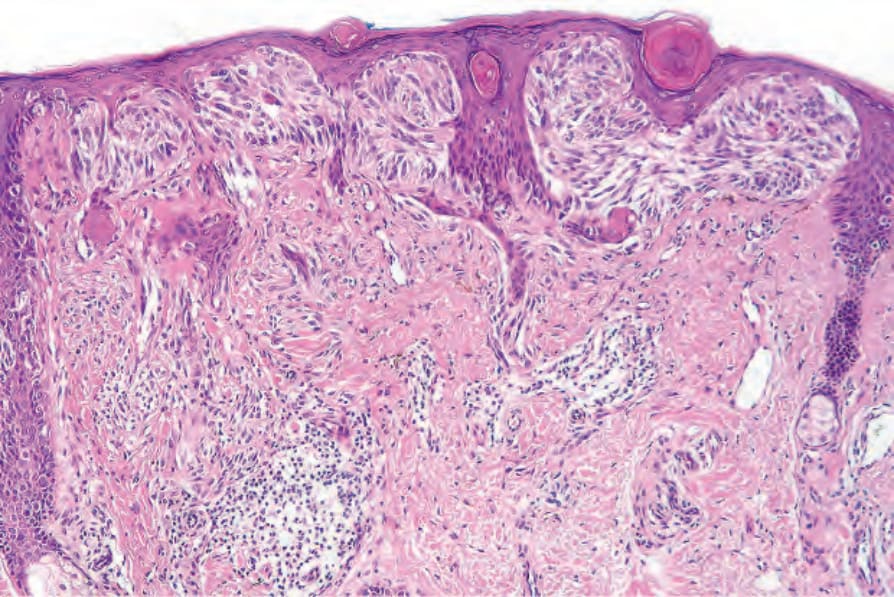
Fig. 26.18 Lentigo maligna: in this example there are conspicuous junctional nests. The tumor cells have a spindled morphology.
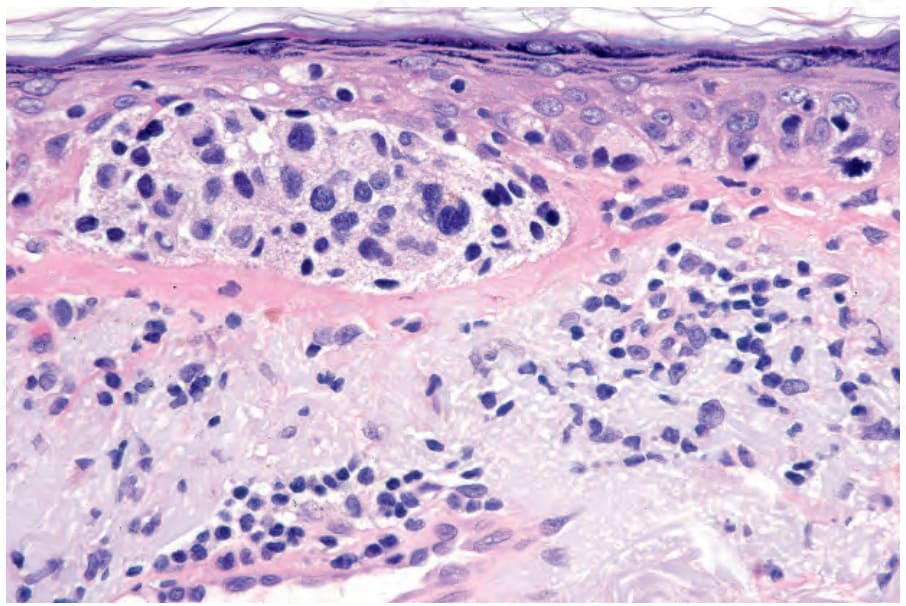
Fig. 26.19 Lentigo maligna: the tumor cells are pleomorphic and show very marked nuclear hyperchromatism.
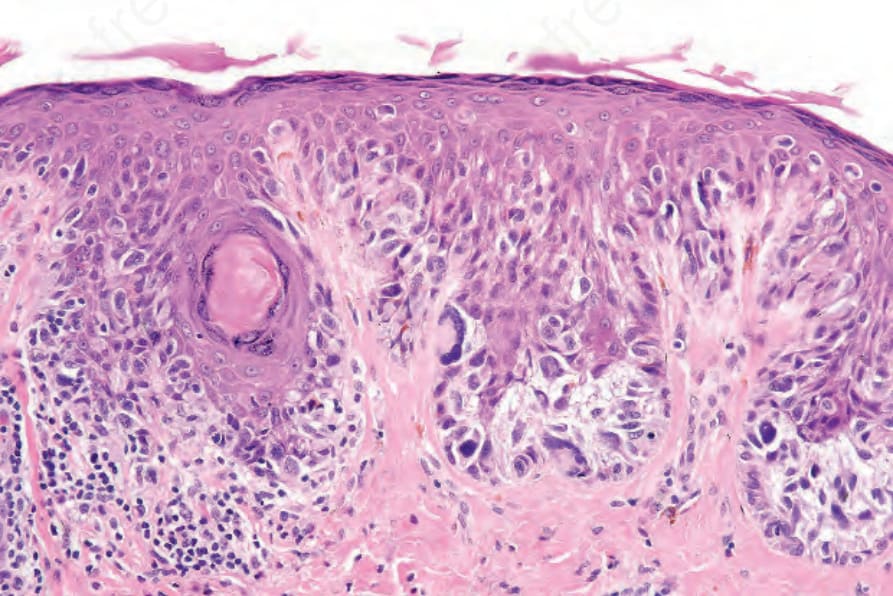
Fig. 26.20 Lentigo maligna: multinucleate tumor cells as shown in this example are a common feature and a useful diagnostic clue.
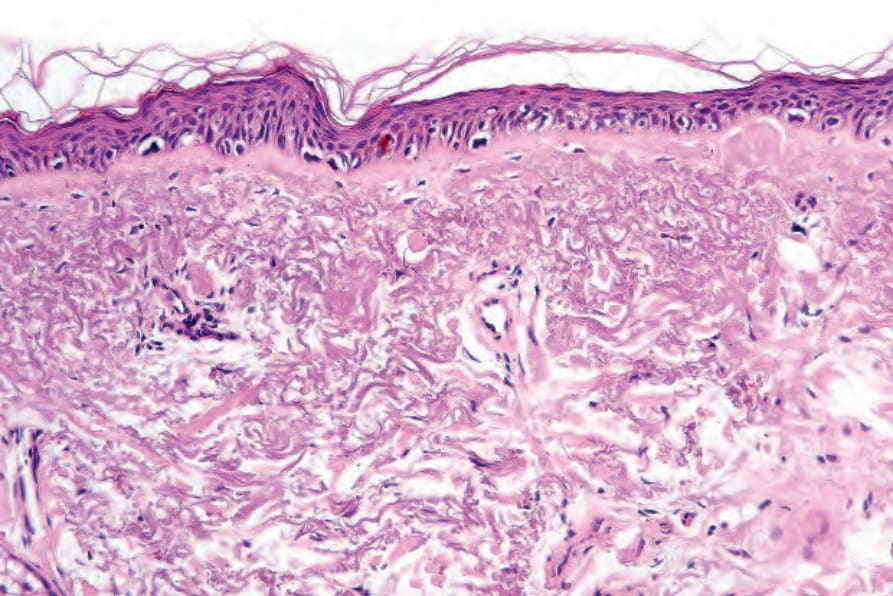
Fig. 26.21 Actinic nuclear atypia: sometimes distinguishing between the former and residual tumor cells as shown in this field can be a real problem. The former, however, show little nuclear enlargement and nucleoli are absent. In addition, such cells do not form nuclear palisades as is typical of lentigo maligna.
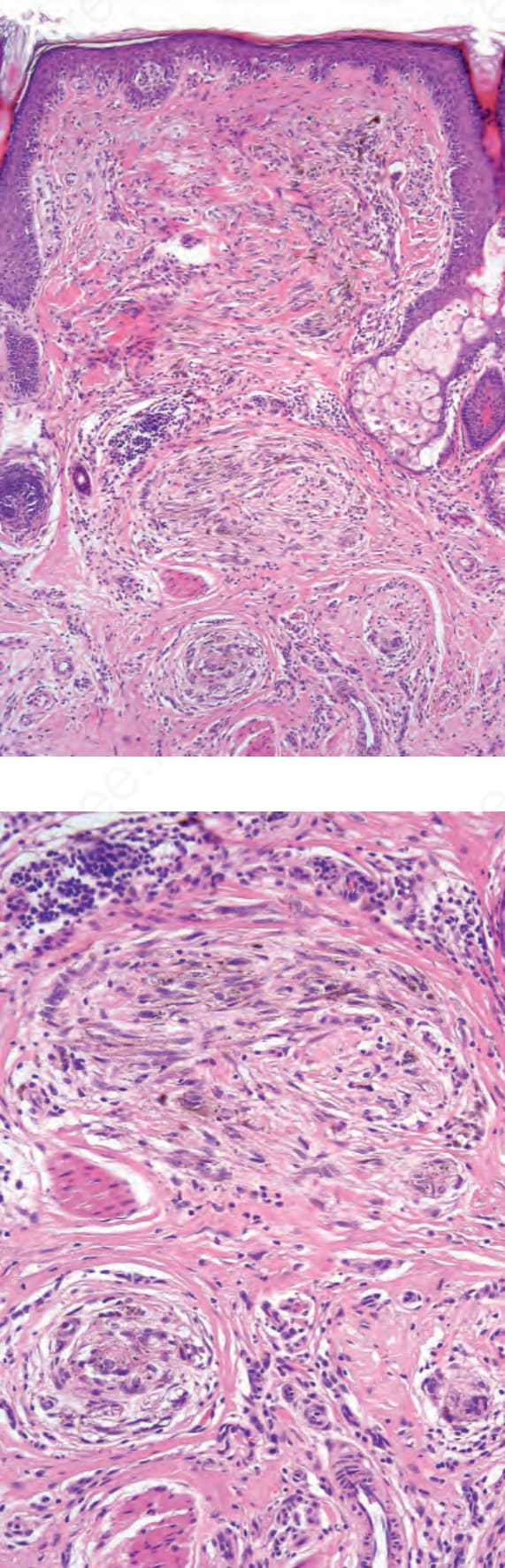
Fig. 26.22 Lentigo maligna melanoma: in this variant of melanoma, the invasive component is often of the spindle cell type.
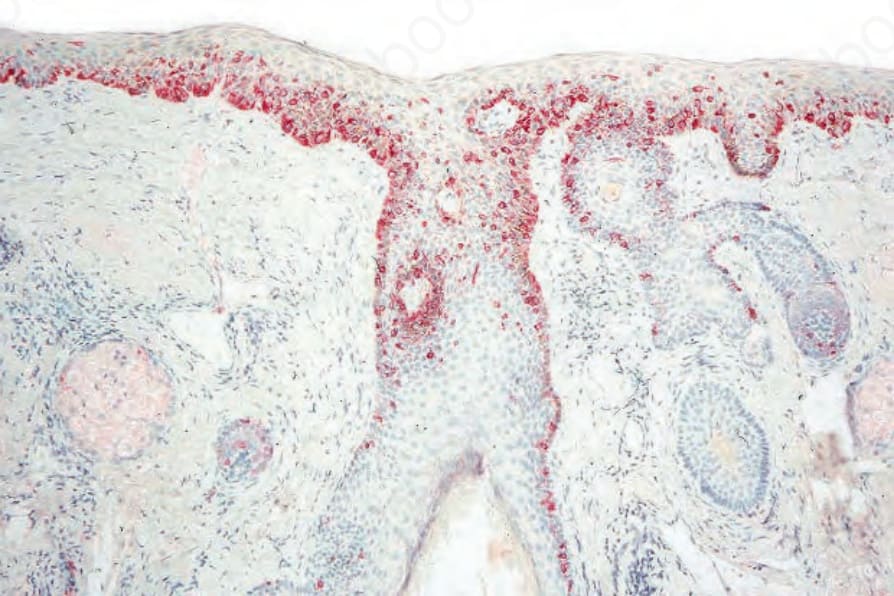
Fig. 26.25 Lentigo maligna melanoma: occasionally the tumor adopts a storiform pattern. When amelanotic, this may be confused with dermatofibrosarcoma protuberans or spindle cell squamous carcinoma.
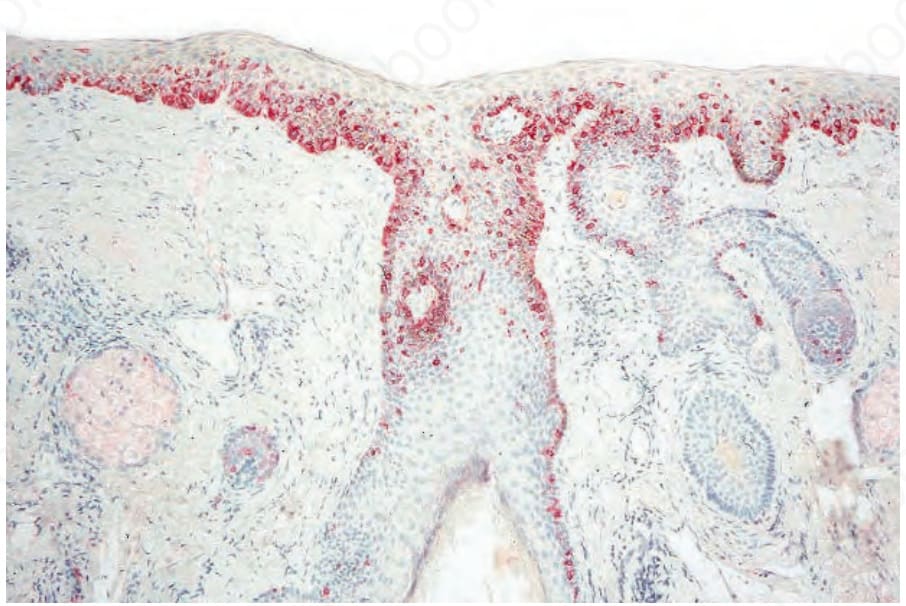
Fig. 26.26 Lentigo maligna: occasionally it is difficult to distinguish between actinic keratosis and lentigo maligna. In such cases, immunohistochemistry using a red chromogen (in this case alkaline phosphatase) can make the distinction easy.