蒙古斑 (Mongolian Spot)
臨床特徵 (Clinical Features)
- 蒙古斑 (Mongolian spot) 表現為相對均勻的板岩藍色 (slate blue)、按壓不褪色 (nonblanching) 的變色區,邊界呈波浪狀、形狀不規則,最常位於薦骨區 (sacral region)(圖 25.217)。較少見的情況下,分布較為廣泛,例如出現在大腿後側、小腿、背部與肩部。
- 病灶通常於出生時或出生後不久即出現,最常見於日本人、中國人及色素較深的種族。蒙古斑在男性中略為多見。病灶可相當大,直徑可達 10 cm。偶爾可疊加在另一個 Mongolian spot 之上。
- 蒙古斑常與多種共病 (comorbidities) 相關,包括遺傳性代謝疾病 (inherited disorders of metabolism)、血管性胎記 (vascular birthmarks) 及隱性脊椎裂閉合不全 (occult spinal dysraphism)。最常見的潛在儲積病 (storage diseases) 為 Hurler syndrome(mucopolysaccharidosis type II)、GM1 type I gangliosidosis 與 mucolipidosis type II,其次為 Niemann-Pick disease 及 mannosidosis。並存的 Mongolian spot 與血管性胎記(例如 nevus flammeus)一般被稱為 phakomatosis pigmentovascularis。此外,Mongolian spot 也曾報導與 noninvoluting congenital hemangioma、Sturge-Weber syndrome、Klippel-Trenaunay syndrome、cutis marmorata telangiectatica congenita、Sjögren-Larsson syndrome 及 segmental café-au-lait macules 同時出現。
1293 真皮黑色素細胞病灶 (dermal melanocytic lesions, dermal melanocytoses)
單側病灶,位於三叉腦神經 (trigeminal cranial nerve) 之眼支 (ophthalmic) 與上頜支 (maxillary) 分布區(圖 25.220)。亦曾報導以雙側多發性雀斑樣痣 (bilateral multiple lentigines) 形式表現,例如 agminated lentigines。Nevus of Ota 在 5% 的病例中呈雙側分布。約 60% 的患者鞏膜 (sclera) 與結膜 (conjunctiva) 受累;偶爾鼻腔與口腔黏膜也會受影響。罕見情況下,類似的變色會侵犯軟腦膜 (leptomeninges)。超過 50% 的此類病灶於出生時即存在,其餘大多於青春期前後出現。其呈現女性優勢。曾記載家族性發生的例外病例。亦可見丘疹與結節,顯示存在 blue nevus 與 cellular blue nevus 成分。與 Mongolian blue spot 相反,nevus of Ota 為永久性。近期曾報導同一部位同時發生 nevus of Ota 與 nevus spilus 的合併性痣 (combined nevus)。
大多數 Mongolian spot 於嬰兒期或兒童期自發消退 (spontaneous regression),並一般於青春期前消失。然而病灶持續至成年期的情況罕見,且通常與薦骨外 (extrasacral) 部位相關。與遺傳性儲積病相關者通常不顯示消退跡象,且可能隨時間變得色素更深。曾記載 Mongolian spot 伴隨 halo nevus 樣外觀的情形。
僅極罕見地,nevus of Ota 會發生惡性轉化(見 malignant blue nevus),主要發生於白種人 (Caucasians)。黑色素瘤 (melanoma) 曾被記載發生於皮膚、虹膜 (iris)、脈絡膜 (choroid)、眼眶 (orbit) 及腦膜 (meninges)。與此痣相關描述的其他腫瘤包括 meningeal melanocytoma 與 melanotic schwannoma。亦曾描述雙側 nevus of Ota 與青光眼 (glaucoma) 及 Klippel-Trenaunay syndrome 的關聯。
組織病理特徵 (Histopathology)
- Mongolian spot 與其他原發性真皮黑色素細胞病灶 (primary dermal melanocytic lesions, dermal melanocytoses) 被認為代表黑色素細胞 (melanocytes) 從神經嵴 (neural crest) 向表皮遷移過程中受阻 (arrested transdermal migration)。因此病灶的特徵為真皮內樹突狀 (intradermal dendritic)、色素含量不一的黑色素細胞稀疏散布,這些細胞傾向平行於皮膚表面排列,並主要位於深層網狀真皮 (deep reticular dermis)(圖 25.218 與 25.219)。上覆的上皮 (epithelium) 正常。
- 雖然 Mongolian spot 代表良性的樹突狀細胞增生 (benign dendritic cell proliferation),但其預後一般由共病 (comorbidities) 決定。
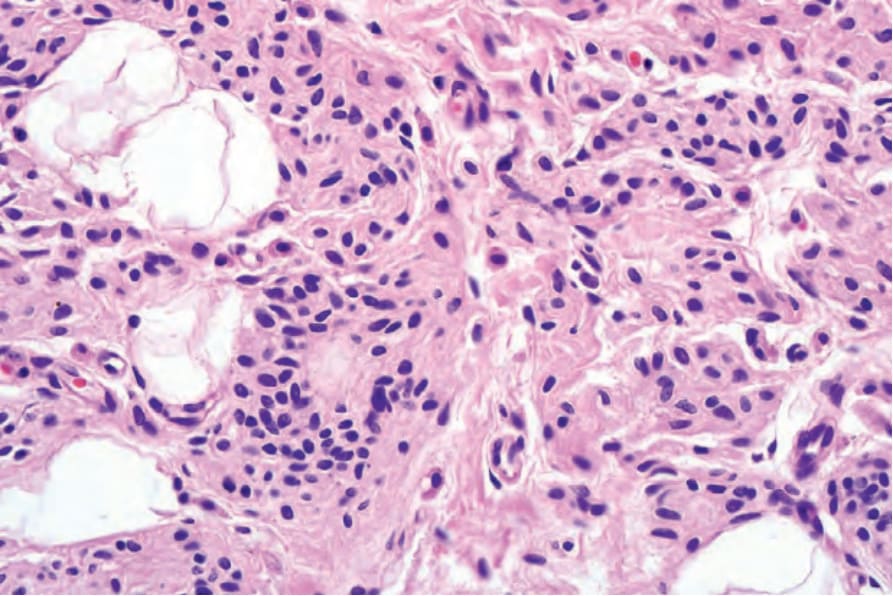
圖 25-215:增生性結節 (proliferation nodule):先天性痣 (congenital nevus) 的高倍視野。
Fig. 25.215 Proliferation nodule: high-power view of the congenital nevus.
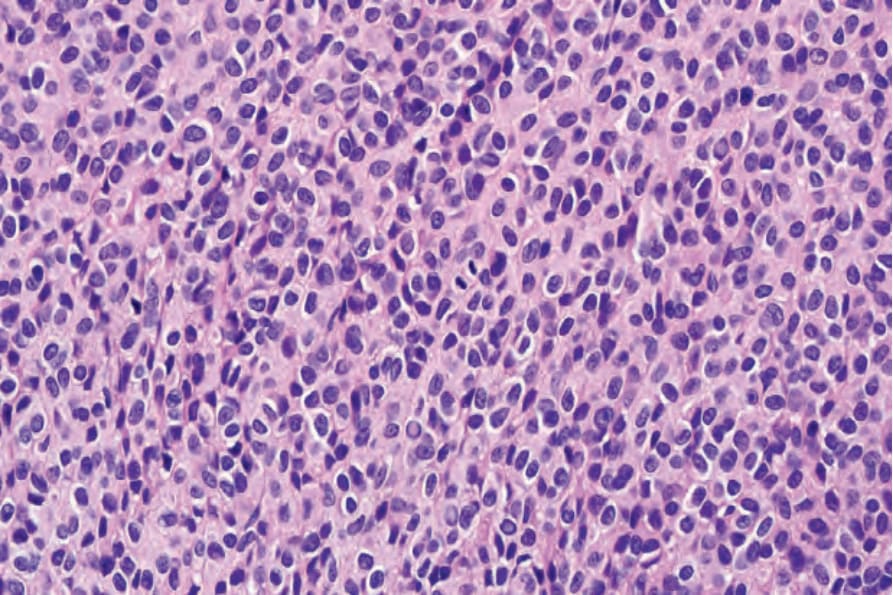
圖 25-216:增生性結節 (proliferation nodule):結節由均勻一致的痣細胞 (nevus cells) 群所組成。注意中央的有絲分裂象 (mitotic figure)。
Fig. 25.216 Proliferation nodule: the nodule is composed of a uniform population of nevus cells. Note the central mitotic figure.

圖 25-217:蒙古藍斑 (Mongolian blue spot):此孩童的軀幹與臀部上有廣泛的淡藍色變色。By courtesy of S. Bleehen, MD, Royal Hallamshire Hospital, Sheffield, UK.
Fig. 25.217 Mongolian blue spot: there is extensive pale blue discoloration on this child’s trunk and buttocks. By courtesy of S. Bleehen, MD, Royal Hallamshire Hospital, Sheffield, UK.
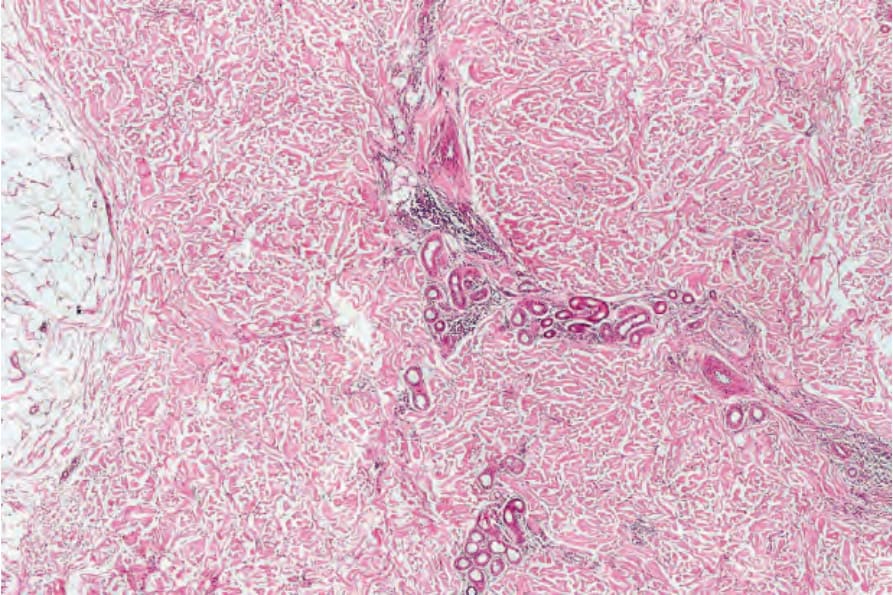
圖 25-218:蒙古藍斑 (Mongolian blue spot):低倍檢查下特徵不明顯,僅見較深層真皮 (deeper dermis) 內細胞數增加。
Fig. 25.218 Mongolian blue spot: at low-power examination, the features are subtle, comprising increased cellularity in the deeper dermis.
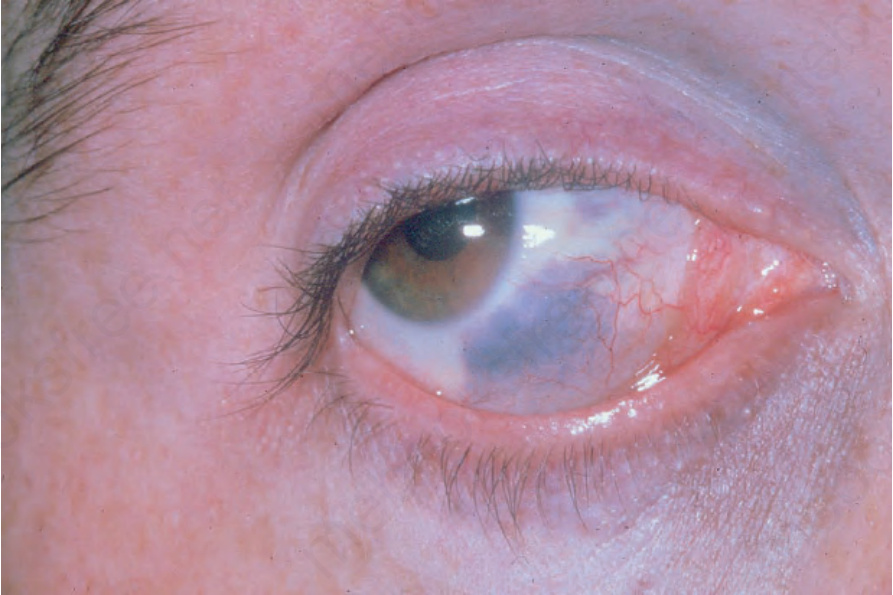
圖 25-220:太田痣 (nevus of Ota):可見鞏膜 (sclera) 受累,眼周 (periocular) 出現明顯的藍色變色。By courtesy of the Institute of Dermatology, London, UK.
Fig. 25.220 Nevus of Ota: there is scleral involvement and a periocular bluish discoloration is evident. By courtesy of the Institute of Dermatology, London, UK.