Mongolian spot
Mongolian spot
Clinical features Mongolian spots present as relatively uniform slate blue areas of nonblanching discoloration with a wavy border and irregular shape, most often situated over the sacral region (Fig. 25.217). Much less often, they are more
widely distributed, for example, over the posterior thighs, legs, back, and shoulders.1,2 They usually present at birth or soon after and are most commonly seen in Japanese, Chinese, and pigmented races.3 Mongolian spots are slightly more common in males. The lesions may be quite large, measuring up to 10 cm in diameter.4 They can, on occasion, be superimposed upon another Mongolian spot.5
Mongolian spots are often associated with different comorbidities, including inherited disorders of metabolism, vascular birthmarks, and occult spinal dysraphism.6 The most common underlying storage diseases are Hurler syndrome (mucopolysaccharidosis type II), GM1 type I gangliosidosis, and mucolipidosis type II, followed by Niemann-Pick disease and mannosidosis.6–11 Coexisting Mongolian spot(s) and vascular birthmark(s), for example, nevus flammeus, have generally been referred to as phakomatosis pigmentovascularis. In addition, Mongolian spot(s) have also been reported in conjunction with noninvoluting congenital hemangioma, Sturge-Weber syndrome, Klippel-Trenaunay syndrome, cutis marmorata telangiectatica congenita, Sjögren-Larsson syndrome, and segmental café-au-lait macules.12–20
1293 Dermal melanocytic lesions (dermal melanocytoses)
unilateral lesion situated in the distribution of the ophthalmic and maxillary divisions of the trigeminal cranial nerve (Fig. 25.220).1–3 Presentation in the form of bilateral multiple lentigines, e.g., agminated lentigines, has also been reported.4 Nevus of Ota shows bilateral distribution in 5% of cases. In about 60% of patients, the sclera and conjunctiva are involved; occasionally, the mucous membranes of the nose and oral cavity are also affected.1,2,5,6–8 Rarely, a similar discoloration involves the leptomeninges. Over 50% of these lesions are present at birth and most of the remainder appear at around puberty. It shows female predominance. Exceptional cases of familial occurrence have been documented.5,9–11 Papules and nodules may also be seen, indicating blue nevus and cellular blue nevus components. In contrast to the Mongolian blue spot, the nevus of Ota is permanent.2 A combined nevus of Ota with nevus spilus occurring in the same area has recently been reported.12
Most Mongolian spots undergo spontaneous regression during infancy or childhood, and generally disappear by puberty.1,2 Persistence of the lesion into adulthood is, however, rare and has been usually linked to extrasacral locations.1,21 Those associated with inheritable storage diseases usually do not show signs of resolution and can become even more pigmented with time.9,10 Mongolian spot associated with a halo nevus-like appearance has been documented.22
Only very rarely has malignant transformation occurred in nevus of Ota (see malignant blue nevus), predominantly in Caucasians.13 Melanoma has been documented in the skin, iris, choroid, orbit, and meninges.4–6,9–10,13–23 Additional tumors, described in association with this nevus, include meningeal melanocytoma and melanotic schwannoma.24–26 Association of bilateral nevus of Ota with glaucoma and Klippel-Trenaunay syndrome has also been described.5,27
Histologic features Mongolian spot and other primary dermal melanocytic lesions (dermal melanocytoses) are believed to represent arrested transdermal migration of melanocytes from the neural crest to the epidermis. The lesion is therefore characterized by a sparse population of intradermal dendritic, variably pigmented melanocytes, which tend to be oriented parallel to the skin surface and situated predominantly in the deep reticular dermis (Figs 25.218 and 25.219). The overlying epithelium is normal.
Although Mongolian spot represents a benign dendritic cell proliferation, comorbidities generally define prognosis.
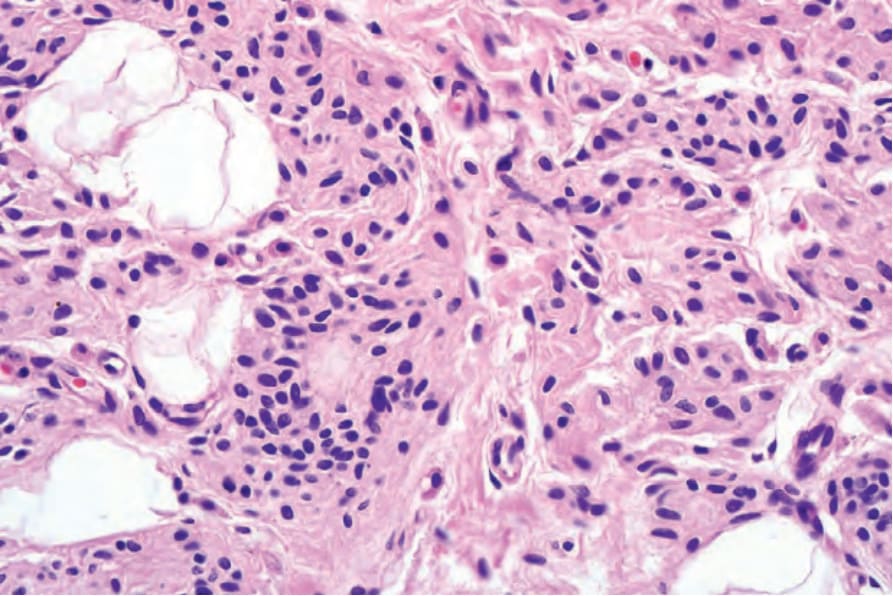
Fig. 25.215 Proliferation nodule: high-power view of the congenital nevus.
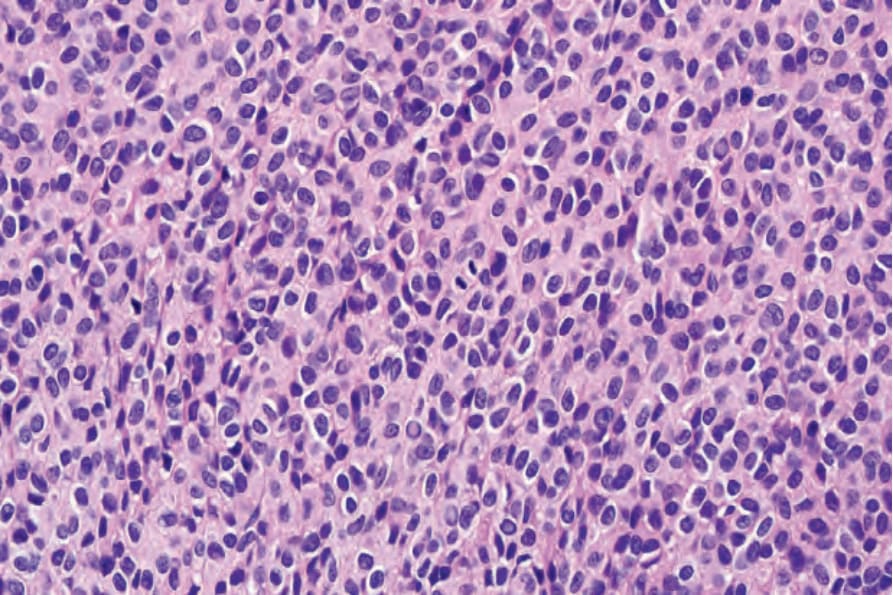
Fig. 25.216 Proliferation nodule: the nodule is composed of a uniform population of nevus cells. Note the central mitotic figure.

Fig. 25.217 Mongolian blue spot: there is extensive pale blue discoloration on this child’s trunk and buttocks. By courtesy of S. Bleehen, MD, Royal Hallamshire Hospital, Sheffield, UK.
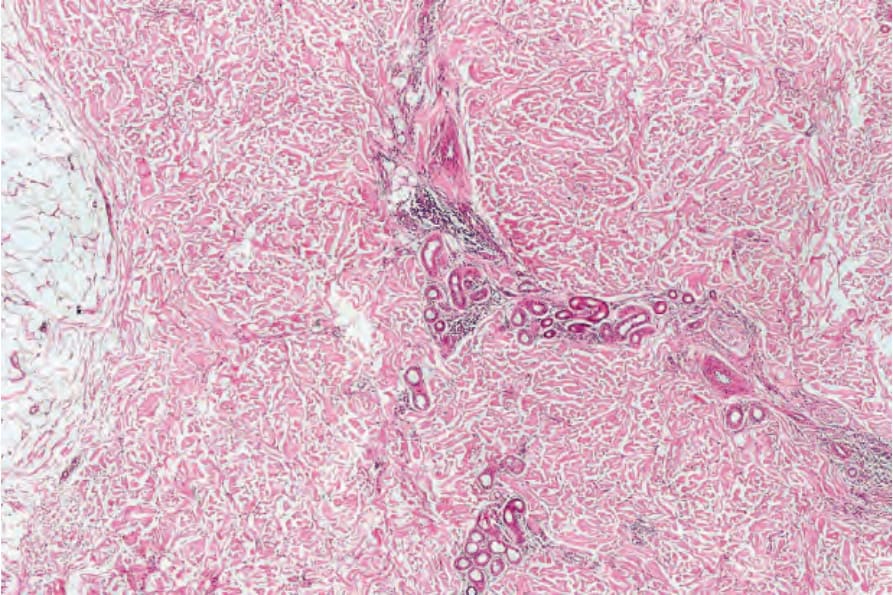
Fig. 25.218 Mongolian blue spot: at low-power examination, the features are subtle, comprising increased cellularity in the deeper dermis.
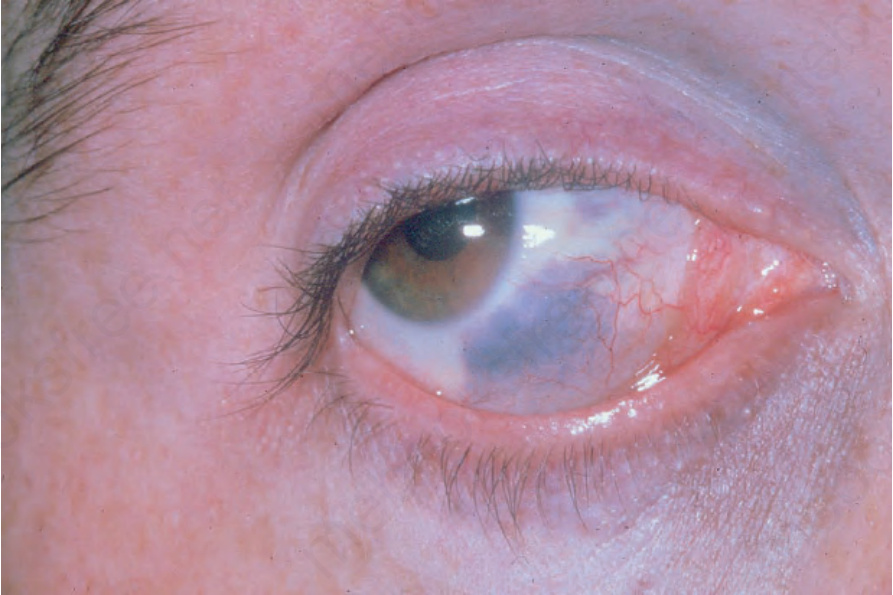
Fig. 25.220 Nevus of Ota: there is scleral involvement and a periocular bluish discoloration is evident. By courtesy of the Institute of Dermatology, London, UK.