臨床特徵 (Clinical Features)
-
復發性痣 (recurrent nevus/pseudomelanoma) 是指在先前良性黑色素細胞痣 (benign melanocytic nevus) 切除不完全後,所發生的一種非典型黑色素細胞病灶。最常見於削切式切片 (shave biopsy) 之後。類似變化也可於外傷、雷射治療及局部外用藥物使用後發生。
-
recurrent nevus 表現為不對稱、不規則、色素深淺不一的斑狀 (macular) 病灶,常見局限於疤痕區域內的點狀黑色斑點 (stippled black areas)(Fig. 25.91)。相對地,復發性 Spitz 痣與藍痣 (recurrent Spitz and blue nevi) 常為丘疹狀或結節狀病灶,並延伸超出疤痕範圍。此外,復發性 Spitz 痣偶可在先前切除區域以多發衛星狀結節 (multiple satellite nodules) 表現。
-
一般而言,復發最常於初次處置後 6 個月內發生,呈女性優勢,且最常發生於背部。
-
混合性痣 (combined nevi) 因其雜色素 (variegate pigmentation) 與頻繁的不對稱性,可能引起臨床疑慮。其性別分布相等,好發於兒童與年輕成人,最常發生於軀幹,其次依頻率遞減為頭頸部、上肢、下肢、會陰及臀部。combined nevi 亦曾於黏膜部位(包括結膜 conjunctiva)被記載。
-
在皮膚鏡 (dermoscopy) 下,有助於辨識復發性/持續性黑色素細胞痣的線索包括:增生的對稱性、放射狀線條 (radial lines) 的存在,以及離心性生長 (centrifugal growth)。相對地,最重要的單一參數
-
最能提示黑色素瘤 (melanoma) 者,被認為是延伸超出疤痕範圍的色素沉著。
組織病理特徵 (Histologic Features)
-
不同類型的黑色素細胞 (melanocytes) 可能相互混雜或彼此相對分隔清楚(Figs 25.88–25.90)。
-
先前所切除痣的殘餘 (remnants) 常可見於淺層真皮,並伴隨真皮疤痕化 (dermal scarring);通常可見淺層血管周圍慢性發炎細胞浸潤 (superficial perivascular chronic inflammatory cell infiltrate)(Fig. 25.92)。噬黑色素細胞 (melanophages) 通常明顯。
-
然而,具意義的組織學特徵存在於表皮 (epidermis)。交界處成分 (junctional component) 界限分明,且特徵性地不延伸超出疤痕區域。recurrent nevus 由非典型黑色素細胞 (atypical melanocytes) 組成,呈單個及成簇分布,通常位於表皮下層,有時顯示輕度或中度核多形性 (nuclear pleomorphism) 與深染 (hyperchromatism)(Fig. 25.93)。黑色素細胞通常以上皮樣形態 (epithelioid morphology) 為主。有時可見輕微的佩吉特樣擴散 (pagetoid spread)。一般不見有絲分裂象 (mitotic figures),凋亡 (apoptosis) 亦非其特徵。覆蓋疤痕之上的表皮突 (rete ridge) 形態常被抹平。然而偶爾可見局限於疤痕區域、呈網狀 (retiform) 形態的表皮增生。在與疤痕相關的淺層真皮成分中(若存在時),有時可見細胞學非典型 (cytological atypia)(Fig. 25.94)。在部分病例中,疤痕下方區域可見痣的殘餘一般成分 (residual ordinary component)。真皮有絲分裂 (dermal mitoses) 一般缺如,惟仔細檢視偶可發現少數正常有絲分裂。
-
「惡性混合性痣 (malignant combined nevus)」一詞曾被用以描述一例使良性與細胞性藍痣 (banal and cellular blue nevus) 併發的原位黑色素瘤 (in situ melanoma)。
鑑別診斷 (Differential Diagnosis)
-
在缺乏臨床資訊的情況下,最初可能懷疑為 melanoma。組織學鑑別要點包括:特徵性的界限分明、交界處成分嚴格局限於緊鄰疤痕正上方的區域、缺乏有絲分裂活性與凋亡,以及存在緻密的反應性疤痕化 (dense reactive scarring)。
-
臨床病理對照 (clinicopathological correlation) 至關重要。亦應謹記,殘餘的異型增生痣 (residual dysplastic nevi) 可能與復發性痣現象相關,而切除不完全的原位黑色素瘤 (incompletely excised melanoma in situ) 可能類似復發性痣。在困難病例中,回顧先前的病理材料至關重要。
-
combined melanocytic nevus 可藉由下列特徵與 melanoma 區別:交界處成分缺乏 melanoma in situ、腫瘤細胞缺乏多形性(包括缺乏明顯核仁 prominent nucleolus)及真皮成分缺乏擴張性生長型態 (expansile growth pattern),以及 combined nevus 中缺乏或僅極偶見正常有絲分裂。
硬化性痣 (Sclerosing Nevus)
- pseudomelanoma 現象亦曾在黑色素細胞痣的一個亞群中被報告,即所謂的硬化性痣 (sclerosing nevi)。其組織學特徵為一中央疤痕化區域(與先前處置或外傷無關),並伴隨疤痕周邊的痣殘餘。與復發性痣中的 pseudomelanoma 現象相似,sclerosing nevus 的表皮成分由大小不規則且融合的黑色素細胞巢 (confluent nests of melanocytes) 組成,偶有黑色素細胞向上延伸,局限於疤痕上方的區域。
- sclerosing nevi 典型呈現有序的纖維化型態,特徵為與表皮平行排列的均質嗜伊紅性膠原纖維束 (homogeneous bundles of eosinophilic collagen fibers)。纖維化/硬化區域內含有不規則的黑色素細胞巢。在表皮黑色素細胞成分或硬化區域內被包裹的黑色素細胞巢中,皆未見明顯的黑色素細胞非典型,有絲分裂缺如或稀少。這些變化被認為與病灶的部分消退 (partial regression) 有關。
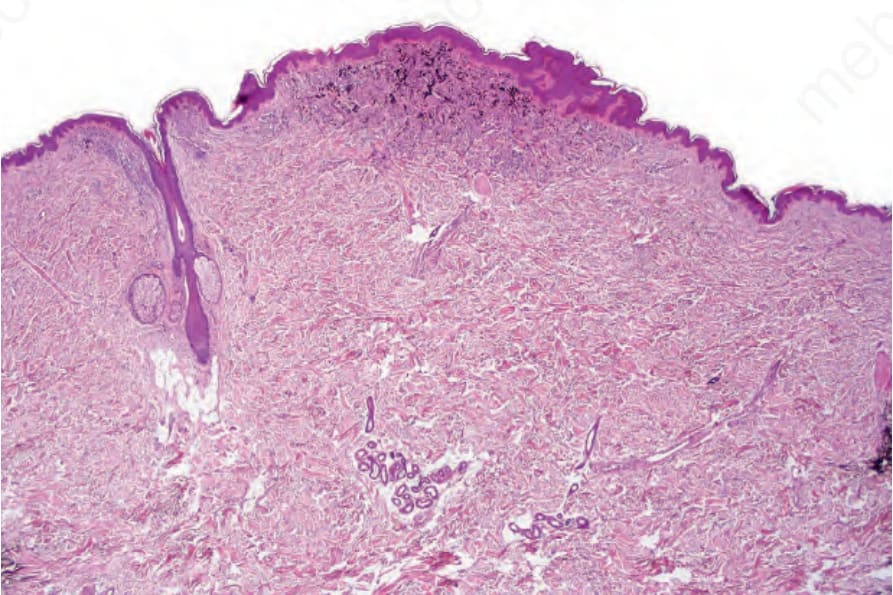
圖 25-88:混合性痣 (combined nevus):低倍視野,顯示毛囊旁的良性痣 (banal nevus) 與視野中央良性痣細胞和藍痣細胞 (banal and blue nevus cells) 的混合。
Fig. 25.88 Combined nevus: low-power view showing banal nevus adjacent to the hair follicle and an admixture of banal and blue nevus cells in the center of the field.
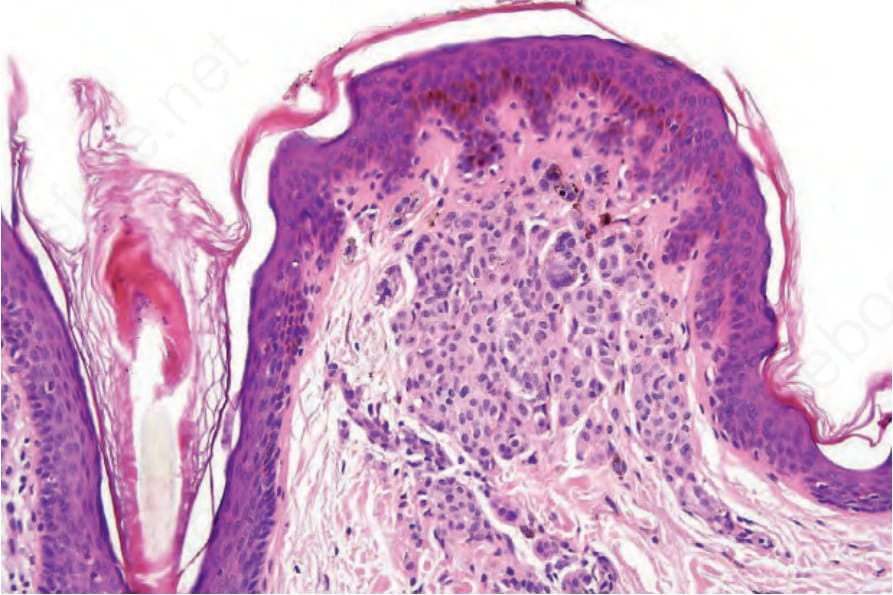
圖 25-89:混合性痣 (combined nevus):毛囊周圍良性痣細胞 (perifollicular banal nevus cells) 的高倍視野。
Fig. 25.89 Combined nevus: high-power view of perifollicular banal nevus cells.

圖 25-90:混合性痣 (combined nevus):混合的良性與樹突狀細胞 (banal and dendritic cells) 及明顯噬黑色素細胞 (melanophages) 的高倍視野。
Fig. 25.90 Combined nevus: high-power view of admixed banal and dendritic cells with conspicuous melanophages.
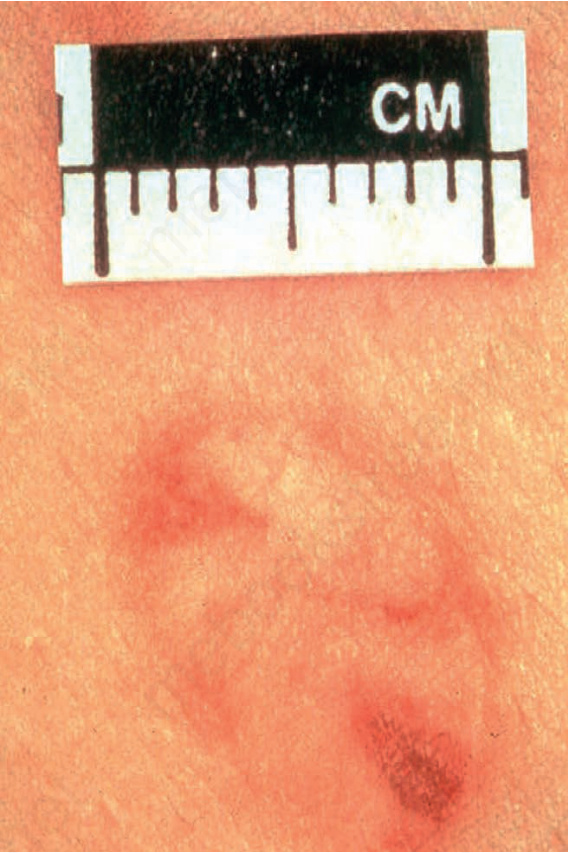
圖 25-91:復發性痣 (recurrent nevus):可見多個不規則的色素沉著病灶,與代表淺層真皮疤痕化的背景蒼白形成對比。承蒙 Institute of Dermatology, London, UK 惠允提供。
Fig. 25.91 Recurrent nevus: there are multiple irregular foci of pigmentation contrasting with background pallor representing superficial dermal scarring. By courtesy of the Institute of Dermatology, London, UK.
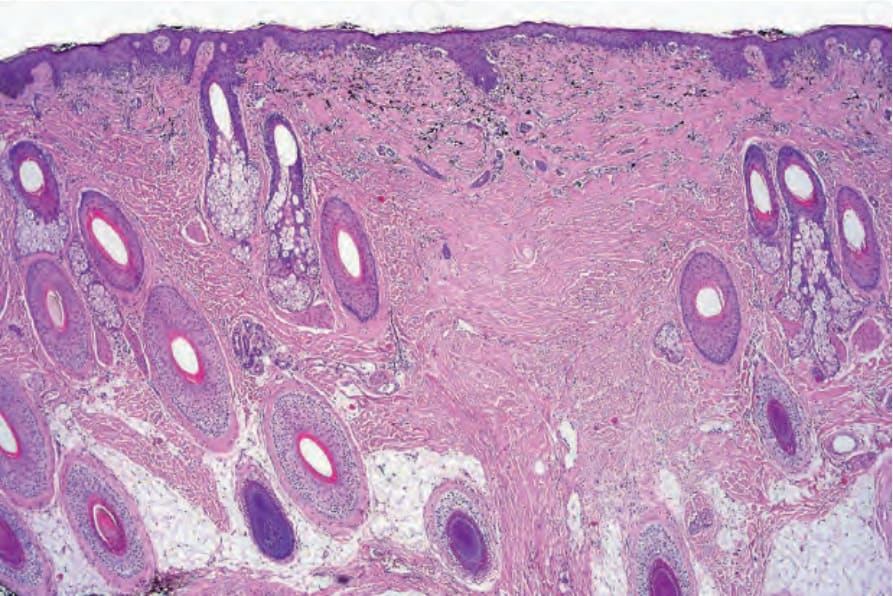
圖 25-92:復發性痣 (recurrent nevus):可見緻密的真皮疤痕化,其上覆蓋以交界處為主的黑色素細胞增生 (predominantly junctional melanocytic proliferation)。真皮噬黑色素細胞 (dermal melanophages) 明顯。
Fig. 25.92 Recurrent nevus: there is dense dermal scarring with an overlying predominantly junctional melanocytic proliferation. Dermal melanophages are conspicuous.
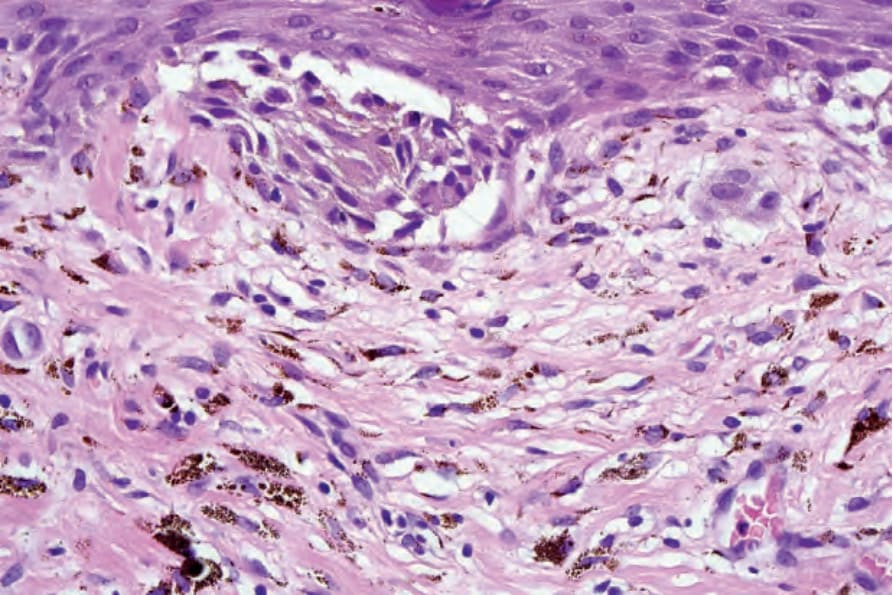
圖 25-93:復發性痣 (recurrent nevus):交界處成分的高倍視野,顯示由非典型痣細胞組成的失黏附細胞巢 (dyscohesive nest of atypical nevus cells)。淺層真皮可見散在的痣細胞與混雜的噬黑色素細胞 (melanophages)。
Fig. 25.93 Recurrent nevus: high-power view of junctional component showing a dyscohesive nest of atypical nevus cells. Scattered nevus cells with admixed melanophages are present in the superficial dermis.
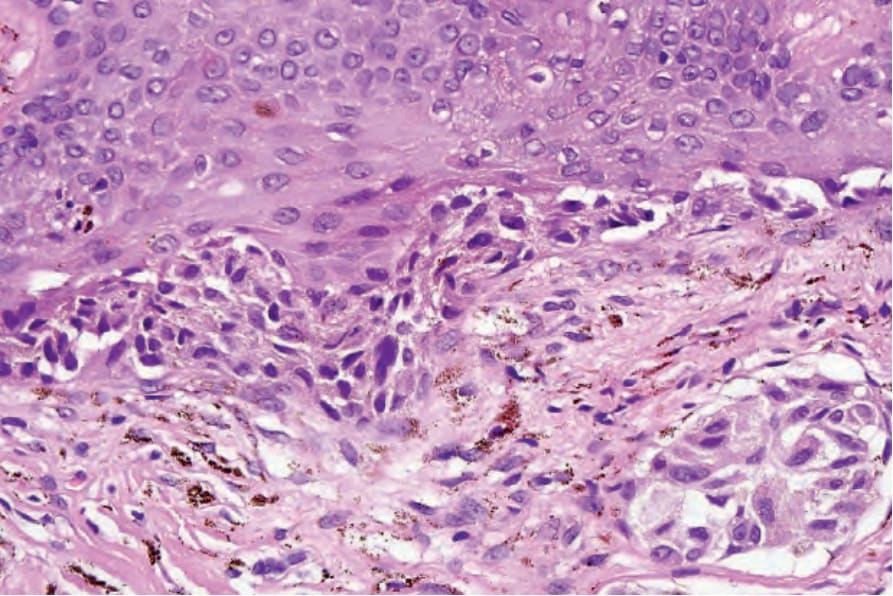
圖 25-94:復發性痣 (recurrent nevus):可見橋接 (bridging),且交界處與真皮成分皆存在細胞學非典型 (cytological atypia)。在可疑病例中,建議回顧先前所切除的病灶。
Fig. 25.94 Recurrent nevus: there is bridging, and cytological atypia is present in both junctional and dermal components. In cases of doubt, review of the previously excised lesion is advised.