Recurrent and sclerosing nevus
Recurrent and sclerosing nevus
Clinical features
Recurrent nevus (pseudomelanoma) refers to the development of an atypical melanocytic lesion following inadequate excision of a previous benign melanocytic nevus.1–4 It most commonly follows a shave biopsy. Similar changes can also occur after trauma, laser treatment, and local application of topical agents.5,6 Recurrent nevus presents as an asymmetrical, irregular, variably pigmented macular lesion, often with stippled black areas restricted to the area of the scar (Fig. 25.91).1 In contrast, recurrent Spitz and blue nevi are frequently papular or nodular lesions that extend beyond the confines of the scar.7–9 Furthermore, recurrent Spitz nevus can exceptionally present with multiple satellite nodules in the area of previous excision.10 In general, recurrences most commonly develop within 6 months following the initial procedure, show female predominance, and most frequently occur on the back.11
Clinical features Combined nevi may be a source of concern because of variegate pigmentation and frequent asymmetry. They show an equal sex distribution and have predilection for children and young adults, developing most frequently on the trunk, followed by head and neck, upper extremity, lower extremity, perineum, and buttocks in decreasing order of frequency.5 Combined nevi have also been documented in mucosal sites, including the conjunctiva.11
On dermoscopy, helpful clues for recurrent/persistent melanocytic nevus include symmetry of the proliferation, the presence of radial lines, and centrifugal growth.12 In contrast, the single most important parameter
Histologic features Different types of melanocytes may be admixed or relatively well separated from each other (Figs 25.88–25.90).
The term malignant combined nevus was used to describe an example of in situ melanoma that complicated a banal and cellular blue nevus.12
Differential diagnosis Combined melanocytic nevus can be distinguished from melanoma by the absence of melanoma in situ in the junctional component, lack of pleomorphism including a prominent nucleolus in tumor cells and expansile growth pattern in the dermal component, and by the absence of or only very occasional normal mitoses in combined nevus.
1258 Melanocytic nevi
hyperchromatism (Fig. 25.93).1 An epithelioid morphology of melanocytes usually predominates.11 Slight pagetoid spread is sometimes evident. Mitotic figures are not usually present, and apoptosis is not a feature. The rete ridge pattern overlying the scar is frequently effaced. On occasions, however, epidermal hyperplasia in a retiform pattern confined to the area of the scar can be seen.11 Cytological atypia is sometimes evident in the superficial dermal component associated with scar (when present) (Fig. 25.94). In some cases, a residual ordinary component of the nevus is seen in the area underlying the scar. Dermal mitoses are generally absent although, exceptionally, careful scrutiny may reveal an occasional normal mitosis.
suggestive of melanoma was found to be pigmentation beyond the confines of the scar.12
Histologic features Remnants of the previously excised nevus are often evident in the superficial dermis accompanied by dermal scarring; a superficial perivascular chronic inflammatory cell infiltrate is commonly present (Fig. 25.92). Melanophages are usually conspicuous.
The significant histologic features, however, are present in the epidermis. The junctional component is sharply delineated and characteristically does not extend beyond the area of scarring. Recurrent nevus consists of atypical melanocytes, both singly and in clusters, usually in the lower epidermis and sometimes showing mild or moderate nuclear pleomorphism and
Differential diagnosis In the absence of clinical information, melanoma may be suspected initially. Histologic points of distinction include the characteristic circumscription, the sharp restriction of the junctional component to the area immediately overlying the scar, the lack of mitotic activity and apoptosis, and the presence of dense reactive scarring.1
Clinicopathological correlation is essential. It should also be borne in mind that residual dysplastic nevi may be associated with a recurrent nevus phenomenon, and incompletely excised melanoma in situ may mimic a
recurrent nevus. Review of previous pathological material is essential in difficult cases.
The pseudomelanoma phenomenon has also been reported in a subset of melanocytic nevi, the so-called sclerosing nevi.13 These are characterized histologically by a central area of scarring, not related to previous procedure or trauma, accompanied by remnants of a nevus at the periphery of the scar. Similar to the pseudomelanoma phenomenon in recurrent nevi, the epidermal component in sclerosing nevus consists of irregularly sized and confluent nests of melanocytes with occasional upward extension of melanocytes, confined to the area above the scar. Sclerosing nevi typically display an orderly pattern of fibrosis, characterized by homogeneous bundles of eosinophilic collagen fibers arranged parallel to the epidermis. Areas of fibrosis/ sclerosis contain irregular nests of melanocytes.13 No significant atypia of melanocytes is seen in either the epidermal melanocytic component or in entrapped melanocytic nests within sclerotic areas, and mitoses are absent or scarce. These changes are thought to be related to partial regression of the lesion.
1259 Halo nevus
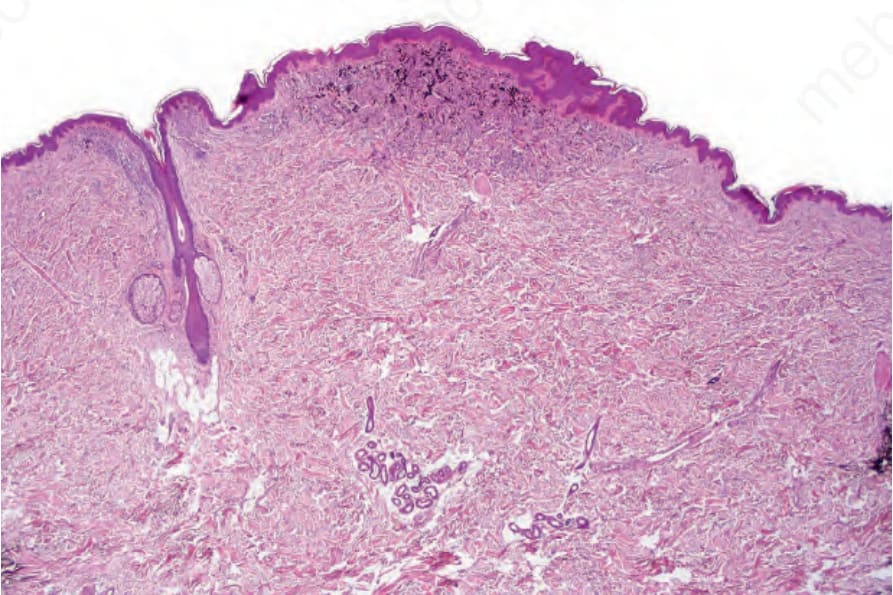
Fig. 25.88 Combined nevus: low-power view showing banal nevus adjacent to the hair follicle and an admixture of banal and blue nevus cells in the center of the field.
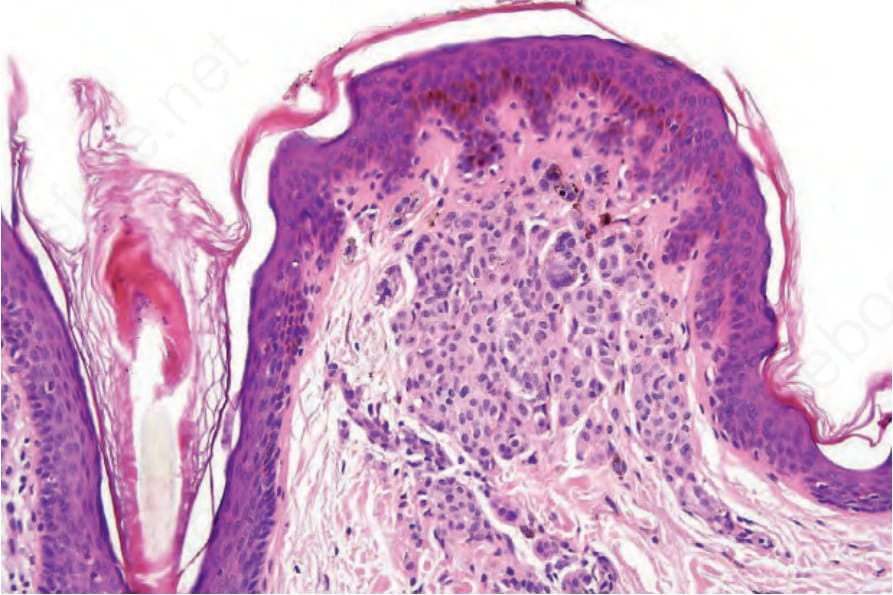
Fig. 25.89 Combined nevus: high-power view of perifollicular banal nevus cells.

Fig. 25.90 Combined nevus: high-power view of admixed banal and dendritic cells with conspicuous melanophages.
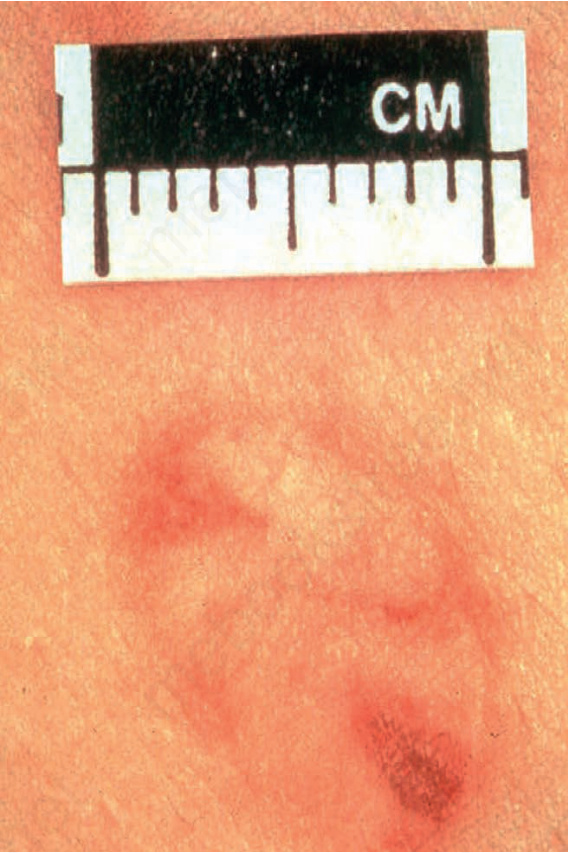
Fig. 25.91 Recurrent nevus: there are multiple irregular foci of pigmentation contrasting with background pallor representing superficial dermal scarring. By courtesy of the Institute of Dermatology, London, UK.
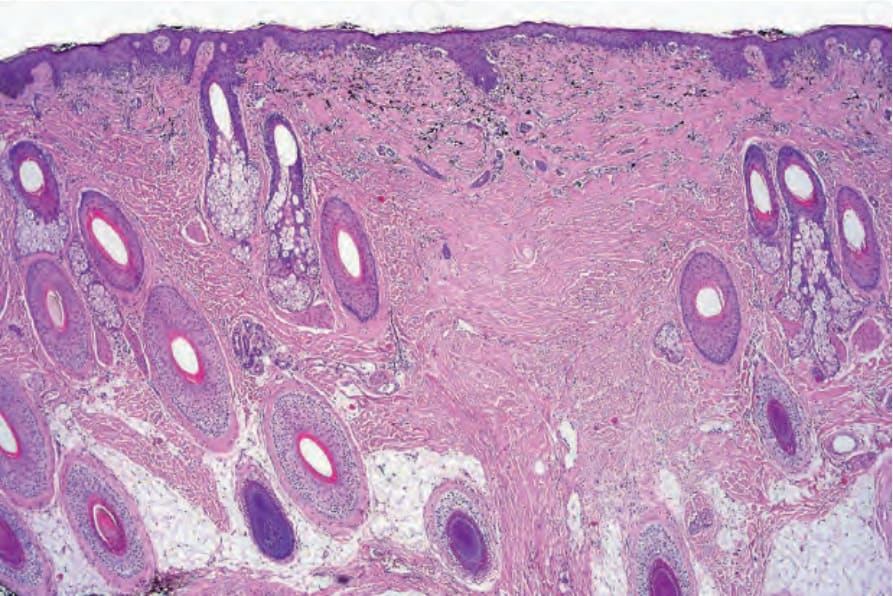
Fig. 25.92 Recurrent nevus: there is dense dermal scarring with an overlying predominantly junctional melanocytic proliferation. Dermal melanophages are conspicuous.
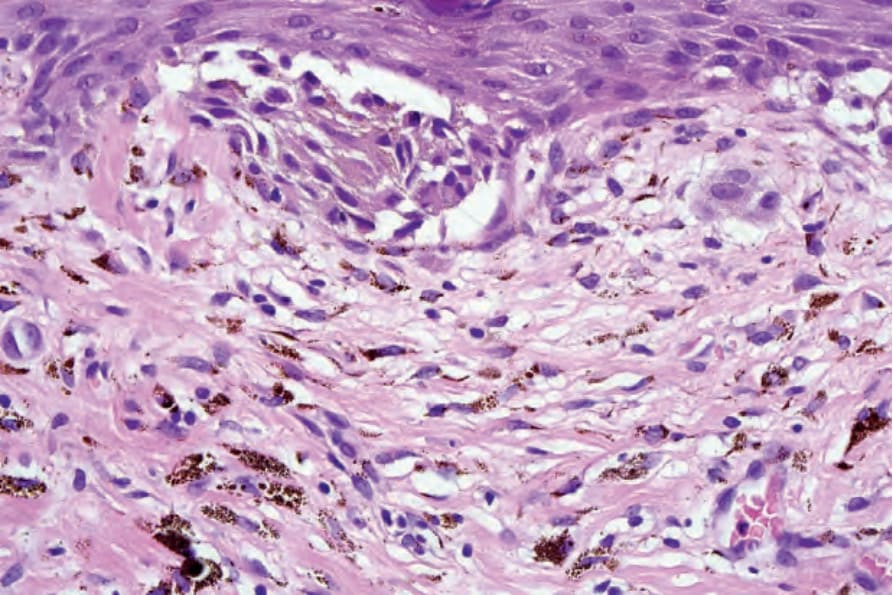
Fig. 25.93 Recurrent nevus: high-power view of junctional component showing a dyscohesive nest of atypical nevus cells. Scattered nevus cells with admixed melanophages are present in the superficial dermis.
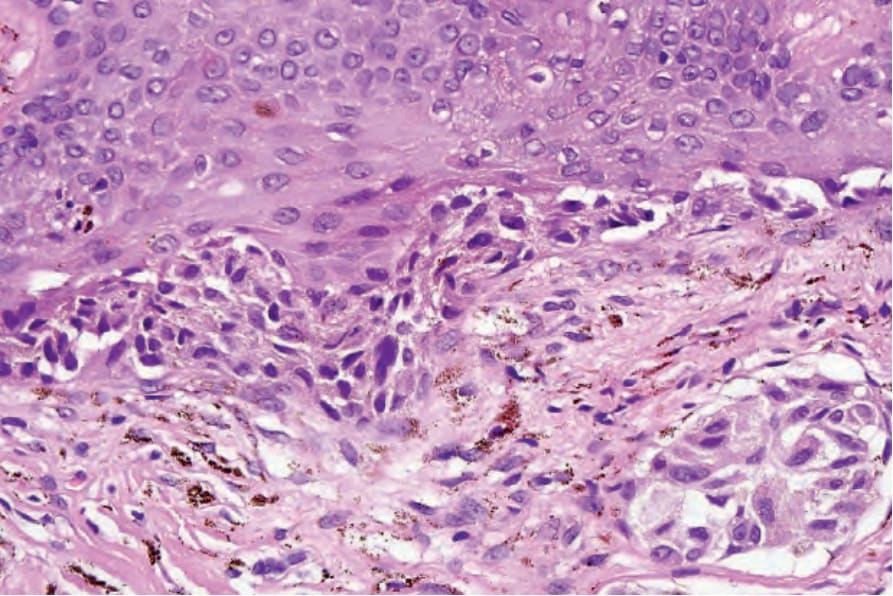
Fig. 25.94 Recurrent nevus: there is bridging, and cytological atypia is present in both junctional and dermal components. In cases of doubt, review of the previously excised lesion is advised.