臨床特徵 (Clinical Features)
- 肢端的掌蹠痣 (acral palmar and plantar nevi) 可能對稱、邊界清楚,與其他部位所見的一般性黑色素細胞痣 (banal melanocytic nevi) 或先天性痣 (congenital nevi) 完全相同;也可能不對稱、邊界不清,無論臨床或病理上皆造成診斷困難。
- 肢端痣 (acral nevi) 在膚色較深的患者 (skin-of-color patients) 及 Fitzpatrick 分型較深者中較白人常見。
- 第二類(acral nevus),有時亦稱為非典型肢端痣 (atypical acral nevus),臨床上通常不具特異性,表現為小於 1.0-cm、均勻色素沉著、深棕至黑色的斑 (macule) 或丘疹 (papule),邊緣不規則、有時界線不清 (Figs 25.79 與 25.80)。類似病變亦可見於手、足、指(趾)的背側面、甲下,以及膝部與肘部。曾有報告指出,兒童於接受急性淋巴母細胞白血病 (acute lymphoblastic leukemia) 化學治療後,足底會出現爆發性肢端痣 (eruptive acral nevi)。
- 肢端痣在皮膚鏡 (dermoscopy) 下具特徵性表現,且受其解剖位置影響。最常見的皮膚鏡特徵為平行溝紋型 (parallel furrow pattern),見於發生在足部非足弓 (non-arch) 及非承重 (non weight-bearing) 部位的大多數肢端痣。相對地,位於足弓 (arch) 的肢端痣典型呈現格子狀型 (lattice-like pattern),而位於承重面者則呈現纖維狀或絲狀型 (fibrillary or filamentous patterns)。
組織病理特徵 (Histopathology)
- 肢端(非典型)痣 (acral [atypical] nevus) 的特徵為沿真皮–表皮交界 (dermal–epidermal junction) 出現邊界清楚、通常對稱的雀斑樣 (lentiginous) 且成巢狀 (nested)、常呈連續性的黑色素細胞增生 (Figs 25.81 與 25.82)。
- 這些巢 (nests) 大小常不一,且常呈垂直走向。一個將其與鄰近角質細胞 (keratinocytes) 分隔開來的收縮假象 (retraction artifact) 為其特徵性表現。
- 表皮突 (rete ridges) 可能延長且變窄。
- 痣細胞具有明顯淡染的細胞質與深染至空泡狀 (hyperchromatic to vesicular) 的細胞核,有時顯示細胞學異型性 (cytological atypia)(通常為輕度)(Fig. 25.83)。核仁 (nucleoli) 可能明顯。
- 輕至中度的佩吉特樣擴散 (pagetoid spread) 並不少見,尤其位於痣的中央。有時 pagetoid spread 可非常顯著,幾乎累及整個病變——此類黑色素細胞增生一般稱為伴有細胞表皮內上行的黑色素細胞肢端痣 (melanocytic acral nevus with intraepidermal ascent of cells, MANIAC) (Fig. 25.84)。因此,角質層 (stratum corneum) 中常可見斑點狀色素沉著。
- 此外,沿 dermal–epidermal junction 的黑色素細胞常顯示樹突狀 (dendritic) 形態。
- 肢端痣的一項特徵為巢的經表皮排除 (transepidermal elimination of nests)。
- 黑色素細胞巢累及外分泌汗管 (eccrine ducts) 並不少見,但通常侷限於汗管的上段。
- 一般可見色素失禁 (pigmentary incontinence),並可能有輕度纖維化 (fibrosis),偶爾伴隨稀疏的淋巴球浸潤 (lymphocytic infiltrate)。淺層真皮纖維化 (superficial dermal fibrosis) 在承重部位(如足底)的病變中較為顯著,不應被解讀為消退 (regression)。真皮成分隨深度而成熟 (matures with depth),且缺乏有絲分裂活性。
鑑別診斷 (Differential Diagnosis)
- 非典型肢端痣 (atypical acral nevus) 可藉由缺乏肩部現象 (shoulder)、塵狀色素沉著 (dusty pigmentation) 與橋接 (bridging),以及缺乏層狀與嗜伊紅性纖維化 (lamellar and eosinophilic fibrosis),與肢端發育不良痣 (acral dysplastic nevus) 區分。肢端痣一般無宿主炎症反應 (host inflammatory response)。
- 其與肢端雀斑樣黑色素瘤 (acral lentiginous melanoma) 的區別在於缺乏不規則的表皮棘層肥厚 (irregular epidermal acanthosis)、嚴重的細胞學異型性、有絲分裂活性,以及在有真皮成分時的真皮成分成熟現象。
- 出現緻密的淋巴球浸潤高度懷疑為黑色素瘤 (melanoma),應促使仔細檢查額外切片以尋找確診特徵。
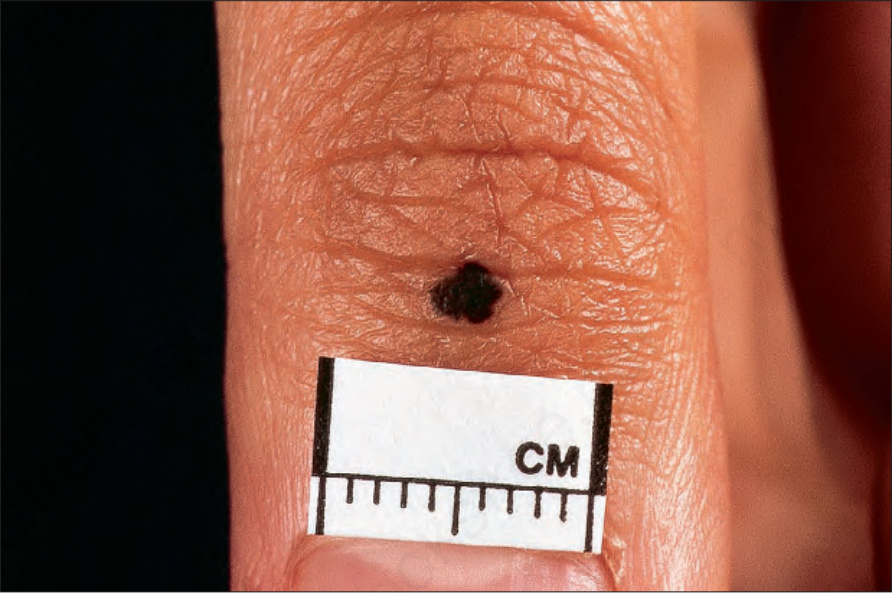
圖 25-79:肢端痣 (acral nevus):注意其強烈的色素沉著與不規則邊界。By courtesy of the Institute of Dermatology, London, UK.
Fig. 25.79 Acral nevus: note the intense pigmentation and irregular border. By courtesy of the Institute of Dermatology, London, UK.
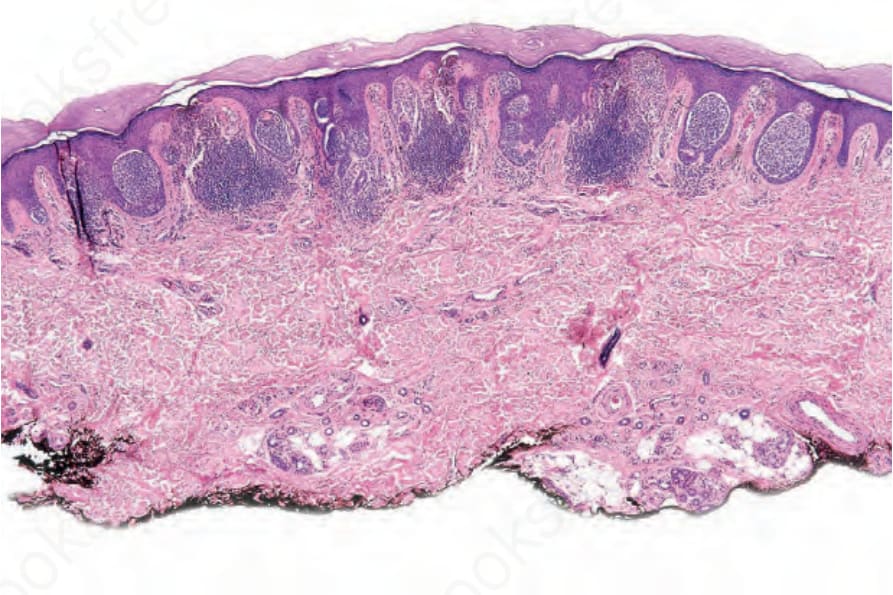
圖 25-81:肢端痣 (acral nevus):複合痣 (compound nevus),顯示被收縮假象 (retraction artifact) 環繞的垂直走向交界處巢 (junctional nests)。
Fig. 25.81 Acral nevus: compound nevus showing vertically oriented junctional nests surrounded by a retraction artifact.
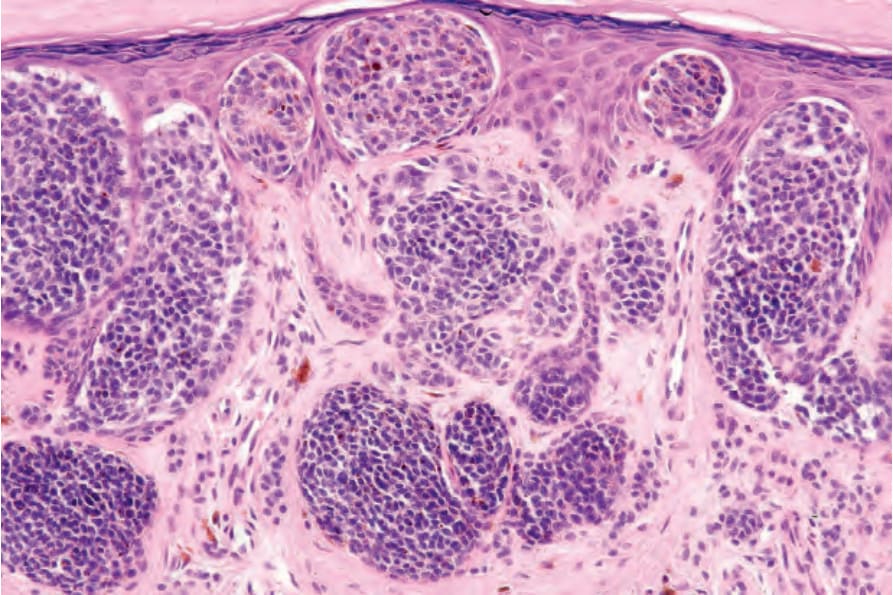
圖 25-82:肢端痣 (acral nevus):近距離視野,顯示表皮內巢 (intraepidermal nests)。
Fig. 25.82 Acral nevus: close-up view showing intraepidermal nests.
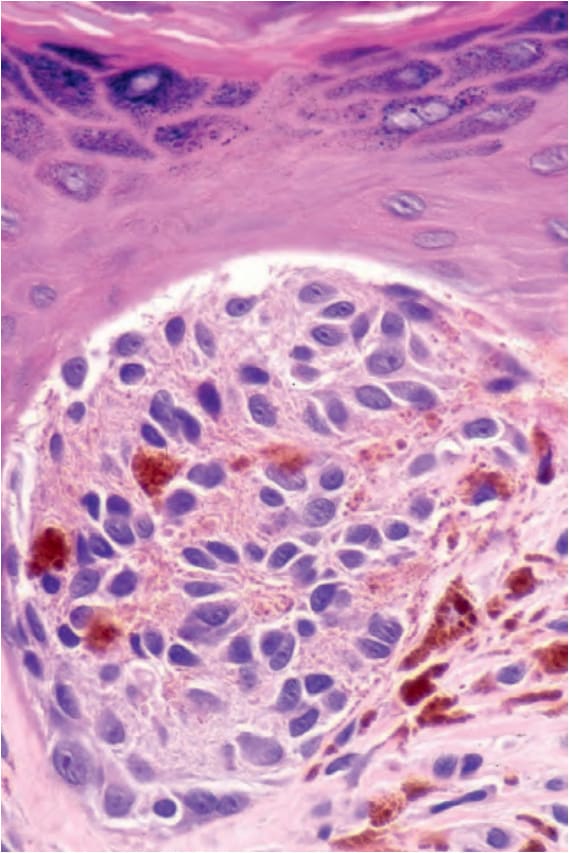
圖 25-83:肢端痣 (acral nevus):注意細胞學異型性 (cytological atypia)。
Fig. 25.83 Acral nevus: note the cytological atypia.
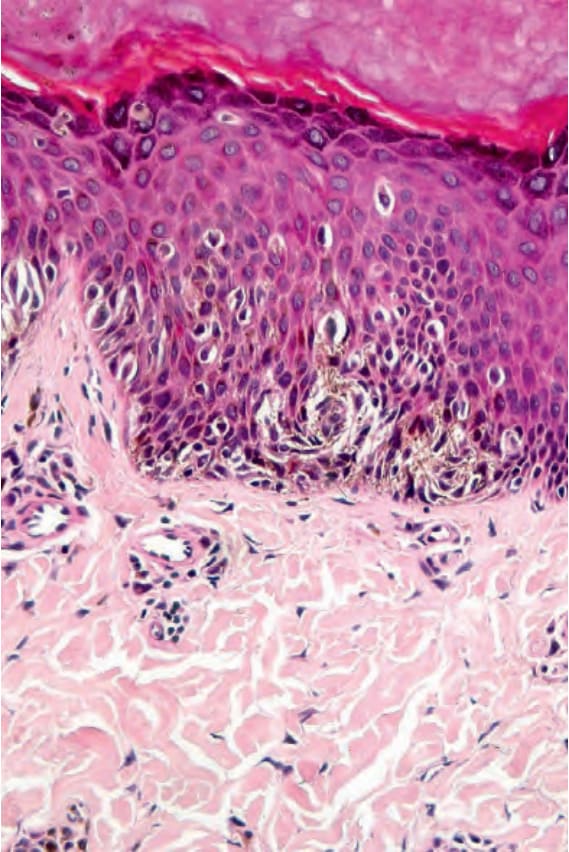
圖 25-84:肢端痣 (acral nevus):佩吉特樣擴散 (pagetoid spread)(尤其在病變中央)常見,不應被誤判為提示惡性。注意樹突狀細胞 (dendritic cell) 族群。
Fig. 25.84 Acral nevus: pagetoid spread (particularly over the center of the lesion) is common and should not be misinterpreted as implying malignancy. Note the dendritic cell population.

圖 25-85:斑痣 (nevus spilus):在背景界線清楚的較淡病變內可見重度色素沉著的斑 (macules)。From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
Fig. 25.85 Nevus spilus: heavily pigmented macules are present within a background circumscribed paler lesion. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 25-86:斑痣 (nevus spilus):此病人的病變呈節段性分布 (segmental distribution)。此類病變與黑色素瘤 (melanoma) 發生風險增加相關。By courtesy of the Institute of Dermatology, London, UK.
Fig. 25.86 Nevus spilus: in this patient, the lesion has a segmental distribution. This type of lesion is associated with an increased risk of developing melanoma. By courtesy of the Institute of Dermatology, London, UK.