Acral nevus
Acral nevus
Clinical features Acral palmar and plantar nevi may be symmetrical, well circumscribed, and identical to banal melanocytic or congenital nevi as seen at any other site, or they may be asymmetrical, poorly circumscribed, and a source of diagnostic difficulty, both clinically and pathologically.1–5 Acral nevi are more common in skin-of-color patients and patients with darker Fitzpatrick types than in whites.6
The second category (acral nevus), also sometimes known as atypical acral nevus, usually is not distinctive clinically, presenting as a less than 1.0-cm uniformly pigmented dark brown to black macule or papule with irregular and sometimes indistinct margins (Figs 25.79 and 25.80).1,5,7 Similar lesions may also be found on the dorsal surfaces of the hands, feet, and digits, under the nails, and on the knees and elbows.5 Development of
1255 Acral nevus
eruptive acral nevi on the sole of the foot has been reported in children following chemotherapy for acute lymphoblastic leukemia.8,9
Acral nevi have distinctive features on dermoscopy, which are influenced by their anatomic position.9–12 The most common dermoscopic feature represents the parallel furrow pattern and is seen in the majority of acral nevi occurring on non-arch and non weight-bearing parts of the foot.9,13 In contrast, acral nevi on the arch of the foot typically display lattice-like pattern, while those on weight-bearing surfaces depict fibrillary or filamentous patterns.9–12
Histologic features Acral (atypical) nevus is characterized by a circumscribed and usually symmetrical, lentiginous and nested, often continuous, melanocytic proliferation along the dermal–epidermal junction (Figs 25.81 and 25.82).4,5,7,14–17 The nests are commonly variable in size and often vertically oriented. A retraction artifact separating them from the adjacent keratinocytes is a characteristic feature. The rete ridges may be elongated and narrowed. The nevus cells have conspicuous pale-staining cytoplasm and hyperchromatic to vesicular nuclei, sometimes showing cytological atypia (usually mild) (Fig. 25.83). Nucleoli may be conspicuous. Mild to moderate pagetoid spread is not uncommonly present, particularly in the center of the nevus. Sometimes pagetoid spread can be very marked and involve almost the entire lesion – such melanocytic proliferation is generally referred to as a melanocytic acral
nevus with intraepidermal ascent of cells (MANIAC) (Fig. 25.84).5,7,15 As a result, spotty pigmentation is frequently evident in the stratum corneum.18 In addition, melanocytes along the dermal–epidermal junction frequently display dendritic morphology. A characteristic feature of acral nevus is transepidermal elimination of nests.4,15 Involvement of eccrine ducts by nests of melanocytes is not infrequent, but is usually limited to upper portions of the ducts.19 Pigmentary incontinence is generally present, and there may be mild
1256 Melanocytic nevi
fibrosis, rarely accompanied by a sparse lymphocytic infiltrate. Superficial dermal fibrosis is more prominent in lesions from weight-bearing areas such as the soles and should not be interpreted as regression. The dermal component matures with depth and lacks mitotic activity.
Differential diagnosis Atypical acral nevus may be distinguished from an acral dysplastic nevus by the absence of a shoulder, dusty pigmentation, and bridging, in addition to lamellar and eosinophilic fibrosis. A host inflammatory response is generally absent in acral nevi. It differs from acral lentiginous melanoma by the absence of irregular epidermal acanthosis, severe cytological atypia, mitotic activity, and by maturation of the dermal component when present.16 The presence of a dense lymphocytic infiltrate is highly suspicious for melanoma and should prompt careful examination of additional sections for confirmatory features.4
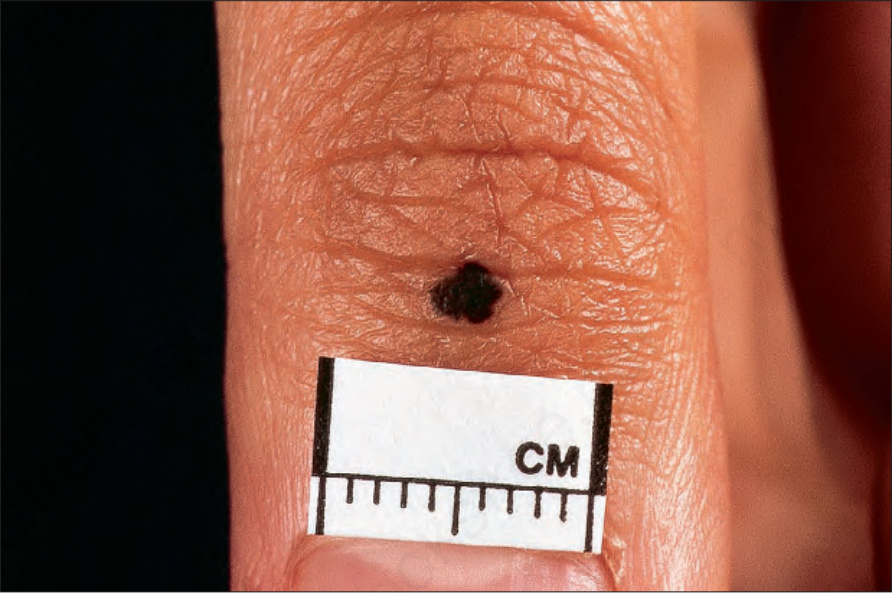
Fig. 25.79 Acral nevus: note the intense pigmentation and irregular border. By courtesy of the Institute of Dermatology, London, UK.
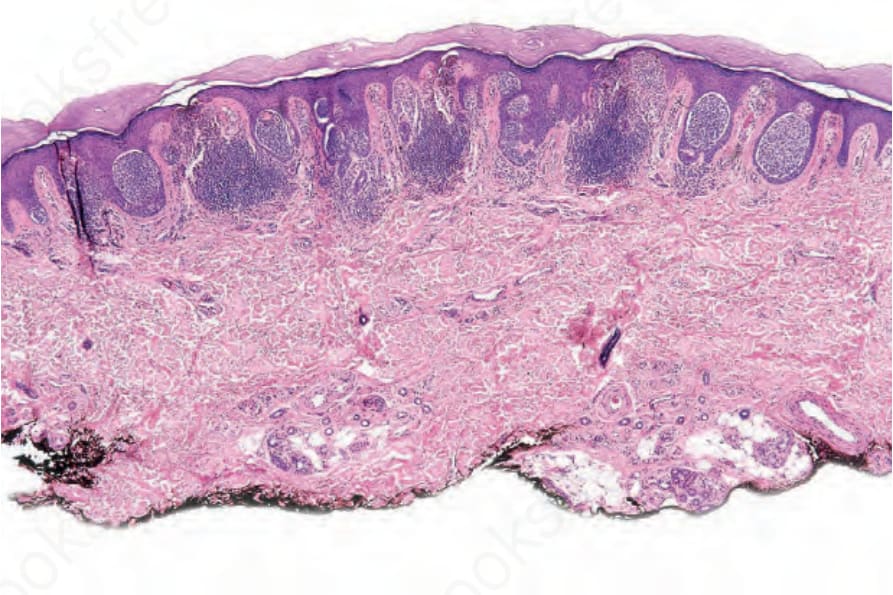
Fig. 25.81 Acral nevus: compound nevus showing vertically oriented junctional nests surrounded by a retraction artifact.
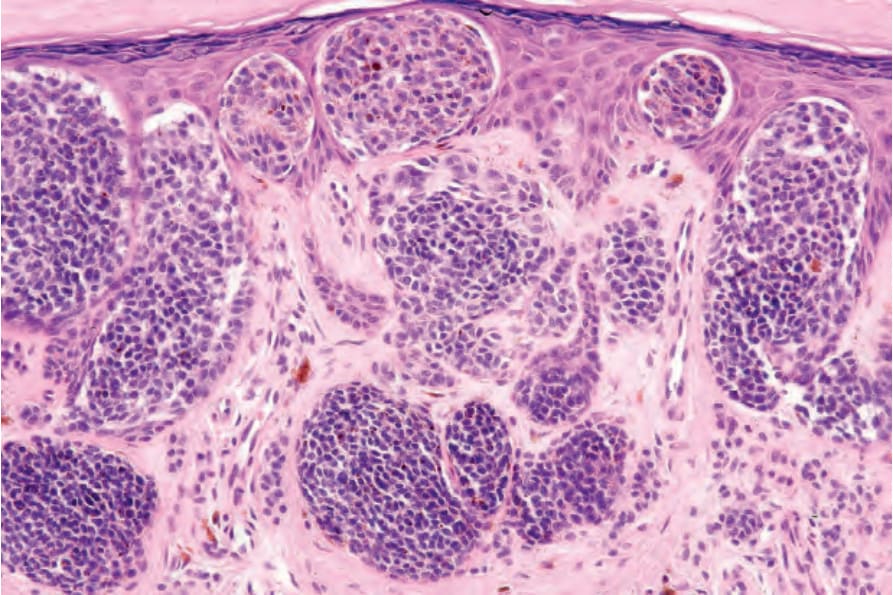
Fig. 25.82 Acral nevus: close-up view showing intraepidermal nests.
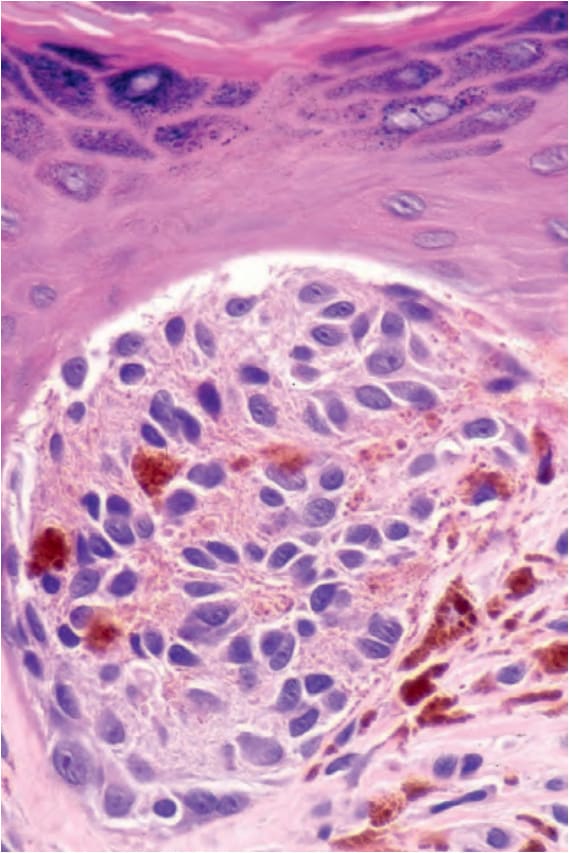
Fig. 25.83 Acral nevus: note the cytological atypia.
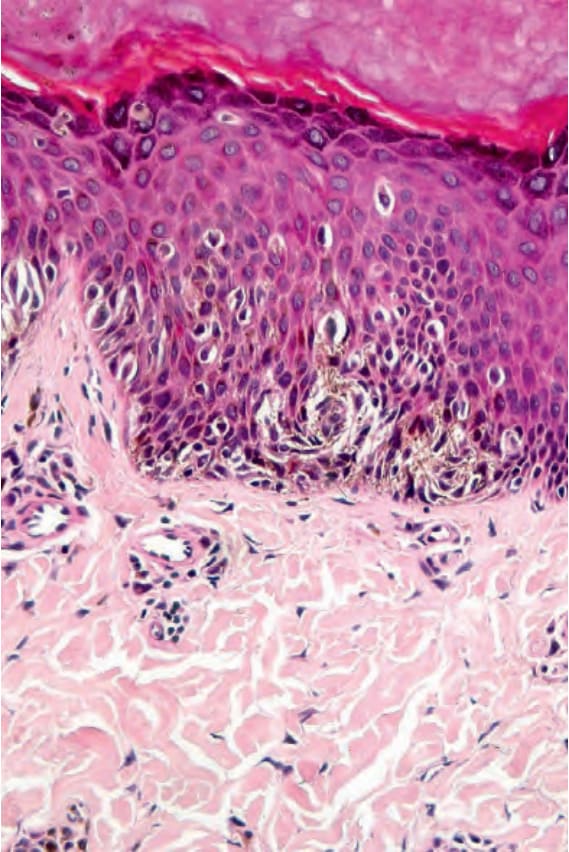
Fig. 25.84 Acral nevus: pagetoid spread (particularly over the center of the lesion) is common and should not be misinterpreted as implying malignancy. Note the dendritic cell population.

Fig. 25.85 Nevus spilus: heavily pigmented macules are present within a background circumscribed paler lesion. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 25.86 Nevus spilus: in this patient, the lesion has a segmental distribution. This type of lesion is associated with an increased risk of developing melanoma. By courtesy of the Institute of Dermatology, London, UK.