Becker 母斑 (Becker nevus)
臨床特徵 (Clinical Features)
- Becker 母斑 (Becker nevus,又稱 pigmented hairy epidermal nevus、Becker melanosis、melanosis neviformis Becker) 是一種雄性素依賴 (androgen-dependent) 的器官樣 (organoid) 病灶,於青春期後變得更為明顯。它並不常見,且兩性分布可能相等,惟在女性身上的病灶據說較男性更難以察覺。
- 雖然各種族皆可能受影響,但似乎好發於非白人族群。本病通常於第二個十年 (second decade) 出現,初期為一逐漸擴大、淡至深棕色的斑狀 (macular) 病灶,其後出現多毛 (hypertrichosis) (Fig. 25.17)。最常侵犯胸部、肩部或上臂,但病例可發生於皮膚表面任何部位。位於頭皮或臉部的病灶可伴隨頭皮毛髮或鬍鬚的不對稱生長。有時病灶為多發性,且曾有家族性病例記載。罕見情況下,Becker nevus 可為先天性。亦曾報告沿 Blaschko 線分布的線狀先天性 Becker nevus、橫跨背部、胸部與上臂的巨大雙側 Becker nevus,以及位於前胸與背部的對稱性雙側 Becker nevus。在一例臉部呈節段性 (segmental) 分布的病例中,亦曾報告口腔黏膜受侵犯。
- 特別重要的是,Becker nevus 偶可伴隨發育異常 (developmental anomalies),包括皮膚、肌肉與骨骼異常 — 即所謂的 pigmented hairy epidermal nevus syndrome(例如乳房與肢體發育不全、漏斗胸 (pectus excavatum)、脊柱裂 (spina bifida)、脊柱側彎 (scoliosis),以及皮下脂肪組織發育不全,僅舉最常見者)。曾有文獻記載一例頭皮病灶伴隨下方顱骨缺損的病例。
- Becker nevus 被認為是早期合子後 (postzygotic) 突變事件的結果,代表一種基因鑲嵌現象 (genetic mosaicism)。
組織病理特徵 (Histopathology)
- 其特徵相當輕微,包括輕度過度角化 (hyperkeratosis)、程度不一的棘層肥厚 (acanthosis),以及表皮突 (epidermal ridges) 的延長,並伴隨基底層區域 (basal region) 色素增加 (Figs 25.18–25.20)。其他變化可包括表皮變平、角栓塞 (keratotic plugging),以及兩三個相鄰延長之表皮突的融合。相較於未受侵犯的表皮,Becker nevus 的表皮顯示雄性素受體 (androgen receptors) 表現增加。黑色素細胞 (melanocytes) 數目常見增加,但無增殖活性 (proliferative activity) 的證據。淺層真皮可含
1240 Melanocytic nevi
組織反應,例如固定性藥物疹 (fixed drug eruptions)、光毒性反應 (phototoxic reactions)、lichen planus pigmentosus、紅斑性狼瘡 (lupus erythematosus),或 pigmented lichenoid keratosis。
病人通常為第六個十年 (sixth decade) 的成人,性別分布相等。病灶為單發或多發,且為近期發生。有趣的是,假黑色素細胞巢 (pseudomelanocytic nests) 亦曾在口腔黏膜中被報告。臨床與病理的相互對照 (clinicopathological correlation) 對於正確辨識這些病灶至關重要。
組織學特徵 (Histologic features) 假黑色素細胞巢代表沿真皮–表皮交界處 (dermal–epidermal junction) 分布、大小不規則且通常缺乏黏附性 (dyscohesive) 的角化細胞 (keratinocytes)、巨噬細胞 (macrophages) 與淋巴球 (lymphocytes) 之聚集。此外,巢內亦可出現孤立的黑色素細胞,但一般不超過兩個細胞。巢內的非黑色素細胞常含有細胞質內黑色素 (cytoplasmic melanin pigment)。表皮可顯示不規則棘層肥厚伴表皮突消失 (effacement of the rete ridges),但更常見的是萎縮。亦可見一密度不一的苔癬樣發炎細胞浸潤 (lichenoid inflammatory cell infiltrate),包含噬黑色素細胞 (melanophages)。在日光曝曬部位常見日光性彈力纖維變性 (solar elastosis)。
藉由免疫組織化學 (immunohistochemistry),巢內的非黑色素細胞可表現 Melan-A/MART-1 陽性,但通常 S100、tyrosinase 與 HMB-45 為陰性。一般認為 Melan-A/MART-1 陽性是黑色素細胞以外細胞之細胞質內黑色素體 (melanosomes) 的非特異性染色 (non-specific staining) 結果,因此代表一個潛在的診斷陷阱,可能導致誤診為黑色素細胞增殖,尤其是原位黑色素瘤 (melanoma in situ)。
鑑別診斷 (Differential diagnosis) 假黑色素細胞巢應與原位黑色素瘤 (melanoma in situ) 區別。後者典型上伴隨非典型黑色素細胞 (atypical melanocytes) 的雀斑樣 (lentiginous)、成巢 (nested) 與佩吉特樣 (pagetoid) 增殖。在可疑病例中,合併使用一組黑色素細胞標記 (melanocytic markers),包括 S100、SOX-10、microphthalmia transcription factor 與 tyrosinase,應有助於鑑別。臨床與病理的相互對照至關重要。
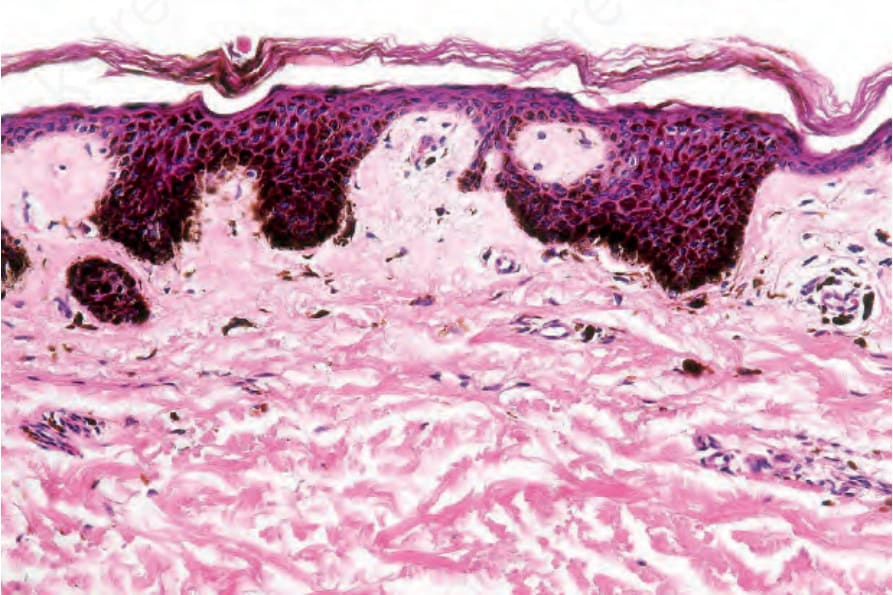
圖 25-16:墨點型雀斑痣 (ink spot lentigo):可見大量基底細胞色素過度沉著 (massive basal cell hyperpigmentation)。
Fig. 25.16 Ink spot lentigo: there is massive basal cell hyperpigmentation.

圖 25-17:Becker 母斑 (Becker nevus):此例顯示環繞肩部區域的特徵性分布。取自已故 N.P. Smith 醫師 (the Institute of Dermatology, London, UK) 的收藏。
Fig. 25.17 Becker nevus: this example shows a characteristic distribution around the shoulder region. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
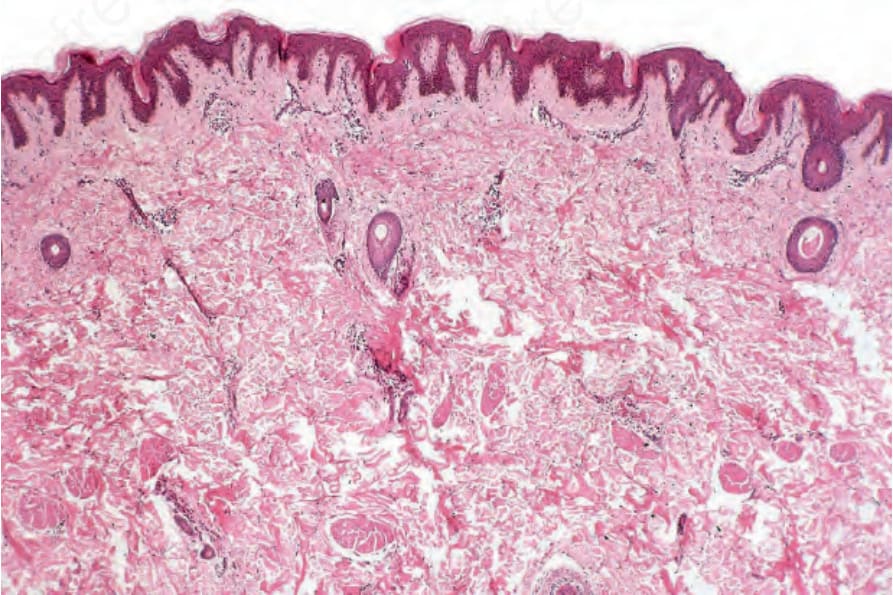
圖 25-18:Becker 母斑 (Becker nevus):在掃描放大倍率 (scanning magnification) 下,變化相當輕微,包括輕度過度角化 (slight hyperkeratosis) 與表皮突型態 (epidermal ridge pattern) 的強化。一極為輕微的慢性發炎細胞浸潤環繞乳頭真皮 (papillary dermis) 的血管。
Fig. 25.18 Becker nevus: at scanning magnification, the changes are subtle and comprise slight hyperkeratosis and accentuation of the epidermal ridge pattern. A very slight chronic inflammatory cell infiltrate surrounds the vessels of the papillary dermis.
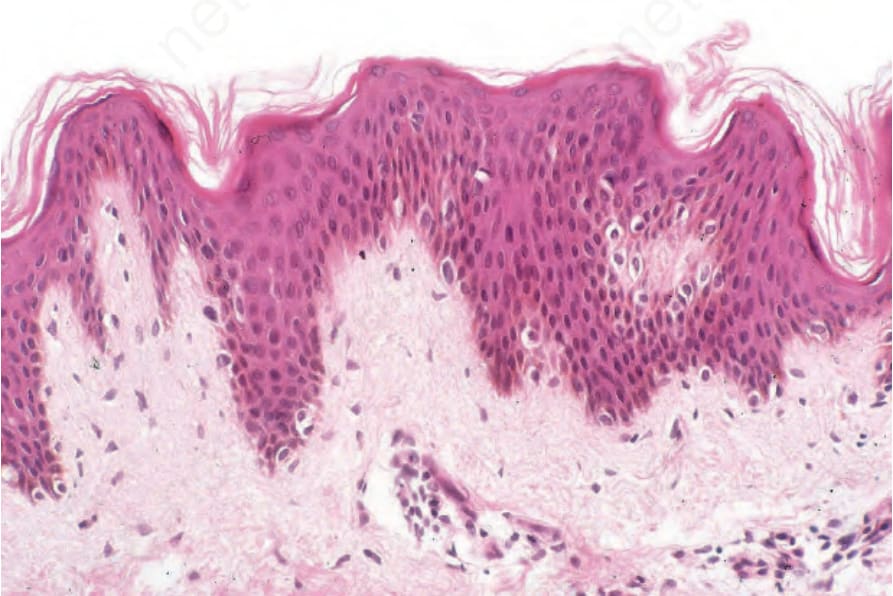
圖 25-19:Becker 母斑 (Becker nevus):可見輕度棘層肥厚 (mild acanthosis),並出現基底黑色素細胞 (basal melanocytes) 數目增加。此外,可見明顯的色素過度沉著 (hyperpigmentation),但無交界活性 (junctional activity)。
Fig. 25.19 Becker nevus: there is mild acanthosis and increased numbers of basal melanocytes are present. In addition, there is obvious hyperpigmentation, but no junctional activity.
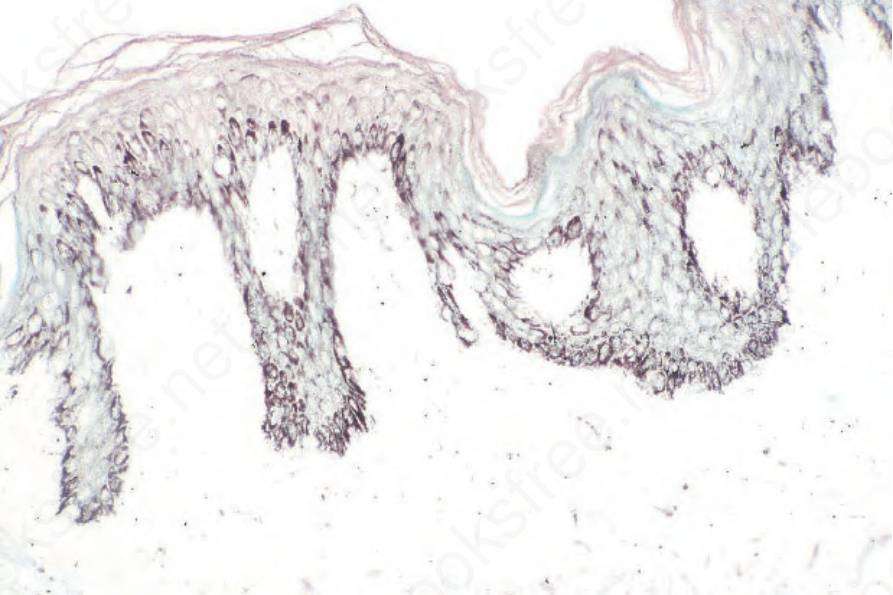
圖 25-20:Becker 母斑 (Becker nevus):色素增加可藉由 Masson-Fontana 反應而被強化。
Fig. 25.20 Becker nevus: the increased pigmentation may be accentuated by the Masson- Fontana reaction.