Becker nevus
Becker nevus
Clinical features Becker nevus (pigmented hairy epidermal nevus, Becker melanosis, melanosis neviformis Becker) is an androgen-dependent organoid lesion that becomes more prominent after puberty.1 It is uncommon and probably shows an equal sex distribution, although lesions in females are said to be
1239 Becker nevus
described.15 Of particular importance is the occasional association of Becker nevus with developmental anomalies, including cutaneous, muscular, and skeletal anomalies – the so-called pigmented hairy epidermal nevus syndrome (e.g., breast and limb hypoplasia, pectus excavatum, spina bifida, scoliosis, and hypoplasia of subcutaneous fatty tissue, to mention just the most common conditions).1,3,6,16–20 A case in which a scalp lesion occurred with underlying loss of cranium has been documented.21
more difficult to appreciate than in males.1 While all races may be affected, there appears to be a predilection for non-whites.2 It usually presents in the second decade, initially as a light to dark brown enlarging macular lesion, which subsequently shows hypertrichosis (Fig. 25.17).1,3–6 Although most frequently the chest, shoulder, or upper arm are involved, examples have occurred everywhere on the skin surface. Lesions on the scalp or face can be associated with asymmetrical growth of scalp hair or beard.7,8 Sometimes they are multiple, and familial examples have been recorded.9 Rarely, Becker nevus may be congenital.10 Linear distribution of congenital Becker nevus following Blaschko lines, giant bilateral Becker nevus over the back, chest and upper arms, as well as symmetrical bilateral Becker nevus on the anterior chest and back have also been reported.11–14 Involvement of oral mucosa in a case with segmental distribution on the face has also been
Becker nevus is thought to be the consequence of an early postzygotic mutational event representing a genetic mosaicism.22
Histologic features The features are subtle, comprising slight hyperkeratosis, variable acanthosis, and elongation of the epidermal ridges, accompanied by increased pigmentation in the basal region (Figs 25.18–25.20). Additional changes can include flattening of the epidermis, keratotic plugging, and fusion of two or three neighboring elongated rete ridges.23 In contrast to uninvolved epidermis, the epidermis of Becker nevus shows increased expression of androgen receptors.23 Melanocytes often appear increased in number, but there is no evidence of proliferative activity.24 The superficial dermis may contain
1240 Melanocytic nevi
tissue reactions, for example, fixed drug eruptions, phototoxic reactions, lichen planus pigmentosus, lupus erythematosus, or pigmented lichenoid keratosis.1–3
Patients are usually adults in their sixth decade of life with equal gender distribution.5 The lesions are either solitary or multiple and of recent onset. Interestingly, pseudomelanocytic nests have also been reported in the oral mucosa.5 Clinicopathological correlation is essential for correct recognition of these lesions.
Histologic features Pseudomelanocytic nests represent irregularly sized and usually dyscohesive collections of keratinocytes, macrophages, and lymphocytes along the dermal–epidermal junction.1,2 In addition, isolated melanocytes can also be present within the nests, but they generally do not exceed two cells.3 Nonmelanocytic cells within the nests frequently contain cytoplasmic melanin pigment. The epidermis can display irregular acanthosis with effacement of the rete ridges, but it is more frequently atrophic. A variably dense lichenoid inflammatory cell infiltrate including melanophages is also seen. Solar elastosis is commonly seen on sun-exposed sites.
By immunohistochemistry, nonmelanocytic cells within the nests can express Melan-A/MART-1 positivity, but are usually S100, tyrosinase, and HMB-45 negative.1–3 It is believed that Melan-A/MART-1 positivity is the result of non-specific staining of melanosomes within the cytoplasm of cells other than melanocytes, thus representing a potential diagnostic pitfall that may lead to a misdiagnosis of a melanocytic proliferation, in particular, melanoma in situ.
Differential diagnosis Pseudomelanocytic nests should be distinguished from melanoma in situ. The latter is typically associated with lentiginous, nested, and pagetoid proliferation of atypical melanocytes. A combination of melanocytic markers, including S100, SOX-10, microphthalmia transcription factor, and tyrosinase, should aid in distinction in dubious cases. Clinicopathological correlation is essential.
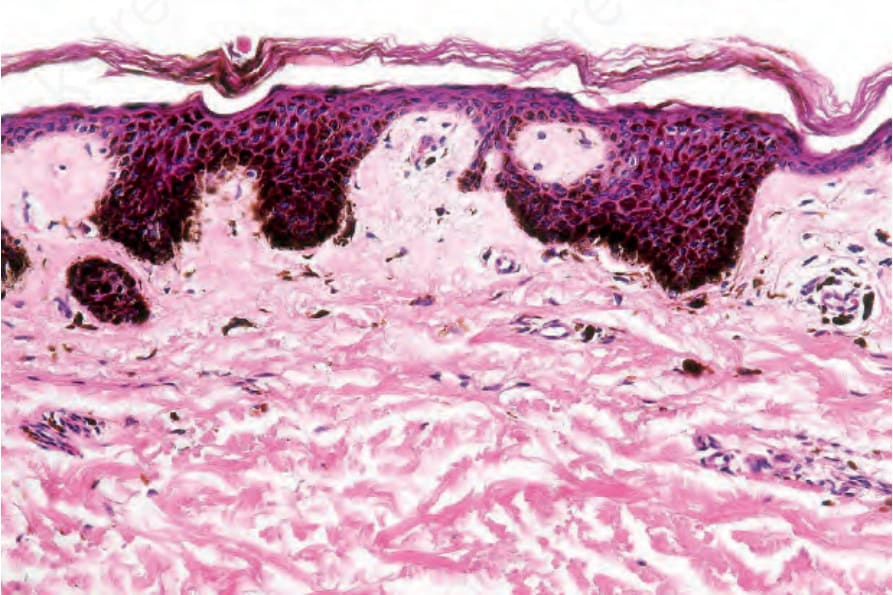
Fig. 25.16 Ink spot lentigo: there is massive basal cell hyperpigmentation.

Fig. 25.17 Becker nevus: this example shows a characteristic distribution around the shoulder region. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
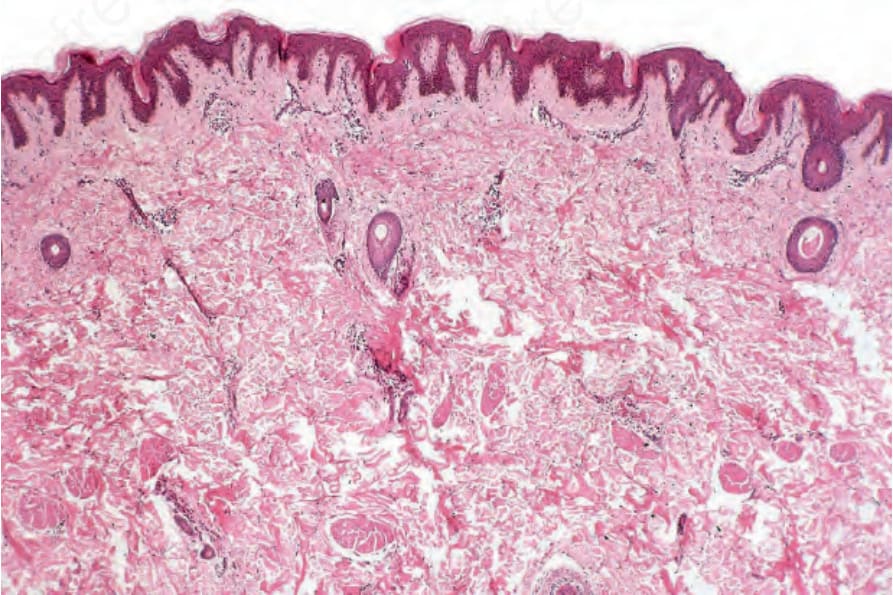
Fig. 25.18 Becker nevus: at scanning magnification, the changes are subtle and comprise slight hyperkeratosis and accentuation of the epidermal ridge pattern. A very slight chronic inflammatory cell infiltrate surrounds the vessels of the papillary dermis.
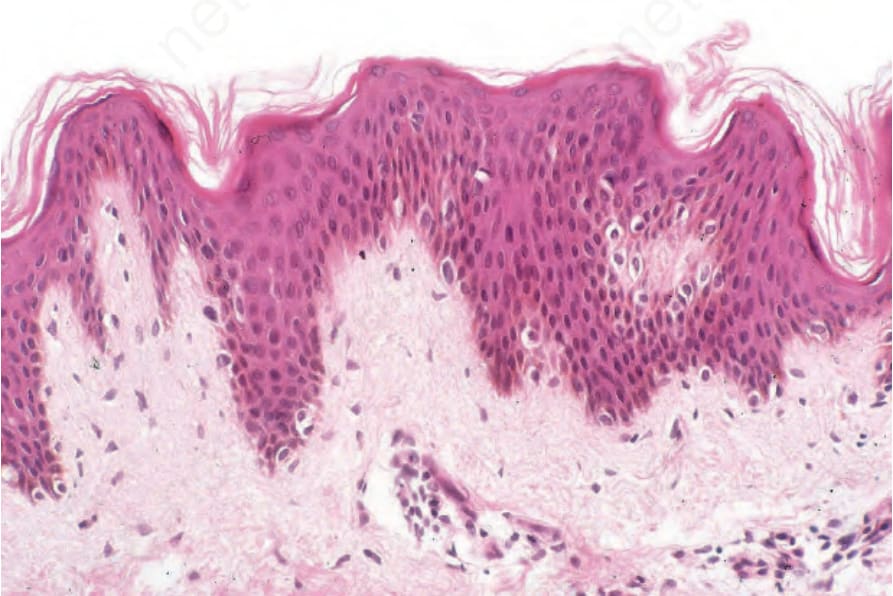
Fig. 25.19 Becker nevus: there is mild acanthosis and increased numbers of basal melanocytes are present. In addition, there is obvious hyperpigmentation, but no junctional activity.
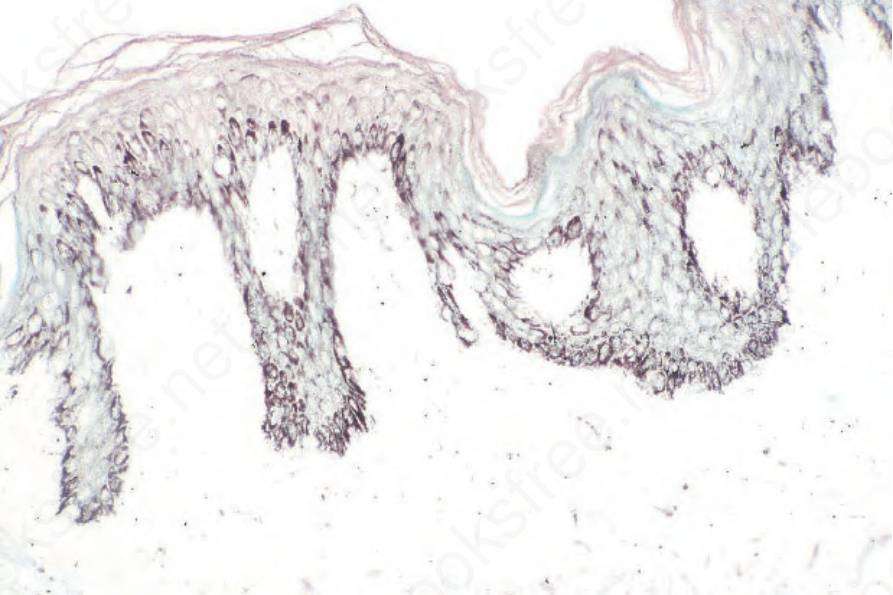
Fig. 25.20 Becker nevus: the increased pigmentation may be accentuated by the Masson- Fontana reaction.