基底細胞癌 (Basal cell carcinoma)
基底細胞癌 (Basal cell carcinoma)
臨床特徵 發生於甲單位 (nail unit) 的基底細胞癌 (basal cell carcinoma) 非常罕見,文獻報告少於 25 例。診斷時的平均年齡為 66.3 歲。本病灶發生於手指(主要為拇指)的頻率約為腳趾的三倍。其略偏好男性。約 50% 的病例可見甲板 (nail plate) 受侵犯(包括兩例伴有縱向黑甲 longitudinal melanonychia)。甲周皺襞 (periungual folds) 受侵犯與潰瘍 (ulceration) 為常見表現。本腫瘤在臨床上可能類似慢性甲溝炎 (chronic paronychia)、化膿性肉芽腫 (pyogenic granuloma)、SCC、無色素性黑色素瘤 (amelanotic melanoma)、外傷、黴菌或細菌感染,以及濕疹 (eczema)。診斷前的病程長短自 1 年至 40 年不等。正確診斷需要切片 (biopsy)。
組織學特徵 甲單位的 basal cell carcinoma 具有與身體其他部位皮膚病灶完全相同的組織學特徵。已有表淺型 (superficial)、結節型 (nodular)、囊性 (cystic)、色素性 (pigmented) 與浸潤型 (infiltrative) 等變異型的報告。
甲器之鱗狀細胞癌或類表皮癌 (Squamous cell or epidermoid carcinoma of the nail apparatus)
臨床特徵 原位 SCC(Bowen 氏病 Bowen disease)與侵襲性 SCC 為甲器 (nail apparatus) 最常見的腫瘤。
SCC 曾於 13 至 90 歲的個體中被報告,發生率以 50–69 歲年齡層為最高。具男性優勢(比例為 2 : 1)。手指甲,尤其是右側食指與右側中指,受侵犯的頻率顯著高於腳趾甲。本腫瘤生長緩慢,自發病至診斷的病程自數月至 30 年不等。在近期一個大型病例系列中,最常見的臨床徵象為甲下角化過度 (subungual hyperkeratosis)、甲剝離 (onycholysis)、滲液 (oozing) 與甲板破壞 (Fig. 23.53)。多數病例屬疣狀型 (warty type)。這些容易誤導的臨床表現經常是診斷延誤的原因。
A
B
1148 Diseases of the nails
過去數年間,甲器的原位 SCC 因下列數項原因而成為關注焦點:
• 對其發生頻率及其潛在多指 (polydactylous) 侵犯之認識日益增加,
• 發現新的臨床表現,例如縱向黑甲 (longitudinal melanonychia)、類纖維角化瘤樣生長 (fibrokeratoma-like growth)、縱向紅甲 (longitudinal erythronychia),以及類色素性甲基質瘤樣特徵 (pigmented onychomatricoma-like features),
• 發現生殖器致癌性 HPV 為一項病因。雖然潰瘍、出血或結節形成通常指示該癌已屬侵襲性,但甲單位的原位與侵襲性類表皮癌 (epidermoid carcinoma) 在臨床上常難以區別。可能會察覺到局部疼痛,但通常不存在。骨侵犯見於少於 20% 的侵襲性甲器 SCC 患者,其特徵為下方骨之骨膜增厚 (periosteal thickening) 與反應性硬化 (reactive sclerosis),係因病程拖延所致。轉移罕見。
在一個 2007 年發表的病例系列中,SCC 在初次就醫時僅有 29% 的病例被懷疑。甲癬 (onychomycosis) 與疣 (warts) 為最常見的診斷。當進行黴菌培養時,三分之一的病例呈陽性,更增添了混淆。診斷的關鍵在於組織學檢查,這需要適當的手術切片。
致病機轉與組織學特徵 致癌性生殖器 HPV(主要為 HPV 16)已在約 60% 至 80% 的甲器原位或侵襲性 SCC 中被報告。已有人提出生殖器—指 (genital-digital) 傳播的可能性。X 光、砷 (arsenic)、外傷、慢性甲溝炎 (chronic paronychia),以及先天性角化不良 (dyskeratosis congenita) 為其他病因。
與 23.57)。多數似源自既存的 Bowen disease,這或許可解釋其相對良好的預後。浸潤深度(定義為自基底層至最深處癌細胞的距離)範圍自 0.3 至 2.6 mm(平均 1.1 mm)。
鑑別診斷 甲器的侵襲性 SCC 不應與甲下類表皮包涵 (subungual epidermoid inclusions)、甲下角化棘皮瘤 (subungual keratoacanthoma)、疣狀癌 (verrucous carcinoma) 及惡性甲鞘瘤 (malignant onycholemmal tumors) 混淆。汗孔癌 (porocarcinoma) 與轉移亦可能進入鑑別診斷。
甲單位 Bowen disease 的組織學特徵與皮膚 Bowen 氏病完全相同。視臨床表現而定,病灶可位於甲基質 (nail matrix)、甲床 (nail bed),以及甲周溝與甲周皺襞 (periungual grooves and folds)。組織學變化常延伸至臨床受侵範圍之外,且檢體邊緣常受侵犯。上皮呈不規則增厚且排列紊亂,並顯示成熟障礙。可見角化不良細胞 (dyskeratotic cells)、具大型且形狀不規則細胞核的非典型角質細胞 (atypical keratinocytes)、壞死性角質細胞 (necrotic keratinocytes),以及散在的有絲分裂象 (mitotic figures) (Figs 23.54 與 23.55)。可見挖空細胞 (koilocytes)。組織學診斷通常容易,但早期病灶若僅有輕微結構紊亂、罕見的角化不良細胞,以及輕至中度非典型,則可能具挑戰性。
雖然原位 SCC 在甲單位較其他皮膚部位更可能轉變為侵襲性,但侵襲性甲癌較不易轉移。甲器的侵襲性 SCC 具有與身體其他部位皮膚相同的特徵,但鮮少被詳盡描述 (Figs 23.56
甲下角化棘皮瘤 (subungual keratoacanthoma) 應根據其臨床、影像學與病理特徵診斷(見前述)。使用 p53 與 Ki-67 免疫組化有助於區別甲下角化棘皮瘤與甲下鱗狀癌。在甲下角化棘皮瘤中,p53 表現罕見,若有也很微弱,與甲下癌之強烈瀰漫性染色形成對比。此外,在甲下角化棘皮瘤中,Ki-67 表現侷限於基底層與基底上層。在鱗狀癌中,染色型態較為瀰漫,遍及整個腫瘤團塊。核因子 kappa B1(在角化棘皮瘤中被放大)亦可作為診斷的輔助。
疣狀癌 (verrucous carcinoma)(兔穴狀癌 carcinoma cuniculatum)為一種罕見、高度角化、低惡性度的 SCC 變異型 (Fig. 23.58)。甲器已有十八例的報告。
1149 Fibroepithelial tumors
該腫瘤同時具有外生 (exophytic) 與內生 (endophytic) 成分。上皮呈顯著角化過度且肥厚,伴有寬大的球狀突起延伸至深部真皮 (Fig. 23.59)。其由大型、分化良好、具毛玻璃樣 (ground-glass) 細胞質的角質細胞組成 (Fig. 23.60)。偶可見角化不良細胞。有絲分裂數目稀少且侷限於基底層。
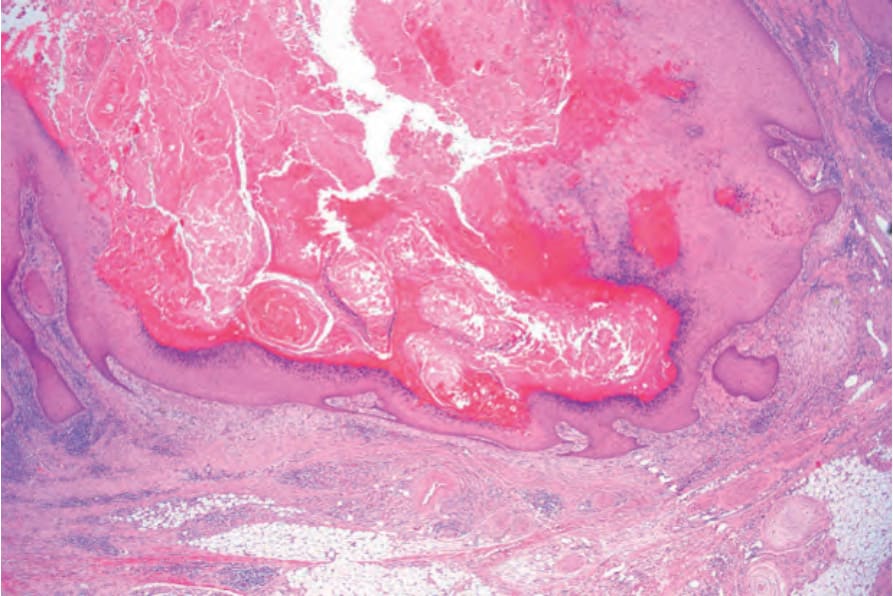
圖 23-51:角化棘皮瘤 (keratoacanthoma):掃描視野。注意充滿角質的火山口狀凹陷 (keratin-filled crater)。
Fig. 23.51 Keratoacanthoma: scanning view. Note the keratin-filled crater.
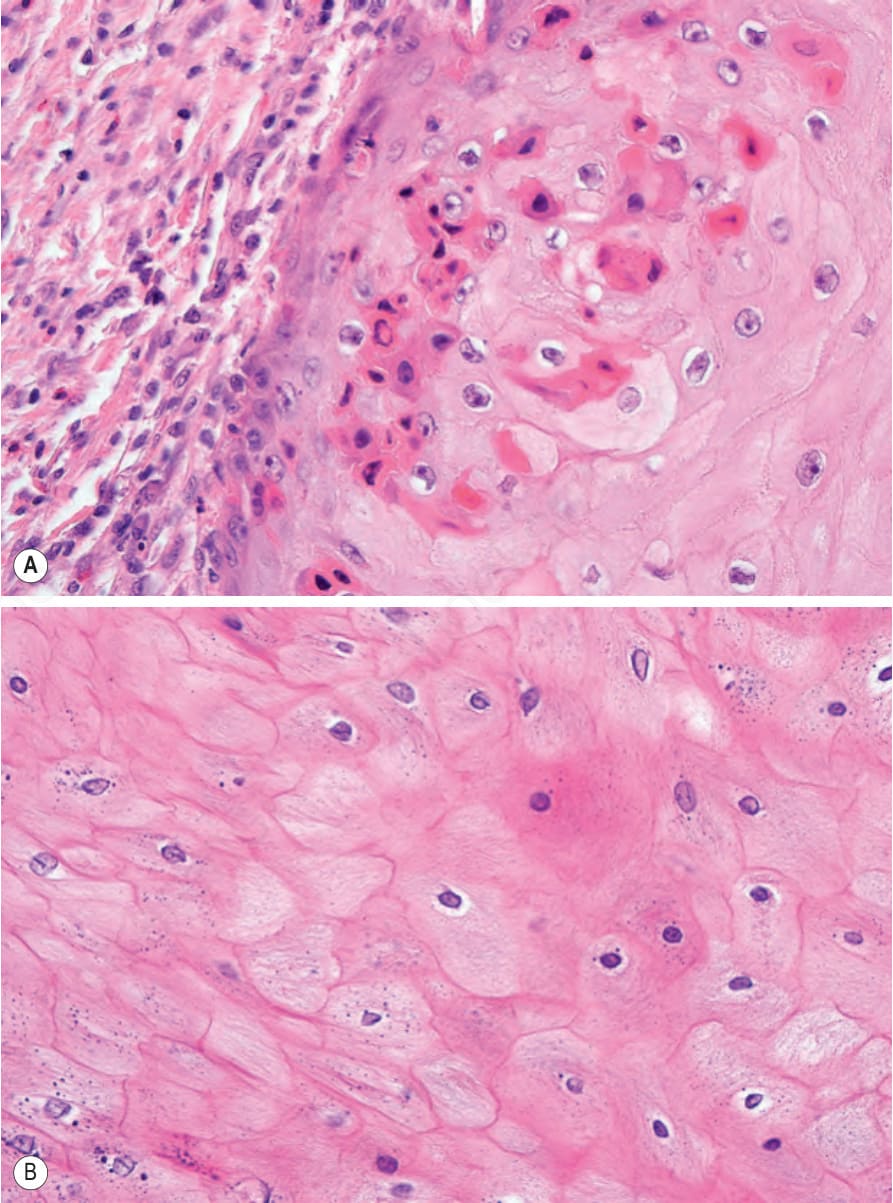
圖 23-52:(A, B) 角化棘皮瘤 (keratoacanthoma):分化鱗狀上皮 (differentiated squamous epithelium) 的高倍視野。無細胞學非典型 (cytological atypia)。角化不良細胞 (dyskeratotic cells) 顯著。
Fig. 23.52 (A, B) Keratoacanthoma: high-power view of differentiated squamous epithelium. There is no cytological atypia. Dyskeratotic cells are conspicuous.

圖 23-53:原位鱗狀細胞癌 (in situ squamous cell carcinoma):甲已被疣狀病灶 (warty lesion) 取代。
Fig. 23.53 In situ squamous cell carcinoma: the nail has been replaced by a warty lesion.
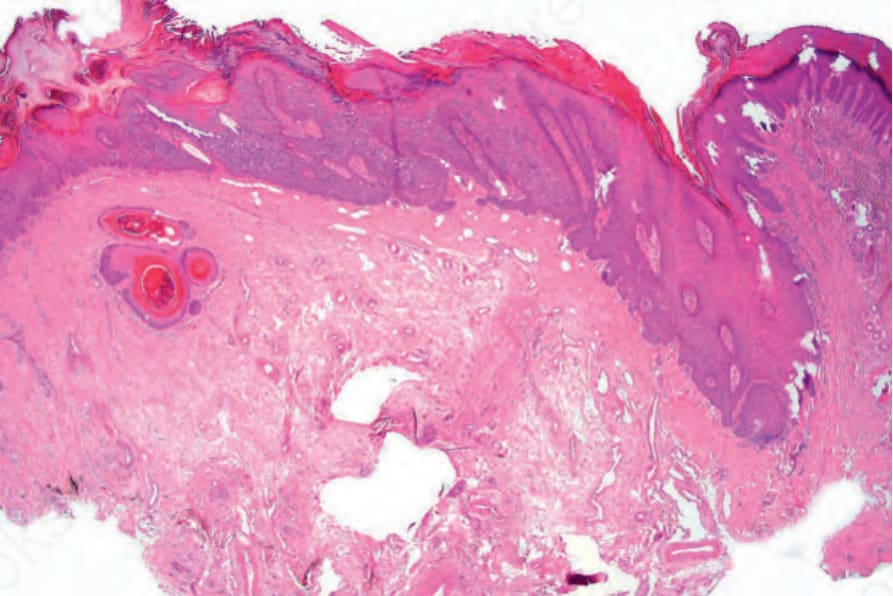
圖 23-54:原位鱗狀細胞癌 (in situ squamous cell carcinoma):上皮增厚,即使在此放大倍率下亦有明顯的非典型 (atypia)。
Fig. 23.54 In situ squamous cell carcinoma: the epithelium is thickened and even at this magnification there is obvious atypia.
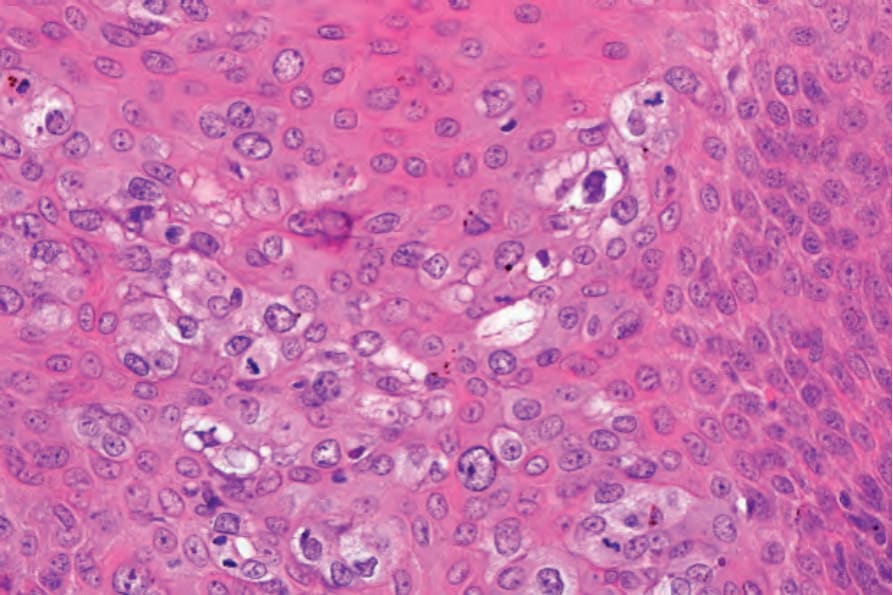
圖 23-55:原位鱗狀細胞癌 (in situ squamous cell carcinoma):高倍視野顯示多形性 (pleomorphism) 與有絲分裂活性 (mitotic activity)。
Fig. 23.55 In situ squamous cell carcinoma: high-power view showing pleomorphism and mitotic activity.
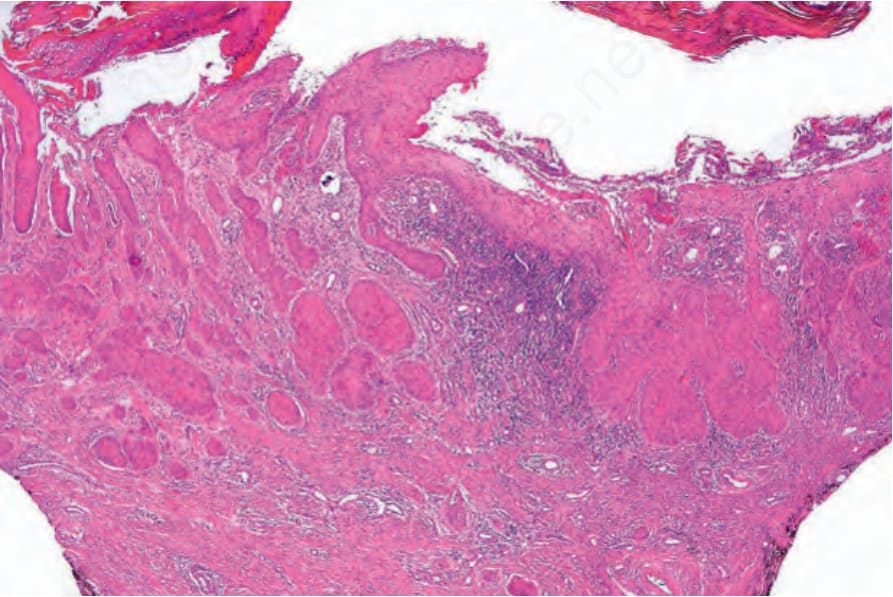
圖 23-56:侵襲性鱗狀細胞癌 (invasive squamous cell carcinoma):低倍視野。
Fig. 23.56 Invasive squamous cell carcinoma: low-power view.
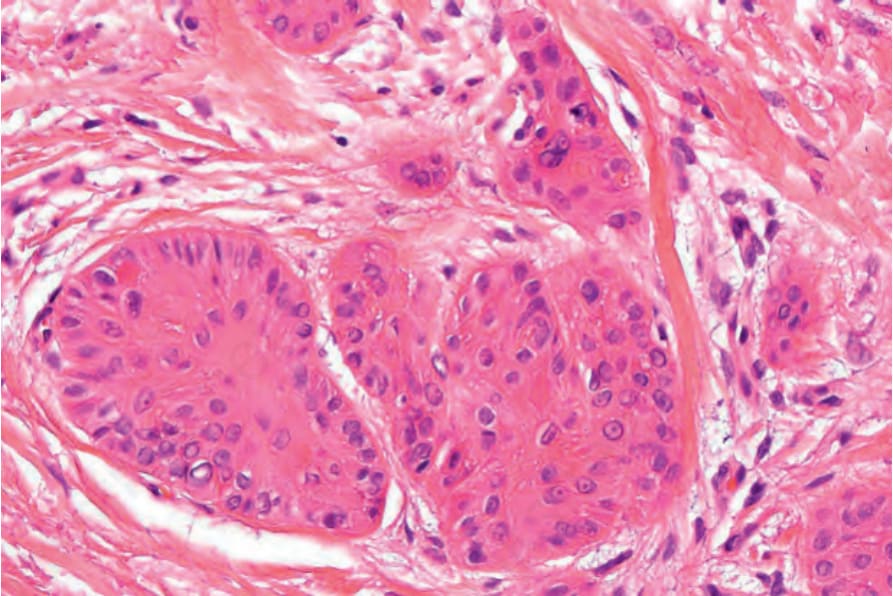
圖 23-57:侵襲性鱗狀細胞癌 (invasive squamous cell carcinoma):分化良好的鱗狀細胞癌巢 (nests) 存在於真皮深處。
Fig. 23.57 Invasive squamous cell carcinoma: nests of well-differentiated squamous cell carcinoma are present deep in the dermis.

圖 23-58:疣狀癌 (verrucous carcinoma):典型例,顯示疣狀、角化過度的表面。Courtesy of P. Gheeraert, MD, Hôpital Brugmann, Université Libre de Bruxelles, Belgium.
Fig. 23.58 Verrucous carcinoma: typical example showing the warty, hyperkeratotic surface. Courtesy of P. Gheeraert, MD, Hôpital Brugmann, Université Libre de Bruxelles, Belgium.
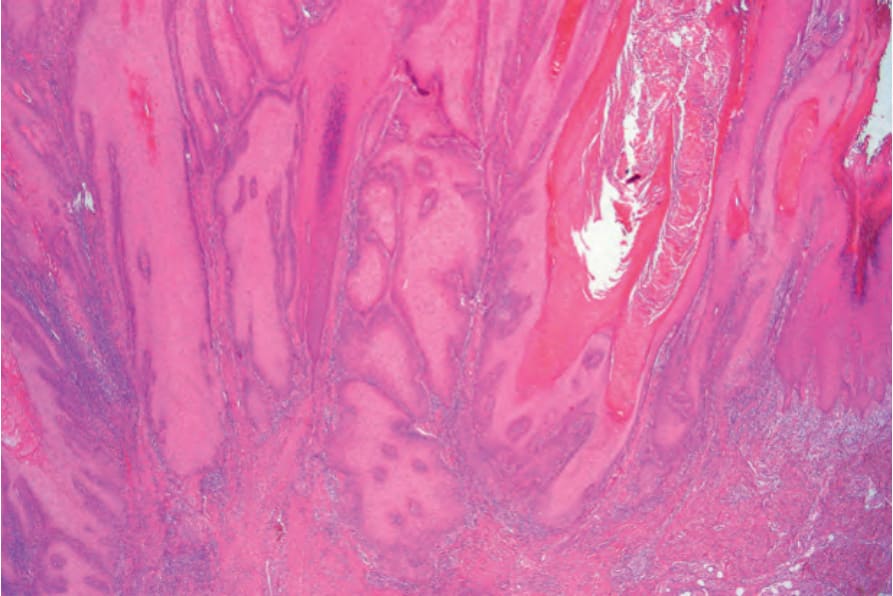
圖 23-59:疣狀癌 (verrucous carcinoma):低倍視野顯示深部穿透的寬大球狀生長型態 (broad bulbous growth pattern)。Courtesy of C. Deprez, MD, Hôpital Brugmann, Université Libre de Bruxelles, Belgium.
Fig. 23.59 Verrucous carcinoma: low-power view showing the deeply penetrating broad bulbous growth pattern. Courtesy of C. Deprez, MD, Hôpital Brugmann, Université Libre de Bruxelles, Belgium.
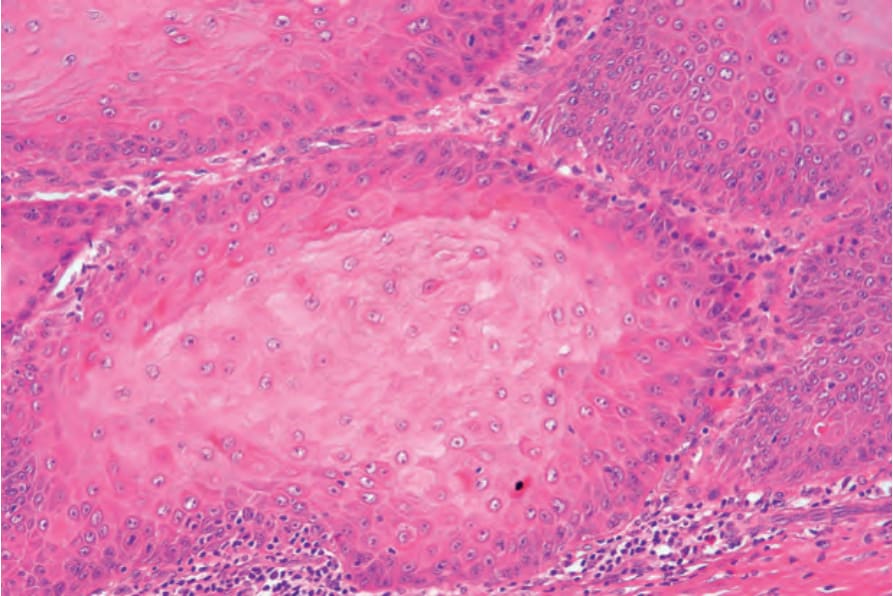
圖 23-60:疣狀癌 (verrucous carcinoma):高倍視野顯示典型的毛玻璃樣上皮 (ground-glass epithelium)。注意無細胞學非典型 (cytological atypia)。Courtesy of C. Deprez, MD, Hôpital Brugmann, Université Libre de Bruxelles, Belgium.
Fig. 23.60 Verrucous carcinoma: high-power view showing typical ground-glass epithelium. Note that there is no cytological atypia. Courtesy of C. Deprez, MD, Hôpital Brugmann, Université Libre de Bruxelles, Belgium.