Basal cell carcinoma
Basal cell carcinoma
Clinical features Basal cell carcinoma arising in the nail unit is very rare, with fewer than 25 cases reported.1 Average age at diagnosis is 66.3 years. The lesion occurs almost three times as often on the fingers, mainly the thumb, than on the toes.2 It has a slight predilection for males.3 Nail plate involvement (including two cases with longitudinal melanonychia) was observed in about 50% of cases. Involvement of the periungual folds and ulceration are common findings. The tumor may clinically mimic chronic paronychia, pyogenic granuloma, SCC, amelanotic melanoma, trauma, mycotic or bacterial infection, and eczema. Duration prior to diagnosis has ranged from 1 to 40 years.1 Correct diagnosis requires a biopsy.
Histologic features Basal cell carcinoma of the nail unit has histologic features identical to those of skin lesions occurring elsewhere. Superficial, nodular, cystic, pigmented, and infiltrative variants have been reported.1
Squamous cell or epidermoid carcinoma of the nail apparatus
Clinical features In situ SCC (Bowen disease) and invasive SCC are the most common neoplasms of the nail apparatus.1
SCC has been reported in individuals between 13 and 90 years, the incidence being highest in the 50–69 year range.2,3 There is a male predominance (ratio 2 : 1).4 Fingernails, particularly right index and right long fingers, are significantly more frequently affected than toenails.4 The tumor grows slowly and the duration from onset to the time of diagnosis varies from several months to 30 years.3 In a large recent series, the commonest clinical signs were subungual hyperkeratosis, onycholysis, oozing, and nail plate destruction (Fig. 23.53). Most cases were of the warty type.4 These misleading clinical appearances are frequently responsible for delayed diagnosis.
A
B
1148 Diseases of the nails
Over the past years, in situ SSC of the nail apparatus has become the focus of interest for several reasons3:
• increasing awareness of its frequency and of its potential polydactylous involvement,1,5
• identification of new clinical presentations such as longitudinal melanonychia,6 fibrokeratoma-like growth,2,7,8 longitudinal erythronychia,9 and pigmented onychomatricoma-like features,10
• the discovery of genital oncogenic HPV as an etiological factor. Although the presence of ulceration, bleeding, or nodule formation usually indicates that the carcinoma is invasive,11 in situ and invasive epidermoid carcinomas of the nail unit are often difficult to differentiate clinically. Localized pain may be noted11 but is usually absent.12 Bone involvement is seen in less than 20% of patients3 with invasive SCC of the nail apparatus and is characterized by periosteal thickening and reactive sclerosis of the underlying bone, due to a protracted course.13 Metastases are rare.4,6,14
In a series published in 2007, SCC was suspected at first medical examination in only 29% of cases. Onychomycosis and warts were the most frequent causes of diagnoses. When mycological cultures were made, they were found positive in one-third of cases, adding to the confusion.12 The key to diagnosis is histologic examination, which requires an appropriate surgical biopsy.
Pathogenesis and histologic features Oncogenic genital HPVs (mainly HPV 16) have been reported in about 60% to 80% of in situ or invasive SCC of the nail apparatus.3,6,14 The possibility of genital-digital transmission has been suggested. X-rays, arsenic, trauma, chronic paronychia, and dyskeratosis congenita are other etiological factors.3
and 23.57).16 Most appear to arise in pre-existing Bowen disease, which may explain their relatively good prognosis.11 The depth of invasion, as defined by the distance from the basal layer to the deepest carcinoma cell, ranged from 0.3 to 2.6 mm (mean, 1.1 mm).12
Differential diagnosis Invasive SCC of the nail apparatus should not be confused with subungual epidermoid inclusions, subungual keratoacanthoma, verrucous carcinoma, and malignant onycholemmal tumors. Porocarcinoma17,18 and metastases19,20 may also enter the differential diagnosis.
The histologic features of Bowen disease of the nail unit are identical to those of Bowen diseases of the skin. Depending on the clinical presentation, the lesion may be located in the nail matrix, the nail bed, and the periungual grooves and folds. Histologic changes frequently extend beyond the area clinically involved, and specimen margins are often involved. The epithelium is irregularly thickened and disorganized, and shows impaired maturation. Dyskeratotic cells, atypical keratinocytes with large, irregularly shaped nuclei, and necrotic keratinocytes are observed as well as scattered mitotic figures (Figs 23.54 and 23.55). Koilocytes may be observed. Histologic diagnosis is usually easy, but early lesions with only slight architectural disorganization, rare dyskeratotic cells, and mild to moderate atypia may be challenging.
Although SCC in situ has a greater likelihood to become invasive in the nail unit than at other skin sites, invasive nail carcinoma is less likely to metastasize.15 Invasive SCC of the nail apparatus has identical features to that seen in the skin elsewhere but is rarely extensively described (Figs 23.56
Subungual keratoacanthoma should be diagnosed based on its clinical, radiological, and pathological features (see above). Use of p53 and Ki-67 immunohistochemistry can help distinguish subungual keratoacanthoma from subungual squamous carcinoma. In subungual keratoacanthoma, expression of p53 is rare and, if present, weak, contrasting with the strong diffuse staining in subungual carcinoma. Moreover, in subungual keratoacanthoma, expression of Ki-67 is restricted to the basal and suprabasal layer. In squamous carcinoma, the staining pattern is more diffuse, throughout the tumor mass.21,22 The nuclear factor kappa B1, which is amplified in keratoacanthoma, could also be used as an aid in diagnosis.22
Verrucous carcinoma (carcinoma cuniculatum) is a rare, highly keratinizing, low-grade variant of SCC (Fig. 23.58). Eighteen cases have been
1149 Fibroepithelial tumors
reported in the nail apparatus.21–31 The tumor has both exophytic and endophytic components. The epithelium is markedly hyperkeratotic and hypertrophic, with broad bulbous processes extending into the deep dermis (Fig. 23.59). It is composed of large, well-differentiated keratinocytes with ground-glass cytoplasm (Fig. 23.60). Occasional dyskeratotic cells may be seen. Mitoses are few in number and confined to the basal layers.32
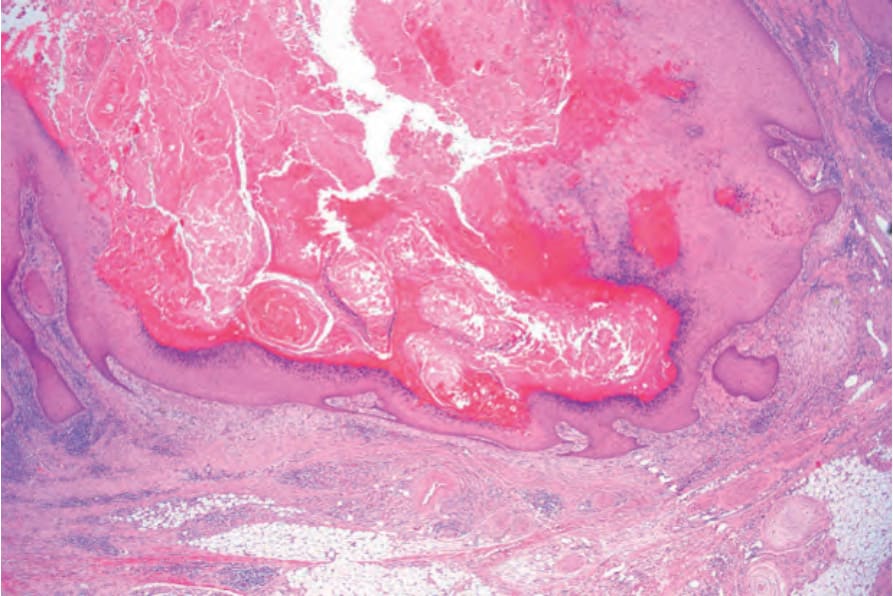
Fig. 23.51 Keratoacanthoma: scanning view. Note the keratin-filled crater.
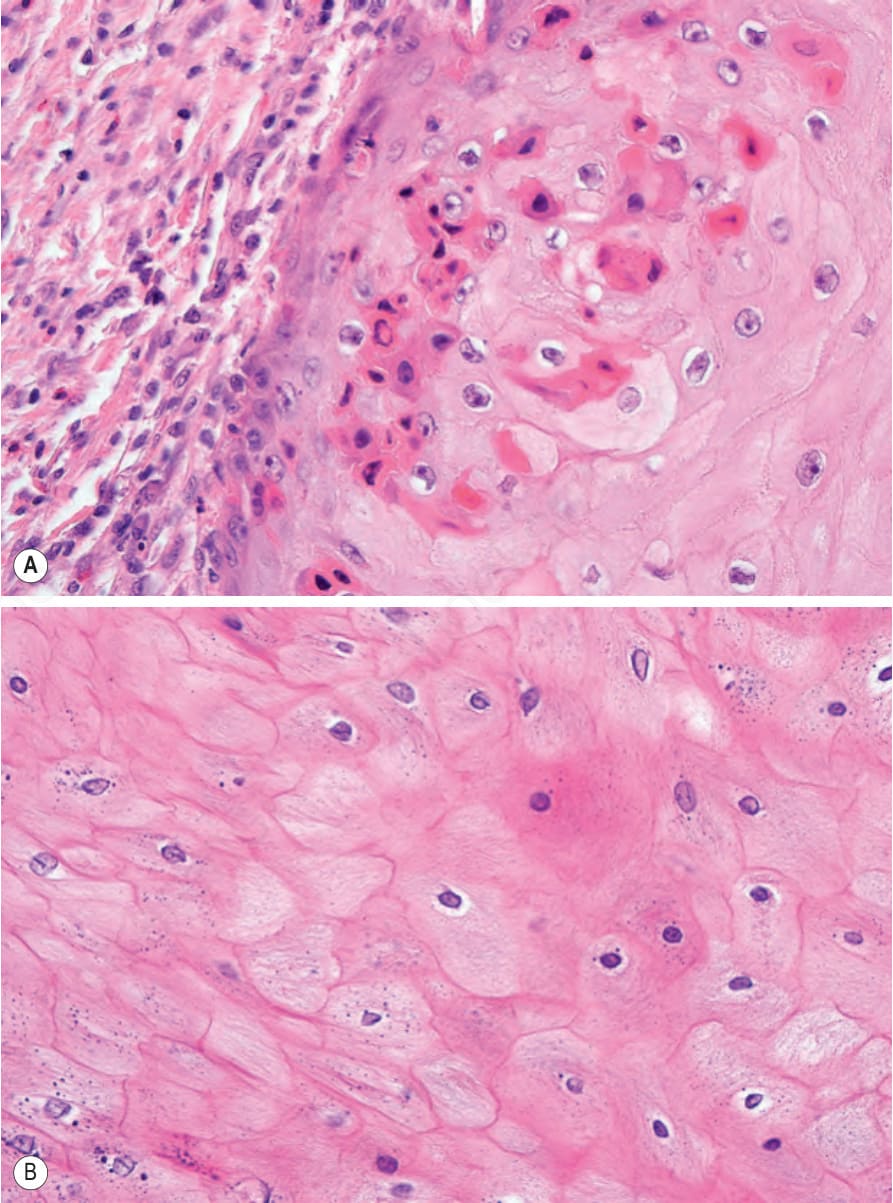
Fig. 23.52 (A, B) Keratoacanthoma: high-power view of differentiated squamous epithelium. There is no cytological atypia. Dyskeratotic cells are conspicuous.

Fig. 23.53 In situ squamous cell carcinoma: the nail has been replaced by a warty lesion.
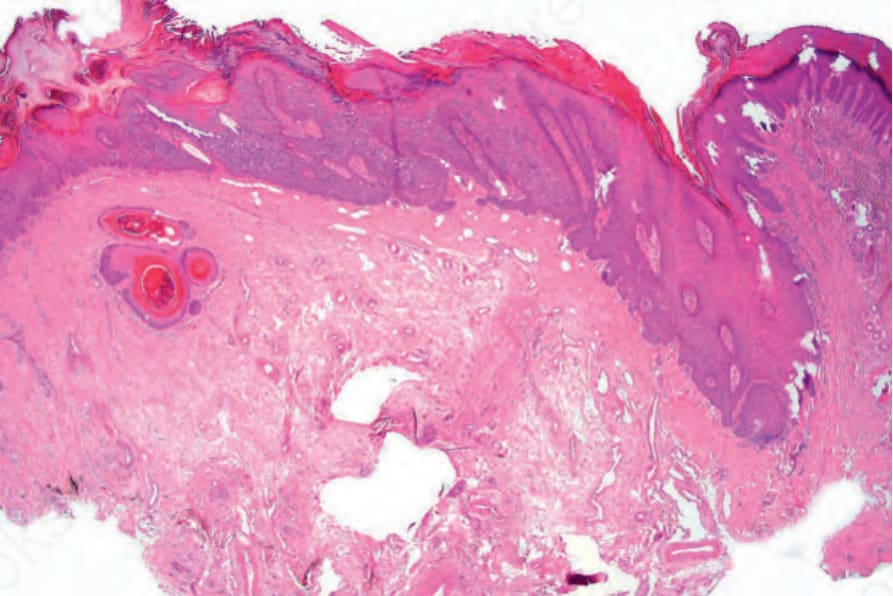
Fig. 23.54 In situ squamous cell carcinoma: the epithelium is thickened and even at this magnification there is obvious atypia.
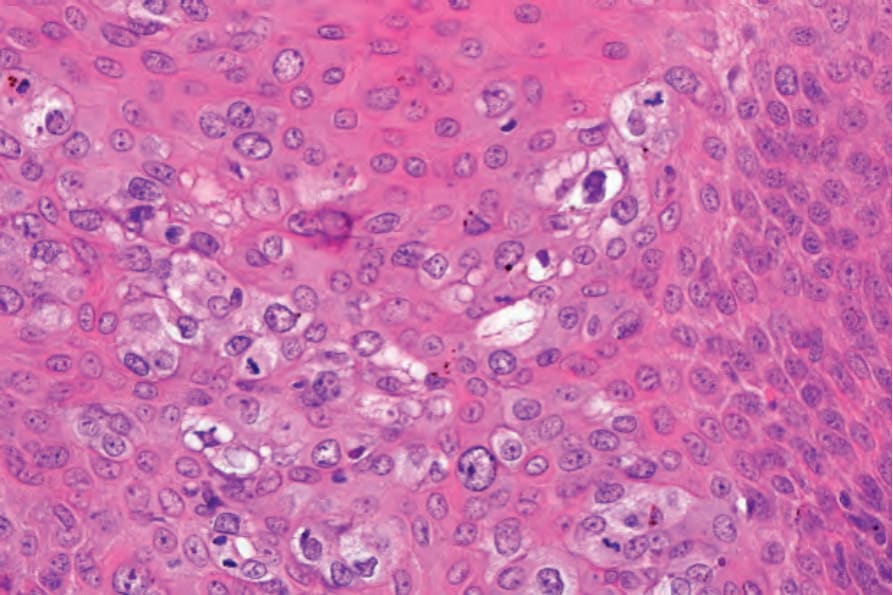
Fig. 23.55 In situ squamous cell carcinoma: high-power view showing pleomorphism and mitotic activity.
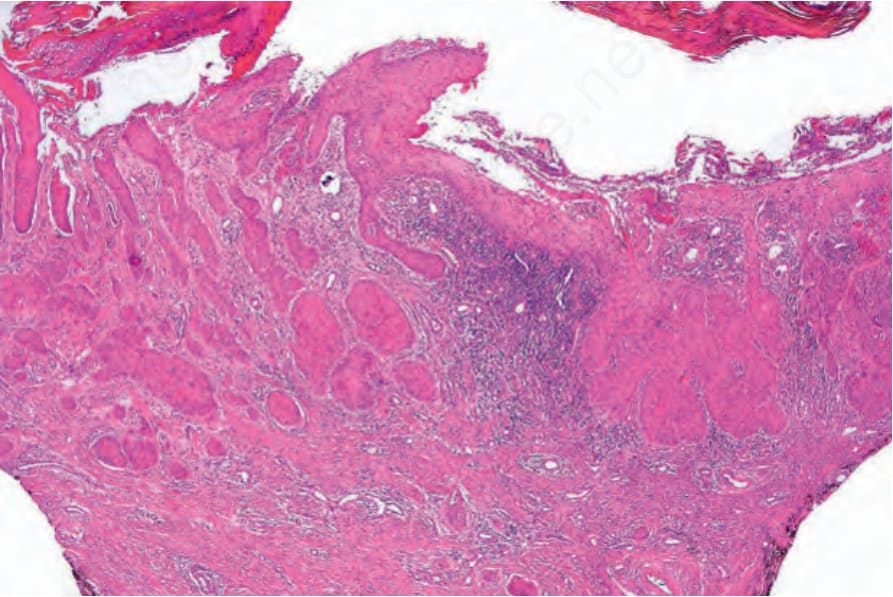
Fig. 23.56 Invasive squamous cell carcinoma: low-power view.
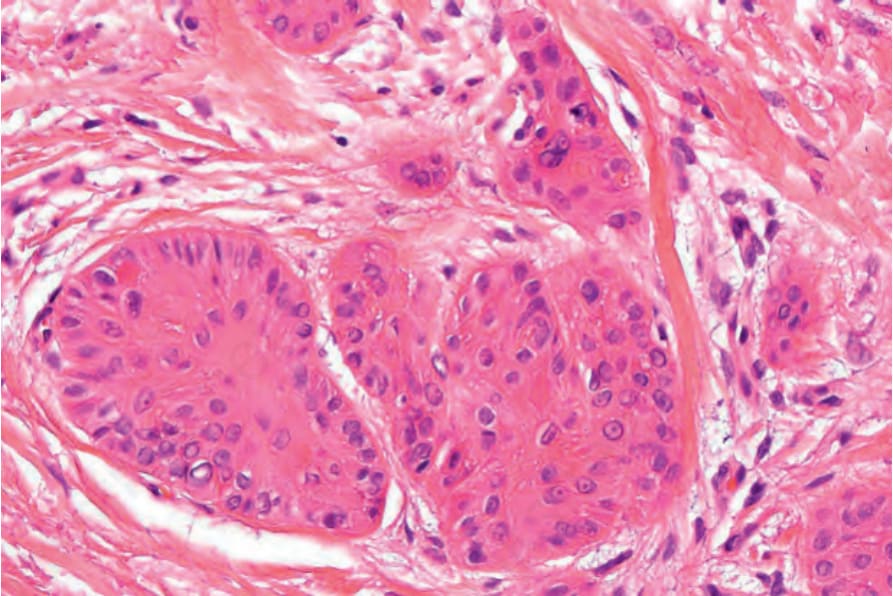
Fig. 23.57 Invasive squamous cell carcinoma: nests of well-differentiated squamous cell carcinoma are present deep in the dermis.

Fig. 23.58 Verrucous carcinoma: typical example showing the warty, hyperkeratotic surface. Courtesy of P. Gheeraert, MD, Hôpital Brugmann, Université Libre de Bruxelles, Belgium.
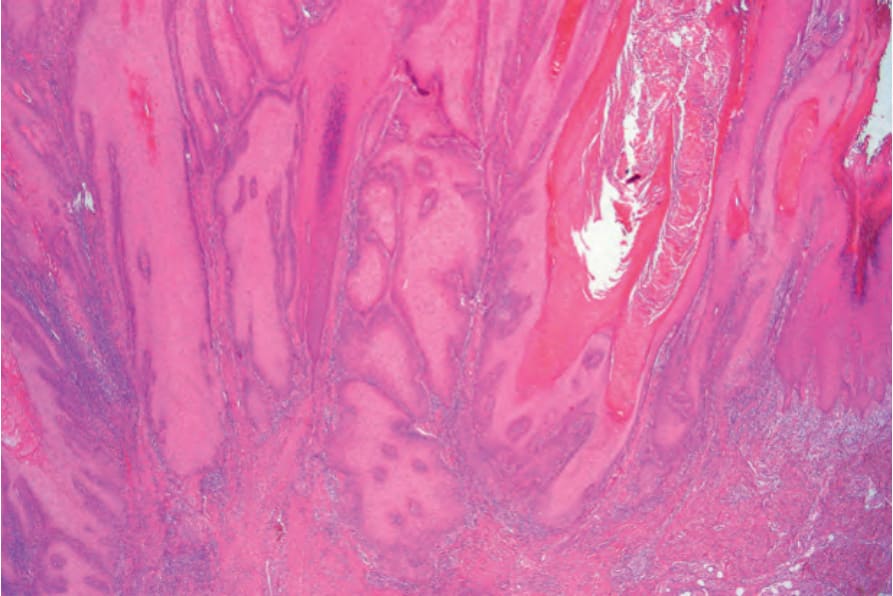
Fig. 23.59 Verrucous carcinoma: low-power view showing the deeply penetrating broad bulbous growth pattern. Courtesy of C. Deprez, MD, Hôpital Brugmann, Université Libre de Bruxelles, Belgium.
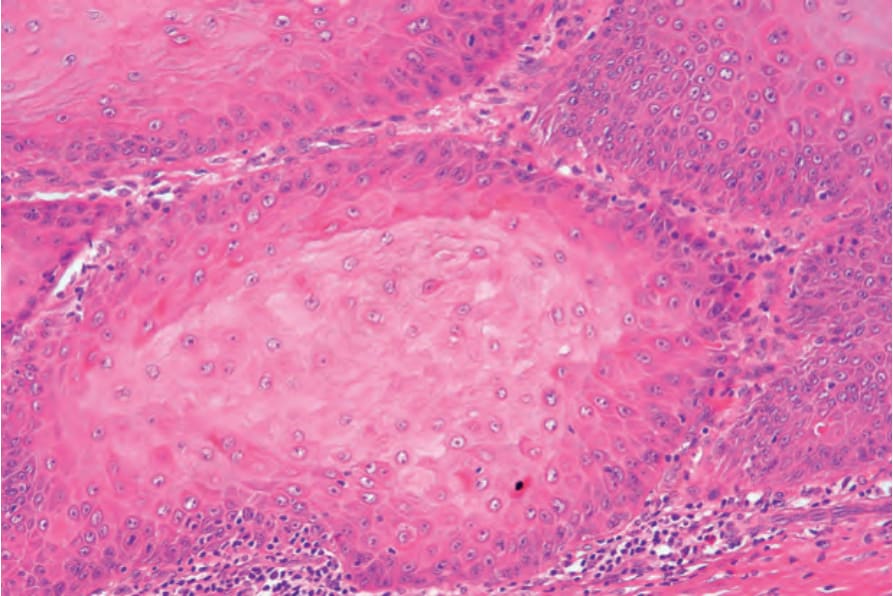
Fig. 23.60 Verrucous carcinoma: high-power view showing typical ground-glass epithelium. Note that there is no cytological atypia. Courtesy of C. Deprez, MD, Hôpital Brugmann, Université Libre de Bruxelles, Belgium.