甲癬 (Onychomycosis)
流行病學與臨床特徵 (Epidemiology and Clinical Features)
- 甲癬 (onychomycosis) 是甲板異常最常見的原因,占甲病的 18% 至 50%。在英國、北美與澳洲,甲真菌病影響一般人口的 2% 至 3%,年長者則高達 15%。
- 目前公認甲癬有六型:遠端與側緣甲下型甲癬 (distal and lateral subungual onychomycosis, DLSO) (Fig. 23.10)、淺表型甲癬 (superficial onychomycosis, SO)、近端甲下型甲癬 (proximal subungual onychomycosis, PSO)、甲內型甲癬 (endonyx onychomycosis, EO)、全甲營養不良型甲癬 (total dystrophic onychomycosis, TDO),以及混合型甲癬 (mixed pattern onychomycosis, MPO)。
- DLSO 為最常見的型態,真菌菌絲 (hyphae) 的侵犯始於甲下皮 (hyponychium),並沿甲床 (nail bed) 向近端擴展,造成變色、甲板增厚、甲下角化過度 (subungual hyperkeratosis) 與甲剝離 (onycholysis)。
- SO 發展為對甲板背側表面的侵犯,表現為白色、較少見為黑色的粉末狀斑塊狀變色。
- PSO 的特徵為真菌侵犯近端甲褶 (proximal nail fold, PNF),隨後甲板發生更深層的感染。可能伴隨甲溝炎 (paronychia)。
- EO 的特徵為直接侵犯遠端甲板而無甲床侵犯,造成具特徵性的型態,伴有甲板的層狀劈裂 (lamellar splitting) 與變色。
- 在 TDO 中,甲板發生完全的營養不良。其可為次發性 (secondary),由前述各型完全進展而來;或為原發性 (primary),影響免疫功能不全患者,特別是罹患慢性黏膜皮膚念珠菌病 (chronic mucocutaneous candidiasis) 者。
- MPO 結合不同型態的甲癬,較常見為 PSO 與 SO,或 DLSO 與 SO 的組合。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
-
甲癬可由三大類病原體引起:
- 皮癬菌 (dermatophytes),
- 酵母菌 (yeasts),
- 非皮癬菌黴菌 (nondermatophyte molds)。
-
皮癬菌是目前最常遇到的病原,在中歐占甲癬病例高達 80%。Trichophyton rubrum 在 60% 至 70% 的病例中被分離出來,其次為 Trichophyton mentagrophytes var. interdigitale。
-
酵母菌在約 5% 至 17% 的病例中生長,且每 10 例中有 7 例的致病菌在指甲為 Candida albicans、在趾甲為 Candida parapsilosis。
-
致病性黴菌 (Scytalydium、Aspergillus、Fusarium、Acremonium 與 Onychocola canadensis) 見於不到 5% 的病例。甲癬的臨床分類及其最常見的致病菌列於 Table 23.1。
-
甲癬通常以直接鏡檢與培養來診斷。以過碘酸-希夫染色 (periodic acid-Schiff, PAS) 染色的甲標本進行組織學檢查是一項有用的輔助技術,尤其是在臨床高度懷疑、但真菌培養與 KOH 製片結果為陰性時。其可使檢查者得以:
- 確認甲癬的診斷,
- 確定甲板侵犯的範圍 (甲下型、淺表型或全甲型甲癬),
- 提示感染病原的性質 (皮癬菌、酵母菌、黴菌),
| 甲癬的臨床型態 | 主要致病菌 |
|---|---|
| 遠端與側緣甲下型甲癬 (Distal and lateral subungual onychomycosis) | Trichophyton rubrum;較少見:Trichophyton mentagrophytes var. interdigitale;罕見:Epidermophyton floccosum |
| 淺表白色型甲癬 (Superficial white onychomycosis) | Trichophyton mentagrophytes var. interdigitale;罕見:Trichophyton rubrum;於熱帶與亞熱帶環境:Aspergillus terreus、Fusarium oxysporum、Acremonium spp.;於兒童:Candida albicans |
| 近端甲下型甲癬 (Proximal subungual onychomycosis) | Trichophyton rubrum;例外情況:Trichophyton megninii、Trichophyton schoenleinii、Epidermophyton floccosum |
| 伴甲溝炎之近端甲下型甲癬 (Proximal subungual onychomycosis with paronychia) | Candida spp.、Fusarium、Scopulariopsis brevicaulis、Aspergillus niger |
| 甲內型甲癬 (Endonyx onychomycosis) | Trichophyton soudanense、Trichophyton violaceum |
-
保存組織病理切片以供可能的重新評估。
-
在無甲癬的情況下,甲板取樣的組織學檢查可能揭示另一種診斷,尤其是乾癬 (psoriasis)。越來越多研究指出,PAS 染色是診斷甲癬最敏感的方法。然而,也有人認為其價值並不優於直接鏡檢。這可能取決於所採用的取樣技術。在罕見情況下,組織學檢查是唯一能確認甲癬臨床診斷的檢查。
-
在甲下型甲癬中,真菌位於甲下角質 (subungual keratin) 內,並由此侵犯腹側甲板 (ventral nail plate)。在 SO 中,真菌通常局限於甲板的淺表部分;然而,它們也可侵犯更深層。在全甲型甲癬中,菌絲侵犯整個甲板與甲下角質。
-
組織學檢查無法精確辨識感染病原,這需要真菌培養或聚合酶連鎖反應 (polymerase chain reaction, PCR)。然而,規則、筆直、有隔的菌絲,傾向與甲表面平行走行,支持皮癬菌感染;而在酵母菌甲癬中則可觀察到小圓形的酵母型 (yeast forms),其中部分出芽 (budding)、假菌絲 (pseudohyphae) 及/或短絲狀構造 (Fig. 23.11)。無假菌絲的孢子 (spores) 可能為污染物,不足以診斷甲癬。截斷狀孢子 (truncated spores) 與不規則菌絲、並由其長出細的穿透性絲狀構造,則代表黴菌感染 (Fig. 23.12)。
-
甲縱向切片活檢 (longitudinal nail biopsies) 在甲癬中通常不會施行,除非臨床懷疑另一種診斷如乾癬或扁平苔癬 (lichen planus)。組織學常為類乾癬樣 (psoriasiform),伴甲床上皮增生 (hyperplasia) 與嗜中性球外溢 (exocytosis of neutrophils)。常出現海綿水腫 (spongiosis)。甲下角質與甲板可能增厚或變薄,其中含有伴嗜中性球堆積 (neutrophil mounds) 的角化不全灶 (parakeratotic foci)。PAS 染色可作出正確的診斷 (Figs 23.13–23.15)。
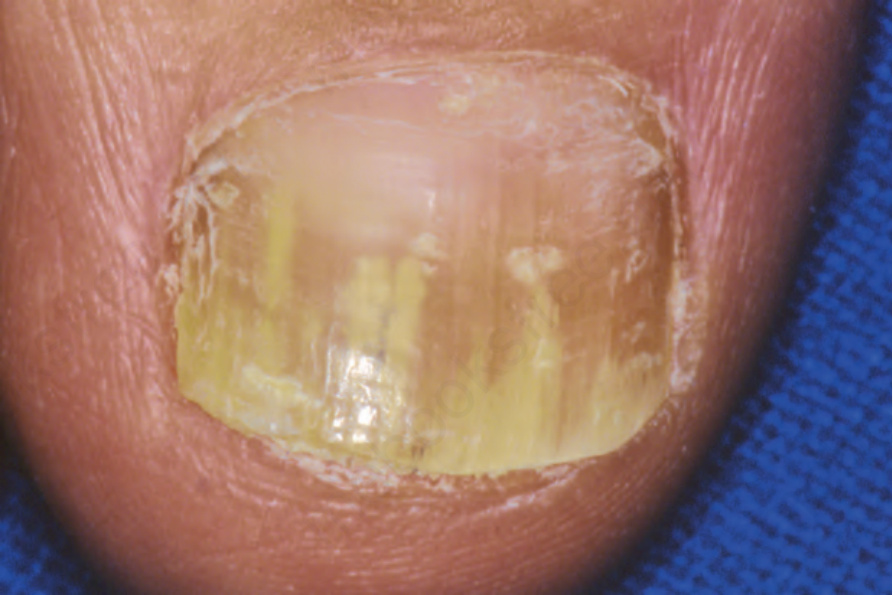
圖 23-10:甲癬:此為遠端側緣甲下侵犯 (distal lateral subungual involvement) 的例子。
Fig. 23.10 Onychomycosis: this is an example of distal lateral subungual involvement.
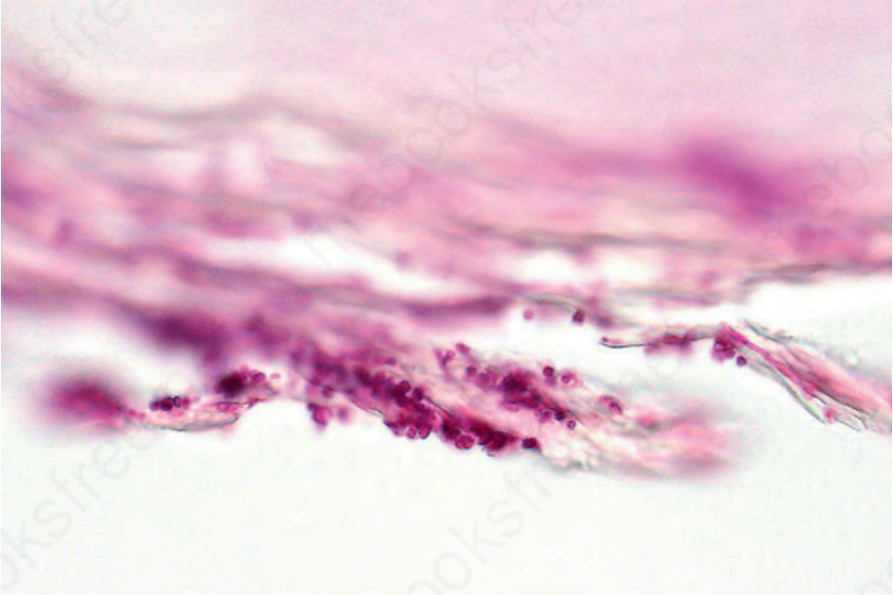
圖 23-11:甲癬:此例由均一的酵母菌 (uniform yeasts) 所引起 (periodic acid-Schiff)。
Fig. 23.11 Onychomycosis: this example is caused by uniform yeasts (periodic acid-Schiff).
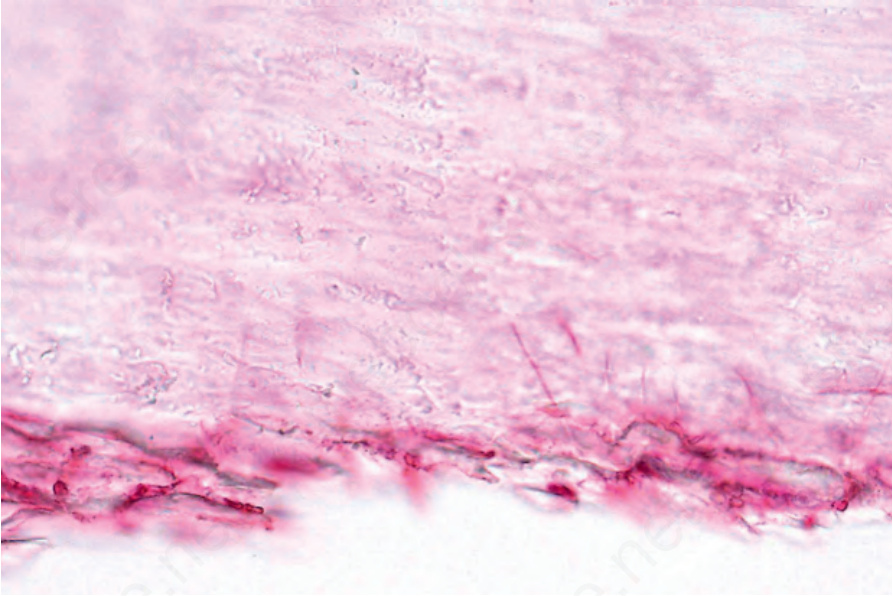
圖 23-12:甲癬:黴菌感染 (mold infection) 的例子。注意垂直走向、侵犯甲板的細的穿透性菌絲 (vertically orientated thin perforating hyphae)。
Fig. 23.12 Onychomycosis: an example of mold infection. Note the vertically orientated thin perforating hyphae invading the nail plate.
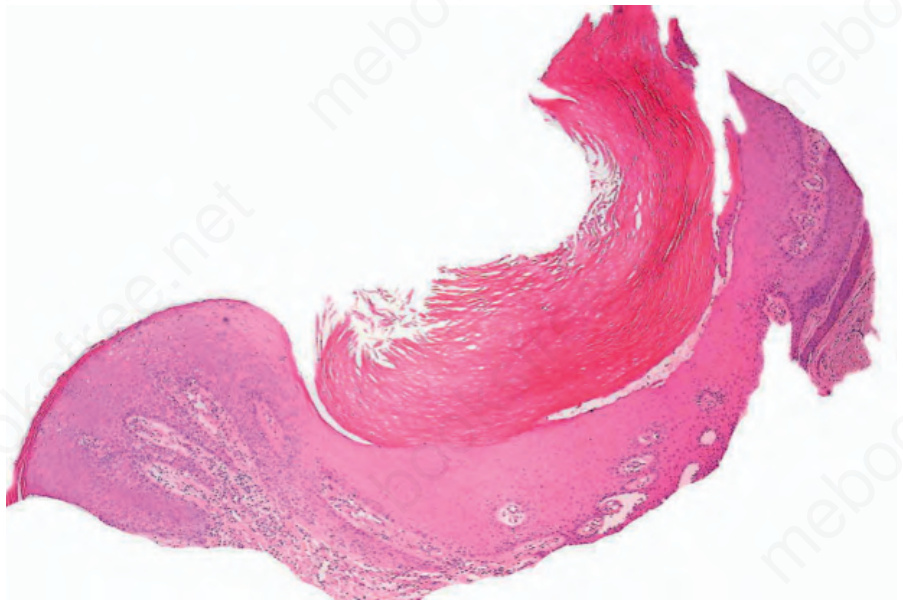
圖 23-13:甲癬:此例由皮癬菌感染 (dermatophyte infection) 引起,造成類乾癬樣外觀 (psoriasiform appearance)。掃描視野 (scanning view)。
Fig. 23.13 Onychomycosis: this example caused by a dermatophyte infection has resulted in a psoriasiform appearance. Scanning view.
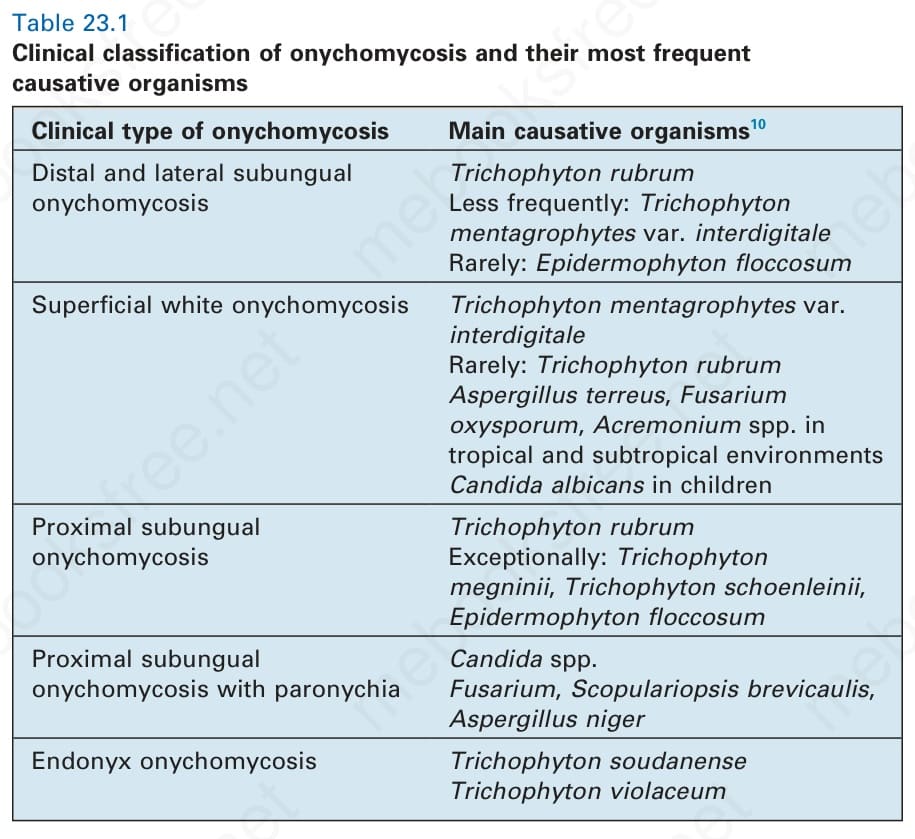
表 23-1:甲癬的臨床分類及其最常見的致病菌 (clinical classification of onychomycosis and their most frequent causative organisms)。
Table 23.1 Clinical classification of onychomycosis and their most frequent causative organisms