Onychomycosis
Onychomycosis
Epidemiology and clinical features Onychomycosis is the most frequent cause of nail abnormality representing 18% to 50% of nail diseases.1,2 In the United Kingdom, North America, and Australia, nail mycoses affect 2% to 3% of the general population and up to 15% of older people.3 Six types of onychomycosis are now recognized: distal and lateral subungual onychomycosis (DLSO) (Fig. 23.10), superficial onychomycosis (SO), proximal subungual onychomycosis (PSO), endonyx onychomycosis (EO), total dystrophic onychomycosis (TDO), and mixed pattern onychomycosis (MPO).4 DLSO is the most common form with invasion of fungal hyphae that begins at the hyponychium and spreads along the nail bed proximally, resulting in discoloration, thickening of the nail,
subungual hyperkeratosis, and onycholysis.5 SO develops as an invasion of the dorsal surface of the nail plate, appearing as a white or, more rarely, black powdery and patchy discoloration. PSO is characterized by fungal invasion of the PNF followed by a deeper infection of the nail plate. It may be associated with paronychia. EO is characterized by direct invasion of distal nail plate and absence of nail bed invasion, resulting in a characteristic pattern with lamellar splitting and discoloration of the nail plate. In TDO, there is complete dystrophy of the nail plate. It can be secondary, resulting from complete progression of any of the different types previously mentioned, or primary, affecting immunocompromised patients, especially those suffering from chronic mucocutaneous candidiasis. MPO associates different types of onychomycosis, more frequently PSO and SO or DLSO and SO.
Pathogenesis and histologic features Onychomycoses may be caused by three groups of pathogens3:
• dermatophytes,
• yeasts,
• nondermatophyte molds. Dermatophytes are by far the most commonly encountered, responsible for up to 80% of cases of onychomycosis in Central Europe.6 Trichophyton rubrum is isolated in 60% to 70% of cases followed by Trichophyton mentagrophytes var. interdigitale.7 Yeasts will grow in about 5% to 17% of cases,8 and in 7 out of 10 cases the responsible agent is Candida albicans in the fingernails and Candida parapsilosis in the toenails. Pathogenic molds (Scytalydium, Aspergillus, Fusarium, Acremonium, and Onychocola canadensis) are found in fewer than 5% of cases.9 The clinical classification of onychomycosis and their most frequent causative organisms are shown in Table 23.1.10
Onychomycosis is usually diagnosed by direct examination and culture. Histologic examination of a nail sample stained with periodic acid-Schiff (PAS) is a useful complementary technique, especially when there is strong clinical suspicion, but negative results have resulted from fungal culture and KOH preparation.11,12 It enables one to:
• confirm the diagnosis of onychomycosis,
• specify the extent of nail plate invasion (subungual, superficial or total onychomycosis),
• suggest the nature of the infecting agent (dermatophyte, yeast, mold),
Clinical type of onychomycosis Main causative organisms10
Distal and lateral subungual onychomycosis
Trichophyton rubrum Less frequently: Trichophyton mentagrophytes var. interdigitale Rarely: Epidermophyton floccosum
Superficial white onychomycosis Trichophyton mentagrophytes var. interdigitale Rarely: Trichophyton rubrum Aspergillus terreus, Fusarium oxysporum, Acremonium spp. in tropical and subtropical environments Candida albicans in children
1133 Periungual warts and other nail infections
Proximal subungual onychomycosis
Trichophyton rubrum Exceptionally: Trichophyton megninii, Trichophyton schoenleinii, Epidermophyton floccosum
Proximal subungual onychomycosis with paronychia
Candida spp. Fusarium, Scopulariopsis brevicaulis, Aspergillus niger
Endonyx onychomycosis Trichophyton soudanense Trichophyton violaceum
• store the histopathological slides for possible re-evaluation.3
• In the absence of onychomycosis, histologic examination of a nail plate sampling may disclose an alternative diagnosis especially psoriasis. More and more studies indicate that staining with PAS is the most sensitive method for diagnosing onychomycosis.13–16 Others, however, consider that it is no more valuable than direct examination.3 This is probably dependent on the sampling technique used.17 In rare cases, histologic examination is the only investigation which confirms the clinical diagnosis of onychomycosis.3
In subungual onychomycosis, the fungi are located in the subungual keratin from where they involve the ventral nail plate. In SO, they are usually restricted to the superficial part of the nail plate. However, they can also invade deeper.18,19 In total onychomycosis, the hyphae invade the entire nail plate and subungual keratin. Histologic examination does not allow precise identification of the infecting agent. This requires fungal culture or polymerase chain reaction (PCR). However, regular, straight, septate hyphae that tend to run parallel to the nail surface speak in favor of a dermatophytic infection while small round, yeast forms, some of them budding, pseudohyphae, and/or short filaments are observed in yeast onychomycosis (Fig. 23.11). Spores without pseudohyphae can be contaminants and do not allow a diagnosis of onychomycosis. Truncated spores and irregular hyphae from which arise thin perforating filaments represent a mold infection (Fig. 23.12).
Longitudinal nail biopsies are usually not performed in onychomycosis, except when another diagnosis such as psoriasis or lichen planus is clinically suspected. The histology is often psoriasiform with hyperplasia of the nail bed epithelium and exocytosis of neutrophils. Spongiosis is frequently present. The subungual keratin and nail plate may be thickened or thinned. They contain parakeratotic foci with neutrophil mounds.20 PAS staining allows the correct diagnosis to be made (Figs 23.13–23.15).
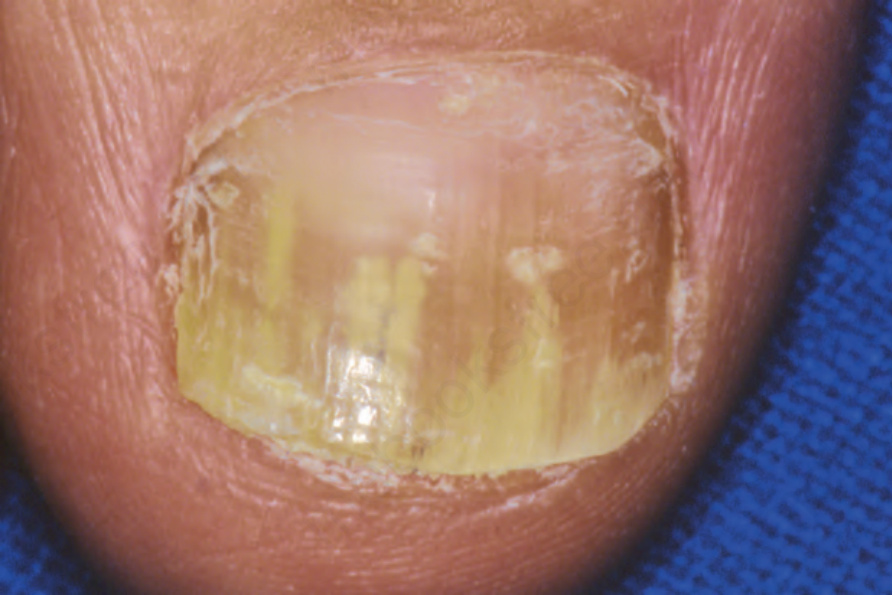
Fig. 23.10 Onychomycosis: this is an example of distal lateral subungual involvement.
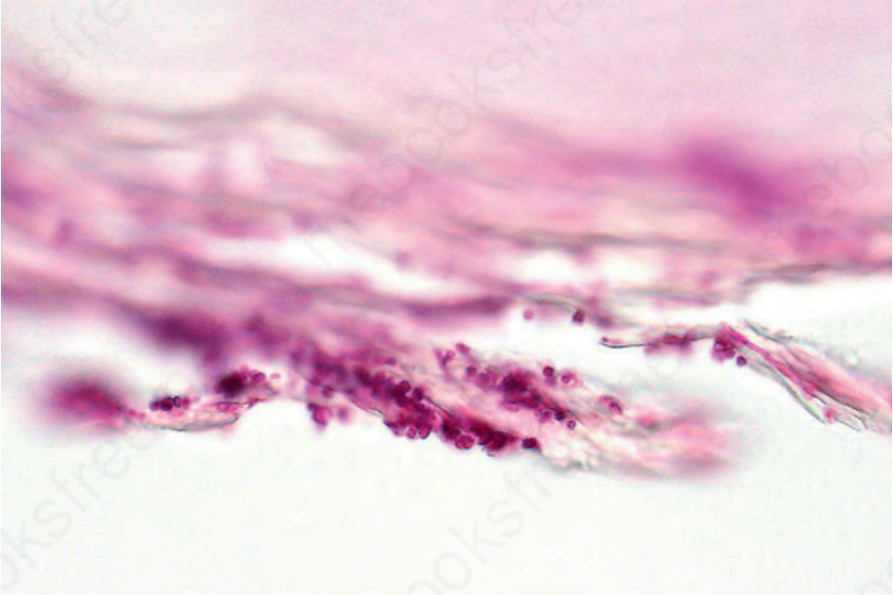
Fig. 23.11 Onychomycosis: this example is caused by uniform yeasts (periodic acid-Schiff).
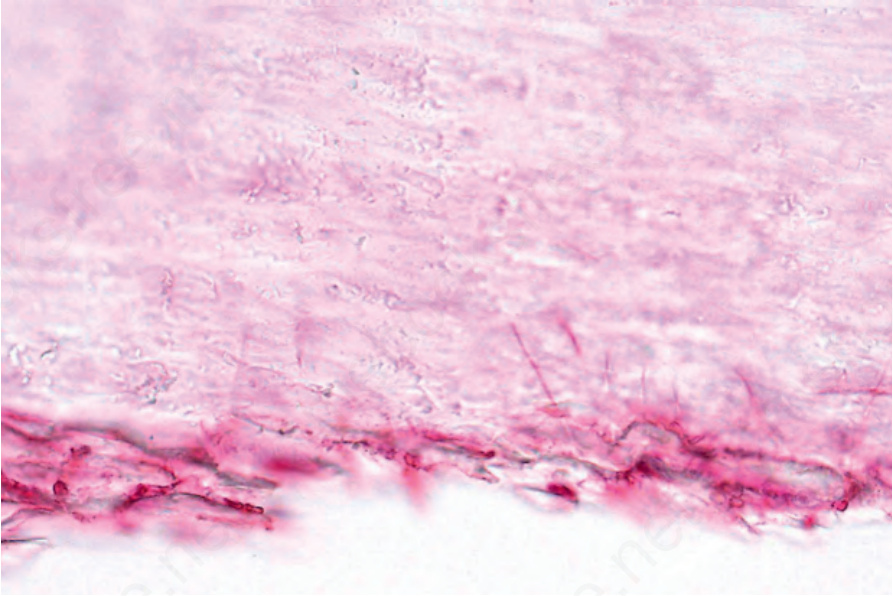
Fig. 23.12 Onychomycosis: an example of mold infection. Note the vertically orientated thin perforating hyphae invading the nail plate.
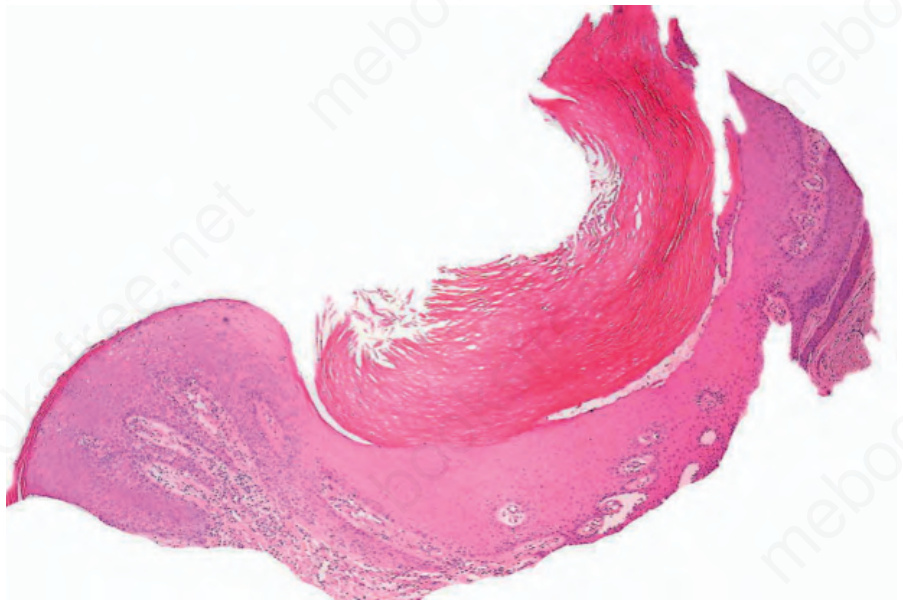
Fig. 23.13 Onychomycosis: this example caused by a dermatophyte infection has resulted in a psoriasiform appearance. Scanning view.
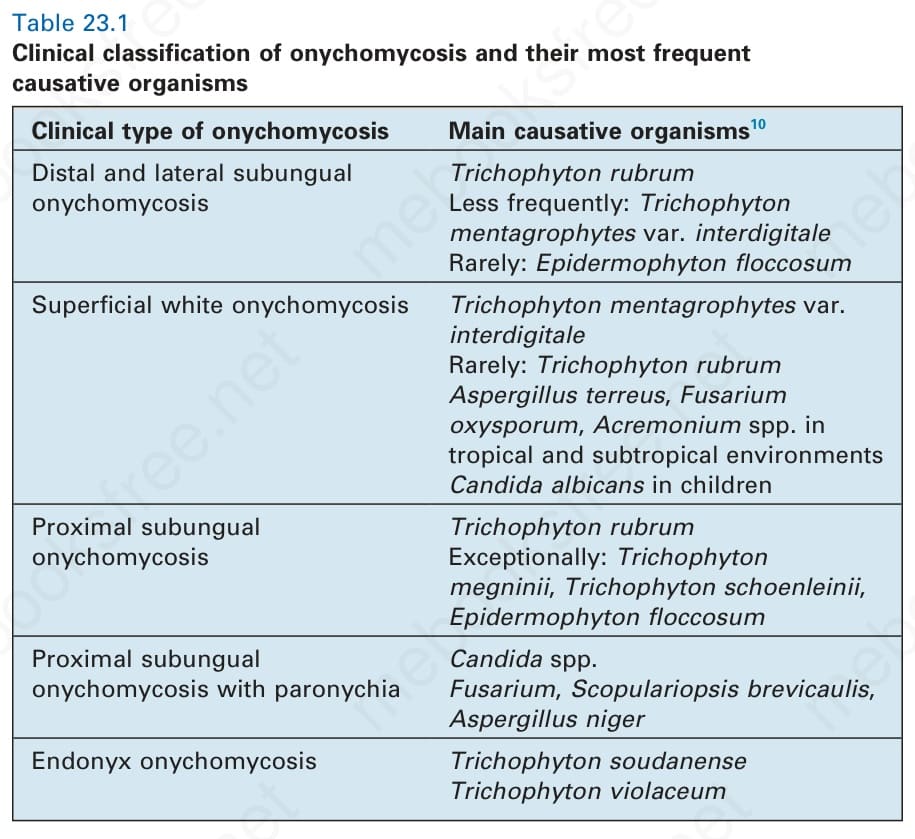
Table 23.1 Clinical classification of onychomycosis and their most frequent causative organisms