臨床特徵 (Clinical Features)
酒糟 (rosacea) 是一種皮膚反應,表現為「潮紅 (flushing)」,即中央臉部凸面 (convexities) 暫時性的發紅,並可能擴及身體其他部位,通常為軀幹與上腹部 (epigastrium)。National Rosacea Society 的酒糟分類與分期專家委員會 (Expert Committee on the Classification and Staging of Rosacea) 確認了酒糟的四種亞型與三套嚴重度分級系統。該委員會不認為本病的各分期會由一個分期演進至另一個分期,且僅承認一種變異型(granulomatous rosacea)(表 22.6 與表 22.7)。
酒糟最常出現於四十至六十多歲(第四至第六個十年),但也可見於青少年晚期或二十出頭。罕見情況下,兒童亦會受影響。本病的特徵為緩解與復發交替的病程。它是一種常見疾病,佔皮膚科門診所見全部病例的百分之零點五至百分之一點零。本病好發於女性(二至三比一),膚色白皙、具北歐 (Northern European) 血統者最常受影響。
鼻部 rhinophyma 的形成(圖 22.199)。這種令人毀容的鼻部增大是最常見的 phyma。它是由持續性淋巴水腫 (lymphedema) 以及皮脂腺 (sebaceous glands) 與周圍結締組織肥大兩者所致。毛囊顯得突出,且常被半凝固狀物質 (grumous material) 阻塞。
在酒糟的 erythematotelangiectatic 亞型中,紅斑可持續數小時至數天。搔癢不是其特徵。微血管擴張 (telangiectasia) 可為粗大或細微。它發生於雙頰、鼻唇溝 (nasolabial folds) 與鼻部(圖 22.197)。
在 papulopustular 亞型中,成簇的丘疹及(較少見的)膿疱出現於前額、顴部 (malar areas)、鼻部與下巴(圖 22.198)。這些丘疹不會壓痛,也不伴隨疤痕形成。
血管變化在女性較常見。在男性,「phymatous」變化可發生於下巴 (gnatophyma)、前額 (metophyma)、耳部 (otophyma)、眼瞼、顴部與鼻部,最終形成鼻部的 rhinophyma。
眼睛在酒糟中常受侵犯,尤其在兒童。病人最常抱怨異物感或灼熱感;臨床上可出現淺表點狀糜爛 (superficial punctate erosions) 或眼瞼炎 (blepharitis)(常伴瞼板腺炎 meibomianitis)。霰粒腫 (chalazia) 與麥粒腫 (sties) 很常見。較少見的情況下,會發生角膜潰瘍、疤痕、變薄與血管新生。Rosacea keratitis 包含角膜邊緣呈三角形舌狀的血管新生。
罕見情況下,臉外型酒糟 (extrafacial rosacea) 以丘疹型或血管型出現,侵犯臀部、四肢及/或胸骨前區 (presternal area)(disseminated rosacea)。
Granulomatous rosacea 變異型的特徵為孔周 (periorificial) 皮膚丘疹或結節,可導致疤痕(圖 22.200)。病人通常沒有持續性臉部紅斑或其他酒糟徵象。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
酒糟的致病機轉大致仍不明,目前的研究特別著重於 cytokines 與其他發炎介質 (inflammatory mediators) 的角色。許多研究顯示,酒糟病人在受到心理與物理因素誘發時,所經歷的「潮紅反應 (flushing reactions)」遠較對照族群更強烈且更頻繁。近來有人提出這可能源於潛在的血管疾病。病灶處的血流量為正常速率的三至四倍。然而這可能是本病的結果,而非原因。酒糟亦曾與陽光、月經、懷孕、高血壓、藥物、口服避孕藥、臉部化妝品、職業性熱暴露、酒精、辛辣食物及生活型態相關聯。蟎蟲 Demodex folliculorum 也被認為與之有關。D. folliculorum 存在於皮膚,尤其在鼻唇溝、鼻部與眼瞼的毛囊內。偏頭痛 (migraine) 常為一相關特徵。沒有證據顯示存在 HLA 易感性。曾有人提出本病與上消化道 Helicobacter pylori 感染相關,但較近期的文獻對此假說鮮少支持。
許多組織病理學發現是非特異性的。在酒糟的 erythematotelangiectatic 亞型中,真皮可見非特異性的淋巴組織球性 (lymphohistiocytic) 發炎浸潤,常呈血管周圍 (perivascular) 與毛囊周圍 (perifollicular) 分布,並伴隨水腫與微血管擴張(圖 22.201)。
在 papulopustular 亞型中,檢查丘疹或膿疱可見嗜中性球聚集於毛囊內,周圍環繞非特異性慢性發炎細胞浸潤。部分丘疹顯示肉芽腫性發炎 (granulomatous inflammation) 的證據(granulomatous rosacea),伴隨受損的毛囊,並可辨識出蟎蟲 D. folliculorum(圖 22.202 與圖 22.203)。日光性彈力纖維變性 (solar elastosis) 常為一特徵,但這可能是巧合。
在 rhinophyma 中,皮脂腺在大小與數目上增加。毛囊漏斗部 (follicular infundibula) 可能擴張並充滿角化碎屑 (keratinous debris)。真皮上層含有慢性發炎細胞浸潤,並有微血管擴張。有時可見真皮結締組織增加,在較晚期此一變化可能占主導,並伴隨皮脂腺的喪失。
Granulomatous rosacea 的組織學診斷通常極為困難,因為對 D. folliculorum、角質 (keratin)、皮脂 (sebum) 與破裂囊腫產生反應的異物肉芽腫 (foreign body granulomata) 在臉部非常常見;因此診斷應僅限於那些在毛囊間 (interfollicular) 分布中顯示清楚界定的肉芽腫、且具相符臨床背景的病灶。
鑑別診斷 (Differential Diagnosis)
酒糟與尋常性痤瘡 (acne vulgaris) 的區別在於前者沒有粉刺 (comedones),且具有微血管擴張及潮紅發作病史。
一種以紅斑、丘疹與膿疱為特徵、類似酒糟的皮膚病 (rosacea-like dermatosis),可能在過度使用外用類固醇後發生,且曾報告僅長期使用 1% 外用 hydrocortisone 即可引發(圖 22.204)。依疹子的位置,類固醇誘發的類酒糟皮膚炎 (steroid-induced rosacea-like dermatitis) 有三種類型:口周型 (perioral)、臉中央型 (centrofacial) 與瀰漫型 (diffuse)。紅斑侵犯整個塗抹區域,且通常伴隨萎縮 (atrophy)。
Acne agminata(lupus miliaris disseminatus faciei)病因不明,但最可能代表對破裂毛囊的肉芽腫反應(圖 22.205)。它表現為中央臉部的黃棕色丘疹,好發於眶周 (periorbital) 區域。鏡壓檢查 (diascopy) 可顯示蘋果醬樣結節 (apple-jelly nodules)。它不伴隨潮紅發作或微血管擴張,且不代表酒糟的一種變異型,雖然與肉芽腫型在組織學上有相當程度的重疊。病灶常進展為深層疤痕。Acne agminata 可分為四個組織病理學群組:具壞死的上皮樣細胞肉芽腫 (epithelioid cell granuloma with necrosis)、不具壞死的上皮樣細胞肉芽腫 (epithelioid cell granuloma without necrosis)、具膿瘍的上皮樣細胞肉芽腫 (epithelioid cell granuloma with abscesses),以及非肉芽腫性的非特異性發炎細胞浸潤 (nongranulomatous non-specific inflammatory cell infiltrates)。在那些有顯著肉芽腫性發炎的病例中,常需要特殊染色以排除黴菌與分枝桿菌 (mycobacterial) 感染。
口周皮膚炎 (perioral dermatitis) 有時被視為酒糟的一種變異型,雖然其臨床表現不同。病人(尤其是年輕女性與兒童)出現程度不一的搔癢性、紅斑性微小水疱 (microvesicles)、脫屑、丘疹、微小結節 (micronodules) 與膿疱,侵犯下巴、鼻唇溝與眼周 (periocular) 區域(圖 22.206)。組織學上,它與酒糟相似,並具海綿水腫性 (spongiotic) 變化。
嚴重的 D. folliculorum 感染(demodicosis)可能以類似酒糟的特徵表現。潮紅與微血管擴張則不存在。
組織學上,本病的特徵為伴有肉芽腫性發炎反應的毛囊囊腫 (follicular cysts) 及大量蟎蟲(圖 22.207)。
Rhinophyma 也可能與其他造成潮紅的原因相關,例如類癌症候群 (carcinoid syndrome) 與酒精濫用。
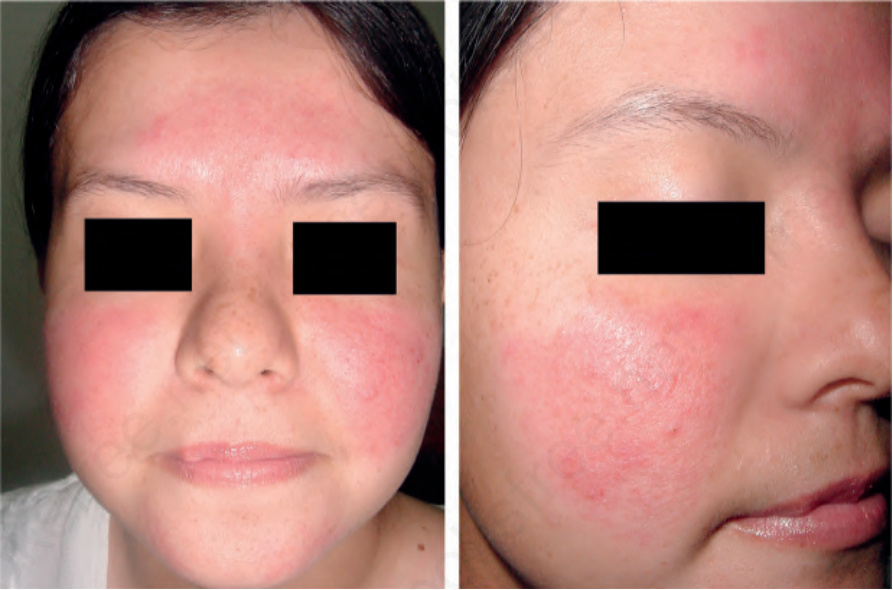
圖 22-197:酒糟 erythematotelangiectatic 亞型:臉部有瀰漫性紅斑伴顴部微血管擴張 (malar telangiectasia)。By courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
Fig. 22.197 Rosacea erythematotelangiectatic subtype: there is diffuse erythema of the face with malar telangiectasia. By courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
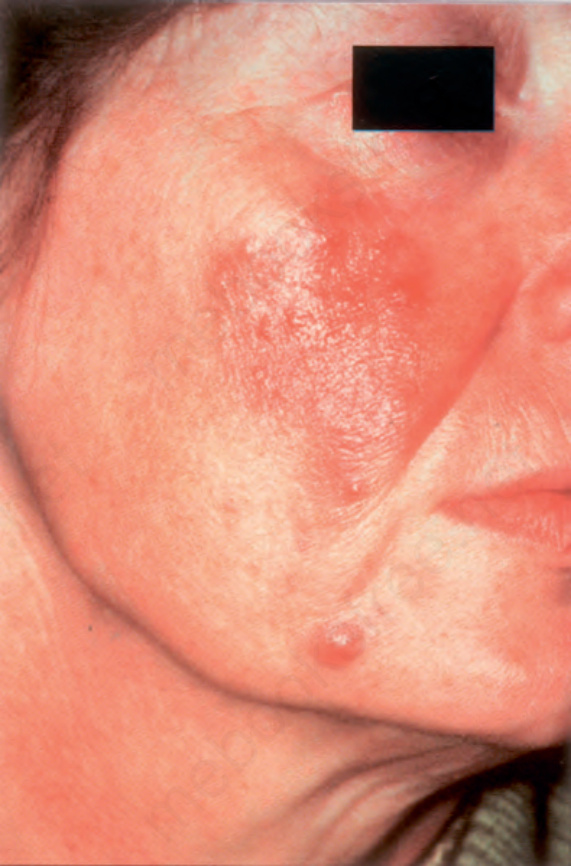
圖 22-198:酒糟 papulopustular 亞型:注意頰部的丘疹與膿疱 (papules and pustules)。By courtesy of the Institute of Dermatology, London, UK.
Fig. 22.198 Rosacea papulopustular subtype: note the papules and pustules on the cheek. By courtesy of the Institute of Dermatology, London, UK.

圖 22-199:酒糟 phymatous 亞型:此為 rhinophyma 的典型外觀。注意鼻部不規則的表面結節狀變化與增大。Courtesy of L.M. Gómez, MD, Universidad Pontificia Bolivariana, Medellín, Colombia.
Fig. 22.199 Rosacea phymatous subtype: this is the typical appearance of rhinophyma. Note the irregular surface nodularities and enlargement of the nose. Courtesy of L.M. Gómez, MD, Universidad Pontificia Bolivariana, Medellín, Colombia.

圖 22-200:granulomatous rosacea 變異型:注意這些在酒糟背景上出現的丘疹 (papules)。By courtesy of the Institute of Dermatology, London, UK.
Fig. 22.200 Granulomatous rosacea variant: note the papules which have arisen against a background of rosacea. By courtesy of the Institute of Dermatology, London, UK.
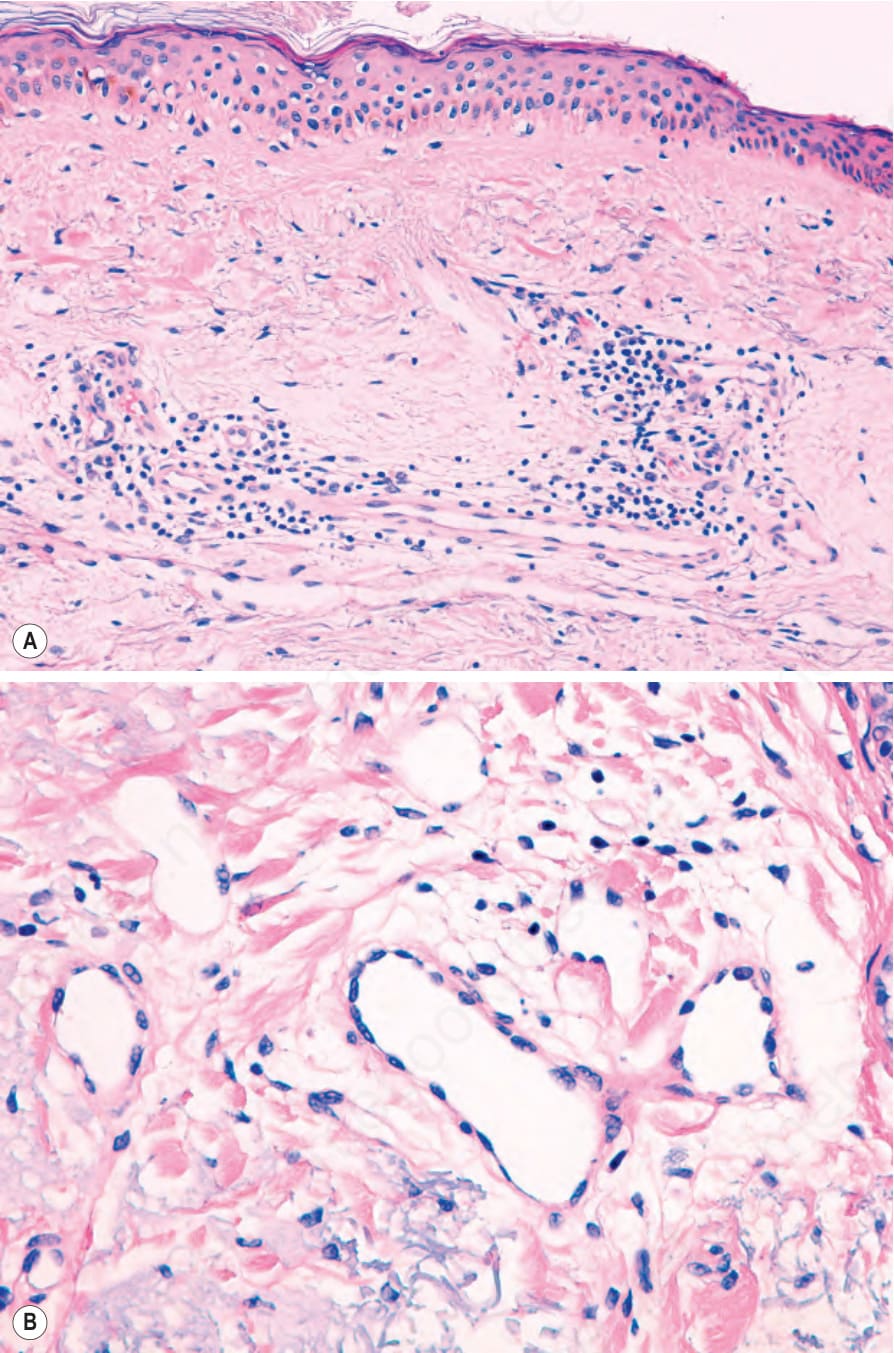
圖 22-201:(A, B) 酒糟 erythematotelangiectatic 亞型:有水腫、微血管擴張,以及輕度淋巴組織球性發炎細胞浸潤 (lymphohistiocytic inflammatory cell infiltrate)。
Fig. 22.201 (A, B) Rosacea erythematotelangiectatic subtype: there is edema, telangiectasia, and a mild lymphohistiocytic inflammatory cell infiltrate.
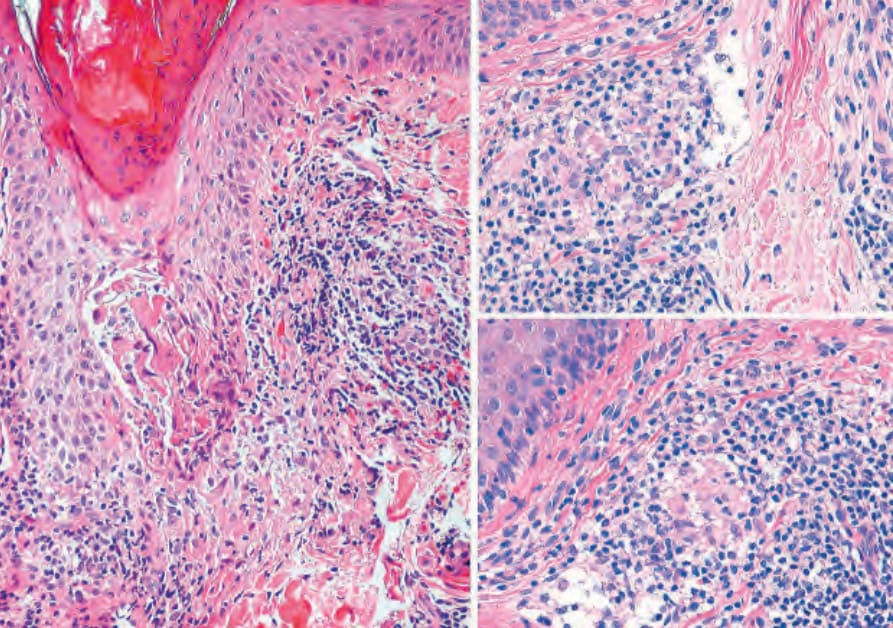
圖 22-202:granulomatous rosacea:注意毛囊周圍的非乾酪化肉芽腫 (perifollicular noncaseating granulomata)。
Fig. 22.202 Granulomatous rosacea: note the perifollicular noncaseating granulomata.
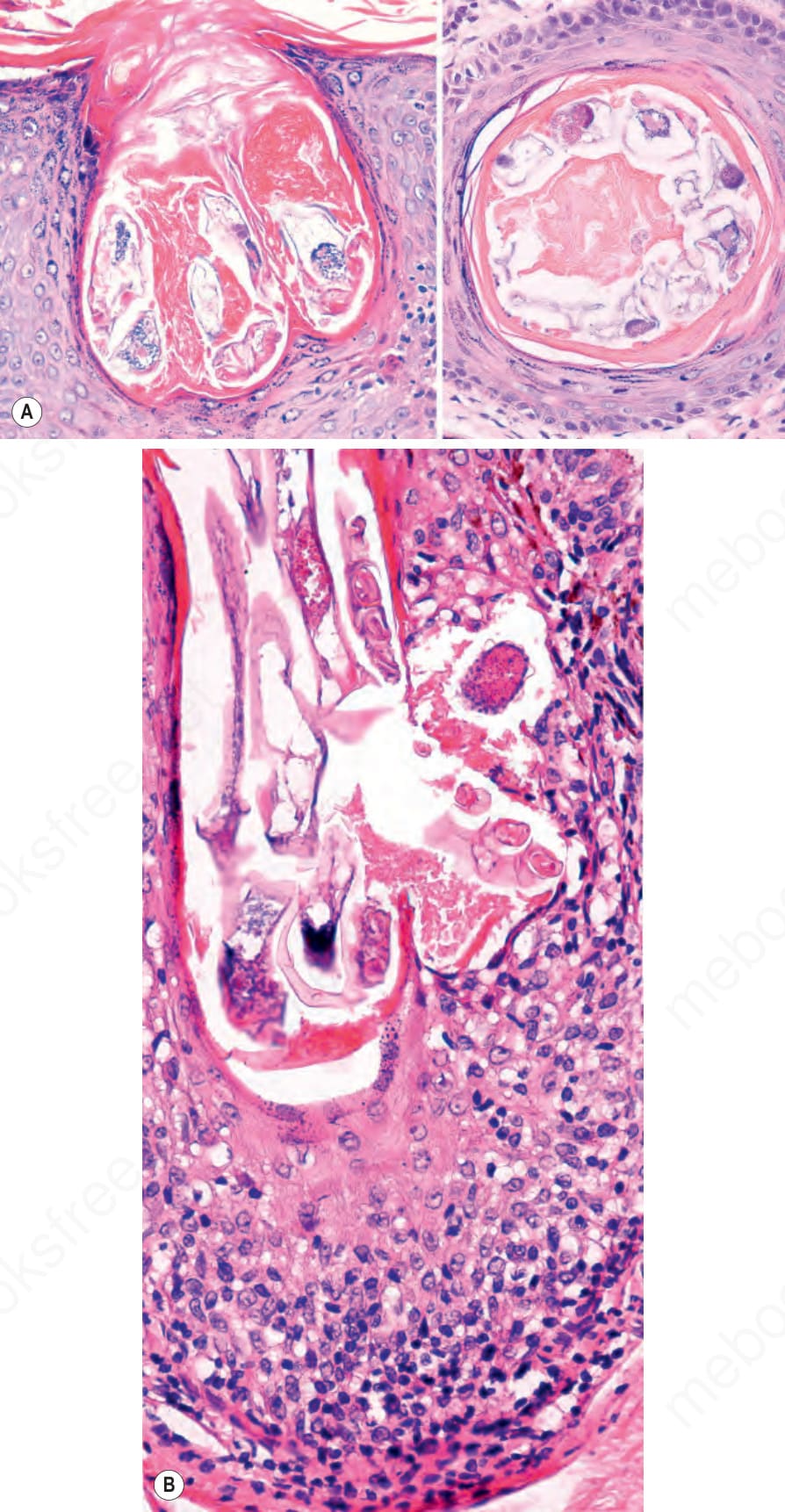
圖 22-203:酒糟:(A) 此漏斗部 (infundibulum) 內的 Demodex folliculorum 蟎蟲(class Arachnida,order Acarina),呈垂直與水平切面。(B) 一些 D. folliculorum 蟎蟲正經由鄰近一處破裂的毛囊向外移出。注意淋巴球浸潤 (lymphocytic infiltrate)。
Fig. 22.203 Rosacea: (A) Demodex folliculorum mite (class Arachnida, order Acarina) within this infundibulum in vertical and horizontal sections. (B) Some D. folliculorum mites exiting through a nearby ruptured hair follicle. Note the lymphocytic infiltrate.
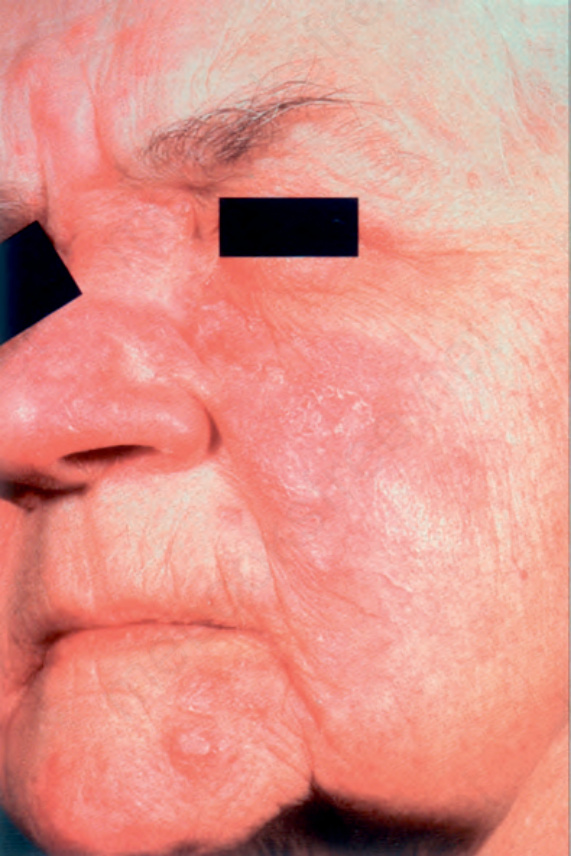
圖 22-204:外用類固醇相關酒糟 (topical steroid-related rosacea):長期外用類固醇治療已導致紅斑、微血管擴張與萎縮 (atrophy)。By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Fig. 22.204 Topical steroid-related rosacea: prolonged topical steroid therapy has resulted in erythema, telangiectasia, and atrophy. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
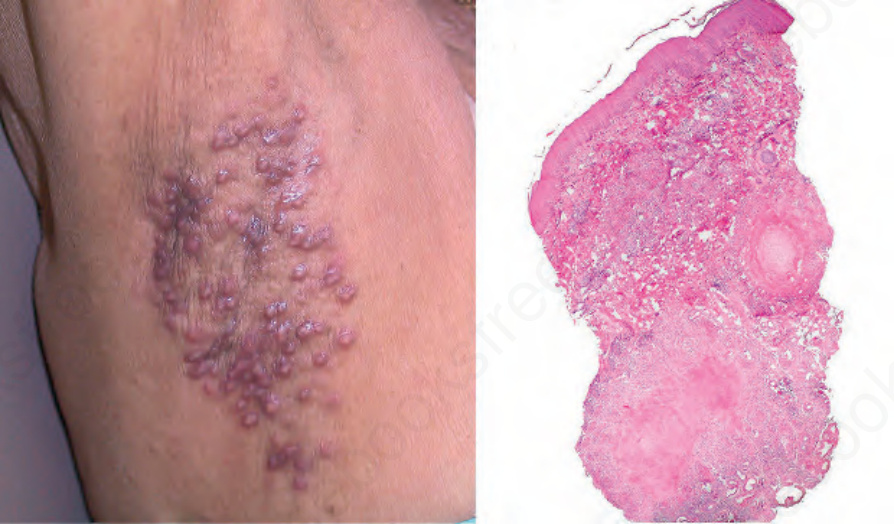
圖 22-205:acne agminata:注意腋下的一些膚色丘疹與結節(左),以及乾酪化肉芽腫性發炎 (caseating granulomatous inflammation)(右)。Courtesy of J.E. Arroyave, MD, Hospital Pablo Tobón Uribe, Medellín, Colombia.
Fig. 22.205 Acne agminata: note some flesh-colored papules and nodules on the axillae (left), and caseating granulomatous inflammation (right). Courtesy of J.E. Arroyave, MD, Hospital Pablo Tobón Uribe, Medellín, Colombia.

圖 22-206:口周皮膚炎 (perioral dermatitis):在濕疹性與紅斑性基底上成群的毛囊性紅色丘疹與丘疹水疱 (papulovesicles)。
Fig. 22.206 Perioral dermatitis: grouped follicular reddish papules and papulovesicles on an eczematous and erythematous base.
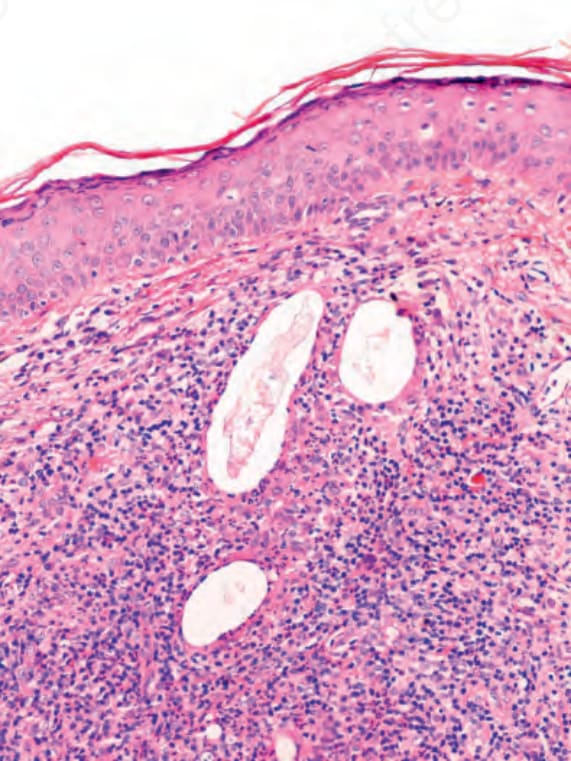
圖 22-207:demodicosis:注意一些游離於真皮中的 Demodex folliculorum 蟎蟲,周圍環繞發炎細胞浸潤 (inflammatory cell infiltrate)。
Fig. 22.207 Demodicosis: note some Demodex folliculorum mites free in the dermis, surrounded by an inflammatory cell infiltrate.
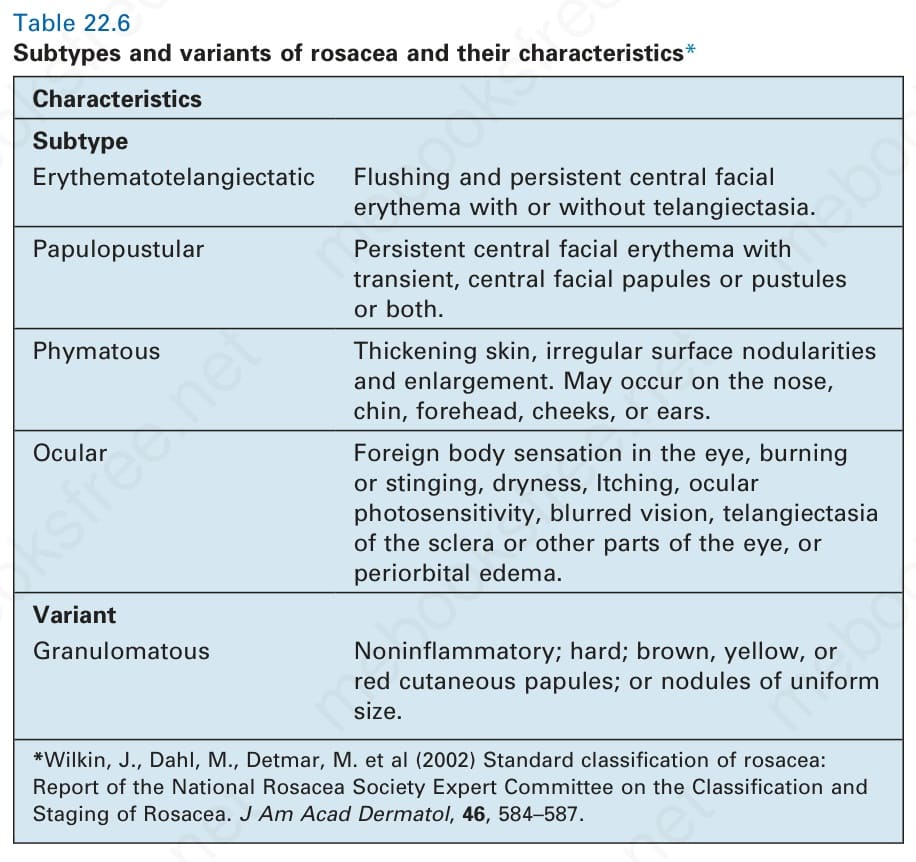
表 22-6:酒糟的亞型與變異型及其特徵 (subtypes and variants of rosacea and their characteristics)。
Table 22.6 Subtypes and variants of rosacea and their characteristics*