Rosacea
Rosacea
Clinical features Rosacea is a cutaneous reaction that presents with ‘flushing’, a transient redness of the convexities of the central face, which may extend to other parts of the body, usually the trunk and epigastrium.1–3 The National Rosacea Society’s Expert Committee on the Classification and Staging of Rosacea identified four subtypes of rosacea and three severity grading systems. This committee does not accept that stages of the disease evolve from one stage to another and recognize only one variant (granulomatous rosacea) (Tables 22.6 and 22.7).4–7
Rosacea most often presents in the fourth to sixth decades but may be seen in the late teens or early twenties. Exceptionally, children are affected.8 The condition is characterized by episodes of remission and recurrence. It is a common disease, accounting for 0.5–1.0% of all cases seen in a
1124 Diseases of the hair
formation of rhinophyma of the nose (Fig. 22.199).5,10,11 This disfiguring enlargement of the nose is the most common phyma. It is caused by both persistent lymphedema and hypertrophy of the sebaceous glands and surrounding connective tissue. The follicles appear prominent and are often plugged with grumous material.
dermatology outpatient department. There is a predilection for females (2–3 : 1), and those with fair skin and a Northern European ancestry are most often affected.9
In the erythematotelangiectatic subtype of rosacea, the erythema may last from hours to days.1 Pruritus is not a feature. Telangiectasia can be coarse or fine. It develops on the cheeks, nasolabial folds, and nose (Fig. 22.197).5
In the papulopustular subtype, crops of papules and (less commonly) pustules are present over the forehead, malar areas, nose, and chin (Fig.
22. 198). The papules are not tender and are not associated with scarring 5
Vascular changes tend to be more common in women. In men, ‘phymatous’ change may occur on the chin (gnatophyma), forehead (metophyma), ears (otophyma), eyelids, malar areas, and the nose, culminating in the
The eye is frequently involved in rosacea, particularly in children.8 Patients complain most often of a foreign body sensation or burning; clinically, superficial punctate erosions or blepharitis (often with meibomianitis) may be present.12 Chalazia and sties are commonly found. Less frequently, corneal ulceration, scarring, thinning, and vascularization occur. Rosacea keratitis comprises a triangular tongue-like vascularization of the margin of the cornea.5
Rarely, extrafacial rosacea occurs in a papular or vascular form involving the buttocks, limbs, and/or the presternal area (disseminated rosacea).7,13
The granulomatous rosacea variant is characterized by periorificial cutaneous papules or nodules that can lead to scarring (Fig. 22.200). Patients often do not have persistent facial erythema or other signs of rosacea.5,7
Pathogenesis and histologic features The pathogenesis of rosacea is largely unknown, and current research is particularly directed toward the role of cytokines and other inflammatory mediators.14 Many studies have shown that patients with rosacea experience much stronger and more frequent ‘flushing reactions’ when provoked by psychological and physical agents than a control population. It has recently been suggested that this may be due to an underlying vascular disorder. Lesional blood flow is three to four times the normal rate.7 This may, however, be a consequence rather than a cause of the condition. Rosacea has also been associated with sunlight, menstruation, pregnancy, hypertension, medications, oral contraceptive pills, facial cosmetics, occupational heat, alcohol, spicy food, and lifestyle.3,15 The mite Demodex folliculorum has also been implicated. D. folliculorum is present, particularly within the hair follicles of the nasolabial folds, nose, and eyelids.16,17 Migraine is often an associated feature.18 There is no evidence of an HLA predisposition. An association with upper gastrointestinal Helicobacter pylori infection has been proposed although the more recent literature offers little support for this hypothesis.19,20
1125 Rosacea
Many of the histopathological findings are non-specific. 21 In the erythematotelangiectatic subtype of rosacea, there is a non-specific lymphohistiocytic inflammatory infiltrate in the dermis, often in a perivascular and perifollicular distribution with associated edema and telangiectasia (Fig. 22.201).
A
Examination of papules or pustules in the papulopustular subtype reveals neutrophils aggregated in the follicle, with a surrounding non-specific chronic inflammatory cell infiltrate. Some papules show evidence of granulomatous inflammation (granulomatous rosacea) associated with damaged follicles, and the mite D. folliculorum may be identified (Figs 22.202 and 22.203). Solar elastosis is often a feature, but this may be coincidental.
In rhinophyma, the sebaceous glands are increased in size and number. The follicular infundibula may be dilated and filled with keratinous debris. The upper dermis contains a chronic inflammatory cell infiltrate and there is dilatation of the capillaries. Increased dermal connective tissue is sometimes present, and in the later stages this may predominate, with loss of the sebaceous glands.22
The histologic diagnosis of granulomatous rosacea is often extremely difficult because foreign body granulomata reacting to D. folliculorum, keratin, sebum, and ruptured cysts are very common on the face; the diagnosis should therefore be restricted to lesions that show clearly defined granulomata in an interfollicular distribution and in the appropriate clinical setting.23,24
Differential diagnosis Rosacea is distinguished from acne vulgaris by the absence of comedones and the presence of telangiectasia and a history of flushing episodes.
A rosacea-like dermatosis characterized by erythema, papules, and pustules may follow excessive use of topical steroids and has been reported to occur with prolonged use of only 1% topical hydrocortisone (Fig. 22.204).24 There are three types of steroid-induced rosacea-like dermatitis based on the location of the eruption: perioral, centrofacial, and diffuse.25 The erythema involves the whole of the area of application and is usually associated with atrophy.
B
Acne agminata (lupus miliaris disseminatus faciei) is of unknown etiology although it most probably represents a granulomatous reaction to ruptured hair follicles (Fig. 22.205). It presents as yellow-brown papules on the central face with a predilection for the periorbital region. Diascopy may reveal apple-jelly nodules. It is not associated with flushing episodes or telangiectasia and does not represent a variant of rosacea although there is considerable histologic overlap with the granulomatous form. The lesions frequently progress to deep scars. Acne agminata can be differentiated into four histopathology groups: epithelioid cell granuloma with necrosis, epithelioid cell granuloma without necrosis, epithelioid cell granuloma with abscesses, and nongranulomatous non-specific inflammatory cell infiltrates.26,27 Special stains to exclude fungal and mycobacterial infections are often necessary in those cases where there is marked granulomatous inflammation.
1126 Diseases of the hair
A
B
Perioral dermatitis is sometimes regarded as a variant of rosacea although it differs clinically.28,29 Patients (particularly young women and children) present with variably pruritic, erythematous microvesicles, scaling, papules, micronodules, and pustules affecting the chin, nasolabial folds, and the periocular region (Fig. 22.206).5,28 Histologically, it is similar to rosacea with spongiotic changes.
Severe D. folliculorum infection (demodicosis) may present with rosacea-like features.30,31 Flushing and telangiectasia are absent.
Histologically, the condition is characterized by follicular cysts with a granulomatous inflammatory reaction and numerous mites (Fig. 22.207).30
Rhinophyma may also be associated with other causes of flushing, such as carcinoid syndrome and alcohol abuse.32
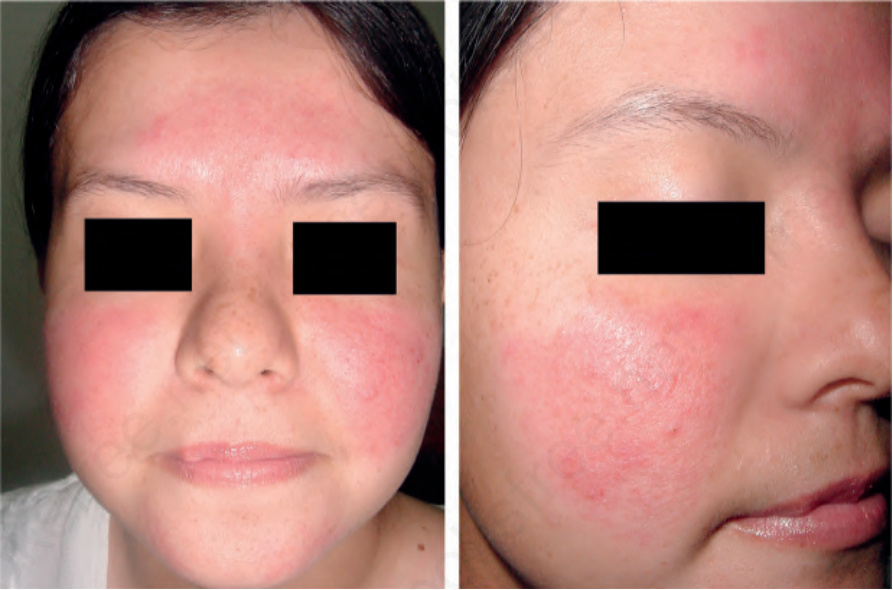
Fig. 22.197 Rosacea erythematotelangiectatic subtype: there is diffuse erythema of the face with malar telangiectasia. By courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
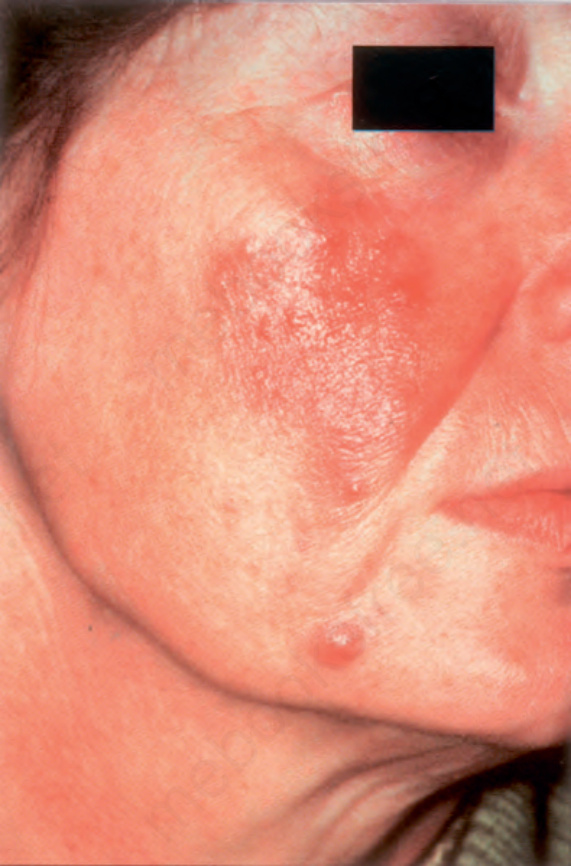
Fig. 22.198 Rosacea papulopustular subtype: note the papules and pustules on the cheek. By courtesy of the Institute of Dermatology, London, UK.

Fig. 22.199 Rosacea phymatous subtype: this is the typical appearance of rhinophyma. Note the irregular surface nodularities and enlargement of the nose. Courtesy of L.M. Gómez, MD, Universidad Pontificia Bolivariana, Medellín, Colombia.

Fig. 22.200 Granulomatous rosacea variant: note the papules which have arisen against a background of rosacea. By courtesy of the Institute of Dermatology, London, UK.
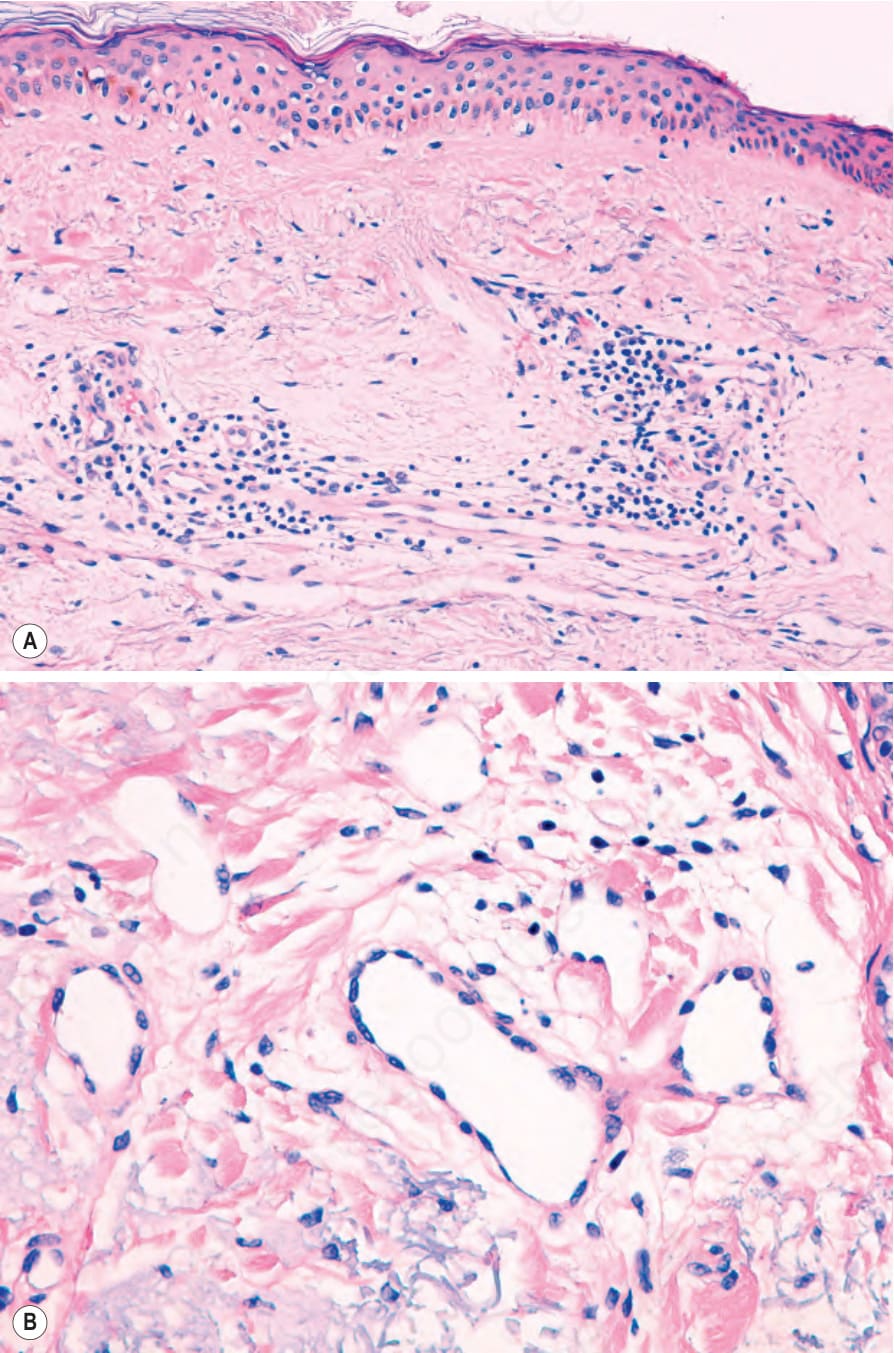
Fig. 22.201 (A, B) Rosacea erythematotelangiectatic subtype: there is edema, telangiectasia, and a mild lymphohistiocytic inflammatory cell infiltrate.
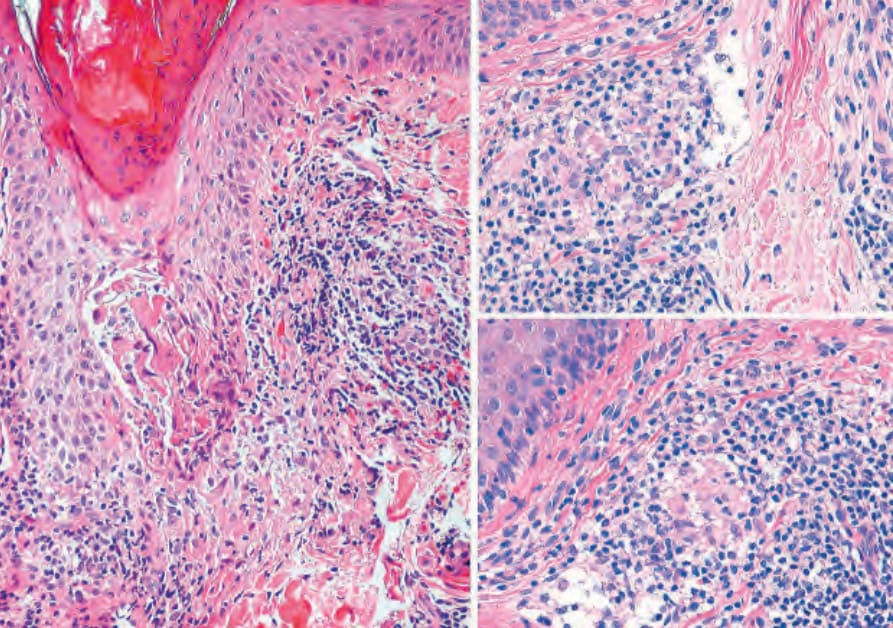
Fig. 22.202 Granulomatous rosacea: note the perifollicular noncaseating granulomata.
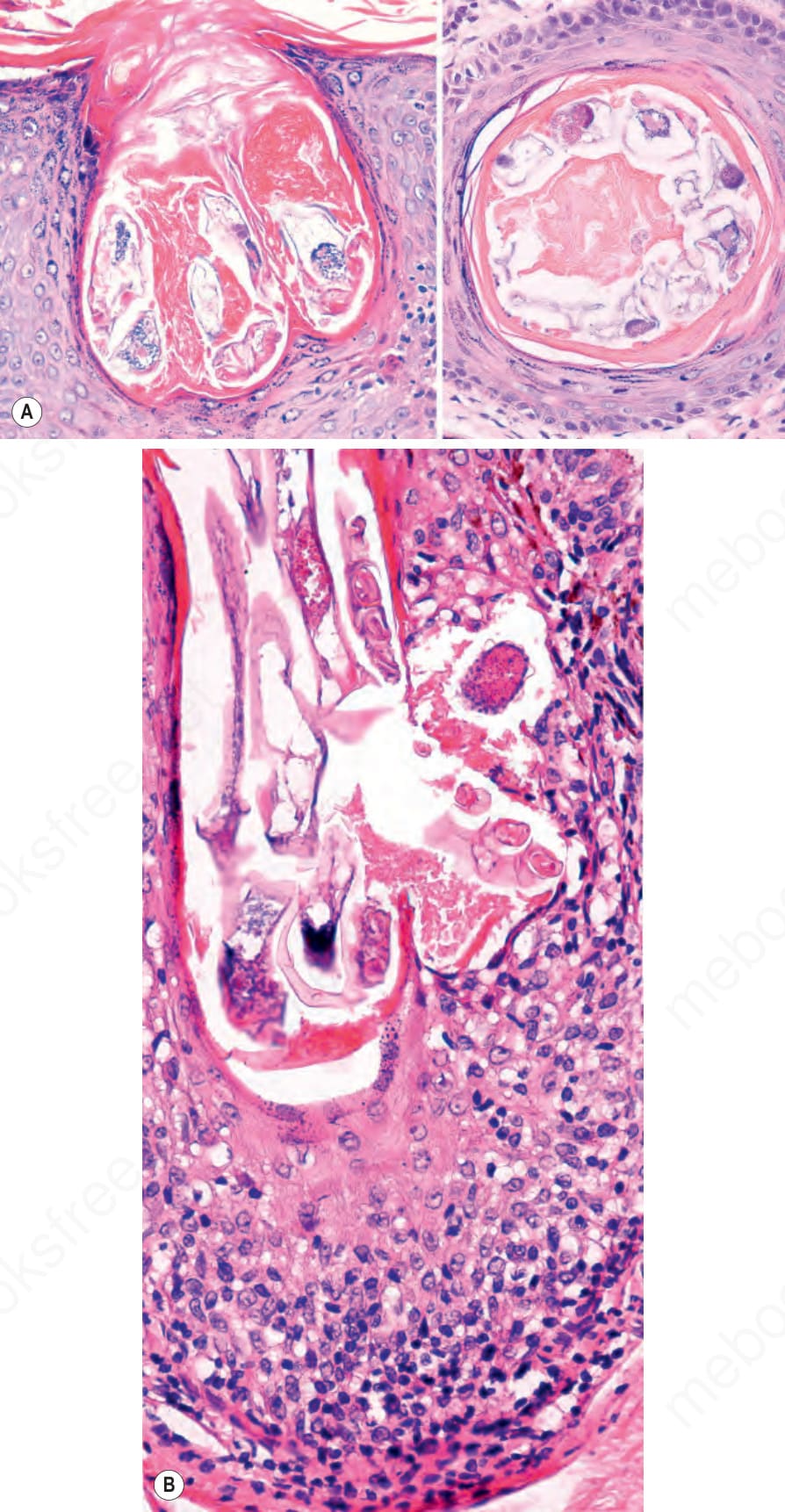
Fig. 22.203 Rosacea: (A) Demodex folliculorum mite (class Arachnida, order Acarina) within this infundibulum in vertical and horizontal sections. (B) Some D. folliculorum mites exiting through a nearby ruptured hair follicle. Note the lymphocytic infiltrate.
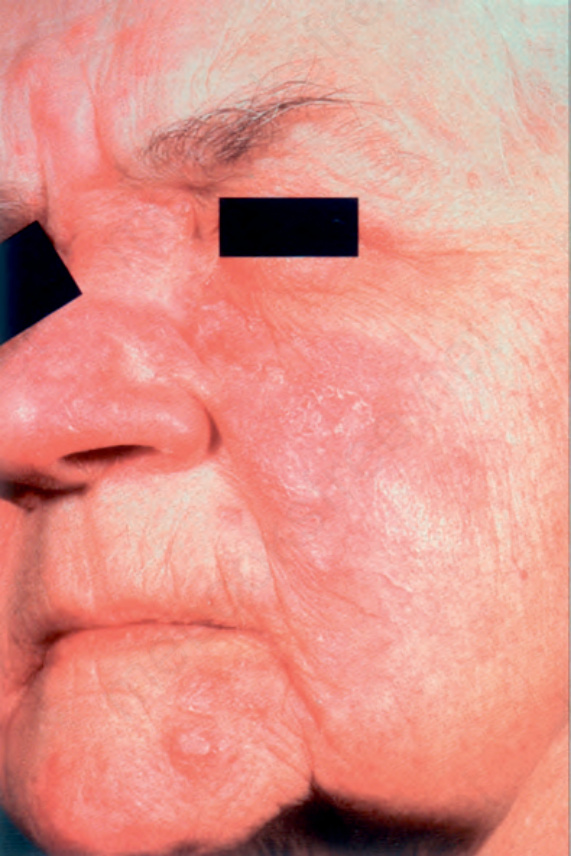
Fig. 22.204 Topical steroid-related rosacea: prolonged topical steroid therapy has resulted in erythema, telangiectasia, and atrophy. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
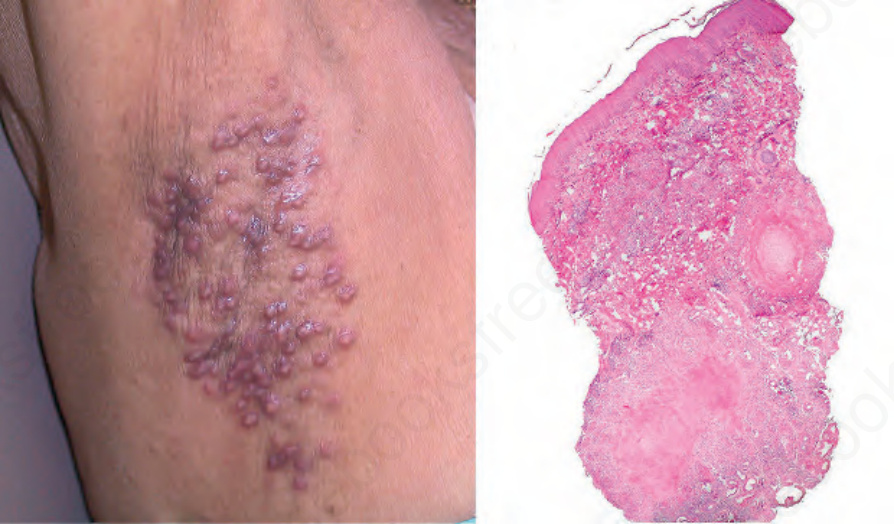
Fig. 22.205 Acne agminata: note some flesh-colored papules and nodules on the axillae (left), and caseating granulomatous inflammation (right). Courtesy of J.E. Arroyave, MD, Hospital Pablo Tobón Uribe, Medellín, Colombia.

Fig. 22.206 Perioral dermatitis: grouped follicular reddish papules and papulovesicles on an eczematous and erythematous base.
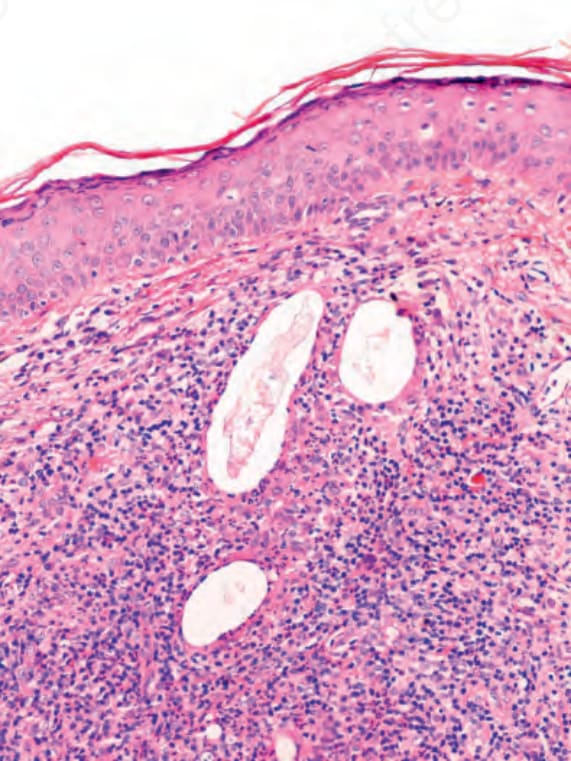
Fig. 22.207 Demodicosis: note some Demodex folliculorum mites free in the dermis, surrounded by an inflammatory cell infiltrate.
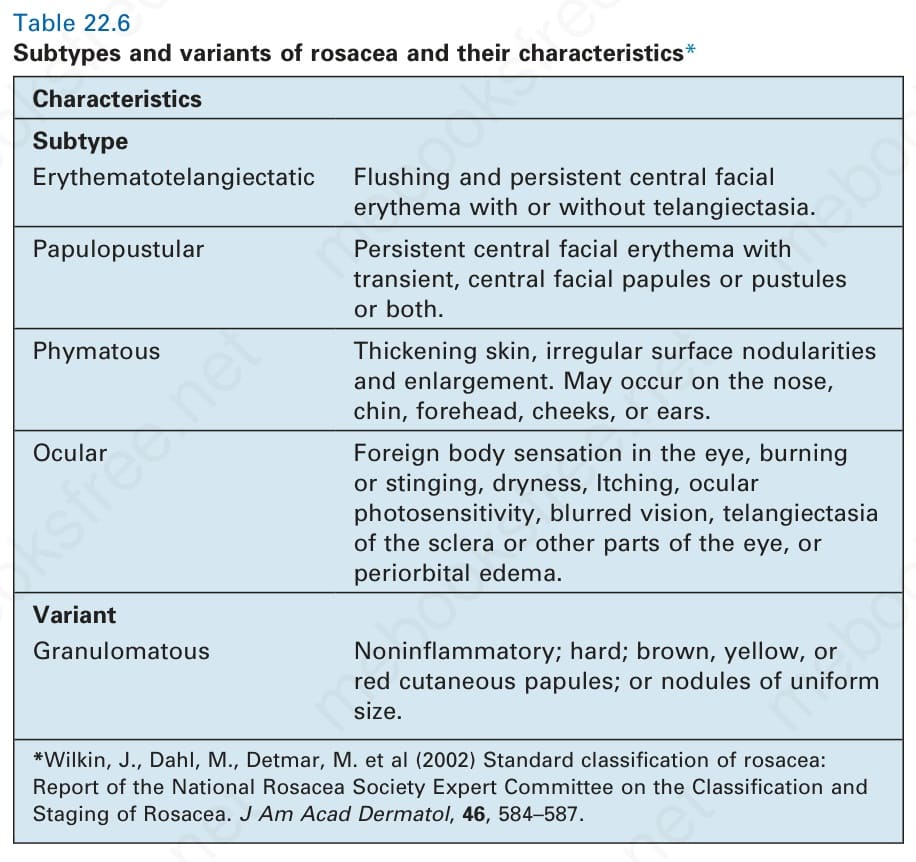
Table 22.6 Subtypes and variants of rosacea and their characteristics*