毛髮扁平苔癬 (Lichen Planopilaris)
Lichen planopilaris
在禿髮斑塊的中央部位,毛囊性過度角化 (follicular hyperkeratosis) 持續存在。在組織學上,圓盤狀紅斑性狼瘡 (discoid lupus erythematosus) 的真皮–表皮交界面變化通常較明顯且屬空泡型 (vacuolar type);而在 lichen planopilaris,毛囊周圍則以苔癬樣特徵 (lichenoid features)(即較呈帶狀的發炎細胞浸潤)為主。其他有助於診斷 lupus erythematosus 的組織學特徵包括較顯著的血管周圍浸潤、真皮黏液 (dermal mucin) 的存在,以及漿細胞 (plasma cells)。
Lichen planopilaris 涵蓋數種具有相似臨床、組織病理及免疫組織病理特徵的變異型:典型毛髮扁平苔癬 (classic lichen planopilaris)、額部纖維化禿髮 (frontal fibrosing alopecia)、呈型態分布的纖維化禿髮 (fibrosing alopecia in a pattern distribution),以及 Graham-Little syndrome。
臨床特徵 (Clinical Features)
典型毛髮扁平苔癬 (Classic lichen planopilaris)
Classic lichen planopilaris 是一種非常常見的瘢痕性禿髮 (scarring alopecia),最早由 Pringle 於 1895 年描述。其特徵為病程多變,導致斑片狀的脫髮區並伴有毛囊發炎。本病較常見於女性 (70%),平均發病年齡為 51 歲。偶有發生於兒童的報告。約 50% 的病人在某個時期會在皮膚其他部位出現典型的扁平苔癬 (lichen planus) 病灶。與頭皮 lichen planopilaris 相關的典型 lichen planus 則甚少觀察到。然而,亦可見指甲及口腔/外陰黏膜的侵犯。
與 pseudopélade of Brocq 的組織學鑑別診斷,是依據 lupus erythematosus 中缺乏明顯發炎、顯著的毛囊栓塞 (follicular plugging)、增厚的基底膜 (thickened basement membrane) 及基底空泡性退化 (basal vacuolar degeneration)。Pseudopélade of Brocq 的特徵為侷限於頭皮、呈白象牙色的禿髮斑塊,具有「雪地足印 (footprints in the snow)」的外觀。
在組織病理學無法確診的病例中,直接免疫螢光 (direct immunofluorescence) 是 discoid lupus erythematosus 鑑別診斷的重要工具。陽性的狼瘡帶試驗 (lupus band test) 可見於多達 83% 的病例,而
常見的臨床症狀包括搔癢、脫屑、壓痛及灼熱感。理學檢查依臨床演變的階段而呈現不同的變化。病灶可為單發或多發,通常侵犯頭皮的頂區 (parietal) 與頭頂區 (vertex)。一般而言,這些表現源於發炎變化與瘢痕形成的混合。發炎的特徵為毛囊性角化丘疹 (follicular keratotic papules)、脫屑及毛囊周圍紅斑 (perifollicular erythema)(見 Fig. 22.110)。瘢痕形成導致脫髮,並伴有擴張的毛囊口 (dilated follicular ostia) 內含角化碎屑 (keratotic debris)(Fig. 22.132)。數根毛幹可能從這些擴張的毛囊口冒出,通常數目少於 3 根。若在疾病晚期檢查頭皮,與其他瘢痕性禿髮(尤其是 pseudopélade of Brocq)重疊的情形很常見。兩者的相似程度,使得部分作者主張這兩種疾病實為同一種病。
1097 Scarring alopecias
在活動期,拔髮試驗 (hair-pull) 與拔毛試驗 (hair-pluck) 會顯示生長期毛髮 (anagen hairs) 數目增加。除切片外,最有用的實驗室檢查包括直接免疫螢光及抗體篩檢,以排除 discoid 與 SLE。
偶爾,lichen planopilaris 可出現於四肢、軀幹及外陰等部位,而不侵犯頭皮。極少數情況下,曾記載過沿著 Blaschko lines 分布的顏面及軀幹線狀分布。另一種可侵犯附屬器結構的 lichen planus 變異型為 lichen planus poritis(汗腺的扁平苔癬,lichen planus of the eccrine glands),它侵犯位於真皮淺層的頂端汗管 (acrosyringium) 與近端小汗管 (proximal eccrine ducts)。
研究,以及在疾病較活動病灶中毛髮易於拔除的現象。
Lichen planopilaris 被視為一種真正的毛髮學急症 (trichologic emergency),應及時開始治療以避免不可逆的脫髮。在此背景下,切片是診斷檢查中不可或缺的一環。從活動性病灶取得適當的切片非常重要,最好取自呈紅斑、脫屑且仍有可輕易拔除、帶生長期樣髮根 (anagen-like hair roots) 之毛囊的區域。如此最有機會辨識出診斷性特徵。取自非活動性或已燃盡 (burned-out) 區域的切片通常無法提供太多資訊,並會導致診斷為原因不明的末期瘢痕性禿髮。
Lichen planopilaris 曾被報告與下列因素相關:暴露於 gold、自體免疫甲狀腺炎 (autoimmune thyroiditis)、psoriasis、刀痕狀硬皮病 (scleroderma en coup de sabre)、疱疹樣皮膚炎 (dermatitis herpetiformis)、持久性色素異常性紅斑 (erythema dyschromicum perstans)、頭皮外傷及霹靂舞 (break dancing)。本病亦曾被報告侷限於一處表皮痣 (epidermal nevus)、與 etanercept 及 imiquimod 治療相關、在全腦放射治療後,以及在毛髮移植與顏面美容手術之後發生。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
雖然 lichen planopilaris 的致病機轉與發生於他處的 lichen planus 相似,但已有數項差異被報告。
Lichen planopilaris 被視為一種毛髮特異性的自體免疫疾病,其中活化的 T 淋巴球以毛囊抗原為標的,主要針對漏斗–峽部區 (infundibulo-isthmic region)(即隆突區,the bulge area)的上皮。在大多數病例中,它不影響毛球 (hair bulb) 或真皮–表皮交界面。此反應所針對的抗原仍屬未知。Lichen planopilaris 曾被報告與 HLA DRB111 及 DQB103 等位基因頻率增加相關。
組織學研究應包含水平切片與垂直切片的檢查(Fig. 22.133)。然而,水平切片可提供特別有價值的資訊,因為浸潤主要侷限於毛囊的漏斗部 (infundibulum) 與峽部區 (isthmic region)。典型表現包括苔癬樣組織反應 (lichenoid tissue reaction),於毛囊上皮內形成凋亡小體 (apoptotic bodies),但很少侵犯其間的表皮。毛囊周圍纖維化 (perifollicular fibrosis) 促使毛囊傾向融合,形成「貓頭鷹眼 (owl eye)」外觀(Fig. 22.134,並見 Fig. 22.117)。毛囊下段與毛球通常不受影響,但在嚴重病例中,下段 (inferior segment) 與球上區 (suprabulbar zone) 亦可能受累。這些變化依疾病進展程度而不均勻,並於活動期及早期病程提供較多資訊。Lichen planopilaris 通常不會呈現一般 lichen planus 所見的典型帶狀浸潤。
部分研究顯示,與 CD4+ T 細胞族群相比,CD8+ T 細胞數目增加,且增殖性隆突幹細胞 (bulge stem cells) 減少。後者支持細胞媒介性細胞毒殺免疫反應 (cell-mediated cytotoxic immune response) 在本病致病機轉中的角色。然而,另一項研究卻顯示,在疾病「早期」活動階段 CD8+ T 細胞數目偏低,且在晚期「纖維化」期隆突幹細胞仍得以保留。這提示毛囊隆突細胞的不可逆喪失,未必是 T 細胞媒介破壞的結果。在 lichen planopilaris 病因發生機轉中另一項重要發現,是觀察到受侵犯之毛囊角質細胞中 integrins 分布的改變,促使毛囊角質細胞與基質間黏附力的喪失。這也可能解釋了在組織學
界面變化的特徵為毛囊上皮與周圍真皮之間附著的局部喪失。因此,有時可見人工裂隙 (artifactual clefts),且常可發現膠樣小體 (colloid bodies)。在毛囊周圍結締組織鞘(通常增厚)內,存在相關的單核發炎細胞浸潤(Fig. 22.135)。受侵犯區域的基底毛囊角質細胞變得鱗狀化 (squamotized),體積增大、具有顯著的嗜伊紅性細胞質及細胞質成角 (cytoplasmic angulation)(Fig. 22.136)。雖然毛囊周圍可觀察到黏液樣毛囊周圍纖維增生 (mucinous perifollicular fibroplasia),但並無真皮黏液 (dermal mucin) 的堆積(Fig. 22.137,見 Fig. 22.111)。
在晚期,毛囊完全被破壞,並由硬化性膠原性毛囊瘢痕 (sclerotic collagenous follicular scar) 取代,伴隨皮脂腺 (sebaceous glands) 的喪失。唯一殘留的結構是豎毛肌 (arrector pili muscles)(見 Fig. 22.115)。有時,主要型態為環繞游離毛幹 (free hair shafts) 分布的異物肉芽腫 (foreign body granulomas)(Fig. 22.138)。其他形式的
1098 Diseases of the hair
毛囊的漏斗部。免疫球蛋白(通常為 IgG 或 IgA)侷限於毛囊上皮的線狀沉積亦曾被描述。然而,這些免疫螢光發現對 lichen planopilaris 並無特異性,亦可見於其他具有界面變化及基底細胞層損傷的疾病。纖維帶內雙折射 (birefringence) 增加是 lichen planopilaris 的常見發現,但偶爾也可見於其他瘢痕性與非瘢痕性禿髮(見 Fig. 22.113)。
瘢痕性禿髮(包括 pseudopélade of Brocq 與 discoid lupus erythematosus)共有此末期組織學外觀。為了凸顯瘢痕組織的存在,用以勾勒彈性纖維 (elastic fibers) 的特殊染色特別有用。它們可區分正常真皮與瘢痕區域,因為後者缺乏彈性纖維。可辨識出毛囊周圍與淺層的楔形瘢痕,環繞纖維帶的彈性鞘 (elastic sheath) 喪失,但偶爾也可見於其他瘢痕性禿髮(Fig. 22.139)。
免疫螢光研究顯示膠樣小體被 IgM 與 IgA 染色,並沿著基底膜呈線狀的纖維蛋白 (fibrin) 沉積,位於
鑑別診斷 (Differential Diagnosis)
在大多數病例中,可藉由仔細關聯組織病理、臨床及免疫組織病理的發現而獲得正確診斷。鑑別診斷中最重要需考慮的疾病為 discoid lupus erythematosus 與 pseudopélade of Brocq。
在 discoid lupus erythematosus 中,典型發現包括淺層與深層的血管周圍淋巴組織球性浸潤 (perivascular lymphohistiocytic infiltrate)、真皮黏液,以及不僅影響毛囊、也影響其間真皮–表皮交界 (dermal–epidermal junction) 的空泡性界面變化。在 lichen planopilaris 中,浸潤主要見於毛囊周圍,而毛囊間表皮 (interfollicular epidermis) 的界面變化則甚少出現。
1099 Scarring alopecias
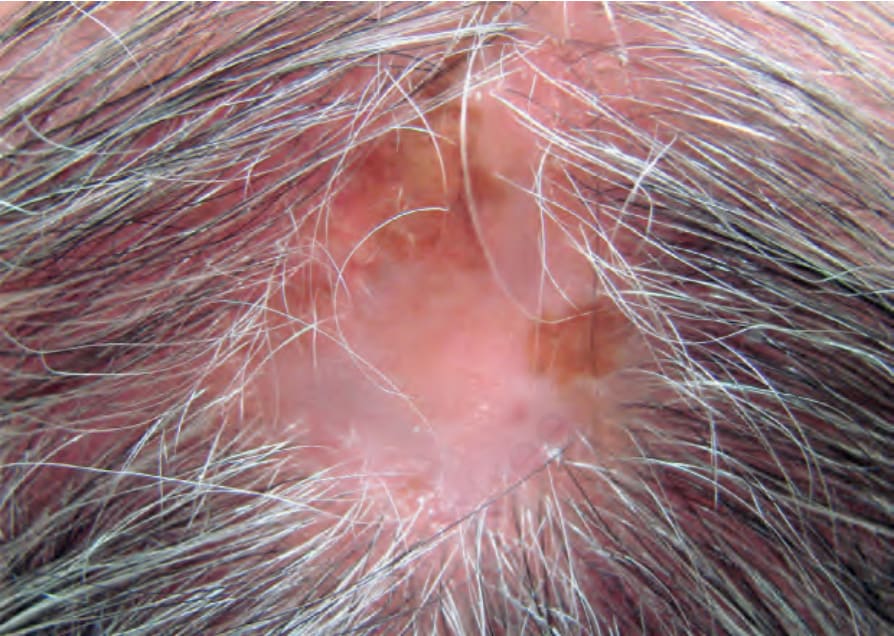
圖 22-110:瘢痕性禿髮,lichen planopilaris:可見一處禿髮斑塊,伴有色素增加與減少、毛囊口喪失,以及周邊的毛囊性過度角化 (follicular hyperkeratosis)。Courtesy of J. Gutiérrez, MD, Instituto de Ciencias de la Salud, Medellín, Colombia.
Fig. 22.110 Scarring alopecia, lichen planopilaris: there is a plaque of alopecia with hyper- and hypopigmentation, loss of follicular ostia, and follicular hyperkeratosis at the periphery. Courtesy of J. Gutiérrez, MD, Instituto de Ciencias de la Salud, Medellín, Colombia.
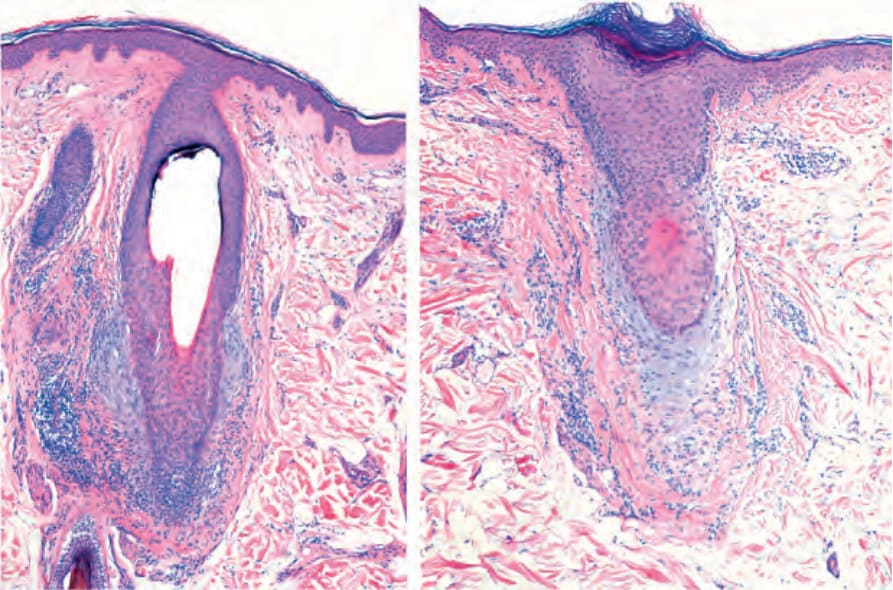
圖 22-111:瘢痕性禿髮,lichen planopilaris。注意峽部 (isthmus) 周圍的發炎浸潤。可見毛囊周圍纖維化 (perifollicular fibrosis)、毛囊周圍黏液沉積 (perifollicular mucin deposition),以及皮脂腺 (sebaceous glands) 的完全喪失。
Fig. 22.111 Scarring alopecia, lichen planopilaris. Note the inflammatory infiltrate around the isthmus. There is perifollicular fibrosis, perifollicular mucin deposition and complete loss of sebaceous glands.
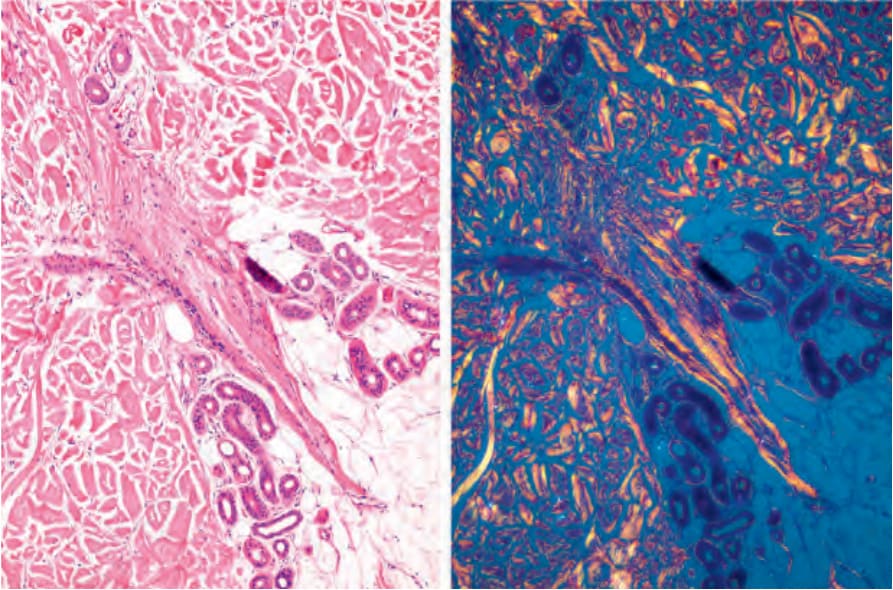
圖 22-113:瘢痕性禿髮,lichen planopilaris,毛囊纖維帶 (follicular tracts)。注意偏光下纖維帶中膠原蛋白的雙折射 (birefringence)。
Fig. 22.113 Scarring alopecia, lichen planopilaris, follicular tracts. Note the birefringence of the collagen in the fibrous tract with polarized light.
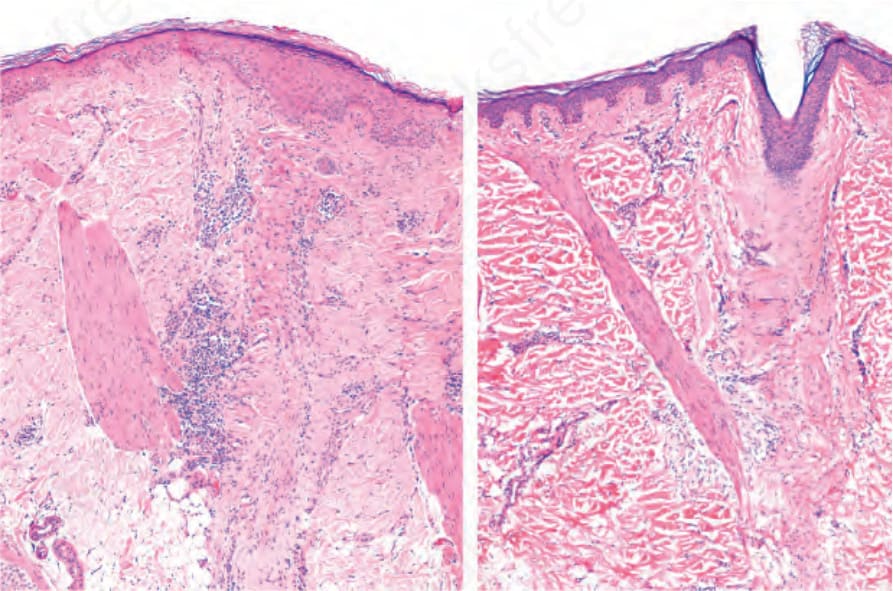
圖 22-115:瘢痕性禿髮,lichen planopilaris:毛囊已消失,並由兩條垂直的纖維瘢痕 (fibrous scars) 取代,其中插入一條豎毛肌 (arrector pili muscle)。
Fig. 22.115 Scarring alopecia, lichen planopilaris: the hair follicles have disappeared and been replaced by two vertical fibrous scars in which an arrector pili muscle is inserted.
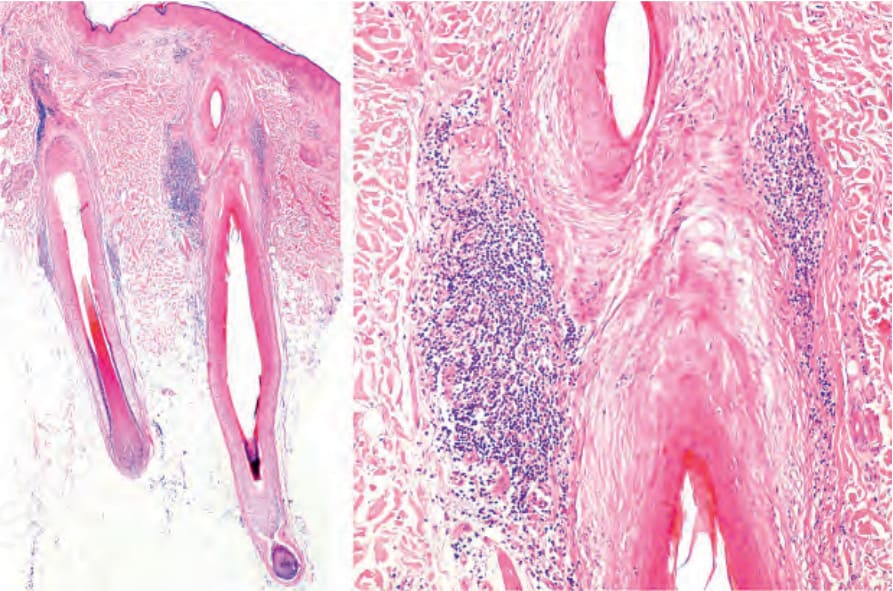
圖 22-117:瘢痕性禿髮,lichen planopilaris:注意上段以及豎毛肌 (arrector pili muscle) 插入區域的淋巴球浸潤。在右圖中,注意皮脂腺 (sebaceous glands) 的喪失以及內毛根鞘 (internal root sheath) 的過早脫落。
Fig. 22.117 Scarring alopecia, lichen planopilaris: note the lymphocytic infiltrate in the upper segment and in the area of insertion of the arrector pili muscle. In the figure on the right, note the loss of sebaceous glands and the premature shedding of the internal root sheath.
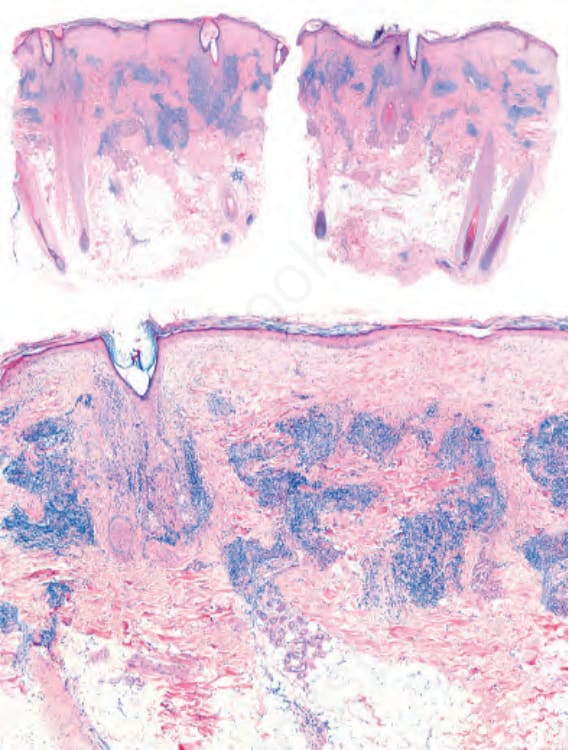
圖 22-130:圓盤狀紅斑性狼瘡 (discoid lupus erythematosus):顯著的發炎細胞浸潤位於毛囊上段周圍,亦位於血管周圍位置。
Fig. 22.130 Discoid lupus erythematosus: Prominent inflammatory cell infiltrate located around the upper segment of the hair follicles and also in a perivascular location.

圖 22-132:Lichen planopilaris:萎縮性斑片,伴有毛囊孔 (follicular orifices) 喪失、毛囊周圍紅斑 (perifollicular erythema) 與脫屑。Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
Fig. 22.132 Lichen planopilaris: atrophic patch with loss of follicular orifices, perifollicular erythema, and scaling. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
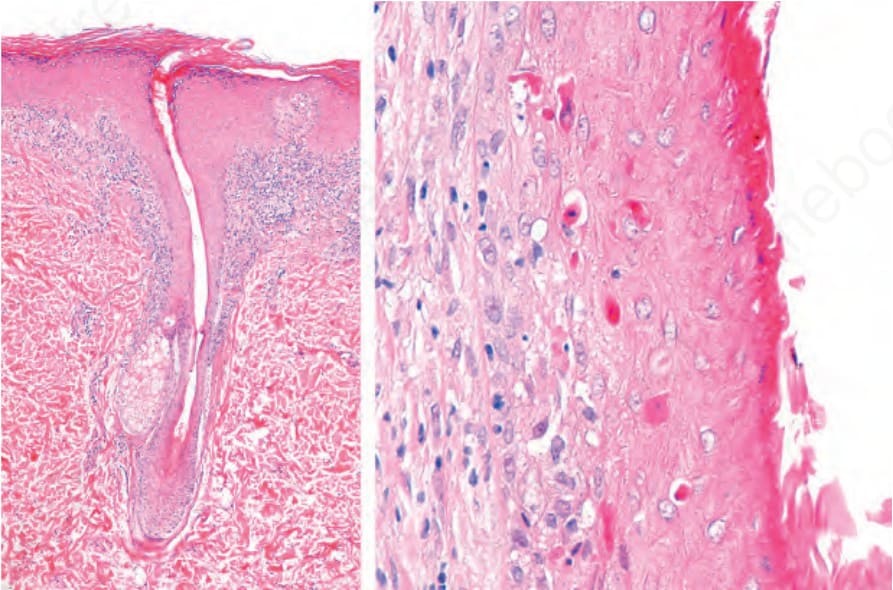
圖 22-133:Lichen planopilaris,垂直切片。左:發炎細胞浸潤環繞上段而不侵犯下段。可見皮脂腺的完全喪失。在這些病例中,一項罕見的發現是表皮下帶狀發炎細胞浸潤 (subepidermal bandlike inflammatory cell infiltrate)。右:外毛根鞘 (outer root sheath) 內可見眾多凋亡小體 (apoptotic bodies)。可見內毛根鞘 (internal root sheath) 的脫落。
Fig. 22.133 Lichen planopilaris, vertical sections. Left: the inflammatory cell infiltrate surrounds the superior segment without involving the inferior segment. There is complete loss of sebaceous glands. In these cases, an infrequent finding is the subepidermal bandlike inflammatory cell infiltrate. Right: numerous apoptotic bodies are seen in the outer root sheath. There is shedding of the internal root sheath.
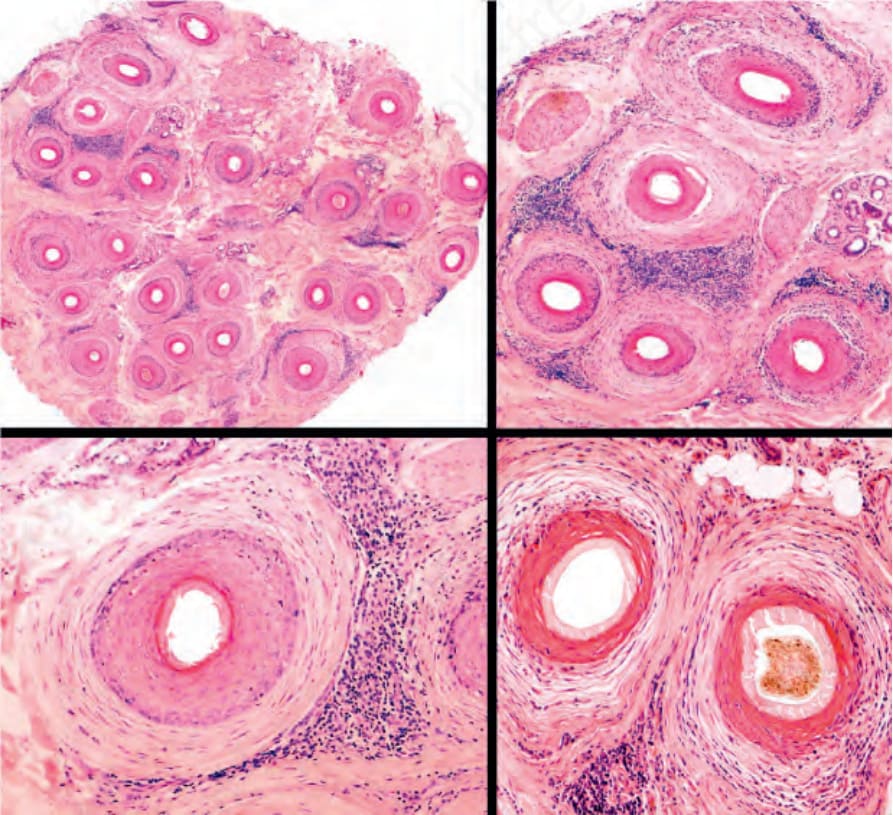
圖 22-134:Lichen planopilaris,水平切片:在此切片中無皮脂腺,且所有毛囊均顯示毛囊周圍單核發炎細胞浸潤 (perifollicular mononuclear inflammatory cell infiltrate)。大多數毛囊顯示板層狀纖維增生 (lamellar fibroplasia),將淋巴球浸潤與外毛根鞘 (outer root sheath) 分隔開來。在右側上、下兩圖中,可見「貓頭鷹眼 (owl eye)」外觀。
Fig. 22.134 Lichen planopilaris, horizontal sections: in this biopsy, there are no sebaceous glands and all the follicles show a perifollicular mononuclear inflammatory cell infiltrate. Most hair follicles show lamellar fibroplasia separating the lymphocytic infiltrate from the outer root sheath. In the right panel, upper and lower images, an ‘owl eye’ appearance is appreciated.
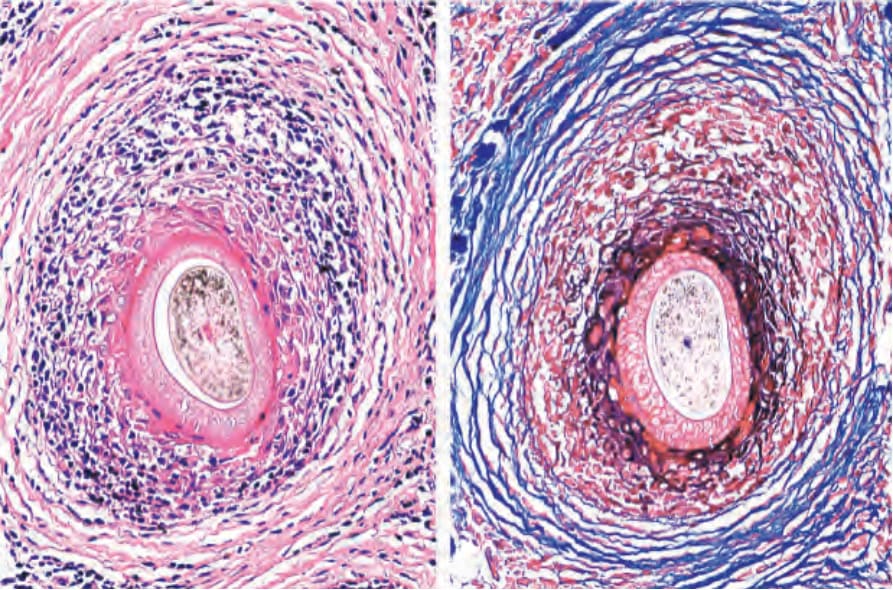
圖 22-135:Lichen planopilaris,額部纖維化禿髮型 (frontal fibrosing alopecia type):水平切片。左:外毛根鞘 (outer root sheath) 的破壞明顯,伴有界面變化、纖維化及淋巴球發炎。右:以 Mason trichrome 染色,環繞單核細胞浸潤的板層狀纖維化 (lamellar fibrosis) 清晰可見。
Fig. 22.135 Lichen planopilaris, frontal fibrosing alopecia type: horizontal sections. Left: the destruction of the outer root sheath is evident with interface change, fibrosis and lymphocytic inflammation. Right: with the Mason trichrome staining, the lamellar fibrosis around the mononuclear cell infiltrate is apparent.
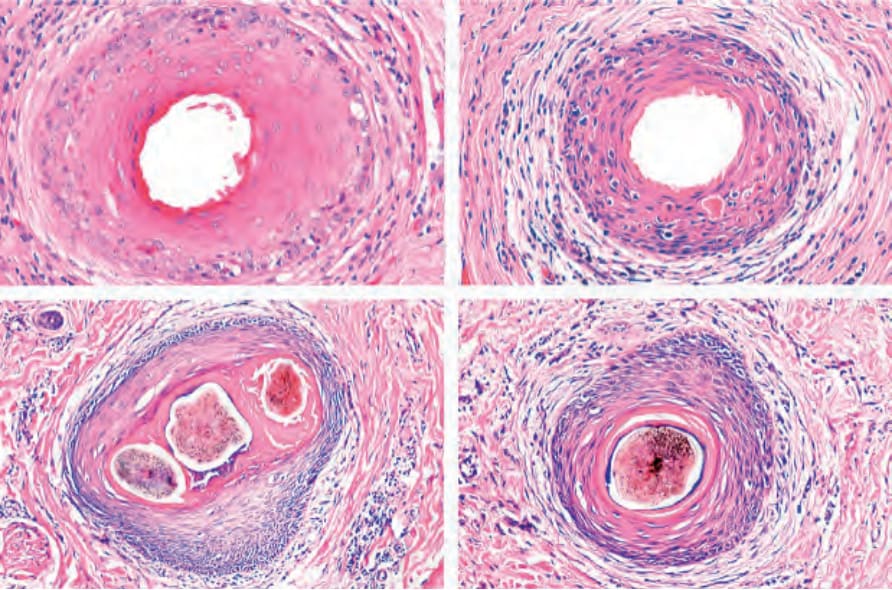
圖 22-136:Lichen planopilaris,水平切片:典型變化的照片組合。(上)初期變化伴隨凋亡 (apoptosis) 及內毛根鞘 (internal root sheath) 喪失。(下)進展期變化伴隨毛囊融合及外毛根鞘 (outer root sheath) 變薄。
Fig. 22.136 Lichen planopilaris, horizontal sections: photographic composition of the typical changes. (Top) Initial changes with apoptosis and loss of internal root sheath. (Bottom) Advanced changes with fusion of follicles and thinning of the outer root sheath.
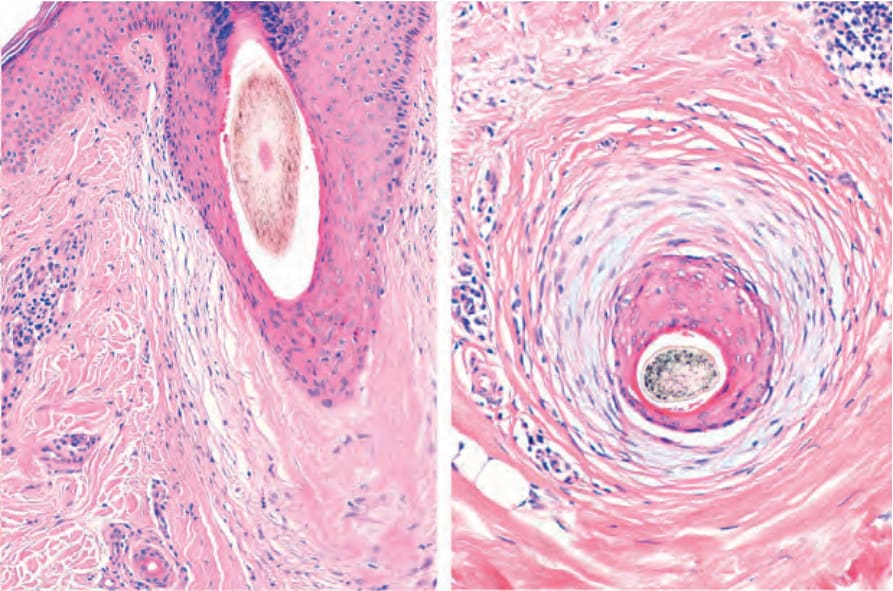
圖 22-137:Lichen planopilaris,垂直與水平切片:可見黏液樣毛囊周圍纖維增生 (mucinous perifollicular fibroplasia)。
Fig. 22.137 Lichen planopilaris, vertical and horizontal sections: there is mucinous perifollicular fibroplasia.
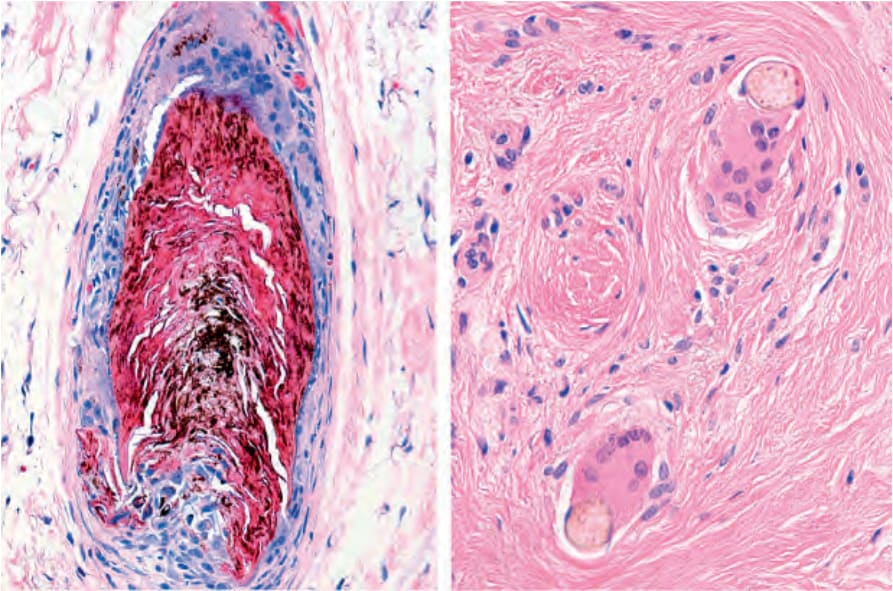
圖 22-138:Lichen planopilaris:真皮中環繞游離毛幹 (free hair shafts) 可見眾多巨細胞 (giant cells) 與上皮樣細胞 (epithelioid cells)。
Fig. 22.138 Lichen planopilaris: there are numerous giant and epithelioid cells surrounding the free hair shafts in the dermis.
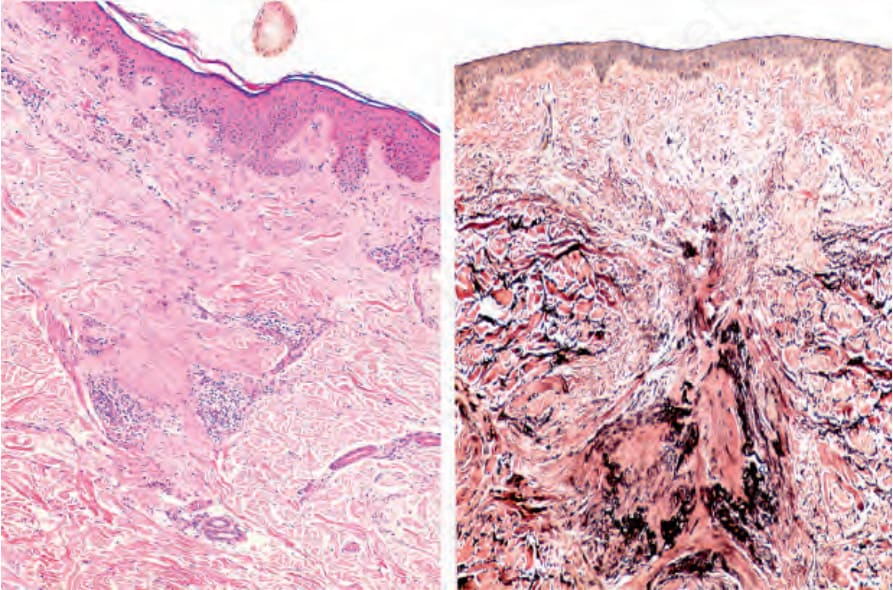
圖 22-139:Lichen planopilaris。左:毛囊瘢痕從表皮延伸至深層真皮。右:以彈性纖維染色 (elastic stain),可見彈性纖維喪失呈三角形、其底部朝向表皮。毛囊瘢痕顯示彈性纖維呈垂直方向的濃聚 (condensation)。
Fig. 22.139 Lichen planopilaris. Left: follicular scar extending from the epidermis to the deep dermis. Right: With the elastic stain loss of elastic fibers in triangular shape with the base toward the epidermis is observed. The follicular scarring shows condensation of elastic fibers with a vertical orientation.
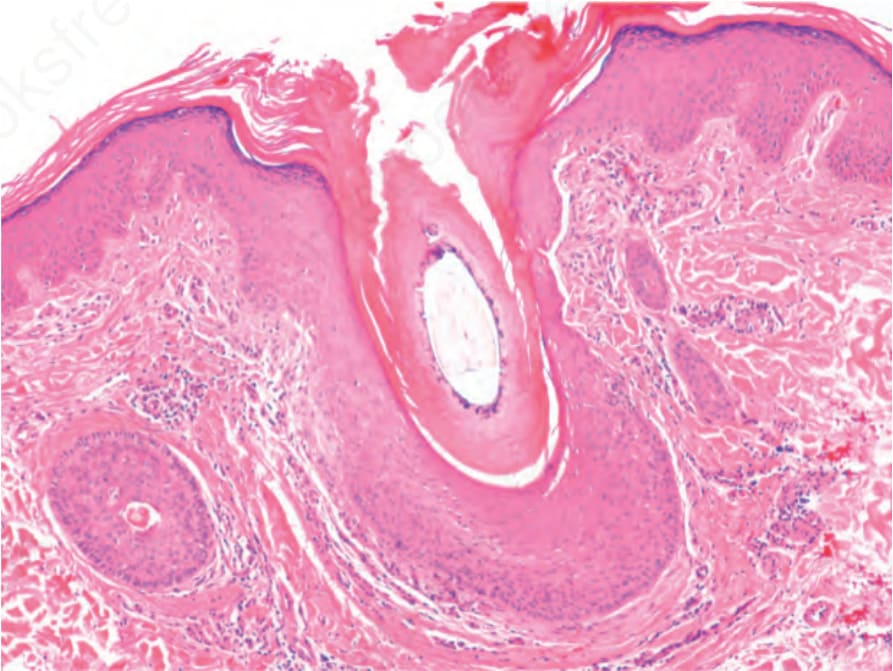
圖 22-146:Graham-Little syndrome:擴張的漏斗部 (dilated infundibulum) 伴有過度角化 (hyperkeratosis)、輕度毛囊周圍發炎及纖維化。
Fig. 22.146 Graham-Little syndrome: dilated infundibulum with hyperkeratosis, mild perifollicular inflammation and fibrosis.
Pseudopélade of Brocq 表現為進行性的瘢痕性禿髮斑片,組織學上其變化基本上為明顯的瘢痕形成而無界面變化。Pseudopélade of Brocq 可能代表多種形式瘢痕性禿髮(包括 lichen planopilaris)的晚期階段。
在疾病的末期,可能無法將 lichen planopilaris 與 pseudopélade of Brocq 及 discoid lupus erythematosus 區分開來。乳頭層真皮 (papillary dermis) 出現一條纖維化帶,並伴隨網狀層真皮 (reticular dermis) 中沿著被破壞毛囊路徑的纖維帶,這似乎是指向 lichen planopilaris 「燃盡 (burn-out)」病灶的有價值線索。
臨床特徵 — 額部纖維化禿髮 (Clinical Features — Frontal Fibrosing Alopecia)
Kossard 於 1994 年首次描述額部纖維化禿髮 (frontal fibrosing alopecia),將其視為一種與 lichen planus 密切相關、主要侵犯停經後婦女的瘢痕性禿髮變異型(停經後額部纖維化禿髮,postmenopausal frontal fibrosing alopecia)。然而,部分病例亦曾被報告於停經前婦女,以及男性的
鬢角與鬍鬚,與非裔病人身上。此外,亦曾有一些發生於兒童與青少年的病例被描述。
本病表現為前額髮際線進行性且對稱性的後退,並伴有平滑而蒼白的皮膚。有時可觀察到毛囊周圍紅斑 (perifollicular erythema)、毛囊角化 (follicular keratinization),並延伸至顳區與頂區 (temporal and parietal zones)(Fig. 22.140)。此外,眉毛、臉部其餘部分,以及四肢、腋下、軀幹與陰部的毛囊也會喪失或減少(Fig. 22.141)。一般認為眉毛禿髮先於頭皮禿髮發生。
進展難以預測,但幾乎所有病人的疾病最終都趨於穩定。臨床上,本病不會呈現 lichen planus 或 pseudopélade of Brocq 典型可見的多灶性脫髮區。通常在他處並無 lichen planus 的表現,雖然個別病例曾在皮膚或黏膜出現典型 lichen planus,尤其是色素性扁平苔癬 (pigmented lichen planus)。在部分病人中,曾描述過瀰漫性脫髮。
1100 Diseases of the hair
A B
其他病例曾被報告與下列情形相關:Piccardi-Lassueur-Graham-Little syndrome 的某些組成成分、Sjögren syndrome、雙側卵巢切除 (bilateral oophorectomy)、額部纖維化禿髮斑塊附近的毛髮再色素化 (hair repigmentation)、針對雄性禿 (androgenetic alopecia) 的毛髮移植、頭皮出汗增加,以及頭皮白斑 (scalp vitiligo)。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
額部纖維化禿髮的致病機轉仍屬未知。曾觀察到某些家族群聚共有 HLA-D,但此非一致性的發現。本病被視為 lichen planopilaris 的額部變異型,因為組織學發現相似。然而,其他研究發現在受侵犯之毛囊類型方面有所差異,強調本病對毳毛樣 (vellus-like) 與不確定型 (indeterminate) 毛囊的選擇性侵犯。與 lichen planopilaris 相似,組織學變化不一定侷限於頭皮,亦可見於眉毛、臉部及上肢,即使在無症狀的病人也是如此。
診斷纖維性額部禿髮 (fibrous frontal alopecia) 最佳的切片,是在皮膚鏡 (dermoscopy) 引導下取得並以水平切片判讀者。組織學研究顯示毛囊數目減少,被纖維帶 (fibrous tracts) 所取代。可見呈苔癬樣型態的淋巴球浸潤,伴隨毛囊周圍板層狀纖維化 (perifollicular lamellar fibrosis)(Fig. 22.142)。本病在初始狀態時,傾向同時侵犯處於各週期階段(包括休止期,telogen)的終毛 (terminal)、不確定型 (indeterminate) 及毳毛 (vellus) 毛囊。隨著疾病進展,侵犯範圍較侷限於終毛毛囊。有時,凋亡 (apoptosis) 很顯著(Fig. 22.143,見 Fig. 22.135)。毛囊間表皮 (interfollicular epidermis) 不受侵犯。其免疫螢光型態與其他較傳統的 lichen planus 變異型相似。
禿髮,發炎浸潤極輕微,組織學畫面以毛囊微小化 (follicular miniaturization) 為主。牽引性禿髮 (traction alopecia) 可依理學檢查及毛髮牽引病史輕易區分。
鑑別診斷 (Differential Diagnosis)
鑑別診斷包括女性型落髮 (female pattern hair loss)、雄性禿 (androgenetic alopecia)、呈「sisaipho」型態(ophiasis inversus)的圓禿 (alopecia areata),以及邊緣性牽引性禿髮 (marginal traction alopecia)。
Female pattern hair loss 與 androgenetic alopecia 不伴有毛囊周圍紅斑,且 female pattern hair loss 與前額髮際後退無關。在 alopecia areata 中,可觀察到非發炎性的禿髮帶,伴有毛囊孔的保留及驚嘆號毛 (exclamation mark hairs) 的存在。皮膚鏡可能是有助益的診斷工具,因為 alopecia areata 中典型可見的黃點 (yellow dots) 在 frontal fibrosing alopecia 中並不存在。組織學上,在 frontal fibrosing alopecia 中浸潤位於峽部 (isthmus) 周圍,而在 alopecia areata 中浸潤位於毛球周圍區 (peribulbar area)。在 female pattern hair loss 及 androgenetic
最後,若無適當的臨床資訊,則無法與傳統的 lichen planopilaris 區分。
臨床特徵 — 呈型態分布的纖維化禿髮 (Clinical Features — Fibrosing Alopecia in a Pattern Distribution)
呈型態分布的纖維化禿髮 (fibrosing alopecia in a pattern distribution) 由 Zinkernagel 與 Trüeb 所描述,為一種與雄性禿 (androgenic alopecia) 及 lichen planopilaris 共有相似特徵的禿髮。它同時侵犯女性與男性。臨床上其特徵為頭皮中央部位毛髮的進行性微小化 (miniaturization)、毛囊周圍紅斑及毛囊性過度角化,導致毛囊口的完全喪失與瘢痕形成(Fig. 22.144)。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
呈型態分布的纖維化禿髮其致病機轉仍屬未知。組織學特徵包括毛囊微小化,並於峽部 (isthmus) 與漏斗部 (infundibulum) 區域伴有淋巴球性
1101 Scarring alopecias
發炎細胞浸潤(Fig. 22.145)。晚期病灶的特徵為毛囊周圍板層狀纖維化 (perifollicular lamellar fibrosis) 與纖維性毛囊帶 (fibrous follicular tracts)。
鑑別診斷 (Differential Diagnosis)
鑑別診斷包括 androgenetic alopecia、lichen planopilaris 及 frontal fibrosing alopecia。雖然在 androgenetic alopecia 中可見漏斗部周圍淋巴球性發炎細胞浸潤(見 Figs 22.17 與 Fig. 22.46),但此浸潤不會集中於峽部周圍,且無凋亡、皮脂腺喪失或板層狀纖維化。Lichen planus 則與上述所有特徵相關,但發炎不會侵犯毳毛,且缺乏毛囊微小化。在 frontal fibrosing alopecia 的初期階段,可能以毳毛的侵犯為主。在這些病例中,密切的臨床病理關聯是必要的。
侵犯異位性 (atopic) 個體。其特徵為頭皮、眉毛及睫毛的斑片狀禿髮。臨床病程難以預測:部分病例在青春期消退,其他則以不同的強度進展。

圖 22-140:額部纖維化禿髮 (frontal fibrosing alopecia):額顳髮際線呈帶狀後退,伴有外側眉毛稀疏。注意前額頭皮的孤立毛髮。Courtesy of L.M. Gómez, MD, Universidad Pontificia Bolivariana, Medellín, Colombia.
Fig. 22.140 Frontal fibrosing alopecia: bandlike recession of the frontotemporal hairline associated with lateral eyebrow thinning. Note the solitary hairs in the frontal scalp. Courtesy of L.M. Gómez, MD, Universidad Pontificia Bolivariana, Medellín, Colombia.
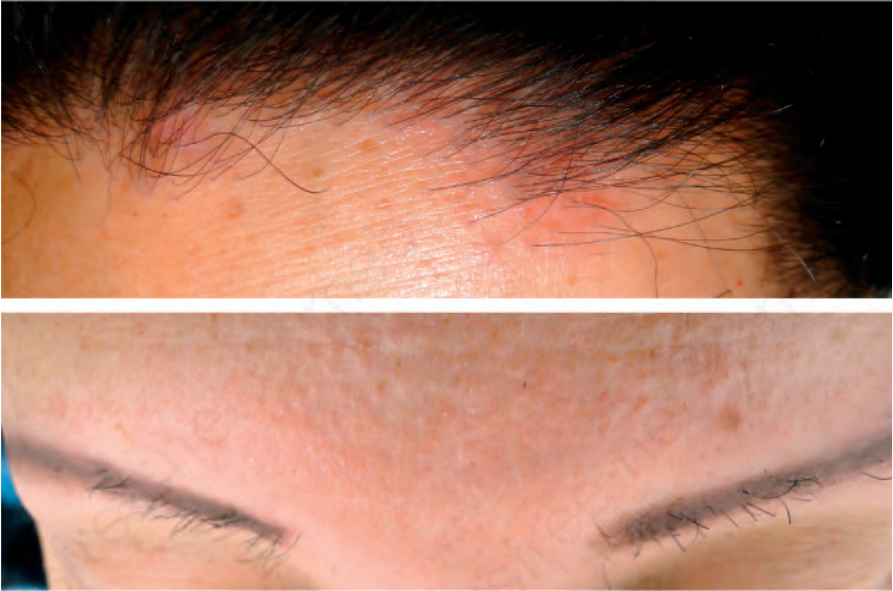
圖 22-141:額部纖維化禿髮。上:前額頭皮可見脫髮。皮膚顯示毛囊周圍紅斑 (perifollicular erythema)。下:皮膚呈輕度瘢痕化,伴有毛囊突出及發炎。眉毛幾乎完全缺失。
Fig. 22.141 Frontal fibrosing alopecia. Above: there is hair loss on the frontal scalp. The skin shows perifollicular erythema. Below: the skin appears mildly scarred with prominence of the follicles and inflammation. There is almost total absence of eyebrows.
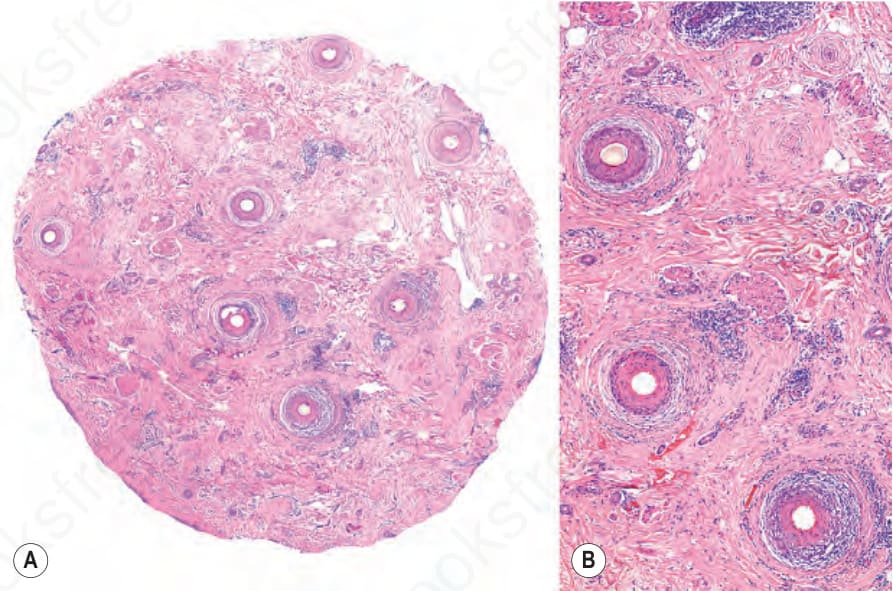
圖 22-142:額部纖維化禿髮,水平切片。(A) 在此掃描放大下,可見皮脂腺缺失、毛囊喪失,以及毛囊周圍纖維化。(B) 外毛根鞘 (outer root sheath) 的苔癬樣界面皮膚炎 (lichenoid interface dermatitis),伴有空泡變化、淋巴球發炎及毛囊周圍板層狀纖維化。
Fig. 22.142 Frontal fibrosing alopecia, horizontal section. (A) In this scanning magnification, there is absence of sebaceous glands, loss of hair follicles, and perifollicular fibrosis. (B) Lichenoid interface dermatitis of the outer root sheath, with vacuolar change, lymphocytic inflammation and perifollicular lamellar fibrosis.
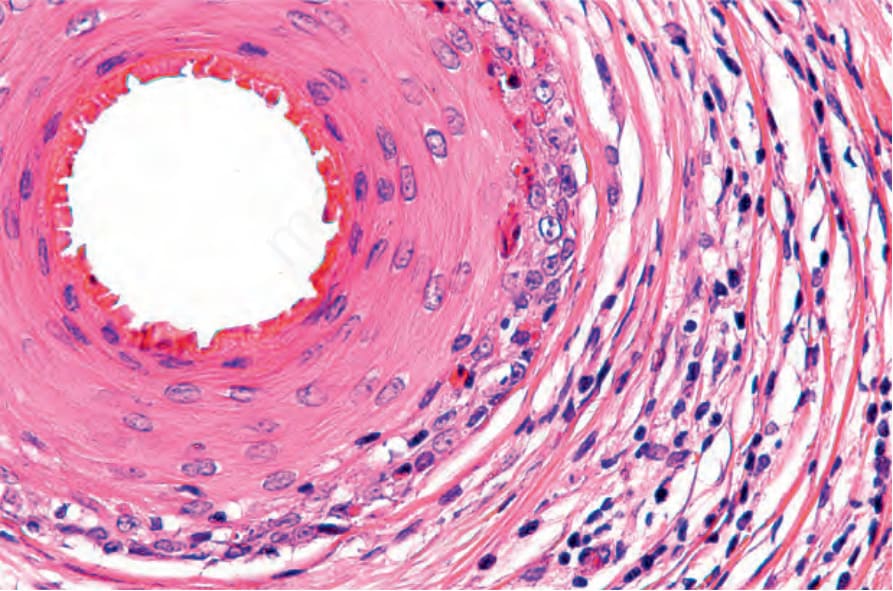
圖 22-143:額部纖維化禿髮,水平切片。外毛根鞘 (outer root sheath) 的破壞明顯,伴有界面變化、眾多凋亡小體 (apoptotic bodies)、纖維化及淋巴球發炎。
Fig. 22.143 Frontal fibrosing alopecia, horizontal section. The destruction of the outer root sheath is evident with interface change, numerous apoptotic bodies, fibrosis, and lymphocytic inflammation.

圖 22-144:Lichen planopilaris,呈型態分布的纖維化禿髮 (fibrosing alopecia in a pattern distribution)。左:注意毛囊孔缺失,並伴有雄性禿型態的色素改變。右:一名罹患 androgenetic alopecia 且伴毛囊發炎的男性病人。Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.
Fig. 22.144 Lichen planopilaris, fibrosing alopecia in a pattern distribution. Left: note the absence of follicular orifices with pigment alteration in the pattern of androgenetic alopecia. Right: a male patient with androgenetic alopecia and follicular inflammation. Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.
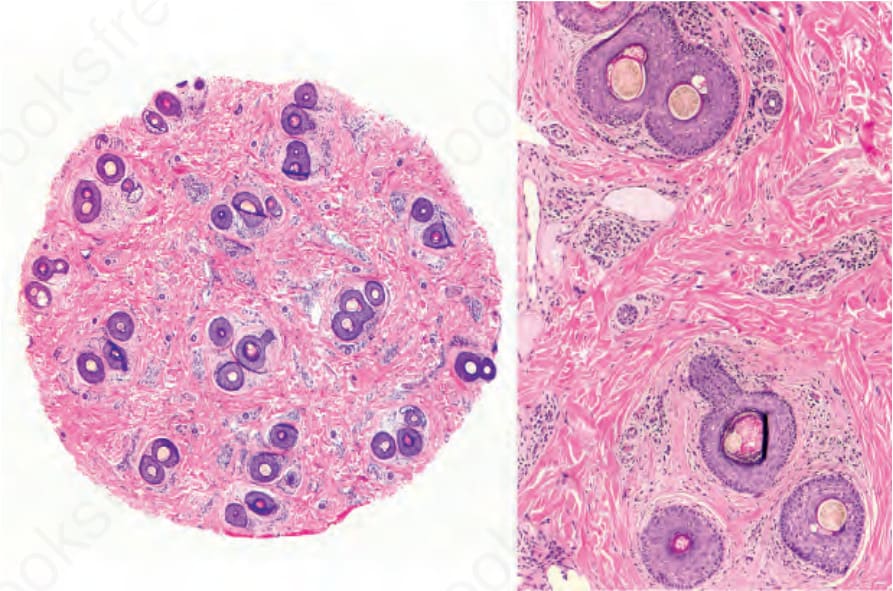
圖 22-145:Lichen planopilaris,呈型態分布的纖維化禿髮:水平切片。廣泛的微小化伴隨皮脂腺喪失、不明顯的纖維化及毛囊周圍淋巴球發炎。Courtesy of Y. Corredoira Salum, MD, Universidad de Chile, Santiago, Chile.
Fig. 22.145 Lichen planopilaris, fibrosing alopecia in a pattern distribution: horizontal section. Extensive miniaturization with loss of sebaceous glands, discrete fibrosis and perifollicular lymphocyte inflammation. Courtesy of Y. Corredoira Salum, MD, Universidad de Chile, Santiago, Chile.
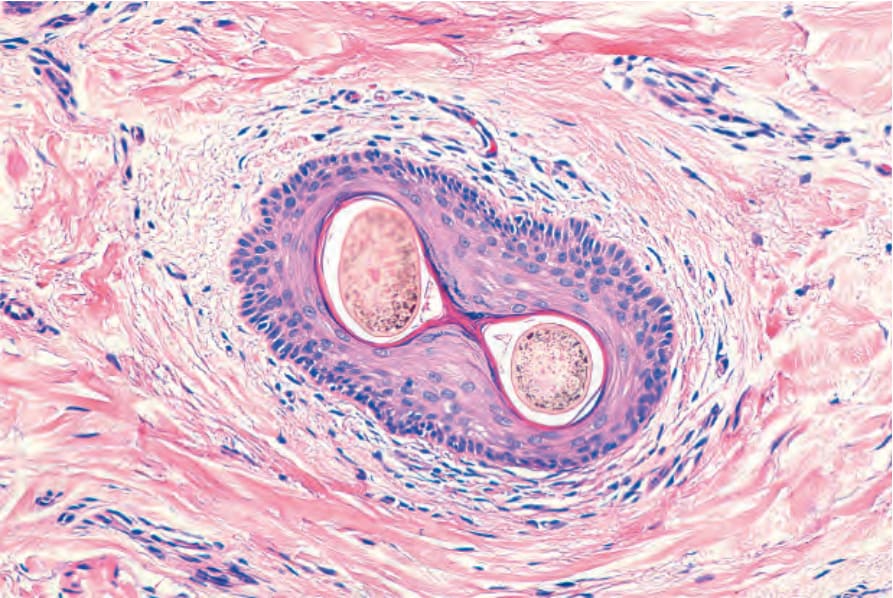
圖 22-17:漏斗部 (infundibulum)。水平切片。其壁由鱗狀複層角化上皮 (squamous stratified keratinized epithelium) 構成。周圍真皮被一些淋巴球浸潤。可見兩根毛幹自單一毛囊口冒出。
Fig. 22.17 Infundibulum. Horizontal section. The wall is made up of squamous stratified keratinized epithelium. The surrounding dermis is infiltrated by some lymphocytes. There are two hair shafts emerging from a single ostium.
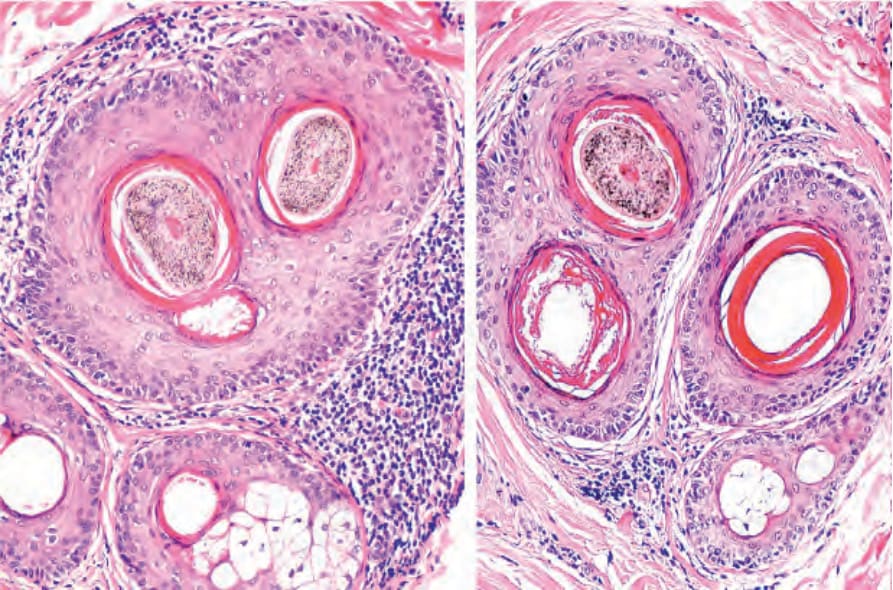
圖 22-46:複合毛髮漏斗部 (compound hair infundibulum),在一名罹患 androgenetic alopecia 的病人中被淋巴球浸潤與輕度同心圓性纖維化所環繞。
Fig. 22.46 Compound hair infundibulum surrounded by a lymphocytic infiltrate and mild concentric fibrosis in a patient with androgenetic alopecia.